

Abstract
Long‐term stress can lead to long‐term increased cortisol plasma levels, which increases the risk of numerous diseases. Dehydroepiandrosterone (DHEA) and its sulfated form dehydroepiandrosterone‐sulfate (DHEAS), together DHEA(S), have shown to counteract some of the effects of cortisol and may be protective during stress. The program “Mindfulness‐Based Stress Reduction” (MBSR) has shown to have positive effects on stress. The present study examined a possible effect of MBSR on DHEAS in plasma compared to a waiting list and a locally developed stress reduction program (LSR) in people with self‐reported stress. The study was a three‐armed randomized controlled trial conducted in a municipal health care center in Denmark. It included 71 participants with self‐reported stress randomized to either MBSR (n = 24) or LSR (n = 23), or a waiting list (n = 24). Blood samples were collected at baseline and at 12 weeks follow‐up to estimate effects of MBSR on DHEAS. The effect of MBSR on DHEAS was statistically significant compared to both the waiting list and LSR. We found a mean effect of 0.70 µmol/L (95% confidence interval [CI] = 0.18–1.22) higher DHEAS in the MBSR group compared with the waiting list group and a mean effect of 0.54 µmol/L (95% CI = 0.04–1.05) higher DHEAS in the MBSR group compared with the LSR group. Findings indicate an effect on DHEAS of the MBSR program compared to a waiting list and LSR program in people with self‐reported stress. However, we consider our findings hypothesis‐generating and validation by future studies is essential.
Study Highlights.
WHAT IS THE CURRENT KNOWLEDGE ON THE TOPIC?
Prolonged stress can alter cortisol levels and entail numerous negative effects in the body. Dehydroepiandrosterone (DHEA) and dehydroepiandrosteron‐sulphat (DHEAS) together DHEA(S), have shown to counteract several of these negative effects. The program “Mindfulness‐Based Stress Reduction” (MBSR) has a scientifically documented effect on symptoms of stress. Only few studies have investigated the role of DHEA(S) as a potential mediator of health improvements associated with MBSR training or interventions that are similar to MBSR (yoga, meditation, and mindfulness). Findings point in different directions, but several studies find an association between the interventions and increased DHEAS levels.
WHAT QUESTION DID THIS STUDY ADDRESS?
This study explores the possibility that MBSR training can affect DHEAS levels positively in people with self‐reported stress.
WHAT DOES THIS STUDY ADD TO OUR KNOWLEDGE?
In the present study, we found a statistically significant effect of the MBSR program on DHEAS levels, alike to the effects found in several other studies with similar interventions. Thus, we consider it likely that MBSR may affect DHEAS. Limitations to this study adds to knowledge on how to conduct future trials in the best way.
HOW MIGHT THIS CHANGE DRUG DISCOVERY, DEVELOPMENT, AND/OR THERAPEUTICS?
We believe that this study can help facilitate future studies that address a possible association between the MBSR program and DHEAS. This can contribute to understanding the health improving effects of MBSR and thereby help promote mental health. In addition, this study contributes to our understanding of how DHEAS can possibly be modulated.
INTRODUCTION
Mental health is just as important as physical health and stress is an increasing health concern worldwide. 1 , 2 Danish national reports reveal that ~ 25% of Danes experience high levels of stress, causing a considerable financial burden of society. 3 In daily life, we are exposed to many positive and negative events, continuously modulating our stress response. The stress response is a complex psychophysiological process, which makes us capable of responding efficiently to stressors. 4 Shifts in the hypothalamus‐pituitary‐adrenal axis (HPA axis) induce changes in cortisol levels, which normally leads to a broad range of adaptive physiological reactions, including alterations in metabolic and immunological processes and brain functions. Prolonged stress causing long‐term rises in cortisol levels can lead to cortisol resistance and associated inflammation, predisposing to numerous serious diseases, including cardiovascular disease, osteoporosis, and depression, 3 , 5 , 6 as well as dysregulation of the HPA axis. 5 , 7 The negative effect of long‐term rise of high cortisol levels on brain functions involve cognition, sleep, and memory. 8 This is partly due to increased reactivity in the amygdala, 9 altered synaptic plasticity and inhibition of neurogenesis in the hippocampus. 10
As long‐term stress can lead to many adverse events, including altered brain function and predisposition to numerous diseases, it is essential to find effective ways to promote mental health and thus reduce stress. The program “Mindfulness‐Based Stress Reduction” (MBSR) developed by Jon Kabat‐Zinn in the late 1970s 11 has received growing interest. The MBSR program has scientifically documented effects on symptoms of anxiety, 12 depression (in terms of Mindfulness Based Cognitive Therapy), 13 , 14 stress, 6 and quality of life. 11 Furthermore, the program has demonstrated positive effects on immune function 15 and chronic pain. 16 Practicing mindfulness has additionally been found to induce functional and structural changes in areas related to stress regulation, including hippocampus, prefrontal cortex, and amygdala. 17 , 18 , 19 , 20 , 21
MBSR is informed by theories and practices from contemplative traditions, science, medicine, psychology, and education. Participants develop a new relationship with experience characterized by present moment focus. Mindfulness is described through systematic mental training that develops meta‐awareness (self‐awareness), an ability to effectively modulate own behavior (self‐regulation), and a positive relationship between self and others that transcends self‐focused needs and increases prosocial characteristics (self‐transcendence). 22 This is reflected in Jon Kabat Zinn’s operational definition of mindfulness “…the awareness arising through paying attention on purpose in the present moment, non‐judgmentally, in the service of self‐understanding, wisdom, and compassion.” 23
Thus, applying and practicing mindfulness in daily life is thought to cultivate enhanced self‐regulation and resilience. 24 , 25 The beneficial effects of MBSR are also correlated by positive effects on various physiological markers of stress, including heart rate variability. 26
Less studied as a marker of stress and resilience is the steroid hormone dehydroepiandrosterone (DHEA), which is primarily released from the adrenal gland after stimulation with adrenocortico‐trophic hormone and subsequently sulfated to its dehydroepiandrosteron‐sulphat derivate (DHEAS). 27 , 28 DHEA and DHEAS (DHEA[S]) levels vary during life, peaking in the 20s and subsequently decreasing with increasing age. 28 There is evidence that DHEAS decreases in people who suffer from stress. 29 DHEA(S) has been shown to counteract several of the negative effects of cortisol by modulating the immune system, protecting against neurotoxicity and inducing neurogenesis in parts of the brain including the hippocampus. 28 , 30 DHEA(S) assert the effects in various ways, partly by modulating neuronal receptor activity 31 and by antagonizing the glucocorticoid suppression of lymphocyte proliferation. 32 The hypothesis is that DHEA(S) protect the brain and body from the adverse events caused by high cortisol levels, and high levels of DHEA(S) are thus an advantage during long‐term stress. 27
Only few studies have investigated the role of DHEA(S) as a potential mediator of health improvements associated with MBSR training. This study explores the possibility that the production and secretion of DHEA(S) can be stimulated by MBSR training in people who suffer from long‐term stress. DHEAS is more abundant than DHEA in the circulation, it undergoes less diurnal variation and has a longer half‐life. 33 Thus, in this study, we used DHEAS plasma levels as an outcome measure. The objective was to test the hypothesis that MBSR training can modulate DHEAS. We compared pre‐post changes in DHEAS in participants randomized to (1) MBSR, (2) TAU (a local stress reduction program [LSR]), and (3) a waiting list control group.
METHODS
Design
This study is based on data from a three‐armed randomized controlled pilot trial (RCT) on the effectiveness of different interventions on self‐reported stress. The primary objective was to investigate the feasibility of examining the effects of MBSR compared to an LSR and a waiting list control group in a real‐life setting—a municipal health care center in Denmark. We found it was feasible to conduct a valid RCT assessing the effect of stress reduction interventions in a real‐life municipal health care setting among adults with a clear need for stress reduction interventions based on scores on mental health. 34 In the feasibility paper, we reported proposed effects on self‐reported measures. As explanations on hypotheses about relationships between mental health promoting interventions and biological markers, such as DHEAS, are more complex, we have chosen to report the proposed effect on DHEAS in this separate paper.
The study included 71 participants with self‐reported stress, who had individually contacted the Aarhus Municipal Health Care Center for this reason. A member from the project team contacted individuals who met the inclusion criteria and provided information about the project. They also received detailed written information about the project via e‐mail. At the appointment for baseline measurements, a member of the project team also verbally informed the individuals about the project. All attendants at the appointment for baseline measurements agreed to participate and provided written consent. After participants were enrolled in the trial, baseline measurements were collected, including blood sampling to quantify (e.g., DHEAS in plasma). This was repeated at the follow‐up visit at 12 weeks. Blood samples were collected by professional medical laboratory technicians at Aarhus University Hospital (AUH), Denmark. Participants were randomized and allocated to the three trial‐arm groups: (1) an MBSR program (2) an LSR, (3) a waiting list (control group). The process of randomization, study design, and interventions are described in detail in the feasibility paper. 34
Interventions
Mindfulness‐Based Stress Reduction
The manualized 8‐week MBSR program consists of one 90‐min weekly session and one 7‐h silent retreat between weeks 6 and 7. The MBSR program is an intensive course in mindfulness meditation and includes teaching about, for example, perception, stress, and communication as well as dialogues. Daily homework consists of 45 min of guided formal mindful yoga and meditation practice and informal practicing being mindful in daily life. 11 For a more detailed description see Juul et al. 34 The MBSR program was conducted in groups of ~ 30 participants and taught by a trained MBSR teacher from the Danish Center of Mindfulness, Aarhus University, Denmark; the teacher was not part of the research team.
Local Stress Reduction Program
The LSR program is aimed at stress reduction, developed and taught by a local psychologist employed in Aarhus Municipality. The program is based on acceptance and commitment therapy, which has a deeper focus on the cognitive‐behavioral component compared to MBSR. The LSR program is structured similarly to MBSR, with one weekly 90‐min group session and 45 min of daily homework between sessions comprising different mindfulness exercises and implementation of self‐care activities. The group size was ~ 12 participants. Before the first group session, participants were offered an individual consultation with the psychologist. For a more detailed week‐to‐week description of the program see Juul et al. 34
Waiting list
Participants in the waiting list control group were offered LSR or MBSR after data collection at the 12‐week follow‐up. To imitate a real‐life setting, participants were not given any restrictions in regard to seek help or participate in stress interventions. During the study period, some participants in all three groups participated in other/additional stress interventions. For details see Juul et al. 34
Outcome
Clinical measures: Blood samples
To evaluate the effects on DHEAS, individual blood samples were collected at baseline and postintervention; at 12‐week follow‐up at AUH. All blood samples were processed and analyzed at the Department of Biochemistry, AUH, centrifuged, pipetted, and subsequently analyzed using high performance liquid chromatography followed by tandem mass spectroscopy to quantify the amount of DHEAS (µmol/L) in the blood. 35
Data analysis
We estimated the effects on DHEAS (µmol /L) comparing change in DHEAS level in the three groups with 95% confidence intervals (95% CIs) and p values. Effect was estimated using linear regression models adjusting for gender, age, educational level, history of mental illness, body mass index, systolic and diastolic blood pressure, perceived stress score, and DHEAS level at baseline. In addition, we analyzed characteristics of participants lost to follow‐up using the χ2 test. A sensitivity analysis was performed because a greater loss to follow‐up was observed in the MBSR group compared with the LSR and waiting list control groups. This analysis was conducted using linear regression models adjusting for the same variables as above. In the sensitivity analysis, we compared the effect on DHEAS levels in the three groups, where changes in DHEAS levels from baseline to follow‐up were set to equal zero for participants missing follow‐up measurements. All analyzes were performed in STATA 16.
Ethics approval and consent to participate
The study was conducted according to the Helsinki Declaration. 36 It was registered at ClincalTrials.gov (identifier: NCT03663244) and approved by the Central Denmark Region Committee of Health Research Ethics (j.no. 1‐10‐72‐182‐17) and the Danish Data Protection Agency (j.no: 2015‐57‐0098). All participants were informed verbally and in writing and signed an informed consent form.
RESULTS
Participant characteristics
Characteristics of the participants are shown in Table 1 and described in detail elsewhere. 34
TABLE 1.
Characteristics of 71 participants included in a three‐armed pilot RCT among individuals seeking help due to stress in a Danish municipal health care center, 2018 from Juul et al. 34
| MBSR (n = 24) | LSR (n = 23) | Waiting list (n = 24) | |
|---|---|---|---|
| Gender, female (%) | 11 (46) | 16 (70) | 15 (63) |
| Age, median (q1, q3) | 46 (36, 51) | 41 (29, 49) | 45 (41, 52) |
| Education (%) | |||
| ≤11 years | 2 (8) | 1 (4) | 0 |
| >11 to <16 years | 6 (25) | 10 (43) | 10 (42) |
| ≥16 years | 16 (67) | 12 (52) | 14 (58) |
| Living alone (%) | 5 (21) | 4 (17) | 5 (21) |
| Living with parents (%) | 0 | 1 (4) | 0 |
| Living with a partner, no children (%) | 9 (38) | 7 (30) | 9 (38) |
| Living with a partner and children/adolescents (%) | 6 (25) | 3 (13) | 6 (25) |
| Living with children/adolescents, no partner (%) | 2 (8) | 4 (17) | 2 (8) |
| Living with other adults (%) | 2 (8) | 4 (17) | 2 (8) |
| Employment status | |||
| Employed (%) | 17 (71) (9 (53%) sick leave) | 15 (65) (8(53%) sick leave) | 16 (67) (13 (81%) sick leave) |
| Unemployed (%) | 3 (13) | 5 (22) | 5 (21) |
| Sick leave >3 months (%) | 2 (8) | 2 (9) | 2 (8) |
| Other | 2 (8) | 1 (4) | 1 (4) |
| Disease, present/earlier (%) | |||
| Asthma | 0/3 (13) | 3 (13)/1(4) | 1 (1)/1(1) |
| Diabetes | 0/0 | 1 (4)/0 | 0/0 |
| Hypertension | 3 (13)/1 (4) | 3 (13) /3 (13) | 3 (13)/3 (13) |
| Myocardial infarction | 0/0 | 0/0 | 0/0 |
| Angina pectoris | 0/2 (8) | 0/0 | 0/0 |
| Stroke | 0/0 | 0/0 | 0/0 |
| COLD | 0 /1 (4) | 1 (5)/0 | 0/0 |
| Osteoarthritis | 5 (21)/0 | 2 (9)/0 | 1 (4)/1 (4) |
| Rheumatoid arthritis | 2/(8)/0 | 1 (4)/0 | 0/1 (4) |
| Osteoporosis | 3 (13)/0 | 0/0 | 0/0 |
| Prolapse | 5 (21)/1 (4) | 1 (5)/2 (9) | 1 (4)/2 (8) |
| Cancer | 0 /1 (4) | 0/0 | 0/0 |
| Migraine | 7 (29)/2 (8) | 4 (17)/8 (35) | 6 (25)/4 (17) |
| Mental disorder ≤6 months | 5 (21)/3 (13) | 2 (9)/1 (4) | 2 (9) /1 (4) |
| Mental disorder >6 months | 4 (17)/1 (4) | 4 (18)/0 | 2 (8) /4 (17) |
| Self‐reported mental health | |||
| Perceived Stress Scale, mean (SD) | 24.6 (5.6) | 24.9 (5.6) | 26.6 (4.6) |
| Clinical measurements | |||
| Systolic blood pressure, mm Hg, mean (SD) | 127.1 (15.1) | 125.7 (18.9) | 123.4 (17.0) |
| Diastolic blood pressure, mm Hg, mean (SD) | 82.6 (9.9) | 80.7 (13.1) | 81.6 (11.6) |
| Weight, kg, median (q1, q3) | 79.0 (70.0, 92.0) | 75.0 (64.0, 92.0) | 68.5 (63.5, 84.0) |
| BMI, kg/m2 ≥25 (%) | 18 (75) | 14 (61) | 9 (39) |
| Waist circumference, cm, median (q1, q3) | 95.5 (90.5, 106.5) | 94.0 (87.0, 105.0) | 92.0 (80.5, 99.0) |
| DHEAS µmol/L mean (SD) | 3.17 (2.25) | 2.79 (1.38) | 3.45 (1.81) |
Abbreviations: RCT, randomized controlled trial; MBSR, Mindfulness‐Based Stress Reduction; LSR, locally developed stress reduction intervention; CI, confidence interval; q, quartile; BMI, body mass index; DHEAS, dehydroepiandrosterone‐sulfate.
Loss to follow‐up
In the present study, nine participants in the MBSR group were lost to follow‐up (missing blood samples at either baseline or follow‐up, or both); loss to follow‐up was five in the LSR group and four in the waiting list group. A total of 15 participants in the MBSR group, 18 participants in the LSR group, and 20 participants in the waiting list group completed all outcome measures (Figure 1).
FIGURE 1.
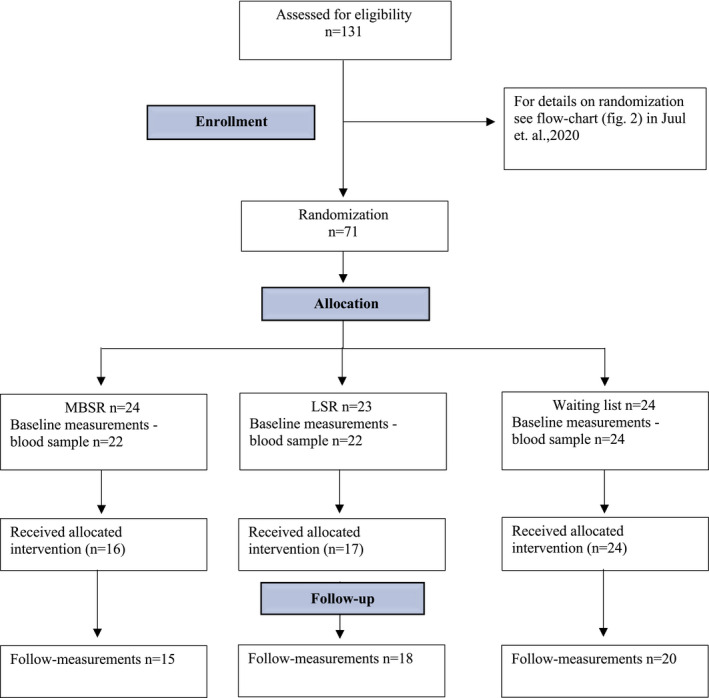
Flow chart showing loss to follow‐up in a three‐armed randomized controlled pilot study comparing effects of different stress interventions on the steroid hormone dehydroepiandosteron (DHEAS) levels in a real life setting in a municipal health care center in Denmark, 2018. LSR, local stress reduction program
Missing outcome measures were only statistically significantly associated with not completing the allocated intervention; however, we found that there were no particular characteristics for participants who completed less than five sessions. There was a tendency though that fewer of these participants were on sick leave (p = 0.07). 34
A mean minor difference in age was seen between the group with missing outcomes compared to those who completed all outcome measures, although not statistically significant.
Effect on outcome
Table 2 shows results on differences in change in DHEAS (µmol/L) from baseline to 12‐week follow‐up between the MBSR group and the LSR and the waiting list group, respectively. Table 3 shows results of a sensitivity analysis. In this analysis, change in DHEAS levels from baseline to follow‐up was set to equal zero for participants with missing follow‐up measurements.
TABLE 2.
Mean change and effect on DHEAS levels (µmol/L) from baseline to 12‐week follow‐up in the three groups
|
Baseline, mean (µmol/L) (SD) |
12‐week follow‐up, mean (µmol/L) (SD) |
Mean change (95%CI) from baseline to 12‐week follow‐up |
Mean effect (µmol/L) of MBSR a (95%CI), p value |
|---|---|---|---|
|
Waiting‐list (n = 24): 3.45 (1.81) |
Waiting‐list (n = 20): 3.04 (1.57) |
Waiting‐list (n = 20): −0.20 (−0.50 to 0.10) |
REF |
|
MBSR (n = 22): 3.17 (2.25) |
MBSR (n = 15): 3.34 (1.70) |
MBSR (n = 15): 0.19 (−0.25 to 0.64) |
0.70 (0.18 to 1.22), 0.01 |
|
LSR (n = 22): 2.79 (1.38) |
LSR (n = 19): 2.64 (1.50) |
LSR (n = 18): −0.18 (−0.47 to 0.12) |
REF |
|
MBSR (n = 22): 3.17 (2.25) |
MBSR (n = 15): 3.34 (1.70) |
MBSR (n = 15): 0.19 (−0.25 to 0.64) |
0.54 (0.04 to 1.05), 0.04 |
Includes participants with completion of outcome measures collected both at baseline and follow‐up.
Abbreviations: BMI, body mass index; DHEAS, dehydroepiandrosterone‐sulfate; MBSR, Mindfulness‐Based Stress Reduction; LSR, locally developed stress reduction program; CI, confidence interval.
Adjusted for gender, age, educational level, history of mental disease BMI, systolic‐ and diastolic blood pressure, DHEAS level and perceived stress score at baseline.
TABLE 3.
Sensitivity analysis: Effects in DHEAS levels (µmol/L) comparing the three groups when taken into account loss to follow‐up
|
Mean effect of MBSR (µmol/L) a (95% CI), p value |
|
|---|---|
| MBSR (n = 22) vs. wait‐list (n = 24) | 0.45 (0.05 to 0.84), 0.03 |
| MBSR (n = 22) vs. LSR (n = 23): | 0.37 (−0.02 to 0.76), 0.06 |
In this analysis, change in DHEAS levels from baseline to follow‐up was set to equal zero, for participants with missing follow‐up measurements.
Abbreviations: DHEASl; dehydroepiandrosterone‐sulfate; MBSR, Mindfulness Based Stress Reduction; LSR, locally developed stress reduction program, CI, confidence interval.
Adjusted for gender, age, educational level, history of mental disease BMI, systolic‐ and diastolic blood pressure, DHEAS level and perceived stress score at baseline.
DISCUSSION
Main findings
The present study indicates an effect of the MBSR program on DHEAS. First, we evaluated the effect on DHEAS in MBSR compared with a waiting list group and found a statistically significant mean effect of 0.70 µmol/L (95% CI = 0.18–1.22) higher DHEAS in the MBSR group (Table 2). In addition, Juul et al. 34 found that the MBSR group had statistically significant better subjective outcomes on well‐being and resilience measured by validated questionnaires (WHO‐5 and Brief Resilience Scale) compared with a waiting list group. Our findings could thus be interpreted as a possible biological marker and even a possible objective measure for improved mental health. When compared to an active control (the LSR group), we found similar results with a mean effect of 0.54 µmol/L (95% CI= 0.04–1.05) higher DHEAS in the MBSR group (Table 2).
Comparison with existing literature
To our knowledge, only two previous studies have examined the association between DHEAS levels and the MBSR program. Carlson et al. 33 investigated the changes in DHEAS during participation in the MBSR program in people with breast and prostate cancer. They did not find any statistically significant change between baseline and post intervention. An effect could possibly have been observed if they had compared with a control group; thus, this study is not directly comparable with our findings.
Robinson 37 examined the effect of MBSR in a group of people with HIV and compared changes in DHEAS in the MBSR intervention with a control group, respectively. No effect of MBSR compared to the control group was observed. It should be noted that only half of the participants in the intervention group completed the MBSR program and these participants differed substantially from those who completed the program having higher cortisol levels and lower viral loads at baseline. This causes some uncertainty concerning the validity of the results.
Schultchen et al. 38 used an 8‐week body scan program inspired by the MBSR program and compared it to an active control group asked to listen to an audiobook every day for the same amount of time. The study population was a nonclinical population. Equally positive changes were observed in both groups.
A few studies examined associations between DHEAS and interventions similar to MBSR, including yoga, meditation, and mindfulness. Several of these studies point in the same direction as findings in the present study. Bisht et al. 39 found significantly increased DHEAS levels before and after a 12‐week yoga‐based lifestyle intervention in parents of kids with retinoblastoma; the same intervention found positive effects on participants’ psychological stress levels. Manzaneque et al. 40 examined changes in DHEAS levels in individuals with anxiety and depression before and after a 2‐month mindfulness meditation program; they also found statistically significantly increased DHEA(S) levels. However, both studies lacked a control group. Chatterjee et al. 41 examined a yogic training program in healthy individuals and compared changes in DHEAS levels between an intervention and a control group, respectively; this study found a statistically significant effect of the yogic training program on DHEAS levels.
A few other studies point in a different direction and do not support present findings. Argerwal et al. 42 found no effect on DHEAS levels of yoga/meditation compared with a control group in patients with HIV who used crack cocaine. Vera et al. 43 studied the effect on DHEAS levels of long‐term yoga practicing in healthy individuals and found no effect. Kim et al. 44 examined individuals suffering from post‐traumatic stress disorder (PTSD) and found no significant changes in DHEA(S) levels after intervention with mindfulness‐based stretching despite significant improvement of PTSD symptoms and cortisol levels.
Existing literature points in different directions regarding a possible association among yoga, meditation, and mindfulness and DHEAS levels. However, we found that most studies support findings from the present study, suggesting that mindfulness, yoga, and meditation may have a positive effect on DHEAS levels.
We notice that in many of the studies not corroborating our findings, the participants were suffering from disease (HIV and cancer) or mental illness like PTSD. The reason for this is unclear, but could be explained by a different or more complex endocrine dysregulation in individuals suffering from these diseases. For instance, patients with HIV have been reported to have affected androgen levels, including altered DHEA(S) levels, depending on the stage of HIV disease. 45 Moreover, in the studies described above, interventions were not fully comparable to those in our study. Therefore, although interventions were similar (meditation, yoga, and mindfulness‐based), the differences still constitute a potentially important limitation compared with our study. Replication studies examining the effects of MBSR on DHEA(S) levels are needed to promote mental health and understand underlying biological mechanisms.
Strengths and limitation
A strength of the present study is the RCT design. However, the study design also has limitations because the RCT was originally conducted as a pilot study with a different primary outcome. It was conducted in a real‐life setting in individuals with self‐reported stress in a municipal health care center in Denmark in order to evaluate effectiveness. Effectiveness trials with broad inclusion criteria are not the optimal design to investigate biomarkers. Changes in DHEA(S) levels have been associated with different disease states and some medication use. 28 , 45 , 46 We lacked information on medication and nutritional supplement use and had only self‐reported information on diseases. The occurrence of self‐reported chronic diseases was not high in this study population. However, to limit the risk of these factors as confounders in a future study, we find it important to use an efficacy trial design with strict inclusion criteria. Furthermore, the exact time of the day for collection of blood samples was not documented, although all samples were collected during the daytime. Some reports suggest diurnal variation of DHEAS, whereas others report this as being limited. 33 , 47 , 48 Therefore, it is relevant to collect samples at the same time, in a future study, to eliminate this as possible bias.
The small sample size given the pilot design constitutes a statistical uncertainty. Despite this, we found a significant effect of the MBSR course on DHEAS compared with the other groups.
We experienced a greater loss to follow‐up in the MBSR group compared to the other groups. To accommodate this, we conducted a sensitivity analysis. Changes in DHEAS levels were set to equal zero for blood samples of participants lost to follow‐up, attempting to eliminate a possible overestimation of effects on DHEAS levels caused by the loss to follow‐up.
We found the effect on DHEAS levels was still statistically significantly higher in the MBSR group compared with the waiting list group (Table 3). On the contrary, the effect on DHEAS were no longer statistically significantly higher in the MBSR group compared with the LSR group. However, the effect still tended to be higher with a mean effect of 0.37 µmol/L (95% CI = −0.02 to 0.76) higher DHEAS for MBSR compared with LSR (Table 3). In Juul et al., 34 results showed greater improvement in all mental outcomes of MBSR compared with LSR, although the results were not statistically significant. It seems that the difference in effect on mental health was not as pronounced between MBSR and LSR. This could explain why changes in DHEAS did not differ quite as much as when comparing MBSR with the waiting list group. The loss to follow‐up in the MBSR group is a limitation of the present study, although we consider it unlikely to cause bias. It is very doubtful that the loss to follow‐up is associated with both the outcome measure (DHEAS) and the allocated intervention group. Juul et al. 34 observed that participants in the MBSR group had better psychological outcome, but there was not a differentiated loss to the questionnaire competition rate at follow‐up. It should also be added that no characteristics were found for the participants who completed less than five sessions of their allocated intervention, which makes it unlikely that these participants would differ regarding DHEAS from those who completed the intervention.
We used the Department of Biochemistry at AUH to conduct our outcome analyses, and the staff who collected and analyzed outcome measures were thus blinded to the study. The participants were not blinded to the intervention they received. However, the outcome was a blood sample, which reduces the risk of information bias.
Altogether, our trial has strengths and limitations. The limitations entail some uncertainty, which underlines that our findings should be regarded as hypothesis generating and not evidence‐bearing. We find it relevant to conduct clinical trials with larger study samples, including a more selected group to limit risk of confounding.
CONCLUSION
We found a statistically significant effect of the MBSR program on DHEAS compared with the waiting list group and LSR group in citizens with self‐reported stress. Still, relatively few studies have addressed the association between DHEAS and the MBSR program or other similar interventions, such as mindfulness, yoga, and meditation. However, many of these have observed an association between the interventions and positive effects on DHEAS. We consider it likely that MBSR may affect DHEAS, although this study can only be considered as hypothesis generating.
CONFLICT OF INTEREST
Aarhus University offers revenue‐funded MBSR teacher training education and MBSR courses. The authors declared no competing interests for this work.
AUTHOR CONTRIBUTIONS
M.A.J. wrote the manuscript. L.J., K.J.P., and L.O.F. designed the research. K.J.P. performed the research. L.J. analyzed the data.
Jørgensen MA, Pallesen KJ, Fjorback LO, Juul L. Effect of Mindfulness‐Based Stress Reduction on dehydroepiandrosterone‐sulfate in adults with self‐reported stress. A randomized trial. Clin Transl Sci. 2021;14:2360–2369. 10.1111/cts.13100
Funding information
This work was supported by TrygFonden (grant number: 119327). TrygFonden had no role in the study design, the collection, analysis, and interpretation of data, or in writing the manuscript.
REFERENCES
- 1. WHO) . Mental health – burden. Available from: https://www.WHO.int/health‐topics/mental‐health#tab=tab_2. Accessed September 25, 2020.
- 2. WHO) . Mental health action plan 2013‐2020. Available from: https://www.WHO.int/mental_health/action_plan_2013/bw_version.pdf?ua=1. Accessed August 14, 2020.
- 3. Sundhedsstyrrelsen . Danskernes sundhed – Den Nationale Sundhedsprofil 2017: Sundhedsstyrrelsen; 2018. Available from: https://www.sst.dk/‐/media/Udgivelser/2018/Den‐Nationale‐Sundhedsprofil‐2017.ashx?la=da&hash=421C482AEDC718D3B4846FC5E2B0EED2725AF517. Accessed May 10, 2021.
- 4. Woda A, Picard P, Dutheil F. Dysfunctional stress responses in chronic pain. Psychoneuroendocrinology. 2016;71:127‐135. [DOI] [PubMed] [Google Scholar]
- 5. Charney DS. Psychobiological mechanisms of resilience and vulnerability: implications for successful adaptation to extreme stress. Am J Psychiatry. 2004;161(2):195‐216. [DOI] [PubMed] [Google Scholar]
- 6. Khoury B, Sharma M, Rush SE, Fournier C. Mindfulness‐based stress reduction for healthy individuals: A meta‐analysis. J Psychosom Res. 2015;78(6):519‐528. [DOI] [PubMed] [Google Scholar]
- 7. Lee DY, Kim E, Choi MH. Technical and clinical aspects of cortisol as a biochemical marker of chronic stress. BMB Rep. 2015;48(4):209‐216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Ouanes S, Popp J. High cortisol and the risk of dementia and Alzheimer's disease: a review of the literature. Front Aging Neurosci. 2019;11:43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Mitra R, Sapolsky RM. Acute corticosterone treatment is sufficient to induce anxiety and amygdaloid dendritic hypertrophy. Proc Natl Acad Sci USA. 2008;105(14):5573‐5578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Frodl T, O'Keane V. How does the brain deal with cumulative stress? A review with focus on developmental stress, HPA axis function and hippocampal structure in humans. Neurobiol Dis. 2013;52:24‐37. [DOI] [PubMed] [Google Scholar]
- 11. Vibe M, Bjørndal A, Fattah S, et al. Mindfulness‐based stress reduction (MBSR) for improving health, quality of life and social functioning in adults: a systematic review and meta‐analysis. Campbell Syst Rev. 2017;13(1):1‐264. [Google Scholar]
- 12. Kabat‐Zinn J, Massion AO, Kristeller J, et al. Effectiveness of a meditation‐based stress reduction program in the treatment of anxiety disorders. Am J Psychiatry. 1992;149(7):936‐943. [DOI] [PubMed] [Google Scholar]
- 13. Goldberg SB, Tucker RP, Greene PA, et al. Mindfulness‐based interventions for psychiatric disorders: A systematic review and meta‐analysis. Clin Psychol Rev. 2018;59:52‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Kuyken W, Warren FC, Taylor RS, et al. Efficacy of mindfulness‐based cognitive therapy in prevention of depressive relapse: an individual patient data meta‐analysis from randomized trials. JAMA Psychiatry. 2016;73(6):565‐574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Davidson RJ, Kabat‐Zinn J, Schumacher J, et al. Alterations in brain and immune function produced by mindfulness meditation. Psychosom Med. 2003;65(4):564‐570. [DOI] [PubMed] [Google Scholar]
- 16. Khoo E‐L, Small R, Cheng W, et al. Comparative evaluation of group‐based mindfulness‐based stress reduction and cognitive behavioural therapy for the treatment and management of chronic pain: A systematic review and network meta‐analysis. Evid Based Ment Health. 2019;22(1):26‐35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. King AP, Block SR, Sripada RK, et al. Altered default mode network (DMN) resting state functional connectivity following a mindfulness‐based exposure therapy for posttraumatic stress disorder (PTSD) in combat veterans of Afghanistan and Iraq. Depress Anxiety. 2016;33(4):289‐299. [DOI] [PubMed] [Google Scholar]
- 18. Lazar SW, Kerr CE, Wasserman RH, et al. Meditation experience is associated with increased cortical thickness. NeuroReport. 2005;16(17):1893‐1897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Taren AA, Gianaros PJ, Greco CM, et al. Mindfulness meditation training alters stress‐related amygdala resting state functional connectivity: a randomized controlled trial. Soc Cogn Affect Neurosci. 2015;10(12):1758‐1768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Tang YY, Hölzel BK, Posner MI. The neuroscience of mindfulness meditation. Nat Rev Neurosci. 2015;16(4):213‐225. [DOI] [PubMed] [Google Scholar]
- 21. Lutz J, Herwig U, Opialla S, et al. Mindfulness and emotion regulation–an fMRI study. Soc Cogn Affect Neurosci. 2014;9(6):776‐785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Vago DR, Silbersweig DA. Self‐awareness, self‐regulation, and self‐transcendence (S‐ART): a framework for understanding the neurobiological mechanisms of mindfulness. Front Hum Neurosci. 2012;6:296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Kenny M, Luck P, Koerbel L. Tending the field of mindfulness‐based programs: the development of international integrity guidelines for teachers and teacher training. Glob Adv Health Med. 2020;9:2164956120923975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Janssen M, Heerkens Y, Kuijer W, et al. Effects of Mindfulness‐Based Stress Reduction on employees’ mental health: A systematic review. PLoS One. 2018;13(1):e0191332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Kabat‐Zinn J. Full catastrophe living. New York, NY, USA: Bantam Books; 2013. [Google Scholar]
- 26. Heckenberg RA, Eddy P, Kent S, et al. Do workplace‐based mindfulness meditation programs improve physiological indices of stress? A systematic review and meta‐analysis. J Psychosom Res. 2018;114:62‐71. [DOI] [PubMed] [Google Scholar]
- 27. Kamin HS, Kertes DA. Cortisol and DHEA in development and psychopathology. Horm Behav. 2017;89:69‐85. [DOI] [PubMed] [Google Scholar]
- 28. Stárka L, Dušková M, Hill M. Dehydroepiandrosterone: a neuroactive steroid. J Steroid Biochem Mol Biol. 2015;145:254‐260. [DOI] [PubMed] [Google Scholar]
- 29. Lennartsson A‐K, Theorell T, Rockwood AL, et al. Perceived stress at work is associated with lower levels of DHEA‐S. PLoS One. 2013;8(8):8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Kimonides VG, Khatibi NH, Svendsen CN, et al. Dehydroepiandrosterone (DHEA) and DHEA‐sulfate (DHEAS) protect hippocampal neurons against excitatory amino acid‐induced neurotoxicity. Proc Natl Acad Sci USA. 1998;95(4):1852‐1857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Schverer M, Lanfumey L, Baulieu E‐E, et al. Neurosteroids: non‐genomic pathways in neuroplasticity and involvement in neurological diseases. Pharmacol Ther. 2018;191:190‐206. [DOI] [PubMed] [Google Scholar]
- 32. Blauer KL, Poth M, Rogers WM, et al. Dehydroepiandrosterone antagonizes the suppressive effects of dexamethasone on lymphocyte proliferation. Endocrinology. 1991;129(6):3174‐3179. [DOI] [PubMed] [Google Scholar]
- 33. Carlson LE, Speca M, Patel KD, et al. Mindfulness‐based stress reduction in relation to quality of life, mood, symptoms of stress and levels of cortisol, dehydroepiandrosterone sulfate (DHEAS) and melatonin in breast and prostate cancer outpatients. Psychoneuroendocrinology. 2004;29(4):448‐474. [DOI] [PubMed] [Google Scholar]
- 34. Juul L, Pallesen KJ, Bjerggaard M, et al. A pilot randomised trial comparing a mindfulness‐based stress reduction course, a locally‐developed stress reduction intervention and a waiting list control group in a real‐life municipal health care setting. BMC Public Health. 2020;20(1):409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Analysefortegnelsen for Blodprøver og Biokemi; P‐Dehydroepiandrosteronsulf [DHEAS] [updated 23rd of April 2019]. Database with information on different analyses/test performed on blood‐samples at University Hospital in Aarhus. Available from: https://www.auh.dk/om‐auh/afdelinger/blodprover‐og‐biokemi/Til‐fagfolk/analysefortegnelsen/Biokemi/. Accessed August 25, 2020.
- 36. Association TWM . WMA declaration of Helsinki – ethical principles for medical research involving human subjects. Available from: https://www.wma.net/policies‐post/wma‐declaration‐of‐helsinki‐ethical‐principles‐for‐medical‐research‐involving‐human‐subjects/. Accessed February 7, 2021.
- 37. Robinson FP, Mathews HL, Witek‐Janusek L. Psycho‐endocrine‐immune response to mindfulness‐based stress reduction in HIV‐infected individuals. J Altern Complement Med. 2003;9(5):683–694. [DOI] [PubMed] [Google Scholar]
- 38. Schultchen D, Messner M, Karabatsiakis A, et al. Effects of an 8‐week body scan intervention on individually perceived psychological stress and related steroid hormones in hair. Mindfulness. 2019;10(12):2532‐2543. [Google Scholar]
- 39. Bisht S, Chawla B, Tolahunase M, et al. Impact of yoga based lifestyle intervention on psychological stress and quality of life in the parents of children with retinoblastoma. Ann Neurosci. 2019;26(2):66‐74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Manzaneque JM, Vera FM, Ramos NS, et al. Psychobiological modulation in anxious and depressed patients after a mindfulness meditation programme: A pilot study. Stress and Health. 2011;27(3):216‐222. [Google Scholar]
- 41. Chatterjee S, Mondal S. Effect of regular yogic training on growth hormone and dehydroepiandrosterone sulfate as an endocrine marker of aging. Evid Based Complement Alternat Med. 2014;2014:240581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Agarwal RP, Kumar A, Lewis JE. A pilot feasibility and acceptability study of yoga/meditation on the quality of life and markers of stress in persons living with HIV who also use crack cocaine. J Altern Complement Med. 2015;21(3):152‐158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Vera FM, Manzaneque JM, Maldonado EF, et al. Subjective sleep quality and hormonal modulation in long‐term yoga practitioners. Biol Psychol. 2009;81(3):164‐168. [DOI] [PubMed] [Google Scholar]
- 44. Kim SH, Schneider SM, Bevans M, et al. PTSD symptom reduction with mindfulness‐based stretching and deep breathing exercise: randomized controlled clinical trial of efficacy. J Clin Endocrinol Metab. 2013;98(7):2984‐2992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Christeff N, Lortholary O, Casassus P, et al. Relationship between sex steroid hormone levels and CD4 lymphocytes in HIV infected men. Exp Clin Endocrinol Diabetes. 1996;104(2):130‐136. [DOI] [PubMed] [Google Scholar]
- 46. Kannisto S, Laatikainen A, Taivainen A, et al. Serum dehydroepiandrosterone sulfate concentration as an indicator of adrenocortical suppression during inhaled steroid therapy in adult asthmatic patients. Eur J Endocrinol. 2004;150(5):687‐690. [DOI] [PubMed] [Google Scholar]
- 47. Carlström K, Karlsson R, Von Schoultz B. Diurnal rhythm and effects of oral contraceptives on serum dehydroepiandrosterone sulfate (DHEAS) are related to alterations in serum albumin rather than to changes in adrenocortical steroid secretion. Scand J Clin Lab Invest. 2002;62(5):361‐368. [DOI] [PubMed] [Google Scholar]
- 48. Zhao Z‐Y, Xie YI, Fu Y‐R, et al. Circadian rhythm characteristics of serum cortisol and dehydroepiandrosterone sulfate in healthy Chinese men aged 30 to 60 years. A cross‐sectional study. Steroids. 2003;68(2):133‐138. [DOI] [PubMed] [Google Scholar]