

Abstract
Objective:
To compare three-dimensional (3D) ClinCheck™ models with the subjects' actual 3D posttreatment models using the American Board of Orthodontics Objective Grading System (OGS).
Materials and Methods:
This prospective, within-subject study included 27 consecutive cases treated with aligner therapy. The posttreatment plaster models taken immediately after treatment were scanned and converted to stereolithography (STL) files; the ClinCheck models were also converted to STL format. MeshLab software was used to measure the seven components of the OGS, including alignment, marginal ridges, buccolingual inclinations, occlusal contacts, occlusal relationships, overjet and interproximal contacts. An overall OGS deduction score was also calculated.
Results:
Compared with the posttreatment models, the ClinCheck models showed significantly (P = .016) fewer overall OGS point deductions (24 vs 15). These overall differences were due to significantly (P < .05) more deductions among the posttreatment models than the ClinCheck models for alignment (4.0 vs 1.0 deductions), buccolingual inclinations (4.0 vs 3.0 deductions), occlusal contacts (3.0 vs 2.0 deductions), and occlusal relations (4.0 vs 2.0 deductions).
Conclusion:
The ClinCheck models do not accurately reflect the patients' final occlusion, as measured by the OGS, at the end of active treatment.
Keywords: Aligners, Occlusion, Prediction, Objective Grading System
INTRODUCTION
In order for aligner treatments to be valid and effective, the predicted and actual outcomes should be comparable. Align Technology provides orthodontists with ClinCheck™ (Align Technology Inc, Santa Clara, Calif) models, which purportedly reflect the treatment outcomes.1 The orthodontist sends the patient's initial records, plus his or her verbal expectations of the treatment outcome, to the company. The company then fabricates a series of custom-made aligners that sequentially reposition the teeth. The aligners incrementally shift the teeth into place based on the outcome the orthodontist expects to achieve. The final end-of-treatment aligner is based on the three-dimensional (3D) ClinCheck model, which provides the patient's visual treatment outcome.
For clinical applications, it remains unclear how closely the occlusion of the ClinCheck model compares with the actual occlusion produced during treatment. Based on superimpositions of the ClinCheck and final treatment models of 37 patients, it has been shown that extrusion of the central incisors and tipping of the mandibular canines were the most difficult to accurately predict.2 Krieger et al.,3 who compared final ClinCheck and posttreatment models of 50 patients, reported differences <0.4 mm for arch width and lengths and a 0.9 mm difference for overbite. Because the existing comparisons are limited to the anterior six teeth, they provide only partial information about the occlusal characteristics thought to be important for evaluating orthodontic treatments.4
Due to the lack of previous studies, the purpose of the present study was to compare the ClinCheck model with the actual treatment outcome to determine whether overall occlusion and the various aspects of occlusion were comparable. This study endeavors to establish the relative validity of ClinCheck models by determining whether the 3D treatment outcome of aligner therapy can be accurately predicted.
MATERIALS AND METHODS
Twenty-seven consecutive posttreatment patient models were included in this study and compared with their ClinCheck models provided by Invisalign™. The impressions for the posttreatment plaster models were taken immediately after treatment. The models were scanned using the Ortho Insight 3D scanner and converted to a stereolithography (STL) format using the MotionView software (OrthoInsight 3D version 5.5.5002 (MotionView Software, Chattanooga, TN). An STL file was created for each set of models in occlusion as well as one for each maxillary and mandibular arch separately. The digital models were compared with the digital ClinCheck models. The accuracy and reliability of scanned 3D models has been previously established.5–8 The study was approved by the Texas A&M University Baylor College of Dentistry Internal Review Board.
The ClinCheck model files were also converted to the STL format to allow them to be read and assessed using the same software. The MeshLab V1.30 software (ISTI–CNR, Pisa, Italy) program was used to make digital measurements and derive the American Board of Orthodontics (ABO) Objective Grading System (OGS) scores on both the posttreatment and ClinCheck models. The measurements were all made by one calibrated investigator (SGS).
The components of the OGS scores included alignment, marginal ridges, buccolingual inclinations, occlusal contacts, occlusal relationships, overjet, and interproximal contacts. Measurements for each component were made from the digital models using the instructions for measurements from an ABO article explaining the OGS scoring system.9 The MeshLab software allowed the measurements to be made using a digital ruler instead of a standard ruler. After drawing a line on the screen representing the occlusal plane, from which measurements were made to the respective cusps, the zoom function was used to enlarge images 150% in order to measure buccolingual inclinations. The occlusal contacts and marginal ridges were also measured after enlarging the images. Root parallelism was not measured because it is not available for the ClinCheck models. The total number of deductions was measured for each component. The sums of the differences were used to determine the patients' OGS score for their posttreatment model and their ClinCheck model. The difference between the scores for the ClinCheck model and the corresponding posttreatment model were calculated for each component of the OGS score and for the total score.
Replicate analyses of 12 randomly selected patient records were performed to establish reliability. Wilcoxon signed rank tests show no statistically significant difference between the individual component scores or total scores. Method errors of the component score deductions ranged from 0.29 (interproximal contacts) to 0.82 (occlusal contacts). The method error for the total component score was 1.21 deduction.
Statistics
The skewness and kurtosis statistics showed that the measurements were not normally distributed. As such, the data were summarized using medians (50th percentile) and interquartiles (25th and 75th percentiles). The models were statistically compared using Mann-Whitney U-tests. Statistical significance was set at ≤.05.
RESULTS
Median scores for each of the components, as well as for the total score, were higher for the actual than for the ClinCheck models (Table 1). The posttreatment models had more points lost in each component of the OGS score. Differences were greatest (P < .001) for alignment, marginal ridges, and occlusal contacts. Differences for occlusal relations were also highly significant. The smallest differences were for inclinations and overjet. No statistically significant difference was found between the interproximal contacts of the ClinCheck and posttreatment models.
Table 1.
Total Points Lost for American Board of Orthodontics Objective Grading System Score Components and Total Score for the ClinCheck™ Models and Actual Posttreatment Models

The median total score for the ClinCheck models was 14 points with a range of 5–32 (Figure 1). The median total score for the posttreatment models was 24 points with a range of 12–43. The median difference between the total scores was 9 points, which was highly significant (P < .001).
Figure 1.
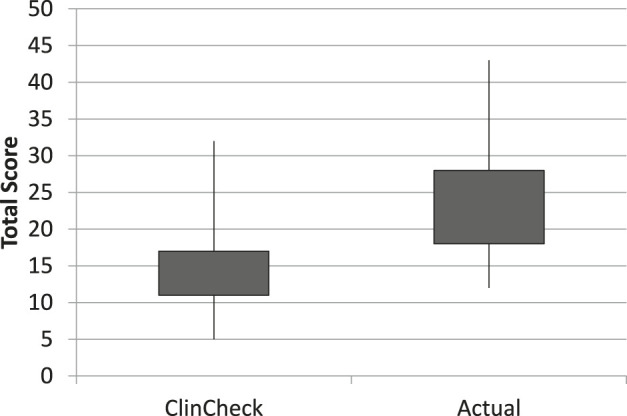
Box-whisker plot of total American Board of Orthodontics Objective Grading System scores (seven components only) for the ClinCheck and actual posttreatment models.
DISCUSSION
The actual posttreatment models showed more deductions than the ClinCheck models for every component of the OGS. Although the OGS has not been previously used for comparison, it has been shown that overjet measured on the posttreatment models is slightly, but not significantly, larger than overjet on the final ClinCheck models.10 It is certainly possible that additional refinement aligners could have been used to improve the scores. However, the orthodontist performing the treatment (DC) purposefully decided to take final records immediately after the end of the last aligner (ie, to give no time for occlusion to settle).
The vertical components of the OGS system, including marginal ridges and occlusal contacts, showed the largest differences between predicted treatment outcome and the posttreatment model. For both of these components, the posttreatment models lost 2 points more on average than the respective ClinCheck model. This might be expected if moving teeth with aligners is more difficult in the vertical than the sagittal plane, as previously suggested.2,10,11 For example, Krieger et al.10 showed that there was only a 14.3% concordance in overbite between the predicted and actual treatment results. This would also explain why Kravitz et al.2 reported that the predicted treatment results were less accurate when teeth were being extruded. Future studies need to be performed to determine whether similar differences are produced after treating subjects who have different malocclusions or were treated with different techniques.
On average, the posttreatment models lost twice as many points for alignment than the respective ClinCheck models. This may have been due to the fact that aligner treatments do not typically incorporate the same level of detailing as conventional braces. In other words a full finishing/detailing phase of treatment may be needed to achieve the results indicated in the ClinCheck model.
Most aligner patients are concerned about esthetics and want their malocclusion corrected accordingly. Once the patients' esthetic expectations are attained, they are usually satisfied with treatment.12 Any extra time that may be necessary for detailing is offset by the fact that aligner therapy is more efficient than conventional treatment and involves shorter treatment times and fewer visits.13
Importantly, the actual treatment outcomes attained with aligner therapy compared well with those attained with conventional treatments. The overall OGS scores for the present study were similar to or lower than most overall scores previously reported (Table 2). Variability clearly exists in orthodontic treatment outcomes, and not all cases are completed to the exact same specifications. Buccolingual inclinations show the greatest variability across studies, followed closely by alignment, occlusal contacts, and marginal ridges. Most importantly, the components exhibiting the greatest discrepancies for aligners (eg, alignment, marginal ridges, and occlusal contacts) have also proven to be problematic for conventional therapies.
Table 2.
Mean Points Lost for American Board of Orthodontics Objective Grading System Scores for the Clincheck Models and Actual Posttreatment Models Compared with Previously Reported Research Results, Along with the Sum of the First Six Components (Minus Interproximal Contacts) and All Seven Componentsa

Even though one component of the OGS was not measured, the average actual posttreatment model scores fell at the high end of the acceptable range of the ABO's OGS. Although other factors are also usually considered, a case must have 27 or fewer deductions to pass the cast/radiograph portion of the exam.9 Therefore, the aligner cases receiving an average of 24 deductions may be clinically acceptable to both patients and orthodontists. The effects of settling must also be considered because the OGS scores in the present study might be expected to improve over time. Areas of occlusal contact and near contact typically increase during retention, especially during the first few months.24–26 The settling that occurs after the last aligner might be expected to be greater than the settling that occurs at the end of braces because the thickness of the aligner material causes posterior open bite. It should take a few weeks for the posterior occlusal contacts to be fully restored.
The fact that digital rather than plaster models were used in the present study should not be considered a limitation. First, both the actual and the ClinCheck models were digital, so any potential problem with inaccuracies would apply to both. More importantly, scanned 3D models have previously been shown to be as accurate and reliable as plaster models.5–8 With respect to the digital ClinCheck models, Krieger et al.10 showed that they were accurate to within 0.08 mm for overjet and 0.1 mm for overbite.
CONCLUSIONS
Within the limits of this study, it can be concluded that:
ClinCheck models do not accurately reflect the patients' final occlusion immediately at the end of active treatment.
Compared with the patients' models taken immediately after treatment, the ClinCheck models overestimated alignment, buccolingual inclinations, occlusal contacts, and occlusal relations.
ACKNOWLEDGMENTS
This research was partially funded by Align Technology, Inc, San Jose, CA, USA.
REFERENCES
- 1.Align Technology, Inc. The Invisalign Reference Guide. Santa Clara, CA: Align Technology, Inc; 2002. [Google Scholar]
- 2.Kravitz ND, Kusnoto B, BeGole E, Obrez A, Agran B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am J Orthod Dentofacial Orthop. 2009;135:27–35. doi: 10.1016/j.ajodo.2007.05.018. [DOI] [PubMed] [Google Scholar]
- 3.Krieger E, Seiferth J, Marinello I, Jung BA, Wriedt S, Jacobs C, Wehrbein H. Invisalign® treatment in the anterior region: were the predicted tooth movements achieved? J Orofac Orthop. 2012;73:365–376. doi: 10.1007/s00056-012-0097-9. [DOI] [PubMed] [Google Scholar]
- 4.Casko JS, Vaden JL, Kokich VG, et al. Objective grading system for dental casts and panoramic radiographs. American Board of Orthodontics. Am J Orthod Dentofacial Orthop. 1998;114:589–599. doi: 10.1016/s0889-5406(98)70179-9. [DOI] [PubMed] [Google Scholar]
- 5.Keating AP, Knox J, Bibb R, Zhurov AI. A comparison of plaster, digital and reconstructed study model accuracy. J Orthod. 2008;35:191–201. doi: 10.1179/146531207225022626. [DOI] [PubMed] [Google Scholar]
- 6.Kusnoto B, Evans CA. Reliability of a 3D surface laser scanner for orthodontic applications. Am J Orthod Dentofacial Orthop. 2002;122:342–348. doi: 10.1067/mod.2002.128219. [DOI] [PubMed] [Google Scholar]
- 7.Quimby ML, Vig KW, Rashid RG, Firestone AR. The accuracy and reliability of measurements made on computer-based digital models. Angle Orthod. 2004;74:298–303. doi: 10.1043/0003-3219(2004)074<0298:TAAROM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 8.Thiruvenkatachari B, Al-Abdallah M, Akram NC, Sandler J, O'Brien K. Measuring 3-dimensional tooth movement with a 3-dimensional surface laser scanner. Am J Orthod Dentofacial Orthop. 2009;135:480–485. doi: 10.1016/j.ajodo.2007.03.040. [DOI] [PubMed] [Google Scholar]
- 9.The American Board of Orthodontics. Grading System for Dental Casts and Panoramic Radiographs. doi: 10.1016/s0889-5406(98)70179-9. Revised June 2012. http://www.americanboardortho.com/professionals/clinicalexam/casereportpresentation/download.aspx. [DOI] [PubMed] [Google Scholar]
- 10.Krieger E, Seiferth J, Saric I, Jung BA, Wehrbein H. Accuracy of Invisalign® treatments in the anterior tooth region. First results. J Orofac Orthop. 2011;72:141–149. doi: 10.1007/s00056-011-0017-4. [DOI] [PubMed] [Google Scholar]
- 11.Joffe L. Invisalign: early experiences. J Orthod. 2003;30:348–352. doi: 10.1093/ortho/30.4.348. [DOI] [PubMed] [Google Scholar]
- 12.Schabel BJ, McNamara JA, Baccetti T, Franchi L, Jamieson SA. The relationship between posttreatment smile esthetics and the ABO Objective Grading System. Angle Orthod. 2008;78:579–584. doi: 10.2319/0003-3219(2008)078[0579:TRBPSE]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.Buschang PH, Shaw SG, Ross M, Crosby D, Campbell PM. Comparative time efficiency of aligner therapy and conventional edgewise braces. Angle Orthod. 2014;84:391–396. doi: 10.2319/062113-466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Abei Y, Nelson S, Amberman BD, Hans MG. Comparing orthodontic treatment outcome between orthodontists and general dentists with the ABO index. Am J Orthod Dentofacial Orthop. 2004;126:544–548. doi: 10.1016/j.ajodo.2003.11.020. [DOI] [PubMed] [Google Scholar]
- 15.Cook DR, Harris EF, Vaden JL. Comparison of university and private-practice orthodontic treatment outcomes with the American Board of Orthodontics objective grading system. Am J Orthod Dentofacial Orthop. 2005;127:707–712. doi: 10.1016/j.ajodo.2004.12.014. [DOI] [PubMed] [Google Scholar]
- 16.Cook MK. Evaluation of Boardcertified Orthodonist's Sequential Finished Cases with the ABO Objective Grading System Orthodontics. St Louis, Mo: St Louis University; 2003. [Google Scholar]
- 17.Costalos PA, Sarraf K, Cangialosi TJ, Efstratiadis S. Evaluation of the accuracy of digital model analysis for the American Board of Orthodontics objective grading system for dental casts. Am J Orthod Dentofacial Orthop. 2005;128:624–629. doi: 10.1016/j.ajodo.2004.08.017. [DOI] [PubMed] [Google Scholar]
- 18.Deguchi T, Honjo T, Fukunaga T, Miyawaki S, Roberts WE, Takano-Yamamoto T. Clinical assessment of orthodontic outcomes with the peer assessment rating, discrepancy index, objective grading system, and comprehensive clinical assessment. Am J Orthod Dentofacial Orthop. 2005;127:434–443. doi: 10.1016/j.ajodo.2004.03.030. [DOI] [PubMed] [Google Scholar]
- 19.Djeu G, Shelton C, Maganzini A. Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American Board of Orthodontics objective grading system. Am J Orthod Dentofacial Orthop. 2005;128:292–298. doi: 10.1016/j.ajodo.2005.06.002. [DOI] [PubMed] [Google Scholar]
- 20.Nett BC, Huang GJ. Long-term posttreatment changes measured by the American Board of Orthodontics objective grading system. Am J Orthod Dentofacial Orthop. 2005;127:444–450. doi: 10.1016/j.ajodo.2004.03.029. [DOI] [PubMed] [Google Scholar]
- 21.Yang-Powers LC, Sadowsky C, Rosenstein S, BeGole EA. Treatment outcome in a graduate orthodontic clinic using the American Board of Orthodontics grading system. Am J Orthod Dentofacial Orthop. 2002;122:451–455. doi: 10.1067/mod.2002.128464. [DOI] [PubMed] [Google Scholar]
- 22.Knierim K, Roberts WE, Hartsfield J., Jr Assessing treatment outcomes for a graduate orthodontic program: follow-up study for the classes of 2001–2003. Am J Orthod Dentofacial Orthop. 2006;130:648–655. doi: 10.1016/j.ajodo.2006.07.014. [DOI] [PubMed] [Google Scholar]
- 23.Wes Fleming J, Buschang PH, Kim KB, Oliver DR. Posttreatment occlusal variability among angle Class I nonextraction patients. Angle Orthod. 2008;78:625–630. doi: 10.2319/0003-3219(2008)078[0625:POVAAC]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 24.Gazit E, Lieberman MA. Occlusal contacts following orthodontic treatment. Measured by a photocclusion technique. Angle Orthod. 1985;55:316–320. doi: 10.1043/0003-3219(1985)055<0316:OCFOT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 25.Dicer M, Meral O, Tumer N. The investigation of occlusal contacts during the retention period. Angle Orthod. 2003;73:640–646. doi: 10.1043/0003-3219(2003)073<0640:TIOOCD>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 26.Horton JK, Buschang PH, Oliver DR, Behrents RG. Comparison of the effects of Hawley and perfector/spring aligner retainers on postorthodontic occlusion. Am J Orthod Dentofacial Orthop. 2009;135:729–736. doi: 10.1016/j.ajodo.2007.05.022. [DOI] [PubMed] [Google Scholar]