

Abstract
Background:
Use of smartphone is on the increase worldwide. They have revolutionized our lives to an extent that was unimaginable before the pandemic. Excessive use of smartphones reaching the levels of potential addiction among medical students and its relation to individual's sleep quality and self-esteem led us to study this prevalence.
Aim:
This stuay aimed to study the prevalence of smartphone addiction and its relation with self-esteem and sleep disturbance in medical college students.
Materials and Methods:
A cross sectional analytical study was carried out and the prevalence of smartphone addiction, self- esteem, and sleep disturbance was measured using standardized questionnaires smartphone addiction scale short form, Rosenberg self esteem scale, Pittsburgh sleep quality index assessment respectively.
Results:
Prevalence of smartphone addiction among medical college students was 52%. Smartphone addiction was seen more in boys than girls. There was a significant association between the smartphone addiction and sleep disturbance. However, there was no significant association between smartphone addiction and low self-esteem.
Conclusion:
The prevalence of smartphone addiction among medical students is found to be high and is associated with poor sleep.
Keywords: Medical students, self-esteem, sleep, smartphone
Smartphones and the easy accessibility of the Internet they provide have revolutionized our lives immensely. Individuals now can communicate with others using multiple apps and stay up to date with the ever-increasing information through search engines. Given the multifaceted applications of a smartphone, it has become an intrinsic part of our lives. Nearly over 300 million of the Indian population uses smartphone.[1] Technology can be both bane and boon for human beings. Despite the technological advantage these devices offer, the growing evidence suggests that the use of smartphone has increased to a problematic use level where this use has a debilitating effect on physical and mental health.
The problematic use of smartphone has taken the form of behavioral addiction where this smartphone addiction can be defined using traditional criteria for behavioral addictions. In general, smartphone addiction consists of four main components: compulsive phone use, behaviors such as repeated checking for messages or updates; tolerance, longer, and more intense bouts of use; withdrawal, feelings of agitation or distress without the phone; and functional impairment, interference with other life activities and face-to-face social relationships.[2] All these are very similar to the characteristics of Internet addiction.[3] As Internet usage is an integral part of smartphone use both Internet addiction and smartphone addiction, most of the time go hand in hand and affect their users mostly simultaneously. There is mounting evidence of smartphone and Internet addiction being significantly associated with many other adverse mental health effects alcohol abuse, depression, and anxiety,[4] poor sleep quality,[5] and impaired quality of life.[6]
Good quality and restorative sleep has been a prime requirement of physical and emotional well-being. There have been many evidences that many physiological processes depend on intact sleep physiology. Researchers have linked Internet and smartphone addiction to poor sleep quality and sleep disturbances.[7] In general, people addicted to smartphones have problems structuring their daily routine things. The same may apply to their sleep habits also. When it comes to students, sleep disturbance may impair their classroom attention as well as poor concentration at studies and hence poor academic outcome.
Self-esteem is another area of interest in relation to young student population. It is well-known fact that peer relationship affects self-esteem in young people[8] and smartphone, especially social networking being a newer mode of communication, may affect self-esteem and self-esteem vice versa may affect smartphone use. This relationship between smartphone addiction and self-esteem has been explored by some researchers in the recent past and has found conflicting results. Some researchers found an association of low self-esteem with smartphone addiction,[9,10] while others found contradictory results.[11,12] This provokes interest in further research.
Recent studies have revealed that the population which is affected by smartphone addiction is mostly young population. Especially, student population has been shown to be affected by smartphone addiction.[13,14] Student population being young, open to new experiences, and techno savvy tends to use smartphones more and also explores its usage more. Hence, they are more vulnerable to fall into the trap of smartphone addiction. Particularly, considering recent COVID-19 pandemic, the changed lifestyle of students such as online classes, homebound environment necessitating the use of social media, and loneliness causing excessive use of smartphone for entertainment and time pass has made students even more vulnerable for smartphone addiction. Hence, we planned this study in medical students to estimate the prevalence of smartphone addiction and its relation with sleep disturbances and self-esteem in medical college students during the COVID-19 pandemic.
MATERIALS AND METHODS
Study setting
This cross-sectional analytical study was carried out from the department of psychiatry of a tertiary care center and medical college in Maharashtra. Permission was obtained from the institutional ethics committee and scientific committee. Written informed consent was obtained from all the participants.
Sample
A total number of 500 medical students were included in the study. The included students were those who have been using smartphones for at least 6 months before the study. The students were recruited by convenience sampling method and recruited students were given to fill-up a semi-structured pro forma consisting of tools given below. Participants were assured that the information given by them would be anonymous and confidential to avoid reporting bias.
Tools
Sociodemographic questionnaire
This was developed by the investigators based on the literature to collect sociodemographic data.
Smartphone addiction scale short form
The smartphone addiction scale short form is a 10 item self report scale to evaluate the risk of smartphone addiction among adolescents. Each item is scored on a 6 point Likert scale, with the responses ranging from “I strongly disagree” to “I strongly agree.”[15]
Rosenberg self esteem scale (RSES)
The RSES is a 10 item scale measuring global self worth by measuring both positive and negative feelings about the self. All items are answered using a 4 point Likert scale format ranging from strongly agree to strongly disagree.[16]
Pittsburgh sleep quality index assessment (PSQI)
The PSQI is a 9 item self report scale measuring quality and patterns of sleep in adults.[17]
RESULTS
Out of 500 medical students, 260 (52%) were found to have scores corresponding to smartphone addiction. A score of >31 is the cutoff for addiction for men and >33 for women. Those falling between 22 and 32 are at risk of addiction in the smartphone addiction scale.
The age of acquiring a phone was found to be earlier in boys as compared to girls around 13 years of age in boys and 14 in girls. However, the age of acquiring a smartphone was not significantly different in both genders [Table 1].
Table 1.
Comparison of age, age of acquiring phone, and age of using smartphone in boys and girls
| Variables | Mean | SD | t | df | P |
|---|---|---|---|---|---|
| Age | |||||
| Boys | 20.021 | 1.973 | 0.576 | 497 | 0.565 (NS) |
| Girls | 19.919 | 1.889 | |||
| Age of the first phone | |||||
| Boys | 13.742 | 2.126 | −2.859 | 497 | 0.004 (S) |
| Girls | 14.313 | 2.195 | |||
| Age of first smartphone | |||||
| Boys | 15.78 | 1.408 | −1.035 | 497 | 0.301 (NS) |
| Girls | 16.233 | 5.943 |
NS – Not significant; S – Significant; SD – Standard deviation
The usage timing was significantly different in both genders where more girls used their phones during daytime and boys used during nighttime. The mode of Internet access for smartphone was not significantly different between WiFi or data card usage; however, the place where smartphone used significantly more was in hostels than at home [Table 2].
Table 2.
Comparison of characteristics of smartphone use
| Characteristics | Boys | Girls | χ 2 | P |
|---|---|---|---|---|
| Use during | ||||
| Day | 17 | 54 | 7.012 | 0.008 (S) |
| Night | 173 | 255 | ||
| Mode | ||||
| WiFi | 26 | 27 | 3.032 | 0.082 (NS) |
| Data card | 164 | 282 | ||
| Place | ||||
| Residence | 18 | 55 | 6.53 | 0.011 (S) |
| Hostel | 172 | 254 |
NS – Not significant; S – Significant
There was no significant difference of scores on the severity of smartphone addiction (SAS), RSEC, and PSQI when compared between boys and girls [Table 3].
Table 3.
Comparison of smartphone addiction scale, Rosenberg self-esteem scale, and Pittsburgh sleep quality assessment scores between boys and girls
| Mean | SD | Minimum | Maximum | Mann-Whitney U | P | |
|---|---|---|---|---|---|---|
| SAS | ||||||
| Boys | 31.837 | 7.767 | 12.0 | 52.0 | 27,586.500 | 0.258 (NS) |
| Girls | 30.709 | 8.202 | 10.0 | 50.0 | ||
| RSES | ||||||
| Boys | 20.568 | 6.376 | 12.0 | 36.0 | 27,605.500 | 0.262 (NS) |
| Girls | 21.275 | 6.467 | 10.0 | 38.0 | ||
| PSQI | ||||||
| Boys | 4.811 | 3.007 | 0.00 | 12.0 | 28,573.500 | 0.615 (NS) |
| Girls | 4.608 | 2.868 | 0.00 | 18.0 |
NS – Not significant; SD – Standard deviation; PSQI – Pittsburgh sleep quality assessment; RSES – Rosenberg self-esteem scale; SAS – PSQI – Pittsburgh sleep quality assessment; RSES – Rosenberg self-esteem scale; SAS – Smartphone addiction scale
Significantly, more number of boys were affected by smartphone addiction than girls. However, low self-esteem measured by RSES and disturbed sleep measured by PSQI assessment were not significantly different in both genders [Table 4 and Figure 1].
Table 4.
Comparison of number of boys (n=190) and girls (n=309) with smartphone addiction, low self-esteem, and sleep quality
| Variable | Boys, n (%) | Girls, n (%) | χ 2 | P |
|---|---|---|---|---|
| Smartphone addiction | ||||
| Yes | 110 (58) | 147 (47) | 5.02 | 0.025 (S) |
| No | 80 | 162 | ||
| Low self-esteem | ||||
| Yes | 53 (28) | 75 (24) | 0.809 | 0.368 (NS) |
| No | 137 | 234 | ||
| Poor sleep quality | ||||
| Yes | 97 (51) | 164 (53) | 0.193 | 0.661 (NS) |
| No | 93 | 145 |
NS – Not significant; S – Significant
Figure 1.
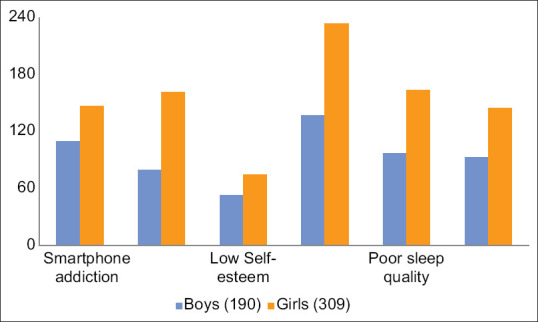
Comparison of smartphone addiction, self-esteem, and sleep quality among undergraduate medical students
Medical students who are addicted to smartphones had significantly more sleep disturbances as compared to those without addiction. Low self-esteem was not found to be associated with smartphone addiction [Table 5].
Table 5.
Prevalence of low self-esteem and sleep disturbance in medical undergraduates with and without smartphone addiction
| Variables | Medical undergraduates, addiction (n=260) | χ 2 | P | |
|---|---|---|---|---|
|
| ||||
| With smartphone | Without smartphone | |||
| Low self-esteem | 82 (31.54) | 68 (28.33) | 0.611 | 0.435 (NS) |
| Sleep disturbance | 180 (69.23) | 70 (29.17) | 80.128 | <0.00001 (S) |
NS – Not significant; S – Significant
Spearman's correlation of age of first phone use, age of first smartphone use, SAS score, self-esteem (RSES score), and sleep disturbance (PSQI score) was done. Age of smartphone usage had a positive correlation with smartphone addiction but had a negative correlation with self-esteem or sleep disturbance. Smartphone addiction had a positive correlation with sleep disturbance and a negative correlation with self-esteem [Table 6]. Multiple regression was run to predict smartphone addiction scale scores from age of first using mobile phone, self-esteem, and sleep quality. These variables statistically significantly predicted smartphone addiction scale scores, F (3, 496) =32.393, P < 0.0005, R2 = 0.577. All four variables added statistically significantly to the prediction, P < 0.05 [Table 7].
Table 6.
Spearman’s correlations between smartphone addiction, self-esteem, and sleep quality
| Age of first phone | Age of first smartphone | SAS | RSES | PSQI | |
|---|---|---|---|---|---|
| Age of first phone | |||||
| Correlation coefficient | 1.000 | 0.644** | 0.098* | −0.084 | −0.005 |
| Significant (two tailed) | 0.000 | 0.028 | 0.059 | 0.912 | |
| Age of first smartphone | |||||
| Correlation coefficient | 0.644** | 1.000 | 0.109* | −0.005 | 0.048 |
| Significant (two tailed) | 0.000 | 0.015 | 0.905 | 0.286 | |
| SAS | |||||
| Correlation coefficient | 0.098* | 0.109* | 1.000 | −0.251** | 0.388** |
| Significant (two tailed) | 0.028 | 0.015 | 0.000 | 0.000 | |
| RSES | |||||
| Correlation coefficient | −0.084 | −0.005 | −0.251** | 1.000 | −0.294** |
| Significant (two tailed) | 0.059 | 0.905 | 0.000 | 0.000 | |
| PSQI | |||||
| Correlation coefficient | −0.005 | 0.048 | 0.388** | −0.294** | 1.000 |
| Significant (two tailed) | 0.912 | 0.286 | 0.000 | 0.000 |
*Significant, **Highly significant. PSQI – Pittsburgh sleep quality assessment; RSES – Rosenberg self-esteem scale; SAS – Smartphone addiction scale
Table 7.
Multiple regression analysis to identify the predictors of smartphone addiction: Coefficientsa
| Model | Unstandardized coefficients | Standardized coefficients | t | Significance | 95.0% CI for B | Collinearity statistics | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | Beta | Lower bound | Upper bound | Tolerance | VIF | ||||
| 3 | ||||||||||
| Constant | 26.649 | 2.668 | 9.987 | 0.000 | 21.406 | 31.892 | ||||
| PSQI | 0.928 | 0.118 | 0.337 | 7.881 | 0.000 | 0.697 | 1.160 | 0.909 | 1.100 | |
| RESTEEM | −0.197 | 0.054 | −0.157 | −3.664 | 0.000 | −0.302 | −0.091 | 0.903 | 1.107 | |
| AgeM | 0.303 | 0.151 | 0.082 | 2.007 | 0.045 | 0.006 | 0.599 | 0.991 | 1.009 | |
aDependent variable: SAS. SAS – Smartphone Addiction Scale; SE – Standard error; CI – Confidence interval; PSQI – Pittsburgh sleep quality assessment; RESTEEM – Rosenberg Self exteem scale; VIF – Variance Inflation Factor
DISCUSSION
Over the last decade use of smartphones has increased drastically especially in young population. Particularly, the COVID pandemic scenario has changed smartphone use in students to necessity as education has shifted to online mode. However, use of smartphones in student population has shifted to problematic use or addiction and causing mental health issues in them. The present study has found a quite high prevalence of smartphone addiction in medical students. In our study, 52% of medical students were addicted to smartphones. This proportion of addicted students is higher compared to other Indian studies in medical students in past which showed a prevalence of 46.15%[18] and 34.4%.[19] This shows the increasing trend of smartphone use and its addiction. Another possible explanation can be due to COVID-19 pandemic everyone has become homebound and lonely. Hence, they are increasingly using smartphones for communication as well as entertainment. Even all learning has become online necessitating increased use of smartphones. This altered way of living in COVID-19 pandemic has probably made students more vulnerable for smartphone addiction.
The age of acquiring a phone was significantly earlier in boys as compared to girls in our study. However, age of acquiring smartphone was similar in both genders. This probably signifies the essential nature the smartphone acquired in recent years. We also found a significant difference in the time of smartphone use between boys and girls. Girls used phones maximum during daytime, while boys used phones mostly at night. This may reflect the predominant purpose for which girls and boys use their smartphones. Girls have been found to use smartphones for social networking more than boys and boys use smartphones more for gaming compared to girls.[20] We also found that students used smartphones more in hostels as compared to homes. This is understandable as most of our students stayed in hostels.
When compared for gender disparity, smartphone addiction was significantly higher in boys as compared to girls. This correlates well with other studies that have similar trends for gender-based disparity in smartphone addiction.[21,22,23] The reason for such a disparity may be the presence of more usage of smartphone for gaming in boys as compared to girls which takes more time as well as concentration to stay glued to the screen for a longer period of time.
When students addicted to smartphone were compared to students not addicted, we found that students addicted to smartphones had significantly more sleep disturbances as measured on PSQI assessment scale. Sleep disturbance is quite likely when a person is spending more time on smartphones as many of them are using it in nighttime, emotional and exciting content they go through on smartphone may disturb calmness of mind causing sleep disturbance as well as light of screen of smartphone may also cause sleep disturbance. Many researchers have elaborated on this association of disturbed sleep with smartphone addiction in past.[24,25] We also tried to elaborate relation of self-esteem with smartphone addiction. However, low self-esteem as measured by RSES was not significantly associated with smartphone-addicted students. In the past, there have been conflicting results of studies regarding association of low self-esteem with phone addiction. There have been studies supporting the association[9,10] and also there have been studies refuting the association.[11,12] Smartphone use can have both positive and negative effects on person's self-esteem depending on different mediating factors including personality and other emotional factors which may be a topic for further exploration.
However, when Spearman's correlation was done for smartphone addiction with other factors of interest, we found SAS had a significant positive correlation with age of first smartphone usage and sleep disturbances and negative correlation with self-esteem scores. Age of first smartphone use is likely to affect a person's probability of having smartphone addiction and it has been corroborated in previous studies that longer duration of smartphone use has been associated with higher chances of smartphone addiction.[26] Impaired sleep quality is also logical in severely addicted people as discussed above. The Association of low self-esteem with more severe smartphone addiction has been congruent to some previous researches.[9,10] Many researchers believe that Internet and smartphone use would provide an alternate way for individuals for communicating who are less confident and shy, and thus, people with low self-esteem would spend more time on these gadgets. The predictors of smartphone addiction in our study are in agreement with previous studies.[9,25]
Limitations
The limitation of this study has been its modest sample size and sample population is from a single medical college.
CONCLUSION
The prevalence of smartphone addiction among medical students is found to be high and is associated with disturbed sleep pattern and is negatively associated with low self-esteem.
Future scope
Future scope of the study was to counsel and take steps in reduction of excessive usage of cell phones to essential use and reduce any interference in academic performance, sleep, and self-esteem.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Iyengar R. India Poised for Smartphone Revolution. [Last accessed on 2017 Sep 28]. Available from: https://money.cnn.com/2017/09/26/technology/indiamobile-congress-market-numbers/index.html .
- 2.Lin YH, Chiang CL, Lin PH, Chang LR, Ko CH, Lee YH, et al. Proposed diagnostic criteria for Smartphone addiction. PLoS One. 2016;11:e0163010. doi: 10.1371/journal.pone.0163010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Block JJ. Issues for DSM-V: Internet addiction. Am J Psychiatry. 2008;165:306–7. doi: 10.1176/appi.ajp.2007.07101556. [DOI] [PubMed] [Google Scholar]
- 4.Matar Boumosleh J, Jaalouk D. Depression, anxiety, and smartphone addiction in university students – A cross sectional study. PLoS One. 2017;12:e0182239. doi: 10.1371/journal.pone.0182239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Zhang MW, Tran BX, Huong LT, Hinh ND, Nguyen HL, Tho TD, et al. Internet addiction and sleep quality among Vietnamese youths. Asian J Psychiatr. 2017;28:15–20. doi: 10.1016/j.ajp.2017.03.025. [DOI] [PubMed] [Google Scholar]
- 6.Tran BX, Huong LT, Hinh ND, Nguyen LH, Le BN, Nong VM, et al. A study on the influence of internet addiction and online interpersonal influences on health-related quality of life in young Vietnamese. BMC Public Health. 2017;17:138. doi: 10.1186/s12889-016-3983-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Yogesh S, Abha S, Priyanka S. Mobile usage and sleep patterns among medical students. Indian J Physiol Pharmacol. 2014;58:100–3. [PubMed] [Google Scholar]
- 8.Rosenberg M. Society and the Adolescent Self-Image. Vol. 11. Princeton, NJ: Princeton University Press; 1965. p. 326. [Google Scholar]
- 9.Walsh SP, White KM, Cox S, Young RM. Keeping in constant touch: The predictors of young Australians' mobile phone involvement. Comput Human Behav. 2011;27:333–42. [Google Scholar]
- 10.Ha JH, Chin B, Park DH, Ryu SH, Yu J. Characteristics of excessive cellular phone use in Korean adolescents. Cyberpsychol Behav. 2008;11:783–4. doi: 10.1089/cpb.2008.0096. [DOI] [PubMed] [Google Scholar]
- 11.Butt S, Phillips JG. Personality and self-reported mobile phone use. Comput Human Behav. 2008;24:346–60. [Google Scholar]
- 12.Ehrenberg A, Juckes S, White KM, Walsh SP. Personality and self-esteem as predictors of young people's technology use. Cyberpsychol Behav. 2008;11:739–41. doi: 10.1089/cpb.2008.0030. [DOI] [PubMed] [Google Scholar]
- 13.Basu S, Garg S, Singh MM, Kohli C. Addiction-like behavior associated with mobile phone usage among medical students in Delhi. Indian J Psychol Med. 2018;40:446–51. doi: 10.4103/IJPSYM.IJPSYM_59_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mangot AG, Murthy VS, Kshirsagar SV, Deshmukh AH, Tembe DV. Prevalence and pattern of phantom ringing and phantom vibration among medical interns and their relationship with smartphone use and perceived stress. Indian J Psychol Med. 2018;40:440–5. doi: 10.4103/IJPSYM.IJPSYM_141_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kwon M, Kim DJ, Cho H, Yang S. The Smartphone Addiction Scale: Development and validation of a short version for adolescents. PLoS One. 2013;8:e83558. doi: 10.1371/journal.pone.0083558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Rosenberg M. Society and the Adolescent Self-Image. Princeton, NJ: Princeton University Press; 1985. [Google Scholar]
- 17.Buysse DJ, Reynolds CF, 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi: 10.1016/0165-1781(89)90047-4. [DOI] [PubMed] [Google Scholar]
- 18.Dharmadhikari SP, Harshe SD, Bhide PP. Prevalence and correlates of excessive smartphone use among medical students: A cross-sectional study. Indian J Psychol Med. 2019;41:549–55. doi: 10.4103/IJPSYM.IJPSYM_75_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Nowreen N, Ahad F. Effect of smartphone usage on quality of sleep in medical students. Natl J Physiol Pharm Pharmacol. 2018;8:1366–70. [Google Scholar]
- 20.Sama AA. Gender differences in smartphone usage patterns of adolescents. Int J Res Anal Rev. 2020;7:355–62. [Google Scholar]
- 21.Aljomaa SS, AlQudah MF, Albursan IS, Bakhiet SF, Abduljabbar AS. Smartphone addiction among university students in the light of some variables. Comput Human Behav. 2016;61:155–64. [Google Scholar]
- 22.Awasthi S, Kaur A, Solanki HK, Pamei G, Bhatt M. Smartphone use and the quality of life of medical students in the Kumaun Region, Uttarakhand. J Family Med Prim Care. 2020;9:4252–8. doi: 10.4103/jfmpc.jfmpc_805_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chen B, Liu F, Ding S, Ying X, Wang L, Wen Y. Gender differences in factors associated with Smartphone addiction: A cross-sectional study among medical college students. BMC Psychiatry. 2017;17:341. doi: 10.1186/s12888-017-1503-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kumar VA, Chandrasekaran V, Brahadeeswari H. Prevalence of Smartphone addiction and its effects on sleep quality: A cross-sectional study among medical students. Ind Psychiatry J. 2019;28:82–5. doi: 10.4103/ipj.ipj_56_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ozcan B, Acimis NM. Sleep quality in Pamukkale University Students and its relationship with Smartphone addiction. Pak J Med Sci. 2021;37:206–11. doi: 10.12669/pjms.37.1.3130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lee EJ, Kim HS. Gender differences in smartphone addiction behaviors associated with parent-child bonding, parent-child communication, and parental mediation among Korean elementary school students. J Addict Nurs. 2018;29:244–54. doi: 10.1097/JAN.0000000000000254. [DOI] [PubMed] [Google Scholar]