

Abstract
Objective:
To investigate whether text message reminders regarding oral hygiene have an effect on plaque removal in orthodontic patients.
Materials and Methods:
In this randomized, controlled clinical trial, 50 orthodontic patients were assigned to either a text message or control group. Patients in the text message group received 12 text messages over the course of 4 weeks and one text message for 8 weeks thereafter. Photos were taken at baseline (T0), at 4 weeks after baseline (T1), and at 12 weeks after baseline (T2). For each subject, photos of eight teeth were taken and then the area of the tooth and amount of plaque were measured using planimetry.
Results:
There was a statistically significant difference in plaque coverage between baseline and both T1 and T2 in the text message group as measured using planimetry. This was demonstrated by comparing the average measurements of the control group and the treatment group.
Conclusion:
This study demonstrated that the use of automated text message reminders sent from an orthodontic office was effective in improving oral hygiene compliance in orthodontic patients.
Keywords: Oral hygiene, Plaque, Text message, Planimetry
INTRODUCTION
Poor oral hygiene can have a negative effect on orthodontic treatment outcomes.1 Gingival inflammation can lead to detrimental effects to the periodontium, including recession, hyperplasia, and subsequent periodontal disease.2–10 Poor oral hygiene has been shown to affect the quality of orthodontic treatment and can prolong treatment times.1,2 Orthodontic treatment with fixed appliances leads to an increased risk of enamel demineralization that is exacerbated in patients with poor oral hygiene.3 Effective plaque removal and oral hygiene compliance have been important concerns for orthodontists. A significant percentage of orthodontic patients experience hygiene challenges, and many demonstrate adverse effects from poor hygiene during treatment. It is well known that oral hygiene compliance can be challenging with the orthodontic treatment population.11–15 There have been numerous studies that looked at hygiene compliance. Rinchuse et al.16 studied the influences of objective feedback and instructions on the oral hygiene of orthodontic patients over an 8-month period and found no effect. An oral health promotion program for patients undergoing fixed appliance orthodontic treatment produced a short-term reduction (up to 5 months) in plaque and an improvement in gingival health.17
Studies in medicine and dentistry have shown text messaging to be an effective tool for behavioral change and disease prevention.18,19 Text message was also shown to be effective in increasing smoking abstinence rates among adolescents and young adults.20 A 2009 systematic review of text message influence on behavior demonstrated positive changes in 13 of the 14 studies meeting the authors' criteria, including smoking cessation, diabetes self-management, and anti-obesity.21 This kind of communication delivered by text messaging is becoming increasingly common.22 With the introduction of text messaging, it has become very easy to communicate with the patient. Text messaging is used to improve attendance in the medical office setting.23 Many patients now prefer text messaging for appointment reminders. The younger generation has embraced this new technology, and the growth of text messaging with teenagers and preteens has increased significantly over the past few years. About 75% of 12- to 17-year-olds in the United States own cell phones, and 75% of these teens send text messages, according to the Pew Research Center's Pew 2010 Internet and American Life Project.24
Text messages sent from the orthodontic office following the initial appliance placement resulted in a lower level of self-reported pain.25 Another study showed that text message reminders to parents of orthodontic patients were shown to be an effective way to improve oral hygiene in these patients.26
The increase of ownership of mobile phones along with the popularity of text messaging as a preferred means of communication ensures comprehensive access to target groups.27 With the introduction of text messaging, it has become easier to communicate with the patient. The aim of this study was to determine if there is a difference in oral hygiene between patients who receive direct text messages and those who do not.
MATERIALS AND METHODS
This research protocol was approved by the Seton Hill University Institutional Review Board. This randomized controlled trial was conducted on a convenience sample of 50 consecutively treated patients at the Seton Hill University Center for Orthodontics, Greensburg, Pennsylvania, between June 2013 and June 2014. Guidelines as described by CONSORT 201028 were followed to enhance the study design and reporting. Inclusion criteria were patients between the ages of 10 and 18 years, access to a cellular telephone, orthodontic treatment with fixed maxillary edgewise appliances, and at least 6 months of remaining orthodontic treatment. The text message group was composed of 15 girls and 10 boys with a mean age of 15.5 years, while the control group included 14 girls and 11 boys with a mean age of 14.6 years. The power analysis showed that our sample size was sufficient enough to achieve a power of 80% and maintain a type I alpha risk of .05.
Subject group assignment was done by preassigning the first 20 subjects to either the text message or control group. The first group received one of several standardized text messages, while the control group did not receive any text messages. Subjects were blinded as to group status and were not made aware that text messages were part of the study. Subsequent study participants were then matched or randomized using a minimization strategy, as described by Pandis.29 Minimization is a randomization method that ensures balance of important prognostic factors between treatment groups without the disadvantages of stratification. This method is considered to be a dynamic method, since the randomization list is not produced before the trial starts but during participant recruitment.29 We used two prognostic factors to assign patients: age (<13 or >13 years) and sex (male or female).
At the initial appointment, subjects were disclosed for plaque using Trace Disclosing Solution. This was followed by photographs of four maxillary and four mandibular teeth in both groups. Plaque was analyzed and recorded with planimetry. Planimetry is a more objective way to measure plaque coverage on a tooth. Planimetry-based scales for measurement of plaque accumulations use digital analysis software. This has been shown in previous studies to be a reproducible, valid, and objective way to analyze in vivo plaque levels.30,31 All photographs were taken using a Canon Power Shot G5 with a 58-mm macro lens, with a Canon ring flash. Photographs were taken as close to perpendicular as possible for each tooth that was being assessed. In an attempt to protect against individual variations of left versus right handedness, maxillary and mandibular arches, and anterior and posterior differences, maxillary lateral incisors, maxillary first premolars, mandibular first premolars, and mandibular canines were analyzed. According to Gorelick et al.,32 the highest incidence of white spot lesions was found at the labiogingival area of the maxillary lateral incisors and the lowest incidence was in the maxillary posterior segment. For this reason, the maxillary lateral incisors and maxillary first premolars were chosen for this study.
Both groups watched an audiovisual presentation on how to properly brush with a conventional toothbrush, using the Bass technique. The treatment group received automated text messages two to three times a week for 4 weeks (totaling 12 texts) as a reminder and encouragement to practice good oral hygiene. These messages addressed the importance of oral hygiene and served as a reminder and encouragement to “brush your teeth” (see Table 1). The text message was limited to 160 characters due to maximum content capacity as set by most cellular companies. The House Calls automated messaging system from Televox was used to send the text messages. The control group received no text messages. After the 4-week period, both groups were reevaluated and intraoral photos were retaken to evaluate plaque. Following the first time point, the text group received a text once a week for 8 weeks. After this second time period, both groups were reevaluated again. Plaque measurements at week 4 and week 12 were taken and compared with baseline values. Digimizer image analysis software (www.digimizer.com) was used to analyze the photographs (see Figure 1). Planimetry-based assessment of plaque used Digimizer software. The Digimizer software system uses pixels of the picture uploaded on the computer and determines the square area in pixels squares. Baseline plaque was recorded and determined as a percentage of the overall facial area of the tooth. These values obtained from the teeth were averaged, and a baseline plaque value was established. Plaque was analyzed the same way for T0, T1, and T2. Statistical analysis was applied to the data to determine if there were any clinical significance.
Table 1.
Text Message Examples

Figure 1.
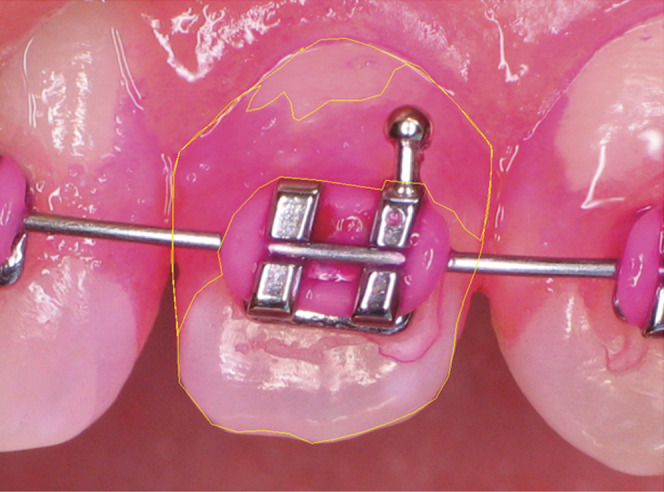
Photograph of disclosed tooth image showing the outline of areas analyzed using the Digimizer software program.
RESULTS
All data were analyzed using SPSS v.21. Summary statistics (means, standard deviations, and frequency) were used to compare the treatment group and the control group. Plaque coverage was analyzed as 2 × 3R analysis of variance (ANOVA). A Bonferroni post hoc analysis was used to analyze the interaction between treatment and time.
There were 55 patients who matched the inclusion/exclusion criteria, and 50 patients consented to participate in the study. Twenty subjects were randomly assigned to the text message or control group. Forty subjects completed all study measurements, as two subjects from the control group and three subjects from the text group did not complete T2 measurements. Overall, there were 24 girls and 16 boys, with a mean age of evaluation of 15.1 years.
Interjudge reliability showed a .952 correlation for tooth size analysis and .972 for plaque analysis (see Table 2). We took the difference in plaque coverage percentages and formulated the means values for the eight teeth in each subject. The mean values of plaque differences between the text group and control group are shown in Table 3. Tests for the main effects of treatment group revealed that there were statistically significant differences between the text messaging and control groups (F = 41.74; df 1, 38; P = .0004), The text group also showed a mean reduction in plaque coverage when compared with the control group when using time as a comparable factor (F = 7.45; df 2, 76; P = .0001). The main effects of time cannot be interpreted directly because there was also a statistically significant interaction between treatment and time.
Table 2.
Paired Sample Correlations for Intrarater Reliabilitya

Table 3.
Mean Values of Plaque Coverage at T0, T1, and T2

A Bonferroni post hoc analysis looking at the interaction between treatment and time revealed that the text group had a statistically significant reduction in plaque when compared with the control group. At T0, these values were statistically the same (experiment = .364 and control = .431). At T1 and T2, these differences were statistically significant. They showed that the text message group had a significant reduction of plaque at T1 and T2 when compared with baseline (T0). The mean differences were significant at the P < .05 level (see Table 4). These values are plotted in Figure 2.
Table 4.
Bonferroni Post Hoc Analysis of Mean Plaque Coverage of Experimental and Control Groups at T0, T1, and T2 (Measure: Plaque Cover)

Figure 2.
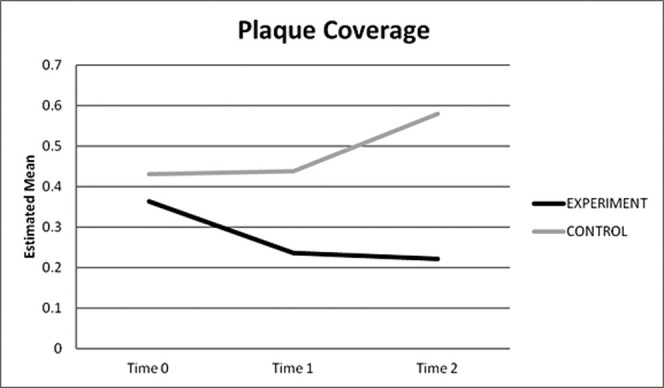
Treatment response for plaque coverage.
DISCUSSION
To our knowledge, this is the first clinical trial comparing the effect of a text message reminder directly to patients on their oral hygiene compliance using planimetry as a tool to measure plaque. We found that text messages reminding and encouraging good oral hygiene resulted in a less measurable surface area of plaque over time. This finding is similar to that reported by Eppright et al.,26 who found that sending text messages to the parents was effective for improving oral hygiene compliance in orthodontic patients. Planimetry is a more objective way to measure plaque coverage on a tooth. Measurements of tooth surface area and the plaque coverage area were traced using the Digimizer software. These area measurements had a corresponding numeric value, and the percentage of plaque coverage could be determined. Another advantage of a photograph is that it is a permanent record, can be analyzed at leisure, and can be viewed multiple times. The drawbacks are the increased complexity and longer time required to evaluate measurements.
In our study, the text message group showed a statistically significant improvement over the control group in both time points evaluated. Although this study showed improvement only over a 12-week time period, this type of reminder system may be beneficial for those orthodontic patients who struggle with compliance issues during treatment. The results of this study suggest that a text message reminder improves the amount of plaque removed at a particular time point. It may not necessarily indicate an improvement in oral hygiene compliance. It is possible that oral hygiene improved because of performance bias that could be introduced in this study from the Hawthorne and novelty effects. The Hawthorne effect is a form of reactivity in which subjects improve or modify an aspect of their behavior being experimentally measured simply in response to the fact that they are being studied, not in response to any particular experimental manipulation.33 The novelty effect is the tendency for a subject to want to do better with a newer or better technology because they are intrigued by it, rather than the effect being truly based on the variable being studied. The control group may have declined in their compliance simply because they were not being given any attention. Since this study looked at only a short time span, the question as to whether there would be any long-lasting effect from text messaging requires further investigation.
The use of texting can help in maintaining good communication with patients. This shows that the orthodontist is still involved and concerned about the patient's well-being between long appointment spans. This has been shown to be important in influencing patient satisfaction and promoting orthodontist-patient relationships.34 The power of the spoken word, or in this instance the written word, appears invaluable when it comes to serving as a means of communicating with young orthodontic patients.
In recent years, e-mail has been used by orthodontic offices as either a replacement or adjunct to telephone calls as a means of patient appointment reminders. Given that virtually every cellular telephone has the ability to receive a text message, it would be reasonable to think that this may be the preferred method of communication short of direct contact. Furthermore, the number of individuals owning a cell phone is greater than the number of individuals owning a computer.35 Ease of use and accessibility appear to be the key issues. Some might argue that texting is just for the teenage population, but that is not the case. Comparing individuals from Generation X and Generation Y, reports state that 43% of those in Generation Y are texting daily, while 31% of Generation X has adopted this method of communication.35 Clearly, texting is not just for the youth movement.
Since introducing text confirmations into their patient reminder armamentarium, US communication company Televox has seen effective response rates ranging from 48% to 61%, which, in comparison, was greater than that seen by phone and e-mail message reminders.27 One might expect that the number of individuals using text messaging as a primary means of correspondence will only grow. For now, texting may be characterized as not only the wave of the future but also the present. Direct text messaging of patients began as a way to remind patients of appointments but may now be used to remind them of brushing, elastic wear, wearing retainers, and so forth. Many orthodontists using self-ligating brackets are scheduling their patients at longer appointment intervals of 8, 10, and 12 weeks. The use of automated texts can keep them in communication with patients over these longer intervals. Automated text-messaging programs such as House Calls by Televox, as used in this study, are a novel way to reach many patients with very little administrative time.
CONCLUSION
The sending of text messages directly to orthodontic patients reminding them of the importance of oral hygiene is an effective way to improve plaque removal from teeth over a 3-month period.
REFERENCES
- 1.Beckwith F, Ackerman R, Cobb C, Tira D. An evaluation of factors affecting duration of orthodontic treatment. Am J Orthod Dentofacial Orthop. 1999;115:439–447. doi: 10.1016/s0889-5406(99)70265-9. [DOI] [PubMed] [Google Scholar]
- 2.Skidmore K, Brook K, Thomson W, Harding W. Factors influencing treatment time in orthodontic patients. Am J Orthod Dentofacial Orthop. 2006;129:230–238. doi: 10.1016/j.ajodo.2005.10.003. [DOI] [PubMed] [Google Scholar]
- 3.Derks A, Kuijpers-Jagtman A, Frencken J, Van't Hof M, Katsarose C. Caries preventive measures used in orthodontic practices: An evidence-based decision. Am J Orthod Dentofacial Orthop. 2007;132:165–170. doi: 10.1016/j.ajodo.2005.10.028. [DOI] [PubMed] [Google Scholar]
- 4.Bollen A, Cunha-Cruz J, Bakko D, Huang G, Hugoel P. The effects of orthodontic therapy on periodontal health: a systematic review of controlled evidence. J Am Dent Assoc. 2008;139:413–422. doi: 10.14219/jada.archive.2008.0184. [DOI] [PubMed] [Google Scholar]
- 5.Zachrisson S, Zachrisson B. Gingival condition associated with orthodontic treatment. Angle Orthod. 1972;42:26–34. doi: 10.1043/0003-3219(1972)042<0026:GCAWOT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 6.Alstad S, Zachrisson B. Longitudinal study of periodontal condition associated with orthodontic treatment in adolescents. Am J Orthod Dentofacial Orthop. 1979;76:277–286. doi: 10.1016/0002-9416(79)90024-1. [DOI] [PubMed] [Google Scholar]
- 7.Zachrisson B, Alnaes L. Periodontal condition in orthodontically treated and untreated individuals, I: loss of attachment, gingival pocket depth and clinical crown height. Angle Orthod. 1973;43:402–411. doi: 10.1043/0003-3219(1973)043<0402:PCIOTA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 8.Burket L. Effects of orthodontic treatment on the soft periodontal tissues. Am J Orthod Dentofacial Orthop. 1963;49:660–671. [Google Scholar]
- 9.Atack N, Sandy J, Addy M. Periodontal and microbiological changes associated with the placement of orthodontic appliances: a review. J Periodontol. 1996;67:78–85. doi: 10.1902/jop.1996.67.2.78. [DOI] [PubMed] [Google Scholar]
- 10.Schluger S. Periodontal aspects of orthodontic treatment. JPO J Pract Orthod. 1968;5:111–117. [PubMed] [Google Scholar]
- 11.Lundstrom F, Hamp S, Nyman S. Systematic plaque control in children undergoing long-term orthodontic treatment. Eur J Orthod. 1980;2:27–39. [PubMed] [Google Scholar]
- 12.Feliu J. Long-term benefits of orthodontic treatment on oral hygiene. Am J Orthod. 1982;82:473–477. doi: 10.1016/0002-9416(82)90315-3. [DOI] [PubMed] [Google Scholar]
- 13.Bratthall D. Programmed self-instruction in oral hygiene. J Periodontol Res. 1967;2:207–214. doi: 10.1111/j.1600-0765.1967.tb01891.x. [DOI] [PubMed] [Google Scholar]
- 14.Casey G. Maintenance of oral hygiene and dental health during orthodontic therapy. Clin Prev Dent. 1988;10:11–13. [PubMed] [Google Scholar]
- 15.Boyd R. Enhancing the value of orthodontic treatment: incorporating effective preventive dentistry into treatment. Am J Orthod Dentofacial Orthop. 2007;17:601–603. doi: 10.1016/s0889-5406(00)70214-9. [DOI] [PubMed] [Google Scholar]
- 16.Rinchuse D, Rinchuse D, Zullo T. Oral hygiene compliance: a clinical investigation. J Clin Orthod. 1992;26:33–38. [PubMed] [Google Scholar]
- 17.Gray D, McIntyre G. Does oral health promotion influence the oral hygiene and gingival health of patients undergoing fixed appliance orthodontic treatment? A systematic literature review. J Orthod. 2008;35:262–269. doi: 10.1179/14653120722770. [DOI] [PubMed] [Google Scholar]
- 18.Fjeldson B, Marshall A, Miller Y. Behavior change interventions delivered by mobile telephone short-message service. Am J Prev Med. 2009;45:184–198. doi: 10.1016/j.amepre.2008.09.040. [DOI] [PubMed] [Google Scholar]
- 19.Cole-Lewis H, Kershaw T. Text messaging as a tool for behavior change in disease prevention and management. Epidemiol Rev. 2010;32:56–69. doi: 10.1093/epirev/mxq004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Haug S, Meyer C, Dymalski A, Lippke S, John U. Efficacy of a text messaging (SMS) based smoking cessation intervention for adolescents and young adults: study protocol of a cluster randomized controlled trial. BMC Public Health. 2012;12:51. doi: 10.1186/1471-2458-12-51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Fjeldsoe B, Marshall, Miller Y. Behavior change interventions delivered by mobile telephone short-message service. Am J Prev Med. 2009;36:165–173. doi: 10.1016/j.amepre.2008.09.040. [DOI] [PubMed] [Google Scholar]
- 22.Porath S. Text messaging and teenagers: a review of the literature. Journal of the Research Center for Educational Technology. 2011;7:86–99. [Google Scholar]
- 23.Geraghty M, Glynn F, Amin M, Kinsella J. Patient mobile telephone “text” reminder: a novel way to reduce non-attendance at the ENT out-patient clinic. J Laryngol Otol. 2007;1:1–3. doi: 10.1017/S0022215107007906. [DOI] [PubMed] [Google Scholar]
- 24.Lenhart A. Teens Cell Phones and Texting Summary of Findings. Washington, DC: Pew Research Center Publications; 2010. [Google Scholar]
- 25.Keith D, Rinchuse D, Kennedy M, Zullo T. Effect of text message follow-up on patient's self-reported level of pain and anxiety. Angle Orthod. 2013;83:605–610. doi: 10.2319/091812-742.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Eppright M, Shroff B, Best A, Barcoma E, Lindauer SJ. Influence of active reminders on oral hygiene compliance in orthodontic patients. Angle Orthod. 2014;84:208–213. doi: 10.2319/062813-481.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Greenhouse DL, Probst JC. After-hours telephone calls in a family practice residency: volume, seriousness, and patient satisfaction. Fam Med. 1995;27:525–530. [PubMed] [Google Scholar]
- 28.Moher D, Hopewell S, Schulz KF, et al. for the CONSORT Group CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomized trial. BMJ. 2010;340:c869. doi: 10.1136/bmj.c869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Pandis N. Randomization. Part 2: minimization. Am J Orthod Dentofacial Orthop. 2011;140:902–904. doi: 10.1016/j.ajodo.2011.08.016. [DOI] [PubMed] [Google Scholar]
- 30.Williams P, Clerehugh V, Worthington HV, Shaw WC. Comparison of a photographic index with a modified clinical plaque index for use with orthodontic fixed appliance patients. J Dent Res. 1991;70:703. [Google Scholar]
- 31.Klukowska M, Bader A, Erbe C, et al. Plaque levels of patients with fixed orthodontic appliances measured by digital plaque image analysis. Am J Orthod Dentofacial Orthop. 2011;139:463–470. doi: 10.1016/j.ajodo.2010.05.019. [DOI] [PubMed] [Google Scholar]
- 32.Gorelick L, Geiger AM, Gwinnett AJ. Incidence of white spot formation after bonding and banding. Am J Orthod Dentofacial Orthop. 1982;81:93–98. doi: 10.1016/0002-9416(82)90032-x. [DOI] [PubMed] [Google Scholar]
- 33.Glantz ST. Primer of Biostatistics 5th ed. New York, NY: McGraw-Hill; 2002. [Google Scholar]
- 34.Sinha P, Nanda R, McNeil D. Perceived orthodontist behaviors that predict patient satisfaction, orthodontist-patient relationship, and patient adherence in orthodontic treatment. Am J Orthod Dentofacial Orthop. 1996;110:370–377. doi: 10.1016/s0889-5406(96)70037-9. [DOI] [PubMed] [Google Scholar]
- 35.Hamilton JY. Orthodontists shd B txN Patients. The Progressive Orthodontist. 2011;Q2:42–44. [Google Scholar]