

Supplemental digital content is available in the text.
Key Words: crew resource management, teams, training, teamwork, intervention, systematic review, patient safety
Abstract
Objective
The aim of this article was to present an overview of the crew resource management (CRM) literature in healthcare. The first aim was to conduct an umbrella review on CRM literature reviews. The second aim was to conduct a new literature review that aims to address the gaps that were identified through the umbrella review.
Methods
First, we conducted an umbrella review to identify all reviews that have focused on CRM within the healthcare context. This step resulted in 16 literature reviews. Second, we conducted a comprehensive literature review that resulted in 106 articles.
Results
The 16 literature reviews showed a high level of heterogeneity, which resulted in discussing 3 ambiguities: definition, outcome, and information ambiguity. As a result of these ambiguities, a new comprehensive review of the CRM literature was conducted. This review showed that CRM seems to have a positive effect on outcomes at Kirkpatrick’s level 1, 2, and 3. In contrast, whether CRM has a positive effect on level 4 outcomes and how level 4 should be measured remains undetermined. Recommendations on how to implement and embed CRM training into an organization to achieve the desired effects have not been adequately considered.
Conclusions
The extensive nature of this review demonstrates the popularity of CRM in healthcare, but at the same time, it highlights that research tends to be situated within certain settings, focuses on particular outcomes, and has failed to address the full scope of CRM as a team intervention and a management concept.
Healthcare organizations located around the globe are increasingly facing the challenge of providing higher levels of care with the same or even less means.1 The demand for care is growing rapidly because of the increasing life expectancy, number of aging people, comorbidity, and treatment possibilities. At the same time, the supply of care cannot be increased because of government-initiated cost-saving programs that aim to keep healthcare systems affordable and sustainable. As a result, teamwork is seen as a key ingredient in helping healthcare organizations face this environmental dynamism. Several studies support the notion that teamwork is one of the most critical components of a high functioning healthcare system (e.g., the study by Rosen et al2). Similarly, the importance of teamwork was loudly acknowledged within the Institute of Medicine hallmark report “To Err Is Human, Crossing the Quality Chasm,” which evidenced a link between the lack of teamwork and preventable medical errors. In addition, they cited that training in team behavior is essential given its role in reducing medical errors and increasing patient safety.3,4
Consequently, healthcare organizations are using interventions that aim to improve team functioning. In particular, Hughes et al5 (2016) showed in their meta-analysis the high potential that team training programs in healthcare had on a variety of outcomes including patient health. Although there are various teamwork training programs being used within the healthcare industry, crew resource management (CRM) is likely the most well-known and widely applied intervention within healthcare organizations aimed to enhance team functioning and improve patient safety.
Crew resource management is often referred to as a training intervention that covers nontechnical skills such as situational awareness, decision making, teamwork, leadership, coping with stress, and managing fatigue.6 A typical CRM training program comprises a combination of information-based methods (e.g., lectures), demonstration-based methods (e.g., videos), and practice-based methods (e.g., simulation, role playing).7 However, at its core, CRM is a management concept that aims to maximize the use of all available resources (i.e., equipment, time, procedures, and people).8 In addition, CRM is an intervention that addresses all aspects of organizational operations rather than being limited to the introduction of a specific training to achieve a specific outcome. As such, the general aim of CRM interventions is “to provide members with the knowledge, skills, and attitudes needed to respond to highly demanding situations in a competent manner that proactively seeks to minimize the risk of errors.”9 Crew resource management is thus a system-wide approach that seeks to avoid errors, detect errors before they occur, and mitigate the consequences of errors that are not detected in a timely fashion.10
As a result of the theorized promise surrounding CRM initiatives, there is a large and rapidly increasing amount of literature that has evaluated CRM in different (especially high-risk) healthcare settings.11 Most of these studies report a positive effect of CRM at 1 or more levels of Kirkpatrick’s framework for evaluation of interventions: reactions, learning/knowledge, behavior, and organizational outcomes (see Appendix 1, http://links.lww.com/JPS/A376). As a result of the growing body of evidence focused on CRM and its potential, multiple literature reviews have been conducted with the aim to provide an overview of what CRM entails and its impact. For example, in 2014, 2 reviews were published on CRM: a meta-analysis by O’dea et al7 (2014) and a systematic review by Verbeek-van Noord et al12 (2014). O’dea et al7 (2014) found 20 studies that evaluated CRM in the acute healthcare domain. Based on their work, they concluded that CRM has a large effect on knowledge and behavior and a small effect on attitudes.7 However, the evidence for an effect on clinical care outcomes was unsupported in their meta-analysis, as was the long-term impact of the training. In comparison, Verbeek-van Noord et al12 (2014) found 22 studies that evaluated classroom-based CRM training on safety culture in a broad range of healthcare domains. They concluded that results regarding the effect of CRM on safety culture were mostly mixed.12 In addition to this unclear picture of the impact of CRM on safety culture, these 2 studies also provide a vivid example of the reviews that have been conducted in this area—they include studies with a variety in levels of quality, and the impact that CRM has depends on how effectiveness is defined. In addition, it should be emphasized that the conclusions derived from such reviews are not based on the same studies given that the target group and CRM content are often different from one review to another. Of the 42 studies included in these 2 reviews, only 2 were included in both reviews.13,14
This lack of overlap speaks to the high level of heterogeneity of studies that exist within the overall CRM literature. In part, this heterogeneity is caused by differences in the CRM curricula, the healthcare setting, the target group within a healthcare setting, and the methods used to evaluate a given CRM intervention. We are not the first to point out these “issues” within the CRM literature. In a recent literature review, Gross et al11 (2019) pointed out these diversities and concluded that CRM seemed to be an umbrella concept of human factors and safety training.
As such, we echo prior sentiments speaking to the need for a comprehensive and structured overview of the CRM literature to ascertain what is really known about CRM in healthcare, given that this has yet to be addressed. Here, we seek to address this gap as this study aims to synthesize the scientific knowledge on CRM by analyzing the results of all literature reviews conducted on CRM to date. This will hopefully provide us insights regarding the current state of the literature based on prior literature reviews. However, given the discrepancies and gaps in the literature reviews conducted thus far, within the current study, we will also conduct a more comprehensive review of the literature with the intent to provide a more complete picture of research conducted on CRM within healthcare to date and highlight where future research is needed.
This literature review consists of 2 phases. The goal of the first phase is to synthesize the findings from all literature reviews (not only systematic reviews) addressing CRM within healthcare settings. During this phase of our work, we will conduct an umbrella review (e.g., the study by Aromataris et al15) of the CRM literature. The second phase of our work aims to review the CRM literature from 2006 to August 2019 addressing the gaps that were identified through the umbrella review process.
METHODS: PHASE 1: UMBRELLA REVIEW OF CRM LITERATURE REVIEWS
Search Strategy
We searched the following databases to locate literature reviews conducted to date on the topic of CRM: EMBASE, Medline, and Web of Science. The search involved a combination of the key words “CRM” OR “crew resource management” OR “crisis resource management,” in combination with (i.e., AND) “review (see Appendix 2,http://links.lww.com/JPS/A377).” This search strategy resulted in 215 hits. This search was expanded by a manual search in Google Scholar. These hits were subject to a stepwise evaluation process as shown in Figure 1. First, the title and abstract were evaluated by adhering to the inclusion and exclusion criteria (see hereinafter), which narrowed our population down to 32 articles. Two of the authors followed these steps, and in the case of disagreement or doubt, it was proceeded to the next step. Second, this subset of articles was evaluated by looking at the entire texts while using the same criteria. This narrowed the list of reviews down to 14 articles. Two of the authors followed this step, and in the case of disagreement, a third author was included in the discussion to make the final decision. In addition, the author team closely analyzed and summarized the reference list of each article to identify any additional articles that may not have surfaced through the literature search process. This step resulted in 2 additional articles. As a result, in total, our umbrella review consisted of the 16 literature reviews that were selected.
FIGURE 1.
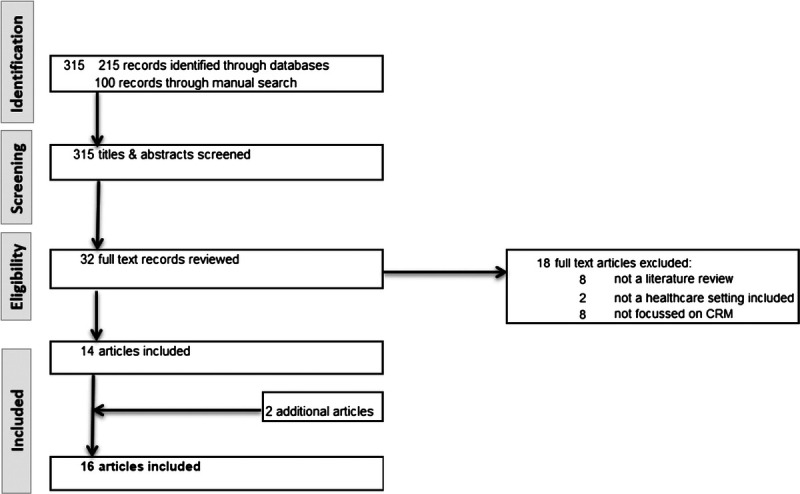
Flow chart phase 1.
Inclusion and Exclusion Criteria
The criteria for inclusion in our study were as follows: the article needed to (1) present a literature review (e.g., systematic, narrative), (2) that was written (or translated) in English, (3) published in a peer-reviewed journal, (4) with a focus on how CRM can improve performance, and (5) focused (at least partly) on CRM in healthcare. We did not weigh the quality of the literature reviews into the inclusion criteria to capture all potentially relevant studies. Likewise, we did not include (nor exclude) articles based on the actual content of the CRM intervention. As such, if the authors of the underlying literature reviews referred to CRM, an inclusion criterion 4 was met. We also included reviews that presented several team interventions that also included CRM, as long as it was clear which articles focused on a CRM intervention and could therefore be extracted. In addition, we did not consider publication year in our decision as to whether to include or to exclude a particular article. Each of these decisions was made in an attempt to ensure that we were able to identify all reviews of the CRM literature within healthcare.
That said, we did apply certain exclusion criteria. Specifically, literature reviews were excluded when (1) no overview of articles was presented as a result of the literature search, (2) the presented articles were not focused on CRM but, for example, on education, and (3) reviews in which articles on CRM in healthcare were not present or represented in an overview of results. Literature reviews that focused on a variety of settings that also included healthcare were included in our umbrella review, but these reviews were selectively summarized and analyzed so as to emphasize the findings relevant to the healthcare context.
Analysis
The 16 literature reviews that were included in our umbrella review are summarized in Table 1. Within this table, we highlight the author, year, title, aim/research question, methods (inclusion and exclusion criteria), setting, number of articles included within the underlying literature review, main result/conclusion, and the quality of the methods using the AMSTAR (A Measurement Tool to Assess Systematic Reviews) tool.29 The AMSTAR consists of 11 items and results in a score ranging from 0 to 11. Based on the 16 literature reviews, 3 categories were constructed, reviews that focused on (1) CRM training in general, (2) simulation training, which is seen as crucial element of CRM, and (3) team training in which CRM is seen as 1 type of team training.
TABLE 1.
Summary of Selected Literature Reviews: Phase 1
| Authors (Year) | Aim/Research Question(s) | Methods: Inclusion and Exclusion Criteria | Setting | Number of Articles | Main Findings | AMSTAR |
|---|---|---|---|---|---|---|
| I. Reviews that focus on CRM | ||||||
| Boet et al16 (2014) | “To gain a better understanding of the impact of simulation-based CRM teaching on transfer of learning to the workplace and subsequent changes in patient outcomes.” | Inclusion criteria: “studies that used simulation-based CRM teaching with outcomes measured at Kirkpatrick level 3 (transfer of learning to the workplace) or 4 (patient outcome).” Exclusion criteria: “studies measuring only learners’ reactions or simple learning (Kirkpatrick level 1 or 2, respectively)”; “papers reporting solely self-assessment data and considered a level 1 (reaction) outcome”; and articles where it’s was not possible to “separate out teaching and/or assessment of technical skills from nontechnical skills in an acute care context.” |
Acute care settings | 9 | “CRM skills learned at the simulation center are transferred to clinical settings, and the acquired CRM skills may translate to improved patient outcomes, including a decrease in mortality.” | 9 |
| Fung et al17 (2015) | “To assess: (i) the effectiveness of simulation-based CRM team training compared to any other educational intervention among interprofessional or interdisciplinary teams and (ii) to determine whether simulation-based CRM team training leads to the modification of attitudes, skill/knowledge acquisition, changes in behaviors, and improved patient outcomes.” | Inclusion criteria: articles with following study characteristics (i.e., randomized controlled trials, quasi-randomized controlled trials, controlled before-after studies, or interrupted time series); patient characteristics (i.e., all healthcare providers and all levels of training); and learning intervention (i.e., interprofessional or Interdisciplinary education, CRM, and simulation-based) | Healthcare | 15 | “CRM simulation-based training for interprofessional and interdisciplinary teams shows promise as a superior training method over traditional nonsimulation clinical teaching of CRM principals.” “All but one of the included interprofessional and interdisciplinary studies found significant improvements in at least one of the learning outcomes when using simulation-based CRM team training compared to alternate forms of training, such as didactic teaching or case-based learning.” “No studies reported outcomes that were worse in the simulation-based CRM training group compared to any comparator group.” |
7 |
| Gross et al11 (2019) | “To identify what is subsumed under the label of CRM in a healthcare context and to determine how such training is delivered and evaluated.” | Inclusion criteria: healthcare staff, individually constructed training formats addressing CRM principles or aviation-derived human factors, studies reporting both the intervention and its effect, published in an academic journal, either in English or German. | Healthcare | 64 | Almost half of the studies “did not explain any key word of their CRM intervention to a reproducible detail. Operating room teams and surgery, emergency medicine, intensive care unit staff and anesthesiology came in contact most with a majority of the CRM interventions delivered in a 1-day or half-day format. Trainer qualification is reported seldomly. Evaluation methods and levels display strong variation.” | 10 |
| Maynard et al18 (2012) | To provide clarity by providing a review of the literature, to highlight the current state of the literature and to identify areas to be addressed by researchers in this field going forward. | A number of search techniques were used. Detailed information on the methods is lacking. | Healthcare | 7 (presented) | CRM and teamwork training programs generally seem beneficial to individual employees, the groups and teams within such settings, and overall healthcare organizations. | 3 |
| O’dea et al7 (2014) | “To determine the aggregate size of the effect of CRM training in acute care settings at four different levels of evaluation: reactions, learning, behavior and clinical care outcomes. Additionally, to identify biases in the research evidence in order to improve the quality of future CRM training interventions in healthcare and also the quality of evaluations of those interventions.” | Inclusion criteria: “studies must report CRM-type training interventions that are focused on improving teamwork within healthcare teams in acute care environments; and training effectiveness must be assessed at least one level of Kirkpatrick’s evaluation hierarchy.” Exclusion criteria: “training that focuses on specific technical skills or procedures rather than on teamwork; and studies that relate to patient or relative centered communication or collaboration, and studies aimed at administrators, leaders or managers.” |
Acute care settings | 20 | “The meta-analysis of CRM-type team training in healthcare found that participants like this type of training.” “There was a large effect of training on knowledge, a small effect of training on attitudes and a large effect of training on behavior.” “The evidence for an effect on clinical care outcomes, or the long-term impact of the training, was unsupported in this meta-analysis.” |
8 |
| O’Connor et al19 (2008) | “To use meta-analyses techniques to evaluate the effectiveness of CRM training.” | Inclusion criteria: “an evaluation had to be reported from at least one of the first three levels of Kirkpatrick’s (1976) evaluation hierarchy: reactions, learning (attitudes and knowledge), or behaviors.” | All settings | 16 (4 HC) |
CRM had a large effect on attitudes and behaviors and a medium effect on their knowledge. | 10 |
| Salas et al20 (2006) | To provide “the state of CRM training evaluations since the Salas et al (2001) review and extends it to areas beyond aviation cockpits.” | Inclusion criteria: articles that present “the findings of a study evaluating the impact of CRM training on trainees’ reactions, learning, or behaviors and/or its impact on the organization.” | All settings | 28 (12 HC) | Although no study was covered “that suggests CRM training does not work, approximately half of the studies indicated mixed results, leading us to question its effectiveness.” | 8 |
| Verbeek-van Noord et al12 (2014) | “To evaluate the evidence of the effectiveness of classroom-based crew resource management training on safety culture (…).” | Inclusion criteria: articles on “training focussed on health-care teams in hospitals and covered at least two CRM topics (e.g., communication and leadership).” Exclusion criteria: “studies evaluating CRM in preclinical medical education, outside healthcare, in primary care, and dental care”; “CRM training courses based (partly) on high-tech simulation techniques”; and “manuscripts based on qualitative research.” |
Hospitals | 22 | “Training settings, study designs, and evaluation methods varied widely.” “Most studies reporting only a selection of culture dimensions found mainly positive results, whereas studies reporting all safety culture dimensions of the particular survey found mixed results.” |
8 |
| Zeltser and Nash21 (2010) | “To report on the body of empirical data about CRM training in clinical settings and to provide a conceptual framework for evaluating its effectiveness in medicine.” | Inclusion criteria: “published in peer-reviewed journals, printed in the English language, published in the past 20 years, and presented original data.” | Clinical settings | 19 | “The purpose of each of the selected studies was to evaluate the effectiveness of a CRM training program for clinical providers.” The authors present “a conceptual framework for evaluating such programs and generating evidence for organizational impact. The framework identified a classification for outcomes measures, which were classified as either learner measures, process measures, or organizational measures.” |
7 |
| II. Reviews that focus on simulation | ||||||
| Doumouras et al22 (2012) | “To appraise and summarize the design, implementation, and efficacy of peer-reviewed, simulation-based CRM training programs for postgraduate trainees (residents).” | Inclusion criteria: “articles that were written in English; were published in peer-reviewed journals; included residents; contained a simulation component; and included a team-based component.” Exclusion criteria: “articles that included staff/fellow physician or medical student training; bore no evaluative component for residents; did not include crisis scenarios; and did not train and evaluate residents in a team environment.” |
Surgery | 15 | “Residents find utility in simulation training and that it can change team-based team behaviors in crisis scenarios.” There is a high degree of satisfaction and perceived value that reflects robust resident engagement. “However, the evidence for translating and measuring the extent of performance from the simulator to the clinical domain remains elusive.” |
7 |
| Murphy et al23 (2015) | “To determine the current state of knowledge about the key components and impacts of multidisciplinary simulation-based resuscitation team training.” | Inclusion criteria: articles that include evaluation of in-hospital resuscitation teams; articles on medical practitioners and allied health staff. Exclusion criteria: articles focused on teams in nonacute settings such as primary care (palliative care, community) or rehabilitation; articles on team performance of end-of-life care; communication tools and clinical handover techniques. |
Emergency department | 11 | The relationship between team training and team performance is supported. “Simulation is an effective method to train resuscitation teams in the management of crisis scenarios and has the potential to improve team performance in the areas of communication, teamwork and leadership.” |
9 |
| Tan et al24 (2014) | To “describe and explore the actual state of multidisciplinary team simulation in surgery.” | Inclusion criteria: “articles that were written or translated to English; published in peer-review journals; contained a simulation component, included surgical trainees/surgeons within a multidisciplinary OT team; and were published during 1990–2012.” Exclusion criteria: articles that “did not train or evaluate multidisciplinary groups in a simulated OT environment (…); assessed only a single professional group (…); included nonsurgeon groups as scripted confederates (…); and assessed only technical skills.” |
Surgery | 26 | “Surgical team simulations are feasible and have received largely positive reactions from participants and some have reported changes to their behavior and interaction within a team environment from this form of learning.” | 6 |
| III. Reviews that focus on team training in general | ||||||
| Buljac-Samardzic et al25 (2010) | “Which types of interventions to improve team effectiveness in healthcare have been researched empirically, for which target groups and for which outcomes? To what extent are these findings evidence based?” | Inclusion criteria: “peer-reviewed English-language publication; a focus on healthcare; a focus on how to improve (and not only measure) team effectiveness; and empirically researched results.” | Healthcare | 48 (15 CRM) | “Three categories of interventions were identified: training, tools, and organizational interventions.” “Studies show that team training can improve the effectiveness of multidisciplinary teams in acute (hospital) care.” Studies that presented high quality evidence were mostly simulation and CRM training. |
7 |
| Low et al26 (2018) | “To describe and evaluate the effects of team-training within intensive care medicine” and “to assess the quality of research and further describe the different team typologies, educational modalities, utilized curricula and the specific skills taught” | Exclusion criteria: “studies focusing on staff from outside the ICU (e.g., staff from emergency departments or medical students), education for individuals (not teams) and studies from non-English journals.” | Intensive care medicine | 27 (12 CRM) | “Team-training has been studied in multiple ICU team types, with CRM and TeamSTEPPS curricula commonly used to support teaching via simulation.” “Team-training in ICU is well received by staff, facilitates clinical learning, and can positively alter staff behaviors.” “Few clinical outcomes have been demonstrated and the duration of the behavioral effects is unclear.” |
8 |
| McCulloch et al27 (2011) | “To identify and evaluate evidence that training of healthcare workers in communication and teamwork improves job performance or patient outcomes.” | Inclusion criteria: randomized and nonrandomized studies; interventions with healthcare workers and healthcare teams. Exclusion criteria: in case “no training intervention was specified; no posttraining evaluation was performed beyond staff attitude and opinion surveys; if it was impossible to define the study population; and in case of lack of numerical data on outcomes.” |
Healthcare | 14 (14 CRM) | “The evidence for technical or clinical benefit from teamwork training in medicine is weak. There is some evidence of benefit from studies with more intensive training programmes (...).” “Most reported improved staff attitudes, and significantly better teamwork after training.” |
10 |
| Weaver et al28 (2014) | “To provide an updated narrative synthesis of the body of evidence evaluating team-training in acute care settings (...).” | Inclusion criteria: articles between January 2000 and December 2012. Exclusion criteria: articles that were “only descriptive in nature; conducted in non-English–speaking populations or if primarily targeting students or trainees.” |
Acute care setting | 26 (9 CRM) |
The “synthesis suggests that there is moderate to high-quality evidence that team-training can positively impact healthcare team processes and, in turn, clinical processes and patient outcomes.” “A key finding is that the studies demonstrating the most robust evidence for effectiveness have implemented team-training as a bundled intervention (...).” |
8 |
RESULTS: PHASE 1: UMBRELLA REVIEW OF CRM LITERATURE REVIEWS
Quality of the Literature Review
Upon pulling together the literature reviews conducted on CRM in healthcare to date and conducting our umbrella review of such work, it became apparent that there is a strong variation between how the 16 literature reviews were conducted and documented. Only 9 of the 16 reviews presented a flowchart that shows the process from initial search until the final set of articles in detail.7,11,12,16,17,22–24,26,27 Others gave a short description of this process.25 Likewise, 2 reviews did not present the full summary table of the selected articles and instead only provided a selection of information.18,19 These and other factors are reflected in the AMSTAR rating, which varies between 3 and 10 with Gross et al11 (2019), McCulloch et al27 (2011) and O’Connor et al19 (2008) receiving the highest AMSTAR scores.
Overall Findings
Table 1 provides a summary of the 16 CRM literature reviews included within our umbrella review. This table highlights some of the key areas of consensus across all the reviews. For instance, all of the reviews provide evidence of the positive effects of CRM on participant reaction, knowledge, attitude, skills, behavior, learning, transfer of knowledge to workplace, safety culture, and teamwork (e.g., communication, coordination) within the healthcare setting. However, although, at a high level, the positive effects of CRM exist, the picture is far from universal across all 16 literature reviews. For instance, the review by Salas et al20 (2006) suggests that the impact of teamwork training is mixed. Even those who found evidence of benefits of CRM were of varying strengths. For instance, O’dea et al7 (2014) suggest that CRM had large effects on knowledge and behavior and a small effect on attitudes. In comparison, O’Connor et al19 (2008) found that the strength of the relationship with attitudes and behaviors was large while the effect with knowledge was only medium.19
Building upon these mixed results, Table 1 also provides insights into other areas of heterogeneity among the reviews. To start, there is substantial variability in the number of studies included in each review (range from 7 to 64 underlying articles). In part, this variability may be the result of the target group examined within each review—from no limitation or all healthcare settings to a specific healthcare setting (e.g., acute care, hospitals), department (e.g., emergency department), or team (e.g., interprofessional teams). Likewise, what CRM entails varies across these various reviews to include techniques such as CRM training, simulation training, simulation crisis resource management training, and classroom-based CRM training.
Synthesis of Themes
Based on our review of the 16 CRM reviews conducted to date, we have identified a variety of issues that raise questions concerning whether any of these reviews provides a complete picture of the CRM literature. Looking closer, we found 3 clusters of ambiguity: in definition of CRM, in outcomes, and in information.
Definition Ambiguity
As each literature review focuses mainly or partly on CRM, it could be expected that a clear description of what CRM entails was presented. Table 2 provides an overview on how the 16 literature reviews described CRM. This table indicates that CRM typically covers competences like knowledge, skills and attitude, and topics such as teamwork, leadership, situation awareness, decision making, and communication. At the same time, Table 2 demonstrates that there is no clear standard set of competencies or topics that CRM should address. Gross et al11 (2019) show a list of key words that are used to describe CRM (e.g., communication, situational awareness, leadership, teamwork, decision making, briefing). However, there is a lack in operationalization of terminology, and therefore, it seems that a universal definition of CRM does not exist. This causes a considerable gap in knowledge about what CRM includes and which elements are the ones that precisely alter behavioral processes and subsequently improve patient safety. Most of the selected literature reviews do not address this issue and circumvent this by pretending that there is consensus about what CRM training interventions actually entail. Interestingly, only 7 of the 16 literature reviews included a description of the CRM training in their summary of the results.7,11,18,20,26–28 These descriptions show us that CRM curricula vary significantly. McCulloch et al27 (2011) suggest that the instructional methods of CRM training could consist of classroom-based methods only, or leverage simulation-based methods only, or a combination of both. O’dea et al7 (2014) provide insights from the standpoint of variation in training time between different methods. Information-based methods, such as lectures, vary between 1 hour and 1 day. Practice-based methods, such as a simulation, vary between 2 hours and 1 day. Although most CRM training interventions had a 1/2- or 1-day format,11 they can last up to 2 or 3 days.31–33 Recently, Gross et al11 (2019) explicitly addressed the issue of a lacked shared definition by showing that less than half of the studies in their systematic review provided information that would allow the CRM intervention to be replicated. In addition, they suggested minimum requirements for describing the intervention design (i.e., aims, methods, contents) in future CRM articles.
TABLE 2.
Descriptions of the CRM Concept
| Authors (Year) | Description of CRM Within Review |
|---|---|
| I. Reviews that focus on CRM | |
| Boet et al16 (2014) | “The ultimate goal of all CRM simulation training is to increase patient safety and result in better patient outcomes.” |
| Fung et al17 (2015) | “CRM includes clinical as well as communication and team-working abilities. CRM refer to principles such as leadership and followership, communication, teamwork, resource use, and situational awareness.” |
| Gross et al11 (2019) | Salas et al30 (1999) defined CRM training as a “a family of instructional strategies designed to improve teamwork in the cockpit by applying well-tested training tools (e.g., performance measures, exercises, feedback mechanisms) and appropriate training methods (e.g., simulators, lectures, videos) targeted at specific content (i.e., teamwork knowledge, skills, and attitudes). The purpose of CRM in high-risk organizations can be summarized as error countermeasures with three lines of defense: (1) avoidance of error, (2) trapping incipient errors before they are committed and (3) mitigating the consequences of those errors which occur and are not mitigated.” |
| Maynard et al18 (2012) | Possible CRM training components: patient safety overview within healthcare, role of CRM in other industries and within healthcare to address safety, communication, normalization of deviance, ingredients for effective teamwork, conflict, team briefings, team debriefings, assertiveness, situational awareness, shared mental models, red flags, and decision making. |
| O’dea et al7 (2014) | “The purpose of CRM training is to promote safety and enhance efficiency through optimum use of all available resources: equipment, procedures and people. The focus of CRM training is not on technical skills but rather cognitive and interpersonal skills, such as communication, situational awareness, problem solving, decision making, leadership, assertiveness and teamwork. Training is usually designed to develop generalizable, transportable teamwork competencies that learners can apply across different settings and teams. Instructional methods include: information-based methods (e.g., didactic lecture); demonstration-based methods (e.g., behavioral modeling, videos); and practice-based methods (e.g., simulation, role playing).” |
| O’Connor et al19 (2008) | CRM training can be defined as “a set of instructional strategies designed to improve teamwork in the cockpit by applying well-tested tools (e.g., performance measures, exercises, feedback mechanisms) and appropriate training methods (e.g., simulators, lectures, videos) targeted at specific content (i.e., teamwork knowledge, skills, and attitudes) (Salas et al, 1999, p.163).30” “An introductory CRM course is generally conducted in a classroom for 2 or 3 days. Teaching methods include lectures, practical exercises, role playing, case studies, and video of accident re-enactments. CRM courses typically cover core topics such as teamwork, leadership, situation awareness, decision making, communication, and personal limitations.” |
| Salas et al20 (2006) | “CRM is an instructional strategy that trains crews to effectively use all of their available resources (i.e., people, equipment, and information). CRM training has been defined as a set of “instructional strategies designed to improve teamwork in the cockpit by applying well tested training tools (e.g., performance measures, exercises, feedback mechanisms) and appropriate training methods (e.g., simulators, lectures, videos) targeted at specific content (i.e., teamwork knowledge, skills, and attitudes)” (Salas et al, 1999, p.163).30” “… it can be conceptualized as a team training strategy focused on improving crew coordination and performance.” |
| Verbeek-van Noord et al12 (2014) | “CRM typically includes educating teams about the limitations of human performance. Operational concepts include inquiry, seeking relevant operational information, assessing personal and peer behavior, communicating proposed actions, conflict resolution, and decision making.” |
| Zeltser and Nash21 (2010) | Not clear. |
| II. Reviews that focus on simulation | |
| Doumouras et al22 (2012) | “Simulation-based crisis resource management (CRM) training using a realistic computer-controlled mannequin is believed to be a useful strategy for teaching team-based skills. This methodology allows for repeated instruction and deliberate practice while posing no threat to patients.” |
| Murphy et al23 (2015) | “It (referring to simulation) is based on the experiential learning theory which provides devices, staff, virtual environments and contrived situations that replicate the clinical environment and events that arise in professional situations.” |
| Tan et al24 (2014) | Not clear. |
| III. Reviews that focus on team training in general | |
| Buljac-Samardzic et al25 (2010) | “CRM encompasses a wide range of knowledge, skills, and attitudes including communication, situational awareness, problem solving, decision making, and teamwork.” |
| Low et al26 (2018) | “Crew resource management (CRM) is an educational curriculum that was initially developed for the aviation industry to improve safety, communication and decision making. CRM was adapted to healthcare when patient simulators were used in anesthesia training programs and highlights five essential core concepts: team structure, leadership, situational awareness, mutual support and communication.” |
| McCulloch et al27 (2011) | Not clear. |
| Weaver et al28 (2014) | “A specific team-training strategy focused on developing a subset of teamwork competencies including hazard identification, assertive communication and collective management of available resources.” |
Outcomes Ambiguity
In addition to the lack of consistency regarding the conceptualization of a CRM training, there also seems to be a lack of agreement regarding the impact of CRM interventions in terms of the relationship between CRM programs and the impact of such an intervention on a variety of outcomes.7 As suggested previously, the 16 literature reviews included in our umbrella review seem to present a clear picture that CRM has a positive effect on outcomes. However, when we look across different outcomes, there are different results. Namely, the impact of a CRM training is especially clear at Kirkpatrick’s hierarchy evaluation level 1 (i.e., reaction) but lacks consistency when looking at level 2 (i.e., learning) and level 3 (i.e., behavior).7,19 Likewise, it is widely debated whether CRM training has an effect on the bottom line: performance outcome such as improvement in specific patient safety outcomes (Kirkpatrick’s level 4). The review by Salas et al20 (2006) states that the evidence included in their review is mixed.20 As a result, some suggest that the relationship between CRM and patient safety is not yet proven. Others, however, point out that there are a couple of studies that have shown CRM to have a beneficial effect for patients but also recognize the limitations regarding the conceptualization and the quality of evidence.11,16,17
An underlying issue is that the variety of outcome measures that have been examined within CRM research is challenging to fit precisely into Kirkpatrick’s categories, which resulted in alterations such as splitting level 2 into attitude (2a) and knowledge/skills (2b) or including marks (e.g., *) that represents deviations such as using qualitative evaluation methods (instead of quantitative), as well as varying the time at which outcomes are measured (i.e., right after the training intervention or after a delay). Nevertheless, only 5 of the 16 literature reviews clearly present the measures used in their findings.7,11,12,17,18,27 Such a sentiment was shared by Gross et al11 (2019) who suggested minimum requirements for describing the evaluation (i.e., method of evaluation, sample group size, statistical data, outcomes) for future CRM articles.11
Information Ambiguity
As detailed in Table 1, many of the reviews conducted to date have focused on the relationship that CRM training interventions have on various outcome metrics. However, there is a lack of information provided in the literature reviews conducted thus far regarding the first and last step in this process: implementation of CRM and sustaining the effects. The review conducted by Verbeek-van Noord et al12 (2014) is the only review that presented information on the implementation strategy. In addition, Gross et al11 (2019) discussed studies with an implementation strategy.11 Similarly, only Tan et al24 (2014), Verbeek-van Noord et al12 (2014), and O’dea et al7 (2014) explicitly address the sustainability of results as they highlight the period over which the effect of CRM was measured. This is unfortunate given that multiple reviews acknowledge the need for more evidence regarding the sustainability of CRM initiatives (e.g., the study by Maynard et al18). In addition, Gross et al11 (2019) emphasize the importance of considering training conditions to include factors such as the trainer qualification and the number of participants.11
Measures to grade the level of evidence or the methodological quality could help make a judgment regarding an article. The level of evidence of the selected CRM articles by the reviews is often not quantified. Tan et al24 (2013) and McCulloch et al27 (2011) are the only ones to address the quality of evidence per study. Tan et al24 (2014) even conclude that all the selected articles (on multidisciplinary simulation training) in their review present a low quality of evidence.
Conclusion Phase 1
Most of the 16 selected reviews base their conclusion on different domains in healthcare. This contributes in part to the interesting finding that within these reviews, there is a lack in overlap between the 16 literature reviews regarding the presented studies. When looking across the 16 reviews, if one were to merge the studies reviewed, it would result in 274 articles in total with 190 of these articles being unique. By digging into the reviews that have been conducted to date, only 17 of the articles were included within 3 or more of the reviews, only 49 of these 190 articles were actually presented by 2 or more reviews, and the remaining 141 articles were presented in only 1 review. Recently, the systematic literature review conducted by Gross et al11 (2019) seems to present the most comprehensive overview of the CRM literature. However, although more comprehensive than others, within their review, only a third of the articles included overlap with the other 15 reviews. Because of the high level of heterogeneity of the present literature reviews, the need to present one overall review is still present. As a result, within phase 2, we conducted our own literature review of the healthcare CRM literature with the aim of being more comprehensive than any single review conducted to date.
METHODS: PHASE 2: COMPREHENSIVE CRM LITERATURE REVIEW
As a result of the conclusion of phase 1, we conducted a new literature review on CRM in healthcare with the aim of providing the most comprehensive review of this literature stream to date and thereby filling several of the identified gaps noted during our umbrella review (i.e., phase 1).
Search Strategy
First, we searched the following databases for CRM articles: PubMed, EMBASE, Web of Science, and Google Scholar. The search involved a combination of the key words “CRM” OR “crew resource management” OR “crisis resource management” and was restricted to articles from 2006 (see Appendix 2, http://links.lww.com/JPS/A377). This search strategy resulted in 891 hits. First, similar to the process used in phase 1, 2 of the authors evaluated the title and abstract by adhering to the inclusion and exclusion criteria highlighted hereinafter and then following this with the full-text evaluation by way of the same criteria (Fig. 2). This resulted in 90 articles. Second, the presented articles within the 16 literature reviews (phase 1) were extracted and also evaluated according the inclusion and exclusion criteria. This second step resulted in 2 additional articles. Third, snowball research was applied by analyzing the included articles and their reference lists, which added 14 articles. In total, 106 articles were included.
FIGURE 2.
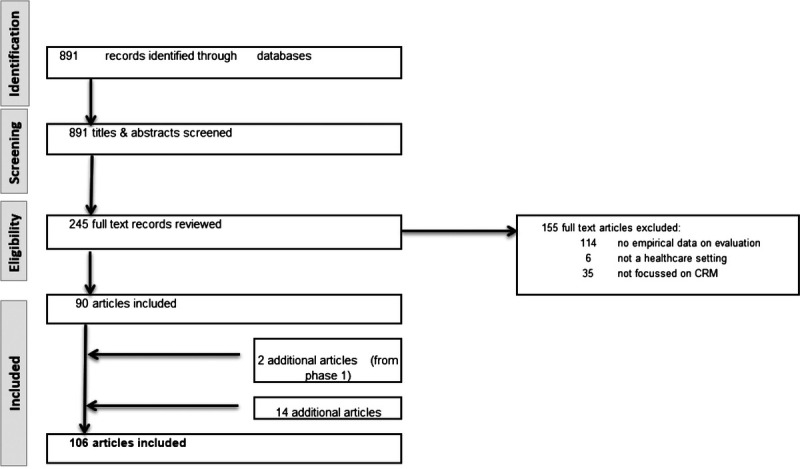
Flow chart phase 2.
Inclusion and Exclusion Criteria
Articles were included if they examined CRM interventions within healthcare and did so by leveraging empirical analysis. In contrast, articles were excluded if they (1) did not cover a CRM intervention, but for example, a related intervention such as TeamSTEPPS or in case results could not be tracked backed to the CRM intervention because it was only 1 element of a bigger intervention; (2) did not present empirical data on the evaluation of CRM, but for example, only described the development of a CRM intervention or only focused on the educational improvement of CRM training; or (3) did not focus on healthcare organizations but on the profit sector or on educational institutions. However, the actual content of the CRM intervention was not considered as an inclusion or exclusion criterion. If the authors themselves referred to CRM, it was included. In addition, we did not consider methodology (e.g., quantitative, experimental, qualitative) as an exclusion criterion.
Analysis
The 106 articles were summarized in Table 3 by author, year, aim of the study, setting, study design, main results as well as the Kirkpatrick’s level of outcome, implementation strategy (yes or no), and sustainability strategy (yes or no). In addition, the quality of the evidence was evaluated by MMAT (Mixed Methods Appraisal Tool). MMAT allows an assessment of methodological quality (quality of reporting) of all articles, regardless of their methodology. Although the criteria differ for each type of research, each domain for quantitative and qualitative research includes 4 criteria. The final score for each article depends on the number of criteria met and can vary from 25%, 50%, 75%, to 100% if all criteria are met. For mixed method research studies, the calculation of the final score is a little different and depends on the quality of the weakest component (qualitative, quantitative, or mixed method).136
TABLE 3.
Summary Included Articles Phase 2
| Authors (Year) | Main Aim of Study | Setting | Study Design | Main Results | Impl. Strategy | Sust. Strategy | Kirkpatrick Level | MMAT |
|---|---|---|---|---|---|---|---|---|
| Allan et al34 (2010) | To evaluate the implementation of a multidisciplinary in situ pCICU–CRM training program on comfort and confidence levels among participants involved in resuscitation events | pCICU | Pre-post survey | > Participants found course useful and realistic, found themselves better prepared to participate in and to lead resuscitation events, felt more confident, had a lower anxiety level to participate in events, and reported to be more likely to raise concerns about inappropriate management to team leader | No | No | 1, 2 | 100% |
| Atamanyuk et al35 (2013) | To evaluate the face validity of an affordable and realistic tool for interprofessional CRM training, and the impact on communication skills | Pediatric ICUs | Pilot study | > High face validity of the scenario, the model, and the content > High impact on practice, teamwork, and communication |
No | No | 1, 2, 3* | 25% |
| Ballangrud et al36 (2014a) | To describe intensive care nurses’ perceptions of simulation-based team training based on CRM for building patient safety in the ICU | ICUs | Qualitative design based on individual interviews | > Participants experienced that the training created awareness about clinical practices and acknowledged the importance of structured teamwork for patient safety > Realistic training makes nurses more prepared to provide care |
No | No | 1, 2 | 100% |
| Ballangrud et al37 (2014b) | To investigate intensive care nurses’ evaluations of simulation-based team training based on CRM | ICUs | Post survey | > Participants were highly satisfied with current learning in the training and scored also high on self-confidence in learning | No | No | 1, 2 | 100% |
| Bank et al38 (2014) | To evaluate the effects of a short, needs-based pediatric CRM simulation workshop with postactivity follow-up on recognizing common errors in teamwork and improving perceived abilities to manage pediatric patients | Pediatric emergency medicine department | Pre-post survey and pre-post video assessment | > Participants improved the abilities to manage the medical and team functioning—related issues in pediatric resuscitation > Improvement in identification of CRM errors |
No | Yes | 1, 2, 3 | 100% |
| Batchelder et al39 (2009) | To examine a specific element of the training and to measure and quantify changes in performance | Prehospital emergency medicine | Beginning and end of the course video evaluation and pre-post survey | > Increase in time from arrival to inflation of tracheal tube cuff > Decreased number of safety critical events > Higher CRM behavior scores > Increased confidence in prehospital anesthesia competencies |
No | No | 2 | 100% |
| Blackwood et al40 (2014) | To examine the effect of a brief CRM teaching session on pediatric advanced life support, CRM skills, resuscitation, and teamwork behavior | Pediatric hospital | Prospective randomized control pilot study | > Intervention group placed monitor leads earlier, placed an IV sooner, called for help faster, and checked for a pulse after noticing a rhythm change quicker > Intervention group had higher crisis resource management performance scores |
No | No | 3* | 100% |
| Budin et al41 (2014) | To describe changes in perinatal nurse and physician caregiver perceptions of teamwork and safety climate after a 6-mo CRM training program | Perinatal units | Pre-post survey | > Improvement in nurses’ and physicians’ perceptions of teamwork and safety climate > Both groups improved |
Yes | Yes | 2 | 100% |
| Burden et al42 (2014) | To compare simulation versus lecture teaching CRM skills and its effect on performance | Internal medicine | Randomized control pre-post study | > Simulation intervention improved team communication and cardiopulmonary arrest management | No | No | 2, 3* | 100% |
| Carbo et al43 (2011) | To evaluate residents’ patient safety attitudes and knowledge after an adapted CRM curriculum from other settings to internal medicine | General medicine units | Pre-post survey | > Improvement in knowledge about key skills of team training > Improvement in assertiveness > Increased likeliness to fill out an incident report for a near miss |
No | No | 1, 2, 3* | 75% |
| Carpenter et al44 (2017) | To research the effect of CRM-based medical team training on creating open, yet structured, communication | OR | Pre-post survey and checklist documentation | > Improvement in job satisfaction, safety climate, and working conditions > Improvement to adherence to checklist |
Yes | Yes | 2, 3 | 50% |
| Castelao et al45 (2011) | To evaluate the effect of video-based CRM training on no-flow time and proportions of team member verbalizations | Students | Randomized control trial | > CRM training reduced no-flow time, improved team leader verbalization, and improved follower verbalization in the category unsolicited information | No | No | 3 | 100% |
| Castelao et al46 (2015) | To assess the impact of CRM team leader training (compared with ALS training) on CPR performance and team leader verbalization | Students | Prospective randomized controlled study | > CRM team leader training had higher ADH scores, team leader verbalizations, but not significantly shorter no-flow time | No | No | 3 | 100% |
| Catchpole et al47 (2010) | To examine the effect of aviation-style team training on surgical teams and to examine the organizational and social context in which the observable changes take place | OR | Pre-post observations, pre survey, and ethnographic observation | > Increased number of stop-checks, briefings, and debriefings > Intraoperative teamwork was not unequivocally improved |
Yes | No | 2, 3 | 100% |
| Chan et al48 (2016a) | To evaluate how healthcare professionals perceive a simulation team-based CRM program | High-risk hospital departments | Post survey | > High scores on overall satisfaction with program, the applicability of the program, and the high standard and expertise of the trainers > Most participants would recommend the program to colleagues |
No | No | 1 | 100% |
| Chan et al49 (2016b) | To evaluate participant reactions and attitudes to CRM teamwork classroom-based training and exploring potential differences in attitudes across the different healthcare professionals | Multiple hospital departments | Pre-post survey and a second post survey | > Positive effect on human factors attitude of frontline professionals > Nurses showed a greater positive shift in attitudes toward patient safety than doctors > Participants found the CRM classroom-based training program useful, relevant, and interesting |
No | No | 1, 2 | 75% |
| Ciporen et al50 (2018) | To evaluate participants on performance metrics and teamwork dynamics and to evaluate CRM-based simulation at the end of the experience | Neurosurgery and anesthesiology | Pre-post survey and observations | > Participants overall agreed that the simulation was realistic, clinically applicable, and useful. No differences were found between disciplines > The simulation was found useful in facilitating improved understanding of relevant anatomy |
No | No | 1, 2 | 75% |
| Clarke et al51 (2014) | To measure the development of NTSs over time | Emergency medicine | Observational longitudinal cohort study | > Improvements over time on Ottawa GRS between year 1 and 2, but no significant improvement between year 2 and 3 | No | No | 3* | 100% |
| Clay-Williams et al52 (2013) | To test the effectiveness of classroom- and simulation-based CRM training alone or in combination, in improving the teamwork attitudes and behaviors of healthcare professionals | Acute hospital settings | Randomized controlled trial, pre-post survey, another post survey, and post hoc observations | > Reaction to classroom training was universally positive (to simulation training was not measured) > Improvements in knowledge and teamwork behavior after classroom training > No impact of additional simulation training next to classroom training > No improvement in teamwork attitude after classroom, simulation, or combination training |
No | No | 1, 2 | 50% |
| Clay-Williams et al53 (2014) | To explore the potential for modularized CRM training to interprofessional healthcare workers | Hospital | Pre-post surveys | > Workshops met the needs of participants and provided interprofessional learning experience and practical skills > Barriers were identified for implementing learned tools/strategies |
No | No | 1, 2, 3* | 100% |
| Clay-Williams and Braithwaite54 (2015) | To test the effectiveness of classroom- and simulation-based CRM courses (alone and in combination), and identify organizational barriers and facilitators to implementation of team training programs in healthcare (process evaluation of Clay-Williams et al,52 2013) | Acute hospital settings | Randomized controlled trial, pre-post interviews, and post implementation interviews | > Improvement in knowledge and teamwork behavior after classroom training > Facilitators and barriers (i.e., hospital time and resource constraints and poor organizational communication) for implementation were identified |
Yes | No | 1, 2, 3 | 100% |
| Cooper et al55 (2008) | To compare the safety climates between departments and to assess the impact of the simulation-based CRM training on safety climate | Anesthesia departments | Pre-post survey | > Different climate scores among hospitals, no difference between the trained and untrained | No | No | 2 | 75% |
| Coppens et al56 (2018) | To investigate (i) whether integrating a course on CRM principles and team debriefings in simulation training, increases self-efficacy, team efficacy, and technical skills of nursing students in resuscitation settings and (ii) which phases contribute the most to these outcomes | Nursing students | Randomized controlled trial, pre-post survey, and observations | > Improvement in self-efficacy and team efficacy in the intervention group, while the control group only showed improvement on team efficacy > The debriefing phase contributes most to these effects |
No | No | 2, 3 | 100% |
| De Korne et al57 (2014) | To evaluate the implementation of a broad-scale TRM program on safety culture | Eye hospital | Pre-post interviews and observations | > Increasing safety awareness and social team interaction > Increased number of reported near incidents > Stabilization of number of wrong-side surgery to a minimum (after reduction) |
Yes | No | 1, 2, 3, 4 | 100% |
| Duclos et al58 (2016) | To assess the impact on major surgical complications of adding a CRM-based team training program after checklist implementation | OR | Cluster randomized trial, case reports on adverse events and compliance of checklist use | > Improvement in surgical outcomes (i.e., major adverse events), with no difference between trial arms across intervention and control hospitals | No | No | 4 | 100% |
| Emani et al59 (2018) | To research the effect of low-fidelity simulation-based crisis resource management CRM training on team performance (in low-resource setting) | pCICU | Pre-post questionnaire and observations | > Improvement in team dynamics and performance > Decrease in time to intervention > Increase in frequency of closed loop communication > No difference in performance |
No | No | 3 | 100% |
| Falcone et al60 (2008) | To evaluate the effectiveness of a multidisciplinary trauma training program (that emphasizes CRM training techniques) on team performance | Pediatric trauma care | Beginning to end of the study observations | > Improvement in overall performance (appropriate and timely care) and performance of specific resuscitation domains | Yes | No | 2 | 100% |
| Fore et al61 (2013) | To assess the impact of sterile cockpit principle on interruptions and distractions (during high-volume medication administration) and number of medication errors | Medical oncology unit at VA Health System | Pre-post design for medical error rates and post design for distractions | > Decrease in interruptions or distractions > Reduction in medication error rate |
Yes | No | 3, 4 | 100% |
| France et al62 (2008) | To evaluate the impact of CRM training on team compliance with perioperative safety practices | Surgical departments | Observational study | > Compliance with 60% of integrated safety and CRM practices > Compliance scores showed a downward trend over time |
Yes | No | 3 | 100% |
| Fransen et al63 (2017) | To investigate whether simulation-based obstetric team training focusing on CRM in a simulation center improves patient outcome | Obstetric units | Cluster randomized controlled trail | > The composite outcome of obstetric complications did not differ between intervention and control groups > In the intervention group damage due to shoulder dystocia was reduced and invasive treatment for severe postpartum hemorrhage was increased |
No | No | 4 | 100% |
| Gallagher64 (2016) | To evaluate a CRM follow-up program on long-term goals | Mother-baby and labor and delivery | Pre-post survey | > Improvement in most safety culture measurements > Improvement in hand hygiene (for labor and delivery) > Mixed results on improvement patient satisfaction |
Yes | Yes | 3*,4 | 100% |
| Gillespie et al65 (2017) | To evaluate the effect of a brief team training intervention on teams’ observed NOTSS | OR | Pre-posttest interrupted time series design (pre-post observation) | > Improvements in mean NOTECHS scores across the pre-posttest phases | No | No | 3 | 100% |
| Gillespie et al66 (2017b) | To evaluate a brief team training program in relation to teams’ observed NTSs in surgery, teams’ perceptions of safety culture, and the training implementation | OR | Mixed-methods design, including structured observations, a survey, and semistructured interviews | > Improvements in NTSs and in the use of the WHO Surgical Safety Checklist > No improvement in teamwork > Nonsignificant increase in safety climate and decrease in teamwork climate > Most participants agreed that the program highlighted the important role of individual and shared SA in identifying and managing risk |
No | No | 1, 2, 3 | 100% |
| Gillman et al67 (2015) | Describe the trauma multidisciplinary crisis resource course titled S.T.A.R.T.T. (Simulated Trauma and Resuscitative Team Training) | Trauma teams | Post study and observations | > High satisfaction of participants > Improvement in Ottawa GRS > No significant improvements in Advanced Trauma Life Support checklist |
Yes | No | 1, 3* | 100% |
| Gore et al68 (2010) | To evaluate the perceived efficacy of CRM initiatives | OR | Pre-post survey | > Improvement in reporting errors (only 2 questions) and patient safety climate (only 2 questions) > No improvement in teamwork |
Yes | No | 2 | 75% |
| Gross et al69 (2019b) | To establish the feasibility of chunking CRM training into microsize interventions and to compare different training approaches in the context of microlearning | Medical students | Pre-post survey and observations | > Both groups (i.e., example and lecture) showed most of the behaviors included in the instructional videos during the simulations and were able to recollect them > The didactic concept of the instruction caused a difference between the learning success of the groups |
No | No | 1, 2 | 100% |
| Guerlain et al70 (2008) | To measure the effect of CRM strategies on the resultant use and perceived utility | OR | Pre-post survey | > Increasing frequency of preoperative briefing elements > Using briefings practices correlates highly with respondents’ perceptions of communication, teamwork, and potential for reducing errors |
No | No | 2, 3* | 75% |
| Haerkens et al31 (2015) | To assess the effects of CRM implementation on outcome in critically ill patients | ICU | Preimplementation-post design for outcome measures, preimplementation survey design, and observations in implementation period | > Reduction of incidence of predefined complications > Reduced standardized mortality rate > Improvement in safety climate |
Yes | Yes | 2, 3, 4 | 75% |
| Haerkens et al71 (2018) | To assess the effects of CRM implementation on safety climate and time spent in the trauma room, and on hospital length of stay and 48-h crude mortality of trauma patients. | Emergency department | Pre-post implementation design for outcome measures (with control group) and surveys | > Improvement in safety climate (i.e., teamwork climate, safety climate, and stress recognition) and decrease perceptions of management > Job satisfaction and working conditions did not change > Length of stay increased > Mortality rate was unchanged |
Yes | Yes | 2, 4 | 100% |
| Haffner et al72 (2016) | To assess a CRM training program on the correction rate of improperly executed chest compressions and communication quality in a simulated cardiac arrest scenario | Medical students | Randomized study, pre-post survey, and pre-post observations | > Team leaders corrected improper chest compressions more often compared with the control group > Improvement in communication quality compared with the control group |
No | No | 2, 3 | 100% |
| Haller et al73 (2008) | To assess the effect of a CRM intervention on teamwork and communication skills in a multidisciplinary obstetrical setting | Labor and delivery unit | Pre-post survey | > Better understanding of teamwork and shared decision making in emergency situations > Improvement in team and safety climate and stress recognition |
No | No | 1, 2 | 75% |
| Hänsel et al74 (2012) | To evaluate the influence of a CRM course on situational awareness and medical performance in crisis scenarios and to compare the results with the effects of a purely clinical simulator training | Medical students | Randomized controlled trial, pre-post design with assessment tool | > The simulator training nor the CRM course influenced clinical performance > Situational awareness improved only after simulator training, not after CRM training |
No | No | 1, 2 | 75% |
| Hansen et al75 (2007) | To assess the educational benefit of a CRM training and whether the damage control techniques are used in daily practice | OR | Pre survey and another post survey | > Increase of number of team members who felt comfortable performing damage control surgery with own role (particularly surgeons) > Roughly 50% of surgeons and OR nurses used damage control techniques in practice > Improvement in the ability to handle severely injured patients improved |
No | No | 1, 2, 3* | 75% |
| Hansen et al76 (2008) | To evaluate a team-oriented and CRM-based approach and its impact on trauma care | OR | Post survey | > Improvement in proficiency with damage control techniques > Team approach was perceived as crucial > Most hospitals reported modifying trauma protocols |
No | No | 1, 2, 3* | 75% |
| Hay et al77 (2016) | To evaluate implementation of a “sterile cockpit” methodology to reduce the number of distractions during procedures | Nursing staff of gastrointestinal endoscopy procedure | Pre survey and another pre-post survey and observations | > Improved awareness of distraction and its impact on patient safety > Reduction of interruptions to zero > While reducing distractions, perception of nursing quality of care improved |
No | No | 2, 3 | 75% |
| Hefner et al78 (2017) | To examine the impact of a systematic multihospital implementation of CRM on staff perceptions of patient safety culture | Hospitals | Pre-post survey | > Significant improvement in dimensions of patient safety culture perception; teamwork and communication dimensions may be more likely influenced by CRM training than supervisor and management dimensions | Yes | No | 2 | 75% |
| Hicks et al79 (2012) | To describe the development, piloting, and multilevel evaluation of CREW training for emergency medicine residents | Emergency department | Pre-post survey and pre-post observational | > The training is perceived to be useful, effective, and highly relevant > Unable to detect a difference in attitude and NTSs |
No | No | 1, 2 | 75% |
| Hughes et al80 (2014) | To describe the development, implementation, and effectiveness of a trauma resuscitation-focused CRM program | Trauma resuscitation | Pre-post survey and pre-post observational design | > Improvement in accuracy of field to medical command information, accuracy of emergency department medical command information to the resuscitation area, team leader identity, communication of plan, and role assignment > More likely to speak up in case of safety concerns |
No | No | 1, 2, 3 | 75% |
| Jankouskas et al81 (2007) | To evaluate improvement in the NTSs of a multidisciplinary team of pediatric residents, anesthesiology residents, and pediatric nurses after participation in the CRM educational program | Pediatrics | Pre-post survey and observations | > Improvement in perceived collaboration, satisfaction with care, and teamwork skills > No significant improvement in situation awareness, decision making, and task management |
No | No | 2, 3 | 75% |
| Jankouskas et al82 (2011) | To evaluate CRM training (in combination with basis life support) during a simulated patient crisis | Nursing and medical students | Experimental pre-post study | > Experimental teams compared with control teams: improvement in team process > Both experimental and control teams showed improvements in team effectiveness |
No | No | 3, 4 | 75% |
| Kemper et al83 (2014) | To examine the impact of pretraining readiness factors and posttraining barriers and facilitators on follow-up on plans of action | ICUs | Pre-post survey | > Perceived barriers and facilitators after CRM training is related with taking action > Readiness factors were positive related to taking action, only when assessed together and not separately > Support of the management for patient safety before the training is a positive determinant of the number of perceived facilitators |
Yes | No | 2, 3* | 100% |
| Kemper et al32 (2016) | To assess the effectiveness of a classroom-based CRM training in ICU | ICUs | Controlled trail, pre-post survey with mixed method data | > Improvement in behavior aimed at optimizing situational awareness (based on survey, not observation) > Improvement in error management culture, job satisfaction, and patient safety culture (also in control group) > Patient outcome and situational awareness attitude were unaffected |
Yes | No | 1, 2, 3, 4 | 100% |
| Kuy and Romero et al84 (2017a) | To determine whether rates of CITN patient safety adverse events change after CRM training | Surgery (VA) | Pre-post outcome measures | > Complete compliance to performance of briefings and debriefings after CRM training > Decrease of CITN events to zero after CRM training |
Yes | No | 3, 4 | 100% |
| Kuy and Romero et al85 (2017b) | To describe implementation of CRM in a VA Surgical Service and to assess whether staff CRM training is related to improvement in staff perception of a safety climate | Surgery (VA) | Pre-post survey | > Improvement in safety climate | Yes | Yes | 2 | 75% |
| LaPointe86 (2012) | To observe the impact of aviation-based CRM training on the safety attitudes of perioperative (surgical) personnel | OR | Quasi-experimental pre-post survey | > Improvements in most of the safety attitudes > No reduction of error rate and safety culture |
No | No | 2, 4 | 100% |
| Lehner et al87 (2017) | To establish interdisciplinary simulation-based team training as a tool to improve the care of trauma patients in the pediatric surgery trauma room | Pediatric emergency department | Pre-post survey and another post survey | > The course was evaluated as very realistic and relevant to the daily routine, detailed debriefings were evaluated as positive > Participants reported improvement in technical and/or medical skills (i.e., cardiopulmonary resuscitation) and NTSs (i.e., setting priorities) |
No | No | 1, 2 | 50% |
| Mah et al88 (2009) | To evaluate mannequin-based simulations (using multidisciplinary teams of clinicians) | ICU | Pre-post (real time) observation and pre-test | > Positive relation of knowledge of sepsis guidelines and proportion of task completion, but correlations between specific tasks and related questions showed no relationship to knowledge | No | No | 2, 3 | 75% |
| Mahramus et al89 (2016) | To assess the effectiveness of a 2-h teamwork training program | Cardiopulmonary arrest (code) team | Quasi-experimental design, pre-post survey, pre-post observations | > Improvement in perception and observation of teamwork > Program was evaluated positively |
No | No | 1, 2, 3 | 75% |
| Man et al90 (2019) | To investigate the impact of locally adopted simulation-based CRM training on participants’ perceptions and knowledge | OR and general | Pre-post survey | > Most participants reported the training to be useful and relevant in daily practice > Improvement in perception and knowledge after 1-mo postcourse but declined after 1-y postcourse |
No | No | 1, 2 | 75% |
| Mancuso et al91 (2016) | To assess the effectiveness of CRM training and interventions on communication | Labor and delivery | Pre-post observation | > Improvement in quantity and quality of communication | Yes | No | 3 | 100% |
| Marshall and Manus92 (2007) | To examine the cultural impact of a CRM-based Human Factors in Healthcare Demonstration Project | Surgery | Pre-post survey | > Overall improvements in patient safety awareness and the quality of team-based behaviors and performance | Yes | Yes | 2, 3 | 100% |
| McCulloch et al13 (2009) | To assess the effect of aviation-style NTS training on the number of potentially significant errors and mishaps with potential for harm to patients and clinical outcome measures | OR | Pre-post observation, pre-post survey with clinical outcome measures | > Improvement in safety climate and nontechnical performance > Decreased operative technical error and nonoperative procedural errors > Operating time was unaffected and length of hospital stay not reduced significantly |
No | No | 2, 3, 4 | 100% |
| Mitchell and Dale93 (2015) | To assess the effect of a 1-d human factors (CRM) training program | Neurosurgical theater staff | Pre-post observation with side error rates | > Prelist briefing meetings were adopted and quickly became widely used > Postlist debriefing meetings were introduced but were not widely adopted > Mean time between side errors increased from 2 to 18 mo > After the training, no errors occurred in 82 mo |
Yes | Yes | 1, 2, 3, 4 | 75% |
| Moffatt-Bruce et al94 (2017) | To evaluate the costs and ROI of implementing a CRM program and to improve understanding about its financial impact | Hospitals | Retrospective analysis | > A 25.7% reduction in observed relative to expected events (725 fewer AEs) > Increased hospital savings from estimated reduction in avoidable events > Significant ROI from reduced adverse events over a 3-y period >The overall ROI for CRM training was in the range of $9.1–$24.4 million |
Yes | No | 4 | 100% |
| Morgan et al95 (2009) | To determine whether simulation-based debriefing and feedback improved performance of practicing anesthetists managing high-fidelity simulation scenarios | Anesthesiology | Prospective, randomized, controlled study | > Improvement of skills > Participants from the debrief group did not overall perform better than those in the control group > The effect of the educational intervention was still evident 6–9 mo later |
No | No | 3* | 100% |
| Morgan et al96 (2011) | To determine whether a high-fidelity simulation educational debriefing session improved the NTSs in the management of simulated anesthetic scenarios | Anesthesia departments | Pre-post observations | > No improvement in task management and team working > Improvement in situation awareness (only in the debrief group) and in decision making (for both groups) |
No | No | 3 | 100% |
| Morgan et al97 (2015) | To test the effectiveness of a combined SOP (standard operating procedures) and CRM-based teamwork training intervention to improve the quality, safety, and reliability of surgical team performance | Orthopedic surgery | Controlled interrupted time series with pre-post observations and clinical outcomes | > Improvement in NTS and WHO compliance > Glitch rates decreased in the intervention as control group > No significant effect on clinical outcomes |
No | No | 3, 4 | 100% |
| Müller et al98 (2007) | To establish and evaluate a CRM course combining psychological teaching with simulator training | Emergency department | Post survey | > All participants rated the course as good or very good > The psychological exercises were highly valued |
No | No | 1 | 75% |
| Müller et al99 (2009) | To evaluate the effect of 2 different simulator-based training approaches, CRM, and MED (classic simulator training), on performance and stress reduction of intensivists | ICUs | Randomized design, pre-post observation design, and pre-post saliva specimen | > Improvement in NTS and clinical performances in both CRM and MED group > Increased stress during the simulation, after the training stress (that is measured by salivary α-amylase) reduced |
No | No | 3 | 100% |
| Neily et al100 (2010a) | To evaluate to what degree skills taught through the CRM-based medical team training program are implemented and the impact on patient safety, processes of care, team functioning, and staff satisfaction | Surgery departments | Structured interviews | > Improvements in teamwork, safety, and efficiency > Most facilities implemented briefings and debriefings and an additional project > Sites with lower volume were more likely to conduct briefings/debriefings |
Yes | No | 1, 2, 3* | 100% |
| Neily et al101 (2010b) | To determine whether an association existed between the CRM-based medical team training program and surgical outcomes | OR | Retrospective mixed methods design with control group: structured interviews and mortality rates | >18% reduction of annual mortality rate compared with 7% in the control group > Decline in the risk-adjusted surgical mortality rate was approximately 50% greater in the intervention group compared with control group |
Yes | Yes | 3*, 4 | 100% |
| Nielsen et al33 (2007) | To evaluate the effect of CRM based teamwork training on the occurrence of adverse outcomes and process of care in labor and delivery | Hospital labor and delivery units | A cluster-randomized controlled trial, pre-post design for outcome measures | > No statistically significant differences between intervention and control group for outcome measures > Mean time elapsed between the decision to perform an emergency cesarean delivery and the time of the incision was shorter in the intervention group |
Yes | Yes | 4 | 75% |
| Nishisaki et al102 (2009) | To evaluate effectiveness on technical and behavioral skills and feasibility (logistics and finance) of a simulation-based orientation training | Pediatric critical care fellows | Post surveys | > Improvements in clinical performance and self-confidence | No | No | 1, 2, 3* | 50% |
| O’Connor et al103 (2013) | To develop and evaluate a CRM training program | Trainees | Pre-post survey, another post survey, and pre-post observations | > Improvement in knowledge > No improvement in speaking up about stress and behavior > Improvement in speaking up to seniors for in-between subject assessment |
No | No | 1, 2, 3 | 100% |
| Paull et al104 (2013) | To investigate the effect of simulation-based CRM team training curriculum on teamwork and communication skills | Surgery | Pre-post survey and observation study | > Improvement in teamwork > Improvements in (most) observed skills |
No | No | 3 | 50% |
| Parsons et al105 (2018) | To design and evaluate a CRM course that could be feasibly incorporated into any EM residency curriculum | Emergency medicine | Pre-post observations | > No improvement in leadership, problem solving, communication, situational awareness, teamwork, resource utilization, and overall CRM skills | No | No | 3 | 75% |
| Phipps et al106 (2012) | To determine whether implementing an L&D unit team training program with simulation training improves patient outcomes as well as perceptions of safety and communication | Labor and delivery units | Pre-post survey design and pre-during-post design for outcome measures | > Improvements in many dimensions of the L&D unit’s safety culture, but not dimensions of the hospital-wide culture > Frequency of event reporting and the overall perception of safety did not change > Overwhelming positive patient responses to both pre-CRM and post-CRM surveys, no changes detected > The Adverse Outcome Index showed a significant decrease compared with baseline measurement |
Yes | No | 2, 3*, 4 | 75% |
| Pratt et al107 (2007) | To assess the impact of CRM-based team training | Obstetrics department | Pre-post study | > Decrease in AOI, WAOS, SI, and malpractices > Improvement in safety attitude |
Yes | No | 3*, 4 | 50% |
| Rêgo et al108 (2008) | To describe the development, evaluation, and outcomes of a pilot CRM course | Ambulatory surgery | Pre-post study | > All participants would recommend this course > Participants would use CRM principles in the future > Improvement in communication and the ability to assert when necessary with more senior staff |
No | No | 1, 2, 3* | 50% |
| Ricci et al109 (2012) | To measure the effect of a surgical CRM training program for all OR personnel, on WSS and RFBs | OR | Pre-post outcome measures and audit data | > Preoperative briefing increased to 99% within 4 mo > Wrong site surgeries and retained foreign bodies decreased to none, but after 14 mo without additional training, rose to 5 |
Yes | Yes | 3, 4 | 75% |
| Rovamo et al110 (2015) | To evaluate the impact of CRM and anesthesia NTS instruction on teamwork | Delivery units | Pre-post observation with control group | > No improvements in team performance > Experience of team leaders improved teamwork over the CRM |
No | No | 3 | 100% |
| Sandahl et al111 (2012) | To describe implementation of simulator-based medical team training and the effect of this program on interprofessional working | ICUs | Case study | > Increased awareness of importance of effective communication for patient safety > Created a need to talk, which resulted in regular reflection meetings |
Yes | Yes | 1, 2, 3 | 25% |
| Savage et al112 (2017) | To evaluate the multilevel effects over time of the implementation of standardized CRM-based team training and targeted system improvement projects | Pediatric surgery | Multilevel prospective single-case study | > Improvement in NTSs, the use of safety tools, and adherence to guidelines for appendectomies > Improvement in safety culture: teamwork across and within units, supervisors’ expectations and actions, nonpunitive response to adverse events, and perceptions of overall patient safety > Improvement in unplanned readmissions after appendectomy |
Yes | No | 1, 2, 3, 4 | 100% |
| Sax et al113 (2009) | To quantify effects of aviation-based CRM training on patient safety–related behaviors and perceived personal empowerment | Surgical departments | Pre-post survey design and check list use and error reporting over time | > Improvement in preoperative checklist use, self-initiated reports, and the percentage of reports related to environment as opposed to actual events increased > Improvement in perceived self-empowerment and creating a culture of safety |
Yes | Yes | 2, 3, 4 | 75% |
| Schwartz et al114 (2018) | To implement and evaluate clinical team training, which is a combination of CRM-based medical team training and nursing CRM | VA facilities | Pre-post survey | > Improvement in communication, teamwork and situational awareness for patient safety > Observed decreases between 6- and 12-mo measurement |
Yes | No | 2 | 50% |
| Sculli et al115 (2013) | To measure the effect of nursing based CRM program using a multifaceted approach | Surgical, intensive care, intensive care step down, and long-term care units | Pre-post survey and pre-post outcome measure design and follow-up interviews | > Improvements in all teamwork domain questions > Significant gains were realized in the areas of medication errors, HAPU, glucose control, FTR events, and care processes |
No | Yes | 2, 3, 4 | 100% |
| Shea-Lewis116 (2009) | To investigate the feasibility of a CRM-based training to improve patient care | Obstetrics | Pre-post outcome measures and continuous surveys | > Improvement in patient outcomes, patient, and staff satisfaction | No | No | 4 | 100% |
| Siems et al117 (2017) | To evaluate CRM NTS training as an improvement technique for rapid response team performance | Pediatric critical care | Pre-post observations | > Improvement in leadership, teamwork, task management, and global scores > Improvement in patient transfer regarding team leader and team introductions, floor team presentations in SBAR format, and confirmation of the plan |
Yes | No | 3 | 100% |
| Stocker et al118 (2012) | To evaluate the impact of an embedded simulation-based team training program on perceived performance and to compare the effect over different phases of the program | Pediatric intensive care | Implementation and post survey | > Impact on overall practice perceived as effective > Nontechnical skills (communication and teamwork) and technical skills showed an effective impact > Increased score for effective impact over phases |
Yes | No | 1, 2, 3* | 100% |
| Sundararaman et al119 (2014) | To implement and evaluate a CRM training | Radiation oncology | Case study using objective outcomes | > Improvement in safety record: decrease in near-miss rate and elimination of all treatment deviations > High sense of teamwork combined with a high degree of personal responsibility to assure patient safety and speaking up about potentially unsafe situations > Increased efficiency |
Yes | No | 3, 4 | 100% |
| Suva et al120 (2012) | To analyze the impact of a CRM program on satisfaction and learning among OR personnel and compare disciplines | OR | Pre-post survey | > High satisfaction for course organization, group dynamics, and teaching methods > Improvement in learning, especially in the domain of teamwork and safety culture, less in stress recognition |
No | No | 1, 2 | 100% |
| Sweeney et al121 (2014) | To evaluate the effectiveness of Project CLEAR!, a novel simulation-based training program designed to instill CRM as the communication standard and to create a service-focused environment by standardizing the patient encounter | Emergency department | Pre-post survey | > Improvement in quality of communication between staff members and between staff and patient | Yes | No | 2, 3* | 75% |
| Tapson et al122 (2011) | To assess to effect of a quality improvement initiative for VTE prophylaxis that combined clinical education with CRM | Surgical department | Pre-post survey and retrospective reviews of patient charts | > Immediate and retained confidence and increased knowledge in identifying process related factors leading to errors > No difference in attitude > Reviews of patient charts preinitiative and postinitiative demonstrated performance improvement in meeting guideline recommendations for the timing, inpatient duration, and use of VTE prophylaxis beyond discharge |
Yes | No | 2, 3* | 75% |
| Taylor et al123 (2007) | To assess the effect of the CRM intervention on adherence to evidence-based diabetes care standards, work processes, standardized clinical communication, and patient outcomes | Primary care clinic | A quasi-experimental, interrupted time-series design, with observation and outcome measures | > Improvement in microalbumin testing and associated patient outcome measures > CRM resulted in reorganized work processes, teamwork with new roles and responsibilities, coordination and communication, and check for omissions using checklists to structure and drive clinical workflow |
Yes | No | 2, 3, 4 | 50% |
| Truijens et al124 (2015) | To explore whether multiprofessional (CRM-based) simulation-based obstetric team training improves patient-reported quality of care during pregnancy and childbirth | Obstetric collaborative network | Pre-post survey | > Improvement in patient-reported quality of care; personal treatment during pregnancy and educational information improved, but personal treatment during delivery showed no significant difference | No | No | 3* | 75% |
| Truta et al125 (2018) | To assess the effect of a single-day CRM training on NTSs | Emergency departments | Pre-post observations | > Improvements in all NTSs | No | No | 3* | 100% |
| Tschannen et al126 (2015) | To evaluate an intervention using NCRM principles implemented to improve communication among RNs and physicians | General medicine telemetry units | Pre-post survey | > Nonsignificant improvement in communication openness and environmental values (both RN’s and physicians) > RNs reported an increase in synchronous and asynchronous communication with physicians, physicians noted a reduction in time spent in asynchronous communication > RNs identified an improvement in the quality of synchronous communication, physicians did not note this improvement |
Yes | No | 2 | 75% |
| Tschannen et al127 (2018) | To examine virtual training on CRM principles on knowledge, applicability, and intended behaviors | Trainees | Pre-post survey | > Postknowledge test scores improved > Participants reported learning new skills and knowledge and intended to use the skills/knowledge gained from the training in clinical practice |
Yes | No | 1, 2 | 100% |
| Turkelson et al128 (2016) | To determine the effectiveness of a multifaceted educational strategy: simulation to introduce communication algorithm adapted from nursing CRM | ICU | Pre-post study | > Participants were satisfied > Improvement in knowledge > Improvement in interprofessional communication and manikin outcomes |
No | No | 1, 2, 3* | 75% |
| Verbeek-van Noord et al129 (2015) | To evaluate the effect of a 2-d classroom-based CRM training at emergency departments on explicit professional oral communication | Emergency departments | Controlled trial, pre-post survey, and observation | > Improvement in human interaction and the overall explicit professional oral communication score, but not in anticipation on environment | Yes | No | 2, 3 | 100% |
| West et al130 (2012) | To describe the application of a CRM technique, the sterile cockpit rule, to improve efficacy and safety for nursing assistants in the performance of patient care duties | Nursing units | Pre-post survey design and post outcome measures | > Improvement in efficiency: extensive improvements, dramatic decreases on all 3 measures of efficiency > Improvement in perception of nursing teamwork, patient safety, and staff moral |
Yes | Yes | 2, 4 | 75% |
| Westfelt et al131 (2013) | To evaluate CRM-based training of teams of endoscopists and endoscopy nurses, to increase self-efficacy | Internal medicine university hospital | Pre-post survey | > Positive perception regarding obtained theoretical knowledge, practical skills, critical thinking, and the usefulness of the course in daily clinical work > Improvement in self-efficacy |
No | No | 1, 2 | 100% |
| Wetzel et al132 (2013) | To investigate the effect of laboratory- and in situ simulation-based training sessions to improve technical and NTSs | Neonatal ICUs | Self-observed and identified latent safety threats | > Laboratory and in situ sessions resulted both in identifying LSTs and the underlying causes related to knowledge gaps, poor procedures or poor NTSs > In situ sessions resulted in improvements at the unit itself, the delivery process, or the hospital in general |
Yes | No | 4 | 50% |
| Wu et al133 (2016) | To assess the effectiveness of an interprofessional CRM education program on satisfaction and safety attitude | Emergency and critical care units | Pre-post survey and another post survey | > Improvement in human factor attitudes > Positive response to the CRM training |
No | No | 1, 2 | 100% |
| Zech et al134 (2017) | To evaluate a CRM-based team-training program | Obstetrics | Pre-post survey | > Strong effects in perception of competence regarding technical skills and handling of emergencies > Some indications for improvements on the patient safety culture level > Differences were found between professional groups and hospitals |
No | No | 1, 2 | 75% |
| Ziesmann et al135 (2013) | To develop and evaluate a national multidisciplinary trauma CRM curriculum | Trauma teams | Pre-post survey | > High satisfaction with the course > Improvement in attitudes toward simulation and attitudes toward CRM principles, including overall scores, teamwork, and safety climate |
No | No | 1, 2 | 50% |
ADH, Adherence to the 2010 Advance life support guidelines; AEs, adverse events; ALS, advanced life support; AOI, adverse outcome index; CITN, Critical Incident Tracking Network; CPR, cardiopulmonary resuscitation; EM, emergency medicine; FTR, failure to rescue; HAPU, Hospital-Acquired Pressure Ulcers; L&D, Labor & delivery; NCRM, nursing CRM; NOTECHS, NOn-TECHnical Skills; NOTSS, nontechnical skills in surgery; NTS, nontechnical skill; OR, operating room; pCICU, pediatric cardiac intensive care unit; RFB, retained foreign body; SA, situational awareness; SBAR, Situation, Background, Assessment, Recommendation; SI, severity index; TRM, team resource management; VA, Veterans Affair; VTE, venous thromboembolism; WAOS, weighted adverse outcome score; WHO, World Health Organization; WSS, wrong site surgery.
RESULTS: PHASE 2: COMPREHENSIVE CRM LITERATURE REVIEW
Taking a closer look at those 106 articles, there are 3 main findings: (1) effect of the training and its sustainability, (2) implementation, and (3) variation.
The Effect of CRM Training and Its Sustainability
All studies included in our comprehensive review presented evidence that CRM had a positive effect on an outcome measure within at least 1 Kirkpatrick level. In particular, CRM seems to positively affect level 1 (i.e., reaction) and 2 (i.e., learning), based on the high quantity of articles and the quality of the evidence noted. Likewise, the effects of CRM interventions on level 3 outcomes (i.e., behavior) are promising. However, we have to note that level 3 sometimes included the perception of behavioral change and was sometimes obtained by observations. In addition, whether CRM affects outcomes at level 4 (i.e., organizational outcome) remains unclear. Only 28 articles included level 4 in their evaluation, and the results here were mixed.
Although most studies presented a positive effect of CRM, this statement requires nuancing. First, the period in which the positive effects occurred varied from directly after the training to 4 years after the training112 Likewise, the number of measurements varied between 1 and 3 (after intervention). Although all positive measured effects are valuable, the sustainability of these effects is equally important. Only half of the studies offered some form of sustainability intervention. Second, most studies measured multiple nontechnical skills and always reported 1 or more significant effects, but also some nonsignificant effects. Across the studies, it is not consistent as to which nontechnical skills are significant and which are not. Third, a couple of valuable outcomes were not measured. Specifically, there are no studies included in our review that described the return of investment as an outcome of a CRM intervention.17 This gap is interesting given that within the healthcare setting where budget constraints have a high priority, this is a relevant outcome measure. Likewise, outcomes related to the well-being of caregivers are scarce. In healthcare settings where the physical and especially the emotional burden is perceived to be high, this is a valuable outcome measure for future researchers in this area to consider.
Implementation of CRM Training
Our review of the CRM literature also highlights that most articles present limited information on the implementation strategy of CRM interventions. That said, of the information provided, there seems to be a high level of variety in the implementation strategies that are leveraged. Information on the possibility to participate in the training was most frequently presented (e.g., CRM training that was offered during working hours, compensating the hours spent within CRM training, or providing multiple possibilities to follow the training). In addition, the status of the CRM training was frequently discussed. For instance, examples include the priority status within an organization and department or if the training was compulsory or voluntary. In addition, in a few cases, an implementation team was composed as part of the implementation strategy. However, it remains an unanswered question as to the impact of how such interventions are implemented and what some potential pitfalls may be from implementing CRM. Likewise, although Weaver et al28 (2014) noted that CRM is often implemented as a bundle of initiatives, research has yet to fully consider whether or when certain bundles represent deadly combinations rather than resulting in synergistic effects for the caregivers, patients, and healthcare organizations.
Variation
Although there is variation in what the CRM training entailed, most CRM training interventions seem to start with a didactic element (e.g., lecture, e-learning) combined with a form of simulation (e.g., high-fidelity simulator) and debriefing. The duration varied between 1/2 day and a couple of weeks. In addition to the variations present during the training, there is variation before (i.e., implementation strategy) and after (i.e., sustainability elements) the training intervention. The question remains whether and how these differences matter. Likewise, research has yet to truly address which CRM elements are best practices and which should be adjusted to create a best fit. Although such variation is typically viewed in a negative light, it can also be a good thing as evidenced by Tschannen et al126 (2015) who showed that a tailored CRM training for nurses, the so-called nursing CRM, indicated a culture change and a more permanent effect. This study is especially valuable as it is focused on a relatively novel area for CRM research (nursing teams).
Conclusion Phase 2
Based on our new and more comprehensive literature review, we can clearly state that CRM seems to have a positive effect on Kirkpatrick’s level 1, 2, and 3. However, effects on level 3 were not only obtained through observations but also through the perception of participants. Whether CRM has a positive effect on level 4 outcomes and how level 4 should be measured remain undetermined. Likewise, the precise manner in which to implement and embed CRM training into the organization so that the desired effects will occur and will be sustained should be given more research attention. Furthermore, future research attention is needed on how long the positive effects will sustain and what the critical factors are to sustain the effects of CRM training interventions.
DISCUSSION AND CONCLUSIONS
The extensive nature of this review demonstrates that a significant number of studies have been conducted over the past decade looking at the effects of CRM in healthcare. At the same time, our review highlights that this research tends to be situated within certain settings (i.e., acute hospital setting) and focused on particular outcomes (i.e., perceived nontechnical skills and team functioning). Accordingly, this suggests that research in this area has provided evidence that CRM is most likely to improve outcomes at Kirkpatrick’s level 1, 2, and 3. However, our review also indicates that there are several gaps that remain within the CRM literature. Therefore, future research should attempt to more fully capture the complete picture of CRM in healthcare.
The first gap that we identified based on our review is that rather than focusing exclusively on the results of a CRM intervention at the 4 Kirkpatrick’s levels, research should also examine the means by which to actually sustain these effects. In particular, studies should measure the extent to which the results of a CRM intervention can be sustained and what factors should be implemented to enhance the gains derived from a CRM intervention over longer periods. In addition, research on the content of sustainability strategies on CRM is needed. Sustainability strategies are needed to adapt the intervention and implementation strategies to the needs and feedback of the professionals, thus building employee engagement and ensuring the long-term success of an intervention.137 In part, such strategies may increase the variability noted within the CRM literature as the factors that assist with sustaining the benefits of CRM interventions may need to be tailored to the particular organization and its context.
The second gap that we identified is the lack of information about the importance that CRM should not be viewed as an isolated intervention but as an element of a broader Human Resource (HR) strategy in which other elements reinforce the attended changes. Research should provide insights in which HR practices (e.g., appraisal, feedback, other training) reinforce or diminish the effect of CRM. Likewise, research should consider whether certain combinations of HR practices and CRM interventions result in a “deadly combination” and thereby actually have detrimental effects. To date, most studies within the CRM literature provided too little information about the context in which CRM is implemented. To truly understand why and how CRM affects (all 4 Kirkpatrick’s levels) outcomes and be able to replicate the effect (by researchers and practitioners), detailed information is required related to the context in terms of implementation process and content of HR strategies.
Limitations
Although we did our best to be as inclusive as possible with our review of the CRM literature, we excluded certain articles because we only focused on articles written in English that presented empirical data and were published in peer-reviewed journals. Consequently, we might have excluded studies that present negative or nonsignificant effects of CRM, also known as the publication bias.138 In addition, given that our focus was only CRM, we did not include related interventions such as TeamSTEPPS or interventions that focused on only 1 element of CRM such as simulation training as CRM is a multifaceted intervention.
ACKNOWLEDGMENT
The authors thank Dr Wichor Bramer, Librarian at the Erasmus Medical Centre Rotterdam, the Netherlands, for his support in conducting the search for this review.
Footnotes
The authors disclose no conflict of interest.
Each author gave his/her final approval of the version to be published and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Supplemental digital contents are available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s Web site (www.journalpatientsafety.com).
Contributor Information
Connie M. Dekker-van Doorn, Email: c.m.dekker-van.doorn@hr.nl.
M. Travis Maynard, Email: Travis.Maynard@business.colostate.edu.
REFERENCES
- 1.Britnell M. Human: Solving the Global Workforce Crisis in Healthcare. Oxford: Oxford University Press; 2019. [Google Scholar]
- 2.Rosen MA DiazGranados D Dietz AS, et al. Teamwork in healthcare: key discoveries enabling safer, high-quality care. Am Psychol. 2018;73:433–450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Donaldson MS, Corrigan JM, Kohn LT, eds. To Err Is Human: Building a Safer Health System. Washington, DC: National Academies Press; 2000:6. [PubMed] [Google Scholar]
- 4.Corrigan JM. Crossing the Quality Chasm: Building a Better Delivery System. Washington, DC: National Academies Press; 2005. [Google Scholar]
- 5.Hughes AM Gregory ME Joseph DL, et al. Saving lives: a meta-analysis of team training in healthcare. J Appl Psychol. 2016;101:1266–1304. [DOI] [PubMed] [Google Scholar]
- 6.Flin R, Maran N. Basic concepts for crew resource management and non-technical skills. Best Pract Res Clin Anaesthesiol. 2015;29:27–39. [DOI] [PubMed] [Google Scholar]
- 7.O’dea A, O’Connor P, Keogh I. A meta-analysis of the effectiveness of crew resource management training in acute care domains. Postgrad Med J. 2014;90:699–708. [DOI] [PubMed] [Google Scholar]
- 8.Lauber JK. Resource management in the cockpit. Air Line Pilot. 1984;53:20–23. [Google Scholar]
- 9.Salas E Wilson KA Murphy CE, et al. What crew resource management training will not do for patient safety: unless. J Patient Saf. 2007;3:62–64. [Google Scholar]
- 10.Helmreich RL, Merritt AC, Wilhelm JA. The evolution of crew resource management training in commercial aviation. Int J Aviat Psychol. 1999;9:19–32. [DOI] [PubMed] [Google Scholar]
- 11.Gross B Rusin L Kiesewetter J, et al. Crew resource management training in healthcare: a systematic review of intervention design, training conditions and evaluation. BMJ Open. 2019;9:e025247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Verbeek-van Noord I de Bruijne MC Zwijnenberg NC, et al. Does classroom-based crew resource management training improve patient safety culture? A systematic review. SAGE Open Med. 2014;2:205031211452956. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.McCulloch P Mishra A Handa A, et al. The effects of aviation-style non-technical skills training on technical performance and outcome in the operating theatre. Qual Saf Health Care. 2009;18:109–115. [DOI] [PubMed] [Google Scholar]
- 14.Watts BV Percarpio K West P, et al. Use of the Safety Attitudes Questionnaire as a measure in patient safety improvement. J Patient Saf. 2010;6:206–209. [DOI] [PubMed] [Google Scholar]
- 15.Aromataris E Fernandez R Godfrey CM, et al. Summarizing systematic reviews: methodological development, conduct and reporting of an umbrella review approach. Int J Evid Based Healthc. 2015;13:132–140. [DOI] [PubMed] [Google Scholar]
- 16.Boet S Bould MD Fung L, et al. Transfer of learning and patient outcome in simulated crisis resource management: a systematic review. Can J Anaesth. 2014;61:571–582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fung L Boet S Bould MD, et al. Impact of crisis resource management simulation-based training for interprofessional and interdisciplinary teams: a systematic review. J Interprof Care. 2015;29:433–444. [DOI] [PubMed] [Google Scholar]
- 18.Maynard MT, Marshall D, Dean MD. Crew resource management and teamwork training in health care: a review of the literature and recommendations for how to leverage such interventions to enhance patient safety. Adv Health Care Manag. 2012;59–91. [DOI] [PubMed] [Google Scholar]
- 19.O’Connor P Campbell J Newon J, et al. Crew resource management training effectiveness: a meta-analysis and some critical needs. Int J Aviat Psychol. 2008;18:353–368. [Google Scholar]
- 20.Salas E Wilson KA Burke CS, et al. Does crew resource management training work? An update, an extension, and some critical needs. Hum Factors. 2006;48:392–412. [DOI] [PubMed] [Google Scholar]
- 21.Zeltser MV, Nash DB. Approaching the evidence basis for aviation-derived teamwork training in medicine. Am J Med Qual. 2010;25:13–23. [DOI] [PubMed] [Google Scholar]
- 22.Doumouras AG Keshet I Nathens AB, et al. A crisis of faith? A review of simulation in teaching team-based, crisis management skills to surgical trainees. J Surg Educ. 2012;69:274–281. [DOI] [PubMed] [Google Scholar]
- 23.Murphy M, Curtis K, McCloughen A. What is the impact of multidisciplinary team simulation training on team performance and efficiency of patient care? An integrative review. Australas Emerg Nurs J. 2016;19:44–53. [DOI] [PubMed] [Google Scholar]
- 24.Tan SB Pena G Altree M, et al. Multidisciplinary team simulation for the operating theatre: a review of the literature. ANZ J Surg. 2014;84:515–522. [DOI] [PubMed] [Google Scholar]
- 25.Buljac-Samardzic M Dekker-van Doorn CM van Wijngaarden JD, et al. Interventions to improve team effectiveness: a systematic review. Health Policy. 2010;94:183–195. [DOI] [PubMed] [Google Scholar]
- 26.Low XM, Horrigan D, Brewster DJ. The effects of team-training in intensive care medicine: a narrative review. J Crit Care. 2018;48:283–289. [DOI] [PubMed] [Google Scholar]
- 27.McCulloch P, Rathbone J, Catchpole K. Interventions to improve teamwork and communications among healthcare staff. Br J Surg. 2011;98:469–479. [DOI] [PubMed] [Google Scholar]
- 28.Weaver SJ, Dy SM, Rosen MA. Team-training in healthcare: a narrative synthesis of the literature. BMJ Qual Saf. 2014;23:359–372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Shea BJ Grimshaw JM Wells GA, et al. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol. 2007;7:10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Salas E Prince C Bowers C, et al. A methodology for enhancing crew resource management training. Hum Factors. 1999;41:161–172. [Google Scholar]
- 31.Haerkens MH Kox M Lemson J, et al. Crew resource management in the intensive care unit: a prospective 3-year cohort study. Acta Anaesthesiol Scand. 2015;59:1319–1329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kemper PF de Bruijne M van Dyck C, et al. Crew resource management training in the intensive care unit. A multisite controlled before-after study. BMJ Qual Saf. 2016;25:577–587. [DOI] [PubMed] [Google Scholar]
- 33.Nielsen PE Goldman MB Mann S, et al. Effects of teamwork training on adverse outcomes and process of care in labor and delivery: a randomized controlled trial. Obstet Gynecol. 2007;109:48–55. [DOI] [PubMed] [Google Scholar]
- 34.Allan CK Thiagarajan RR Beke D, et al. Simulation-based training delivered directly to the pediatric cardiac intensive care unit engenders preparedness, comfort, and decreased anxiety among multidisciplinary resuscitation teams. J Thorac Cardiovasc Surg. 2010;140:646–652. [DOI] [PubMed] [Google Scholar]
- 35.Atamanyuk I Ghez O Saeed I, et al. Impact of an open-chest extracorporeal membrane oxygenation model for in situ simulated team training: a pilot study. Interact Cardiovasc Thorac Surg. 2014;18:17–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ballangrud R Hall-Lord ML Persenius M, et al. Intensive care nurses’ perceptions of simulation-based team training for building patient safety in intensive care: a descriptive qualitative study. Intensive Crit Care Nurs. 2014;30:179–187. [DOI] [PubMed] [Google Scholar]
- 37.Ballangrud R Hall-Lord ML Hedelin B, et al. Intensive care unit nurses’ evaluation of simulation used for team training. Nurs Crit Care. 2014;19:175–184. [DOI] [PubMed] [Google Scholar]
- 38.Bank I, Snell L, Bhanji F. Pediatric crisis resource management training improves emergency medicine trainees’ perceived ability to manage emergencies and ability to identify teamwork errors. Pediatr Emerg Care. 2014;30:879–883. [DOI] [PubMed] [Google Scholar]
- 39.Batchelder AJ Steel A Mackenzie R, et al. Simulation as a tool to improve the safety of pre-hospital anaesthesia—a pilot study. Anaesthesia. 2009;64:978–983. [DOI] [PubMed] [Google Scholar]
- 40.Blackwood J Duff JP Nettel-Aguirre A, et al. Does teaching crisis resource management skills improve resuscitation performance in pediatric residents? Pediatr Crit Care Med. 2014;15:e168–e174. [DOI] [PubMed] [Google Scholar]
- 41.Budin WC Gennaro S O’connor C, et al. Sustainability of improvements in perinatal teamwork and safety climate. J Nurs Care Qual. 2014;29:363–370. [DOI] [PubMed] [Google Scholar]
- 42.Burden AR Pukenas EW Deal ER, et al. Using simulation education with deliberate practice to teach leadership and resource management skills to senior resident code leaders. J Grad Med Educ. 2014;6:463–469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Carbo AR Tess AV Roy C, et al. Developing a high-performance team training framework for internal medicine residents: the ABC’S of teamwork. J Patient Saf. 2011;7:72–76. [DOI] [PubMed] [Google Scholar]
- 44.Carpenter JE Bagian JP Snider RG, et al. Medical team training improves team performance: AOA critical issues. J Bone Joint Surg Am. 2017;99:1604–1610. [DOI] [PubMed] [Google Scholar]
- 45.Castelao EF Russo SG Cremer S, et al. Positive impact of crisis resource management training on no-flow time and team member verbalisations during simulated cardiopulmonary resuscitation: a randomised controlled trial. Resuscitation. 2011;82:1338–1343. [DOI] [PubMed] [Google Scholar]
- 46.Castelao EF Boos M Ringer C, et al. Effect of CRM team leader training on team performance and leadership behaviour in simulated cardiac arrest scenarios: a prospective, randomized, controlled study. BMC Med Educ. 2015;15:116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Catchpole KR Dale TJ Hirst DG, et al. A multicenter trial of aviation-style training for surgical teams. J Patient Saf. 2010;6:180–186. [DOI] [PubMed] [Google Scholar]
- 48.Chan CKW So EHK Ng GWY, et al. Participant evaluation of simulation training using crew resource management in a hospital setting in Hong Kong. Hong Kong Med J. 2016;22:131–137. [DOI] [PubMed] [Google Scholar]
- 49.Chan CK So HK Ng WY, et al. Does classroom-based crew resource management training have an effect on attitudes between doctors and nurses? Int J Med Educ. 2016;7:109–114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Ciporen J Gillham H Noles M, et al. Crisis management simulation: establishing a dual neurosurgery and anesthesia training experience. J Neurosurg Anesthesiol. 2018;30:65–70. [DOI] [PubMed] [Google Scholar]
- 51.Clarke S Horeczko T Carlisle M, et al. Emergency medicine resident crisis resource management ability: a simulation-based longitudinal study. Med Educ Online. 2014;19:25771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Clay-Williams R Mcintosh CA Kerridge R, et al. Classroom and simulation team training: a randomized controlled trial. Int J Qual Health Care. 2013;25:314–321. [DOI] [PubMed] [Google Scholar]
- 53.Clay-Williams R Greenfield D Stone J, et al. On a wing and a prayer: an assessment of modularized crew resource management training for health care professionals. J Contin Educ Health Prof. 2014;34:56–67. [DOI] [PubMed] [Google Scholar]
- 54.Clay-Williams R, Braithwaite J. Reframing implementation as an organisational behaviour problem: inside a teamwork improvement intervention. J Health Organ Manag. 2015;29:670–683. [DOI] [PubMed] [Google Scholar]
- 55.Cooper JB Blum RH Carroll JS, et al. Differences in safety climate among hospital anesthesia departments and the effect of a realistic simulation-based training program. Anesth Analg. 2008;106:574–584. [DOI] [PubMed] [Google Scholar]
- 56.Coppens I Verhaeghe S Van Hecke A, et al. The effectiveness of crisis resource management and team debriefing in resuscitation education of nursing students: a randomised controlled trial. J Clin Nurs. 2018;27:77–85. [DOI] [PubMed] [Google Scholar]
- 57.de Korne DF van Wijngaarden JDH van Dyck C, et al. Evaluation of aviation-based safety team training in a hospital in the Netherlands. J Health Organ Manag. 2014;28:731–753. [DOI] [PubMed] [Google Scholar]
- 58.Duclos A Peix JL Piriou V, et al. Cluster randomized trial to evaluate the impact of team training on surgical outcomes. Br J Surg. 2016;103:1804–1814. [DOI] [PubMed] [Google Scholar]
- 59.Emani SS Allan CK Forster T, et al. Simulation training improves team dynamics and performance in a low-resource cardiac intensive care unit. Ann Pediatr Cardiol. 2018;11:130–136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Falcone RA Jr. Daugherty M Schweer L, et al. Multidisciplinary pediatric trauma team training using high-fidelity trauma simulation. J Pediatr Surg. 2008;43:1065–1071. [DOI] [PubMed] [Google Scholar]
- 61.Fore AM Sculli GL Albee D, et al. Improving patient safety using the sterile cockpit principle during medication administration: a collaborative, unit-based project. J Nurs Manag. 2013;21:106–111. [DOI] [PubMed] [Google Scholar]
- 62.France DJ Leming-Lee S Jackson T, et al. An observational analysis of surgical team compliance with perioperative safety practices after crew resource management training. Am J Surg. 2008;195:546–553. [DOI] [PubMed] [Google Scholar]
- 63.Fransen AF van de Ven J Schuit E, et al. Simulation-based team training for multi-professional obstetric care teams to improve patient outcome: a multicentre, cluster randomised controlled trial. BJOG. 2017;124:641–650. [DOI] [PubMed] [Google Scholar]
- 64.Gallagher D. Crew resource management... following up. Nurs Manage. 2016;47:50–54. [DOI] [PubMed] [Google Scholar]
- 65.Gillespie BM Harbeck E Kang E, et al. Effects of a brief team training program on surgical teams’ nontechnical skills: an interrupted time-series study. J Patient Saf. 2017. [DOI] [PubMed] [Google Scholar]
- 66.Gillespie BM Steel C Kang E, et al. Evaluation of a brief team training intervention in surgery: a mixed-methods study. AORN J. 2017;106:513–522. [DOI] [PubMed] [Google Scholar]
- 67.Gillman LM Brindley P Paton-Gay JD, et al. Simulated Trauma and Resuscitation Team Training course—evolution of a multidisciplinary trauma crisis resource management simulation course. Am J Surg. 2016;212:188–193.e3. [DOI] [PubMed] [Google Scholar]
- 68.Gore DC Powell JM Baer JG, et al. Crew resource management improved perception of patient safety in the operating room. Am J Med Qual. 2010;25:60–63. [DOI] [PubMed] [Google Scholar]
- 69.Gross B Rusin L Kiesewetter J, et al. Microlearning for patient safety: crew resource management training in 15-minutes. PLoS One. 2019;14:e0213178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Guerlain S Turrentine FE Bauer DT, et al. Crew resource management training for surgeons: feasibility and impact. Cognit Technol Work. 2008;10:255–264. [Google Scholar]
- 71.Haerkens MHTM Kox M Noe PM, et al. Crew resource management in the trauma room: a prospective 3-year cohort study. Eur J Emerg Med. 2018;25:281–287. [DOI] [PubMed] [Google Scholar]
- 72.Haffner L Mahling M Muench A, et al. Improved recognition of ineffective chest compressions after a brief crew resource management (CRM) training: a prospective, randomised simulation study. BMC Emerg Med. 2017;17:7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Haller G Garnerin P Morales MA, et al. Effect of crew resource management training in a multidisciplinary obstetrical setting. Int J Qual Health Care. 2008;20:254–263. [DOI] [PubMed] [Google Scholar]
- 74.Hänsel M Winkelmann AM Hardt F, et al. Impact of simulator training and crew resource management training on final-year medical students’ performance in sepsis resuscitation: a randomized trial. Minerva Anestesiol. 2012;78:901–909. [PubMed] [Google Scholar]
- 75.Hansen KS Uggen PE Brattebø G, et al. Training operating room teams in damage control surgery for trauma: a follow up study of the Norwegian model. J Am Coll Surg. 2007;205:712–716. [DOI] [PubMed] [Google Scholar]
- 76.Hansen KS Uggen PE Brattebø G, et al. Team-oriented training for damage control surgery in rural trauma: a new paradigm. J Trauma. 2008;64:949–953. [DOI] [PubMed] [Google Scholar]
- 77.Hay JM, Barnette W, Shaw SE. Changing practice in gastrointestinal endoscopy. Gastroenterol Nurs. 2016;39:181–185. [DOI] [PubMed] [Google Scholar]
- 78.Hefner JL Hilligoss B Knupp A, et al. Cultural transformation after implementation of crew resource management: is it really possible? Am J Med Qual. 2017;32:384–390. [DOI] [PubMed] [Google Scholar]
- 79.Hicks CM Kiss A Bandiera GW, et al. Crisis Resources for Emergency Workers (CREW II): results of a pilot study and simulation-based crisis resource management course for emergency medicine residents. CJEM. 2012;14:354–362. [DOI] [PubMed] [Google Scholar]
- 80.Hughes KM Benenson RS Krichten AE, et al. A crew resource management program tailored to trauma resuscitation improves team behavior and communication. J Am Coll Surg. 2014;219:545–551. [DOI] [PubMed] [Google Scholar]
- 81.Jankouskas T Bush MC Murray B, et al. Crisis resource management: evaluating outcomes of a multidisciplinary team. Simul Healthc. 2007;2:96–101. [DOI] [PubMed] [Google Scholar]
- 82.Jankouskas TS Haidet KK Hupcey JE, et al. Targeted crisis resource management training improves performance among randomized nursing and medical students. Simul Healthc. 2011;6:316–326. [DOI] [PubMed] [Google Scholar]
- 83.Kemper PF van Dyck C Wagner C, et al. Barriers and facilitators for taking action after classroom-based crew resource management training at three ICUs. Jt Comm J Qual Patient Saf. 2014;40:311–318. [DOI] [PubMed] [Google Scholar]
- 84.Kuy S, Romero RA. Eliminating critical incident tracking network patient safety events at a Veterans Affairs Institution through Crew Resource Management Training. Am J Med Qual. 2017;32:480–484. [DOI] [PubMed] [Google Scholar]
- 85.Kuy S, Romero RAL. Improving staff perception of a safety climate with crew resource management training. J Surg Res. 2017;213:177–183. [DOI] [PubMed] [Google Scholar]
- 86.LaPoint JL. The effects of aviation error management training on perioperative safety attitudes. Int J Bus Soc Sci. 2012;3. [Google Scholar]
- 87.Lehner M Heimberg E Hoffmann F, et al. Evaluation of a pilot project to introduce simulation-based team training to pediatric surgery trauma room care. Int J Pediatr. 2017;2017:9732316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Mah JW Bingham K Dobkin ED, et al. Mannequin simulation identifies common surgical intensive care unit teamwork errors long after introduction of sepsis guidelines. Simul Healthc. 2009;4:193–199. [DOI] [PubMed] [Google Scholar]
- 89.Mahramus TL Penoyer DA Waterval EM, et al. Two hours of teamwork training improves teamwork in simulated cardiopulmonary arrest events. Clin Nurse Spec. 2016;30:284–291. [DOI] [PubMed] [Google Scholar]
- 90.Man APN Lam CKM Cheng BCP, et al. Impact of locally adopted simulation-based crew resource management training on patient safety culture: comparison between operating room personnel and general health care populations pre and post course. Am J Med Qual. 2020;35:79–88. [DOI] [PubMed] [Google Scholar]
- 91.Mancuso MP Dziadkowiec O Kleiner C, et al. Crew resource management for obstetric and neonatal teams to improve communication during cesarean births. J Obstet Gynecol Neonatal Nurs. 2016;45:502–514. [DOI] [PubMed] [Google Scholar]
- 92.Marshall DA, Manus DA. A team training program using human factors to enhance patient safety. AORN J. 2007;86:994–1011. [DOI] [PubMed] [Google Scholar]
- 93.Mitchell P, Dale T. Side errors in neurosurgery and human factors training. Acta Neurochir. 2015;157:487–491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Moffatt-Bruce SD Hefner JL Mekhjian H, et al. What is the return on investment for implementation of a crew resource management program at an academic medical center? Am J Med Qual. 2017;32:5–11. [DOI] [PubMed] [Google Scholar]
- 95.Morgan PJ Tarshis J LeBlanc V, et al. Efficacy of high-fidelity simulation debriefing on the performance of practicing anaesthetists in simulated scenarios. Br J Anaesth. 2009;103:531–537. [DOI] [PubMed] [Google Scholar]
- 96.Morgan PJ Kurrek MM Bertram S, et al. Nontechnical skills assessment after simulation-based continuing medical education. Simul Healthc. 2011;6:255–259. [DOI] [PubMed] [Google Scholar]
- 97.Morgan L Pickering SP Hadi M, et al. A combined teamwork training and work standardisation intervention in operating theatres: controlled interrupted time series study. BMJ Qual Saf. 2015;24:111–119. [DOI] [PubMed] [Google Scholar]
- 98.Müller MP Hänsel M Stehr SN, et al. Six steps from head to hand: a simulator based transfer oriented psychological training to improve patient safety. Resuscitation. 2007;73:137–143. [DOI] [PubMed] [Google Scholar]
- 99.Müller MP Hänsel M Fichtner A, et al. Excellence in performance and stress reduction during two different full scale simulator training courses: a pilot study. Resuscitation. 2009;80:919–924. [DOI] [PubMed] [Google Scholar]
- 100.Neily J Mills PD Lee P, et al. Medical team training and coaching in the veterans health administration; assessment and impact on the first 32 facilities in the programme. Qual Saf Health Care. 2010;19:360–364. [DOI] [PubMed] [Google Scholar]
- 101.Neily J Mills PD Young-Xu Y, et al. Association between implementation of a medical team training program and surgical mortality. JAMA. 2010;304:1693–1700. [DOI] [PubMed] [Google Scholar]
- 102.Nishisaki A Hales R Biagas K, et al. A multi-institutional high-fidelity simulation “boot camp” orientation and training program for first year pediatric critical care fellows. Pediatr Crit Care Med. 2009;10:157–162. [DOI] [PubMed] [Google Scholar]
- 103.O’Connor P Byrne D O’dea A, et al. “Excuse me:” teaching interns to speak up. Jt Comm J Qual Patient Saf. 2013;39:426–431. [DOI] [PubMed] [Google Scholar]
- 104.Parsons JR Crichlow A Ponnuru S, et al. Filling the gap: simulation-based crisis resource management training for emergency medicine residents. West J Emerg Med. 2018;19:205–210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Paull DE DeLeeuw LD Wolk S, et al. The effect of simulation-based crew resource management training on measurable teamwork and communication among interprofessional teams caring for postoperative patients. J Contin Educ Nurs. 2013;44:516–524. [DOI] [PubMed] [Google Scholar]
- 106.Phipps MG Lindquist DG McConaughey E, et al. Outcomes from a labor and delivery team training program with simulation component. Am J Obstet Gynecol. 2012;206:3–9. [DOI] [PubMed] [Google Scholar]
- 107.Pratt SD Mann S Salisbury M, et al. John M. Eisenberg Patient Safety and Quality Awards. Impact of CRM-based training on obstetric outcomes and clinicians’ patient safety attitudes. Jt Comm J Qual Patient Saf. 2007;33:720–725. [DOI] [PubMed] [Google Scholar]
- 108.Rêgo P Walker K Thompson A, et al. Being ready on the day... a short report on the evaluation and outcomes of a pilot ambulatory surgery crisis resource management course. Ambulatory. 2008;14:90–93. [Google Scholar]
- 109.Ricci MA, Brumsted JR. Crew resource management: using aviation techniques to improve operating room safety. Aviat Space Environ Med. 2012;83:441–444. [DOI] [PubMed] [Google Scholar]
- 110.Rovamo L Nurmi E Mattila M-M, et al. Effect of a simulation-based workshop on multidisplinary teamwork of newborn emergencies: an intervention study. BMC Res Notes. 2015;8:671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Sandahl C Gustafsson H Wallin CJ, et al. Simulation team training for improved teamwork in an intensive care unit. Int J Health Care Qual Assur. 2013;26:174–188. [DOI] [PubMed] [Google Scholar]
- 112.Savage C Gaffney FA Hussain-Alkhateeb L, et al. Safer paediatric surgical teams: a 5-year evaluation of crew resource management implementation and outcomes. Int J Qual Health Care. 2017;29:853–860. [DOI] [PubMed] [Google Scholar]
- 113.Sax HC Browne P Mayewski RJ, et al. Can aviation-based team training elicit sustainable behavioral change? Arch Surg. 2009;144:1133–1137. [DOI] [PubMed] [Google Scholar]
- 114.Schwartz ME Welsh DE Paull DE, et al. The effects of crew resource management on teamwork and safety climate at Veterans Health Administration facilities. J Healthc Risk Manag. 2018;38:17–37. [DOI] [PubMed] [Google Scholar]
- 115.Sculli GL Fore AM Neily J, et al. The case for training Veterans Administration frontline nurses in crew resource management. J Nurs Adm. 2011;41:524–530. [DOI] [PubMed] [Google Scholar]
- 116.Shea-Lewis A. Teamwork: crew resource management in a community hospital. J Healthc Qual. 2009;31:14–18. [DOI] [PubMed] [Google Scholar]
- 117.Siems A Cartron A Watson A, et al. Improving pediatric rapid response team performance through crew resource management training of team leaders. Hosp Pediatr. 2017;7:88–95. [DOI] [PubMed] [Google Scholar]
- 118.Stocker M Allen M Pool N, et al. Impact of an embedded simulation team training programme in a paediatric intensive care unit: a prospective, single-centre, longitudinal study. Intensive Care Med. 2012;38:99–104. [DOI] [PubMed] [Google Scholar]
- 119.Sundararaman S Babbo AE Brown JA, et al. Improving patient safety in the radiation oncology setting through crew resource management. Pract Radiat Oncol. 2014;4:e181–e188. [DOI] [PubMed] [Google Scholar]
- 120.Suva D Haller G Lübbeke A, et al. Differential impact of a crew resource management program according to professional specialty. Am J Med Qual. 2012;27:313–320. [DOI] [PubMed] [Google Scholar]
- 121.Sweeney LA Warren O Gardner L, et al. A simulation-based training program improves emergency department staff communication. Am J Med Qual. 2014;29:115–123. [DOI] [PubMed] [Google Scholar]
- 122.Tapson VF, Bongiorno Karcher R, Weeks R. Crew resource management and VTE prophylaxis in surgery: a quality improvement initiative. Am J Med Qual. 2011;26:423–432. [DOI] [PubMed] [Google Scholar]
- 123.Taylor CR Hepworth JT Buerhaus PI, et al. Effect of crew resource management on diabetes care and patient outcomes in an inner-city primary care clinic. Qual Saf Health Care. 2007;16:244–247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Truijens SEM Banga FR Fransen AF, et al. The effect of multiprofessional simulation-based obstetric team training on patient-reported quality of care: a pilot study. Simul Healthc. 2015;10:210–216. [DOI] [PubMed] [Google Scholar]
- 125.Truta TS Boeriu CM Copotoiu SM, et al. Improving nontechnical skills of an interprofessional emergency medical team through a one day crisis resource management training. Medicine (Baltimore). 2018;97:e11828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Tschannen D McClish D Aebersold M, et al. Targeted communication intervention using nursing crew resource management principles. J Nurs Care Qual. 2015;30:7–11. [DOI] [PubMed] [Google Scholar]
- 127.Tschannen D, Dorn R, Tedesco C. Improving knowledge and behavior of leadership and followership among the interprofessional team. Int J Med Educ. 2018;9:182–188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Turkelson C Aebersold M Redman R, et al. Improving nursing communication skills in an intensive care unit using simulation and nursing crew resource management strategies. J Nurs Care Qual. 2017;32:331–339. [DOI] [PubMed] [Google Scholar]
- 129.Verbeek-van Noord I de Bruijne MC Twisk JWR, et al. More explicit communication after classroom-based crew resource management training: results of a pragmatic trial. J Eval Clin Pract. 2015;21:137–144. [DOI] [PubMed] [Google Scholar]
- 130.West P Sculli G Fore A, et al. Improving patient safety and optimizing nursing teamwork using crew resource management techniques. J Nurs Adm. 2012;42:15–20. [DOI] [PubMed] [Google Scholar]
- 131.Westfelt P Hedman L Axelsson Lindkvist M, et al. Training nonanesthetist administration of propofol for gastrointestinal endoscopy in scenario-based full-scale hybrid simulation—a pilot study. Scand J Gastroenterol. 2013;48:1354–1358. [DOI] [PubMed] [Google Scholar]
- 132.Wetzel EA Lang TR Pendergrass TL, et al. Identification of latent safety threats using high-fidelity simulation-based training with multidisciplinary neonatology teams. Jt Comm J Qual Patient Saf. 2013;39:268–273. [DOI] [PubMed] [Google Scholar]
- 133.Wu W-T Wu Y-L Hou S-M, et al. Examining the effects of an interprofessional crew resource management training intervention on perceptions of patient safety. J Interprof Care. 2016;30:536–538. [DOI] [PubMed] [Google Scholar]
- 134.Zech A Gross B Jasper-Birzele C, et al. Evaluation of simparteam—a needs-orientated team training format for obstetrics and neonatology. J Perinat Med. 2017;45:333–341. [DOI] [PubMed] [Google Scholar]
- 135.Ziesmann MT Widder S Park J, et al. S.T.A.R.T.T.: development of a national, multidisciplinary trauma crisis resource management curriculum—results from the pilot course. J Trauma Acute Care Surg. 2013;75:753–758. [DOI] [PubMed] [Google Scholar]
- 136.Pluye P Robert E Cargo M, et al. Proposal: a mixed methods appraisal tool for systematic mixed studies reviews. 2011. Available at: http://mixedmethodsappraisaltoolpublic.pbworks.com. Accessed January 06, 2018.
- 137.Powell BJ Waltz TJ Chinman MJ, et al. A refined compilation of implementation strategies: results from the Expert Recommendations for Implementing Change (ERIC) project. Implement Sci. 2015;10:21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Dwan K Gamble C Williamson PR, et al. Systematic review of the empirical evidence of study publication bias and outcome reporting bias - an updated review. PLoS One. 2013;8:e66844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Kirkpatrick JD, Kirkpatrick WK. Kirkpatrick’s Four Levels of Training Evaluation. Alexandria, VA: ATD Press: 2016. [Google Scholar]