

Abstract
Purpose
To compare early postoperative outcomes after transversus abdominis release (TAR) for ventral hernia repair with open (oTAR) and robotic (rTAR) approach.
Methods
A systematic search of PubMed/MEDLINE, EMBASE, SCOPUS and Web of Science databases was conducted to identify comparative studies until October 2020. A meta-analysis of postoperative short-term outcomes was performed including complications rate, operative time, length of stay, surgical site infection (SSI), surgical site occurrence (SSO), SSO requiring intervention (SSOPI), systemic complications, readmission, and reoperation rates as measure outcomes.
Results
Six retrospective studies were included in the analysis with a total of 831 patients who underwent rTAR (n = 237) and oTAR (n = 594). Robotic TAR was associated with lower risk of complications rate (9.3 vs 20.7%, OR 0.358, 95% CI 0.218–0.589, p < 0.001), lower risk of developing SSO (5.3 vs 11.5%, OR 0.669, 95% CI 0.307–1.458, p = 0.02), lower risk of developing systemic complications (6.3 vs 26.5%, OR 0.208, 95% CI 0.100–0.433, p < 0.001), shorter hospital stay (SMD − 4.409, 95% CI − 6.000 to − 2.818, p < 0.001) but longer operative time (SMD 53.115, 95% CI 30.236–75.993, p < 0.01) compared with oTAR. There was no statistically significant difference in terms of SSI, SSOPI, readmission, and reoperation rates.
Conclusion
Robotic TAR improves recovery by adding the benefits of minimally invasive procedures when compared to open surgery. Although postoperative complications appear to decrease with a robotic approach, further studies are needed to support the real long-term and cost-effective advantages.
Keywords: Transversus abdominis release, Robotic TAR, Ventral hernia repair
Introduction
Incisional hernia is one of the most common complications following abdominal surgery, with a reported incidence of 3–13% [1]. Ventral hernia repair (VHR) including Primary Ventral Hernia (PVH) and Incisional Hernia (IH), with up to 350,000 procedures performed annually, remains one of the most common procedures performed by general surgeons, amounting over $3.4 billion dollars in health costs [2].
There has been a recent trend in hernia surgery to reconstruct abdominal wall defects by reestablishing the fascial edges to their normal anatomic position, through a retromuscular approach. The Rives-Stoppa technique has been adopted by the Americas Hernia Society as the gold standard procedure for VHR with a recurrence less than 5% [3, 4]. Transversus abdominis release (TAR) was introduced in 2012 as a modification of the Rives-Stoppa technique [4], and it has become one of the procedures of choice in case of wide and complex ventral hernias. Respect to other types of component separation, it seems to decrease the risk of wound morbidity and hernia recurrence. In the last years, some surgeons have begun to investigate the role of the mini-invasive approach in retromuscular repairs. While TAR has been described laparoscopically [5], it is rarely performed in this manner due to several limitations as ergonomic, mechanical, and technical.
With advances in robotic surgery, to combine the benefits of minimally invasive approach and TAR, robotic retromuscular repairs are increasingly being used to treat complex ventral hernias. Some recent studies suggested that robotic approach seems to have some benefits despite an hypothetical increase of health-system costs. Therefore, the purpose of this study was to compare clinical outcomes, through a systematic review with meta-analysis, of robotic TAR (rTAR) and Open TAR (oTAR) for VHR.
Materials and methods
Literature search and selection of primary studies
The strategy for building the evidence base for the assessment of the outcomes of rTAR versus oTAR was performed with a systematic review of the existing evidence in the literature, conducted in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines [6].
The systematic literature review was performed in PubMed/MEDLINE, EMBASE, SCOPUS and Cochrane databases to identify studies that compared outcomes of rTAR vs oTAR reinforcement from the beginning of indexing for each database till Sep 1, 2020. Bibliographic review of selected articles was assessed as secondary sources for full-length articles of studies. A literature search was performed and verified by 2 independent reviewers (R.P. and N.I.) using the following index terms: “transversus abdominis release” AND “robotic” OR “open” AND “abdominal wall reconstruction” OR “hernia”.
Eligibility criteria
Two reviewers (R.P. and N.I.) independently evaluated all the studies retrieved according to the eligibility criteria and any differences between the datasets were resolved by discussion. Studies were included if they met all of the following criteria: (1) case–control studies, randomized controlled trial (RCT), prospective or retrospective studies directly comparing rTAR and oTAR; (2) original studies published in a peer-reviewed journal; (3) studies involving adult patients (aged > 18 years). We excluded the articles if there was no sufficient documentation on—or no possibility to calculate—the percentage of postoperative complications (primary endpoint), if they were in languages other than English, if they were focused on pediatric patients. Narrative reviews, duplicate publications and editorials were also excluded.
Data extraction and management
Data were extracted independently and entered into standardized Excel spreadsheets (Microsoft Inc., Redmond, Washington, USA). Any disagreements were resolved through discussion. The following data were extracted from each study: first author, year of publication, study design, sample size, type of TAR (robotic or open), age, gender, BMI, ASA status, operative time (minutes), length of stay (LOS, days), post-operative complications, number of patients developing surgical site infection (SSI), surgical site occurrence (SSO), SSO requiring intervention, number of systemic complications, percentage of readmission and reoperation.
Primary study outcome was the assessment of post-operative complications rate in the two groups (rTAR vs oTAR) at the end of follow-up for each included study. Furthermore, secondary outcomes included the evaluation of differences in: operative time, SSI development, SSO, SSO requiring intervention (SSOPI), number of systemic complications, need for readmission and reoperation and LOS.
Statistical analysis
Statistical analyses were performed by using Comprehensive Meta-analysis Software version 3.0 (Biostat, Englewood, New Jersey, USA).
Heterogeneity was assessed by using Chi-squared statistics and I2 measure of inconsistency. The quality of the analyzed studies and publication bias was evaluated by two reviewers (R.P. and N.I) in consensus using a quality assessment tool for diagnostic accuracy studies (QUADAS-2) [7]. The risk of publication bias and concerns regarding the applicability of studies were then assessed by visually inspecting QUADAS-2 plots.
The meta-analysis was conducted using a fixed-effect model in the case of non-significant heterogeneity (p > 0.1), and a random effect model (DerSimonian–Laird method) when significant heterogeneity was present (p < 0.1). Corresponding forest plots were constructed for the pooled estimates of these outcomes and weight of individual studies are represented by the size of individual squares. The odds ratio (OR) was assessed for dichotomous outcomes, while standardized mean difference (SMD) with 95% confidence interval (CI) was estimated for continuous outcomes.
Furthermore, a random effect meta-regression was performed to evaluate possible patient (age, gender, comorbidities such as diabetes, BMI, respiratory diseases) or disease (type of hernia, hernia dimensions) or technical (use and type of mesh) variables able to impact upon the outcomes. Similarly, a random effect meta-regression was used to evaluate how the length of follow-up affected the primary outcome.
A p value < 0.05 was considered statistically significant for all outcomes.
Results
Figure 1 shows the PRISMA flow diagram of the literature selection process. The search strategy identified a total of 68 publications in the initial search. After the screening of title and abstract and removal of duplicates, 17 articles were selected for further review. After exclusion of 11 articles based on exclusion criteria, 6 studies were included in the meta-analysis [8–13].
Fig. 1.

Flow diagram of the search strategy and selection of studies included in the meta-analysis
In accordance with the inclusion criteria, all studies were retrospective case–control studies based on prospective maintained database.
Finally, a total of 831 patients who underwent TAR with a robotic approach (n = 237) or open approach (n = 594) were included in the meta-analysis. Table 1 shows the baseline characteristics of the studies included.
Table 1.
Details of studies selected for meta-analysis
| Authors | Study period | Study design | Sample size | Study group | Mean hernia width/length (cm) | Hybrid robotic repair | Robotic platform | Follow-up (days) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| rTAR | oTAR | rTAR | oTAR | |||||||
| Abdu et al. [8] | 2016–2018 | Retro–PSM | 380 | 95 | 285 | 12/19 | 12/19 | Yes | NR | 30 |
| Bittner et al. [9] | 2015–2016 | Retro | 102 | 26 | 76 | 12.3 ± 3/18.5 ± 5.1 | 13.7 ± 5.9/17.1 ± 7.1 | No | Da Vinci Si + Xi | 90 |
| Dauser et al. [10] | 2017–2019 | Retro | 26 | 16 | 10 | NR | NR | No | Da Vinci Si | 30 |
| Halka et al. [11] | 2013–2017 | Retro | 183 | 49 | 134 | 38.8 ± 6.7/41.6 ± 6.1 | 37.4 ± 8.3/42.2 ± 9.1 | Yes | Da Vinci Xi | 30 |
| Martin-del-Campo et al. [12] | 2015–2016 | Retro | 114 | 38 | 76 | 13.5 ± 4.5/NR | 13.5 ± 4.5/NR | No | NR | NR |
| Reeves et al. [13] | 2018–2020 | Retro | 26 | 13 | 13 | NR | NR | No | Da Vinci Xi | 30 |
rTAR robotic transversus abdominis release, oTAR open transversus abdominis release, NR not reported, Retro retrospective study, PSM propensity score matching
Quality of studies and risk of bias
Scores of QUADAS-2 [7] evaluation are presented in Fig. 2. Overall, the studies showed a low-to-moderate risk of bias and a few concerns about applicability. Four studies scored low risk of bias in all domains of the QUADAS-2 system. The highest risk of bias was associated to flow and timing. Considering concerns regarding applicability, all studies but two presented a low risk.
Fig. 2.

QUADAS-2 studies evaluation
Post-operative complications rate
All studies reported the rate of patients who developed complications after rTAR or oTAR, with an overall rate of 17.4%.
However, rTAR was associated with lower risk of complications rate (9.3 vs 20.7%, OR 0.358, 95% CI 0.218–0.589, p < 0.001) than oTAR (Fig. 3A). No heterogeneity was found in this analysis (I2 = 38.4%, p = 0.57).
Fig. 3.
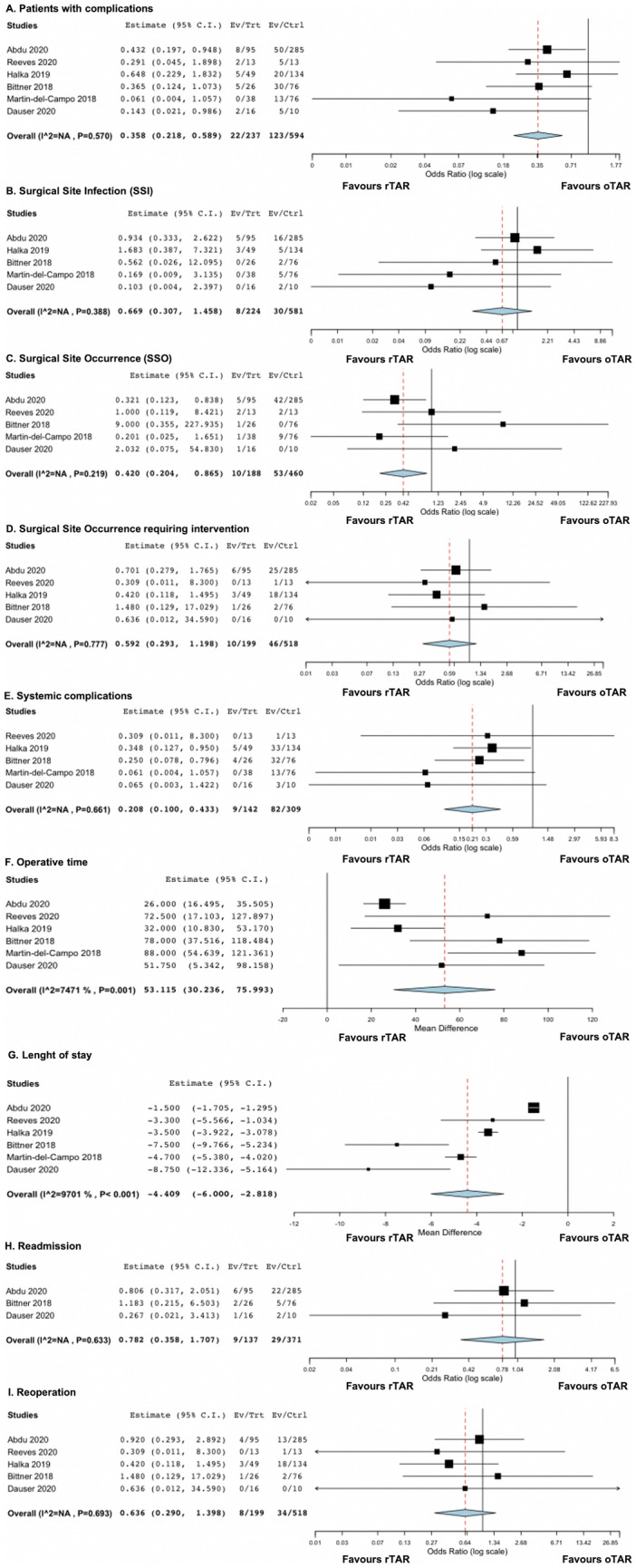
Forest plots of outcomes included in the analysis: patients with complications (A); SSI (B); SSO (C); SSO requiring intervention (D); systemic complications (E); operative time (F); length of stay (G); readmission (H); reoperation (I)
Then, we performed a meta-regression to evaluate possible patient (age, gender, comorbidities such as diabetes, BMI, respiratory diseases) or disease (reason for stoma creation) or technical (stoma type, site of mesh placement) variables able to impact upon the outcomes.
At meta-regression, no variable impacted the risk of complications (age p = 0.52; gender male vs female p = 0.38; diabetes p = 0.31; BMI p = 0.23; respiratory diseases p = 0.28; ASA status p = 0.34; type of hernia p = 0.41; hernia dimensions p = 0.16, mesh used yes vs not p = 0.27, type of mesh synthetic vs hybrid vs biologic p = 0.31). The meta-regression found also that the length of follow-up was not able to influence the post-operative complications rate (p = 0.46).
Surgical site infection
When we explored the surgical site infection (SSI) rate, we found 5 studies [8–12] on 805 patients reporting such outcome. The cumulative SSI rate was, therefore, 4.7%. There was no statistically significant difference in terms of risk of SSI development between rTAR and oTAR (3.6 vs 5.2%, OR 0.669, 95% CI 0.307–1.458, p = 0.44) (Fig. 3B). Also, in this case, there was no heterogeneity (I2 = 21%, p = 0.39).
Surgical site occurrence
Five studies [8–10, 12, 13] involving 648 patients reporting the rate of SSO, with a cumulative rate was 9.7%. Robotic TAR was associated with lower risk of developing SSO compared with oTAR (5.3 vs 11.5%, OR 0.669, 95% CI 0.307–1.458, p = 0.02) (Fig. 3C). No heterogeneity was found in this analysis (I2 = 0%, p = 0.2).
However, when we evaluated the rate of SSOPI (five studies [8–11, 13] on 717 subjects), no differences were noted between rTAR and oTAR (5 vs 8.9%, OR 0.592, 95% CI 0.293–1.198, p = 0.11) (Fig. 3D). Also in this case, no heterogeneity was found (I2 = 0%, p = 0.78).
Systemic complications
All studies but one [9–13], reported the rate of systemic complications after surgery (451 patients). The overall rate was 20.2%. However, rTAR was associated with lower risk of developing systemic complications as compared with oTAR (6.3 vs 26.5%, OR 0.208, 95% CI 0.100–0.433, p < 0.001) (Fig. 3E). No heterogeneity was found in this analysis (I2 = 0%, p = 0.7).
Operative time
All studies reporting operative time differences between rTAR and oTAR. As expected, a significant longer operative time was reported in the rTAR group when compared with oTAR group, (SMD 53.115, 95% CI 30.236–75.993, p < 0.01) (Fig. 3F). High heterogeneity was found (I2 = 74.71%, p = 0.001).
Length of hospital stay
The LOS was reported by all studies. Robotic TAR was associated with a significant shorter hospital stay than oTAR (SMD − 4.409, 95% CI − 6.000 to − 2.818, p < 0.001) (Fig. 3G). Overall heterogeneity was high in this analysis (I2 = 97%, p < 0.001).
Readmission and reoperation
The need for readmission was reported by only three studies [8–10] and 508 patients. No differences were seen between rTAR and oTAR in terms of readmission rate (6.6 vs 7.8%, OR 0.782, 95% CI 0.358–1.707, p = 0.77) (Fig. 3H). No heterogeneity was found (I2 = 12.5%, p = 0.63). Similarly, the rate of reoperation, explored by 5 studies [8–11, 13] and 717 patients, was not significantly different between rTAR and oTAR (4% vs 6.5%, OR 0.636, 95% CI 0.29–1.398, p = 0.26) (Fig. 3I). No heterogeneity was found (I2 = 0%, p = 0.69).
Discussion
In the current study, rTAR seems to be associated with lower risk of complications rate, with a significant longer operative time and a shorter hospital stay than oTAR. No difference was found about readmission and reoperation rate.
The oTAR with mesh reinforcement has emerged as an adequate approach for a VHR. It allows wide prosthesis overlap of larger hernia defects in the preperitoneal space lateral to the posterior rectus sheath. Ventral hernias with substantial width (≥ 10 cm) on cross-sectional imaging will often require TAR, and smaller defects may require TAR depending on the chronicity of the hernia and retraction of the rectus muscles. More generally, any patient who undergoes retrorectus dissection in whom the posterior sheath cannot be closed without tension likely needs unilateral or bilateral TAR [14]. It also seems to decrease the wound morbidity typically associated with the anterior component separation that requires the creation of a large subcutaneous flap [15, 16].
Meanwhile, to combine the benefits of minimally invasive approach and posterior component separation, rTAR is increasingly being used to treat complex ventral hernias. Some recent studies suggested that robotic approach seems to have some benefits despite a hypothetical increase of health-system costs [10].
From our review, all the analyzed papers reported a very low conversion rate (0–3%) suggesting that, in experienced hands, the robotic approach could be a feasible approach.
About post-operative complications, we found an overall rate of 17.4% after rTAR or oTAR, comparable with the international literature trend [17]. More particularly, we found a lower risk of complications rate in the rTAR group than the oTAR one (p < 0.001). This result is due to a lower risk of developing SSO and systemic complications after rTAR. No difference was found about SSI and SSOPI. Our results are consistent with that of a previous qualitative review about more generally robotic retromuscular repair. The authors reported a range of 3–52% of complications that are not necessarily infected (i.e., hematoma, seroma) [18]. This finding is not related to a proportional occurrence of SSOPI between both groups. Few papers reported a SSOPI rate ranged from 4 to 6%, for the most part reported as interventional radiology guided drainage [9, 16, 19, 20]. Few authors reported specific details regarding the nature of post-operative complications and there appeared to be broad distribution over various organ systems. No studies reported hernia recurrences with a length of follow-up ranged from 23 to 180 days.
These encouraging results could partly justify a decreased LOS for the rTAR group observed in our metanalysis. However, analyzing each metanalyzed papers, seems to be clear that the literature supporting robotic TAR is frankly lacking by some selection bias.
Martin-del-Campo et al. [12] which showed a shorter LOS with robotic TAR (1.3 days vs 6 days), reported more than double the number of patients with recurrent hernias in the oTAR group compared to the rTAR group (64.5 vs 28.9%, p = 0.001). Also Bittner et al. showed similar differences about the LOS (3.5 vs 6.7 days, p = 0.001). However, in the oTAR group, there was a 16% rate of concomitant procedures performed, including small bowel, colon, pancreatic, and kidney resections [9].
The first paper reporting a shortened LOS in the rTAR group was that of Carbonell et al. [16]. They suggested that this result may be attributable to decreased pain due to smaller incisions size in the rTAR versus oTAR group as well as a decreased traction on the abdominal wall by retractors.
The decreased LOS seems to be attributable to the typical advantages of a minimally invasive surgery respect to an open approach: reduced morbidity and less abdominal wall trauma seem to be the most important factors positively affecting this outcome.
Conversely, we found a longer operative time in the rTAR than oTAR group with a mean difference of about 53 min between the two surgical approaches.
This outcome is often affected when we compare a robotic procedure respect to an open one. This is due clearly to the docking and undocking steps required in the robotic operations that need additional time not required with open procedures. However, it cannot be excluded that this outcome may be affected also by cases performed during a learning curve period as reported by some study concerning robotic abdominal wall reconstruction (AWR) and other minimally invasive procedures [8, 16, 21, 22]. Abdu et al. [8] reported that the dataset timeframe includes cases from the beginning robotic experience of the two largest contributing authors to the robotic cohort. This may reflect, partly, increased time due to both surgeon techniques and case flow learning curve. The remaining 12 cases came from eight additional surgeons, for whom we would also expect longer operative times given they were in their experience with this technique.
However, Muysoms et al. showed that during the transition to robotic groin hernia repair there is a decrease in operative time by approximately 25% over a 4-month period of using the technology [23].
The higher cost of a robotic procedure represents always a discussed issue [24]. However, the cost analysis regarding the use of a robotic platform for AWR represents an item likewise debated. If we analyze the procedure-related, Personnel, reusable and disposables costs, we may of course conclude that a robotic AWR is not a cost saving procedure comparing to open AWR. But, as reported by Dauser et al. [10], adding procedure-related costs and costs for in-patient stay, total costs of EUR 8108.93 and 8650.12 were calculated for robotic-assisted and open TAR, respectively. However, the high costs for robotic AWR procedures result in an important issue about the economically sustainability of many National or Regional Health Systems.
Generally, the benchmark for a cost analysis of a robotic approach for quite all the digestive procedures, is represented by a laparoscopic approach. In the AWR, the robotic benchmark for a cost-analysis is the open approach because of the wide limitations found with the use of a laparoscopic approach during a complex AWR. So, it is conceivable that the use of a robotic platform for complex AWR may be comparable in total and social costs to the Open AWR. This is even more possible in the next future with a desirable reusables and disposables cost reduction due to the advent of new robotic platform on the health market.
The major strengths of this study are the systematic approach and that it is the first meta-analysis published on the direct comparison of the results of rTAR and oTAR.
Our study has some limitations. The retrospective nature of the studies analyzed is the main source of bias. None of them is a prospective randomized trial providing high level of evidence. The quality of the papers’ evidence was moderate, but proper blinding, for example, was always lacking. Accordingly, a selection bias was introduced.
These studies have no adequate follow-up period and so it is not possible to gain firm conclusions regarding the effectiveness of rTAR on recurrence rate. Two of the 6 six included studies [8, 11] report the results of Hybrid rTAR which could be another factor affecting the selection bias. Finally, none of the included studies clearly reported if the enrolled ventral hernia were PVH or IH. In a previous metanalysis [25], we supported the hypothesis that PVH and IH are different conditions with the latter being more challenging to treat. Accordingly, EHS classifications should be adopted systematically, as well as pooling data analysis should be no longer performed in clinical trials.
Conclusion
Based on the data from our meta-analysis, robotic approach for TAR seems safe and fasible, even in more difficult cases. The rTAR shows the common advantages of minimally invasive procedures that improve short-term outcomes with significant benefits in the early postoperative period. However, no firm recommendations can be drawn from the available evidence and further prospective, randomized studies should investigate clinical outcomes with longer follow-up and perform comparative cost-effective analyses.
Funding
Open access funding provided by Università degli Studi di Napoli Federico II within the CRUI-CARE Agreement. This study was not funded.
Declarations
Conflict of interest
Umberto Bracale, Francesco Corcione, Daniele Neola, Simone Castiglioni, Giuseppe Cavallaro, Cesare Stabilini, Emanuele Botteri, Francesco Corcione, Maurizio Sodo, Nicola Imperatore, Roberto Peltrini declare that they have no conflict of interest.
Ethical approval
Ethical approval was not sought for the present study because it is a systematic review of published literature.
Informed consent
For this type of study, formal consent is not required.
Human and animal rights
This article does not contain any studies directly involving participants, as it is a review of data already collected in a hernia database.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
U. Bracale, Email: umbertobracale@gmail.com
F. Corcione, Email: francesco.corcione@unina.it
D. Neola, Email: danieleneola@gmail.com
S. Castiglioni, Email: simone.castiglioni90@gmail.com
G. Cavallaro, Email: giuseppe.cavallaro@uniroma1.it
C. Stabilini, Email: cesare.stabilini@unige.it
E. Botteri, Email: e.botteri@libero.it
M. Sodo, Email: maurizio.sodo@unina.it
N. Imperatore, Email: nicola.imperatore@alice.it
R. Peltrini, Email: roberto.peltrini@gmail.com
References
- 1.Stabilini C, Bracale U, Pignata G, Frascio M, Casaccia M, Pelosi P, Signori A, Testa T, Rosa GM, Morelli N, Fornaro R, Palombo D, Perotti S, Bruno MS, Imperatore M, Righetti C, Pezzato S, Lazzara F, Gianetta E. Laparoscopic bridging vs anatomic open reconstruction for midline abdominal hernia mesh repair [LABOR]: single-blinded, multicenter, randomized, controlled trial on long-term functional results. Trials. 2013;14:357. doi: 10.1186/1745-6215-14-357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Guzman-Pruneda Huang Collins Renshaw Narula Poulose AFLCCSVKB. Abdominal core quality of life after ventral hernia repair: a comparison of open versus robotic-assisted retromuscular techniques. Surg Endosc. 2021;35(1):241–248. doi: 10.1007/s00464-020-07386-x. [DOI] [PubMed] [Google Scholar]
- 3.Temudom T, Siadati M, Sarr MG. Repair of complex giant or recurrent ventral hernias by using tension-free intraparietal prosthetic mesh (Stoppa technique): lessons learned from our initial experience (fifty patients) Surgery. 1996;120(4):738–743. doi: 10.1016/s0039-6060(96)80025-0. [DOI] [PubMed] [Google Scholar]
- 4.Novitsky YW, Elliott HL, Orenstein SB, Rosen MJ. Transversus abdominis muscle release: a novel approach to posterior component separation during complex abdominal wall reconstruction. Am J Surg. 2012;204(5):709–716. doi: 10.1016/j.amjsurg.2012.02.008. [DOI] [PubMed] [Google Scholar]
- 5.Belyansky I, Zahiri HR, Park A. Laparoscopic transversus abdominis release, a novel minimally invasive approach to complex abdominal wall reconstruction. Surg Innov. 2016;23(2):134–141. doi: 10.1177/1553350615618290. [DOI] [PubMed] [Google Scholar]
- 6.Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA. PRISMA-P Group Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1. doi: 10.1186/2046-4053-4-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, Leeflang MM, Sterne JA, Bossuyt PM. QUADAS-2 Group QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529–536. doi: 10.7326/0003-4819-155-8-201110180-00009. [DOI] [PubMed] [Google Scholar]
- 8.Abdu R, Vasyluk A, Reddy N, Huang LC, Halka JT, DeMare A, Janczyk R, Iacco A (2020) Hybrid robotic transversus abdominis release versus open: propensity-matched analysis of 30-day outcomes. Hernia. 30. 10.1007/s10029-020-02249-9 (Epub ahead of print. PMID: 32607651) [DOI] [PubMed]
- 9.Bittner JG, 4th, Alrefai S, Vy M, Mabe M, Del Prado PAR, Clingempeel NL. Comparative analysis of open and robotic transversus abdominis release for ventral hernia repair. Surg Endosc. 2018;32(2):727–734. doi: 10.1007/s00464-017-5729-0. [DOI] [PubMed] [Google Scholar]
- 10.Dauser B, Hartig N, Vedadinejad M, Kirchner E, Trummer F, Herbst F (2020) Robotic-assisted repair of complex ventral hernia: can it pay off? J Robot Surg. 15: 45-52. 10.1007/s11701-020-01078-3. Epub ahead of print. PMID: 32277399. [DOI] [PubMed]
- 11.Halka JT, Vasyluk A, Demare A, Iacco A, Janczyk R. Hybrid robotic-assisted transversus abdominis release versus open transversus abdominis release: a comparison of short-term outcomes. Hernia. 2019;23(1):37–42. doi: 10.1007/s10029-018-1858-1. [DOI] [PubMed] [Google Scholar]
- 12.Martin-Del-Campo LA, Weltz AS, Belyansky I, Novitsky YW. Comparative analysis of perioperative outcomes of robotic versus open transversus abdominis release. Surg Endosc. 2018;32(2):840–845. doi: 10.1007/s00464-017-5752-1. [DOI] [PubMed] [Google Scholar]
- 13.Reeves J, Mehta S, Prabha RD, Salama Y, Mittal A. Robotic versus open transversus abdominis release and incisional hernia repair: a case-control study. Laparoscop Endoscop Robot Surg. 2020;3(3):59–62. doi: 10.1016/j.lers.2020.06.002. [DOI] [Google Scholar]
- 14.Zolin SJ, Fafaj A, Krpata DM. Transversus abdominis release (TAR): what are the real indications and where is the limit? Hernia. 2020;24(2):333–340. doi: 10.1007/s10029-020-02150-5. [DOI] [PubMed] [Google Scholar]
- 15.Krpata DM, Blatnik JA, Novitsky YW, Rosen MJ. Posterior and open anterior components separations: a comparative analysis. Am J Surg. 2012;203(3):318–322. doi: 10.1016/j.amjsurg.2011.10.009. [DOI] [PubMed] [Google Scholar]
- 16.Carbonell AM, Warren JA, Prabhu AS, Ballecer CD, Janczyk RJ, Herrera J, Huang LC, Phillips S, Rosen MJ, Poulose BK. Reducing length of stay using a robotic-assisted approach for retromuscular ventral hernia repair: a comparative analysis from the Americas hernia society quality collaborative. Ann Surg. 2018;267(2):210–217. doi: 10.1097/SLA.0000000000002244. [DOI] [PubMed] [Google Scholar]
- 17.Stabilini C, Cavallaro G, Bocchi P, Campanelli G, Carlucci M, Ceci F, Crovella F, Cuccurullo D, Fei L, Gianetta E, Gossetti F, Greco DP, Iorio O, Ipponi P, Marioni A, Merola G, Negro P, Palombo D, Bracale U. Defining the characteristics of certified hernia centers in Italy: the Italian society of hernia and abdominal wall surgery workgroup consensus on systematic reviews of the best available evidences. Int J Surg. 2018;54(Pt A):222–235. doi: 10.1016/j.ijsu.2018.04.052. [DOI] [PubMed] [Google Scholar]
- 18.Santos DA, Limmer AR, Gibson HM, Ledet CR. The current state of robotic retromuscular repairs-a qualitative review of the literature. Surg Endosc. 2021;35(1):456–466. doi: 10.1007/s00464-020-07957-y. [DOI] [PubMed] [Google Scholar]
- 19.Warren JA, Cobb WS, Ewing JA, Carbonell AM. Standard laparoscopic versus robotic retromuscular ventral hernia repair. Surg Endosc. 2017;31(1):324–332. doi: 10.1007/s00464-016-4975-x. [DOI] [PubMed] [Google Scholar]
- 20.Halpern DK, Howell RS, Boinpally H, Magadan-Alvarez C, Petrone P, Brathwaite CEM. Ascending the learning curve of robotic abdominal wall reconstruction. JSLS. 2019;23(1):e2018.00084. doi: 10.4293/JSLS.2018.00084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bracale U, Merola G, Sciuto A, Cavallaro G, Andreuccetti J, Pignata G. Achieving the learning curve in laparoscopic inguinal hernia repair by tapp: a quality improvement study. J Invest Surg. 2019;32(8):738–745. doi: 10.1080/08941939.2018.1468944. [DOI] [PubMed] [Google Scholar]
- 22.Merola G, Cavallaro G, Iorio O, Frascio M, Pontecorvi E, Corcione F, Andreuccetti J, Pignata G, Stabilini C, Bracale U. Learning curve in open inguinal hernia repair: a quality improvement multicentre study about Lichtenstein technique. Hernia. 2020;24(3):651–659. doi: 10.1007/s10029-019-02064-x. [DOI] [PubMed] [Google Scholar]
- 23.Muysoms F, Van Cleven S, Kyle-Leinhase I, Ballecer C, Ramaswamy A. Robotic-assisted laparoscopic groin hernia repair: observational case-control study on the operative time during the learning curve. Surg Endosc. 2018;32(12):4850–4859. doi: 10.1007/s00464-018-6236-7. [DOI] [PubMed] [Google Scholar]
- 24.Merola G, Sciuto A, Pirozzi F, Andreuccetti J, Pignata G, Corcione F, Milone M, De Palma GD, Castaldo R, Pecchia L, Ceccarelli G, Bracale U. Is robotic right colectomy economically sustainable? A multicentre retrospective comparative study and cost analysis. Surg Endosc. 2020;34(9):4041–4047. doi: 10.1007/s00464-019-07193-z. [DOI] [PubMed] [Google Scholar]
- 25.Stabilini C, Cavallaro G, Dolce P, Capoccia Giovannini S, Corcione F, Frascio M, Sodo M, Merola G, Bracale U. Pooled data analysis of primary ventral (PVH) and incisional hernia (IH) repair is no more acceptable: results of a systematic review and metanalysis of current literature. Hernia. 2019;23(5):831–845. doi: 10.1007/s10029-019-02033-4. [DOI] [PubMed] [Google Scholar]