

Abstract
To address low family planning (FP) use and high unmet need in West Africa, attention has been paid to addressing FP-related social networks and norms. Most work focuses on women. This analysis assesses men’s FP-related social networks and norms and their relation to FP use in Benin using data from baseline surveys from the Tékponon Jikuagou intervention. We descriptively analyzed men’s egocentric FP-related social networks and norms at the village level. Multivariable logistic regression analyses (N=885) examined the relationship between FP-related social networks, norms, and men’s current and future FP use. Twenty-three percent of men reported current modern contraception use and 47% reported intended future use. Most had few network members. While most believed it was acceptable to discuss FP, few talked with peers about FP and most did not discuss FP with their partner(s). In multivariable analyses, neither networks nor norms were significantly related to men’s FP use. Men’s networks being small and men rarely discussing FP indicate an opportunity for village-based approaches to engage men in FP discussions and spark FP dialogue within couples, between men, and within villages. Future work should further explore the relationship between men’s social networks, norms, and FP use.
Keywords: Family Planning, Men, Social Networks, Social Norms, Benin
I. Introduction
Background
Global progress has been made on addressing supply-side barriers to family planning (FP) use and on increasing knowledge of FP methods since the 1994 Cairo Declaration on Population and Development (Khan et al., 2007; UNFPA, 2014). Despite these investments made over recent decades and high FP demand, we see a consistent unmet need for FP in West Africa. A woman has an unmet need for FP if she wants to avoid childbearing, is sexually active, and is not using effective contraception (Casterline & Sinding, 2000). Low FP use and high unmet need have multiple consequences for women’s health including unsafe abortion and closely spaced births (WHO, 2007, 2014). Beyond physical health, FP use impacts women’s empowerment, child welfare, and social and economic development (Cleland et al., 2006; WHO, 2017).
Benin, the country of focus for this study, has high unmet need for contraception, low rates of modern contraception (MC) use, and poor maternal and child health. Women have access to variuos MC methods with implants, injectables, and oral contraceptives being the most commonly used by women (Government of Benin, 2018). In 2016, as part of the FP2020 Initiative, Benin committed to a 20% contraceptive prevalence rate by 2018 (FP2020, 2016). MC use among women in Benin increased from 3% to 12% between 1996-2019 (FP2020, 2016; INSAE & ICF International, 2013). Yet, unmet need increased from 28% to 36% in the same period. The most commonly cited reasons for unmet need in Benin are fear of side effects among married women and not being married for sexually active unmarried women (Guttmacher Institute, 2018). Across sub-Saharan Africa, the most common factors influencing contraceptive use are fear of side effects, male partner disapproval, sociocultural and normative beliefs about fertility, women’s education and employment, and partner communication (Blackstone et al., 2017). High fertility and large desired family size contribute to continued low MC use in Benin, and in 2015 women had, on average, 4.9 children (Guttmacher Institute, 2018). Benin also has a high maternal mortality ratio (397 maternal deaths per 100,000 live births) and infant mortality rate (63 infant deaths per 1,000 live births) (The World Bank, 2015b, 2015a).
To address low MC use, high unmet need, and their resulting health outcomes, global attention has focused on identifying and addressing demand-side barriers to MC use, including social factors (e.g., perception of others’ FP use; FP norms; FP stigma) (Costenbader et al., 2017; Khan et al., 2007). In West Africa, social factors have been shown to prevent individuals from acting on FP desires (Igras et al., 2017). There is a need to acknowledge social factors as key influences on FP behaviour. Specifically, recent work in Benin shows that women and men rarely speak with each other about fertility and FP and that couple decision-making is uncommon. Yet, fertility decisions are typically made within the context of a large sphere of relationships (e.g., husband-wife dyad, friendship and family networks) and are under the influence of village norms (IRH, 2017). FP-related stigma prevents women and men from talking publicly about FP or acknowledging its use (Igras et al., 2017). Recent work also suggests that alignment of foundational building blocks at the individual, couple, services, and social level are essential to meet FP need in Benin (Igras et al., 2021). The two features of social factors that this analysis focuses on are social networks and norms. We were interested in how the social context of villages influences social networks and norms and how these affect FP use. Throughout this manuscript, we use the term ‘village’ as villages are the communities of reference and the terms are used interchangeably in French in Benin.
Literature on the connection between social networks, FP use, and fertility behavior has grown in recent years (Agadjanian, 2001; Madhavan et al., 2005; Shakya et al., 2020). In egocentric social network analysis, individuals are asked about contacts with which they have direct ties (i.e., their personal network) and the characteristics of those individuals and relationships (Valente, 2010). Both the structure (i.e., size) and content (i.e., FP approval) of peoples’ networks related to FP are associated with FP use (Behrman et al., 2002; Madhavan et al., 2005; Paz Soldan, 2004). Prior FP network studies with women find that women with network contacts outside their village report greater use of FP, women naming their husband as a network contact is positively related to the number of children the couple has, and women who report more conjugal kin as network contacts report lower rates of FP use and ascribe to more traditional gender norms (Madhavan et al., 2005). Studies with women also find that having other FP users in one’s network is associated with higher FP use as women find out about others’ FP use through direct communication and that being socially isolated is associated with not using FP (Behrman et al., 2002; Paz Soldan, 2004; Shakya et al., 2020).
The second aspect of social factors is social norms. Social norms have been conceptualized and measured in various ways, but are commonly defined as unspoken rules of behavior shared by members of a given group (Chung & Rimal, 2016; Cislaghi & Heise, 2019; The Learning Collaborative to Advance Normative Change, 2019). Individuals are thought to conform to social norms based on their belief that others in a social group are doing the same, and that they would disapprove of behavior that deviates from this shared norm (Bicchieri, 2016). Descriptive norms refer to people’s perceptions about the prevalence of a behavior in their social sphere, injunctive norms to perceptions about what is approved or correct behavior, and sanctions to the anticipated opinion or reaction of others that would result from diverging from the norm (Chung & Rimal, 2016; Stefanik & Hwang, 2017; Yzer, 2012). We focus here on descriptive norms and sanctions.
Social norms have long been recognized as playing a role in shaping fertility preferences (Udry, 1982). Furthermore, social sanctions are a particularly salient mechanism for enforcing fertility norms (e.g., a woman believes she will be ostracized from her village if she uses FP, a woman believes her partner will disapprove) (Alvergne et al., 2011; Buesseler & Diakité, 2013; Madhavan et al., 2005; Oheneba-Sakyi & Takyi, 1997; Sedgh & Hussain, 2014; Shah, 1974). Improved couple communication has been shown to increase FP use (Parker & Sommer, 2010; Sanusi et al., 2014; Shattuck et al., 2011). However, less work has examined the relationship between social norms and FP discussion and use, and there is limited research that rigorously examines how social norms interventions influence FP behaviour (Herbert, 2015). A review of social norms measures related to FP use found that all studies measuring social norms and FP use that met review criterion documented significant relationships between at least one FP norm and FP behavior (Costenbader et al., 2017). Prior work has also found significant associations between condom use and social norms (Nöstlinger et al., 2010; Wang & Wang, 2005). Notably, attention has focused on understanding and addressing peoples’ social environment for FP more recently, specifically social networks and norms related to FP, to understand and address village-level influences on FP. Most of this work has focused on women (Alvergne et al., 2011; Guttmacher Institute, 2018; Madhavan et al., 2005).
Yet, the global community has recognized the importance of men in FP decision-making with couple communication about FP being a critical component (Costenbader et al., 2017; Rimal et al., 2015; Wegs et al., 2016). In Benin, one commonly cited reason for women not using FP is opposition from a male partner, yet less than 4% of women reported discussing FP with their partner in 2015 (Guttmacher Institute, 2018). One qualitative study in rural Malawi found that both women’s and men’s social networks influence their FP use, but that networks impact their FP behaviors differently (Paz Soldan, 2004). For example, men’s perception of network contacts use of FP was based on assumptions rather than direct communication. This qualitative work found that gender shapes the way individuals speak about and perceive FP. Additionally, prior qualitative work has found that men’s social networks may be more influential on men’s FP use than women’s networks are to their FP use (Behrman et al., 2002). Men are also more likely than women to have known their network contacts for a long period of time. Thus, we cannot transfer findings about women’s networks and norms to men. A greater understanding of men’s social networks and their perceptions of social norms surrounding FP is needed.
The Tékponon Jikuagou (TJ) intervention
The TJ intervention was implemented as a response to a need to increase social acceptability of FP discussion and use. The Institute of Reproductive Health at Georgetown University, CARE International, and Plan International, designed a social network intervention to catalyse critical dialogue on fertility and FP and diffuse new ideation about FP use through women’s and men’s social networks to lead people to act on their unmet need for FP by seeking services (IRH, 2017). Prior to designing the intervention, TJ conducted formative research through ethnography and a participatory social network mapping methodology (Igras et al., 2017). TJ used a social network approach to address the contextual and relational issues that prevent couples from spacing or limiting births through FP (Igras et al., 2017). TJ's social network approach is anchored in social network and behaviour change theory, which focuses on the role of social relationships in channeling interpersonal or media influence, and transmitting, influencing, and enabling attitude or behaviour change (Kadushin, 2012; Valente, 2010). TJ also employs communication for social change techniques, which empower people and facilitate equitable social transformation (Figueroa et al., 2002). TJ was implemented in the Couffo and Ouémé Departments of Benin from 2015-2017 (IRH, 2017).
Study Objectives
Given the lack of information and understanding on men’s social networks and norms, we focused this analysis on analyzing data from surveys completed by men living in villages that would later be reached by the TJ intervention. Our goal was to understand the content and structure of men’s social networks and social norms surrounding FP and the relation of these factors to men’s current and intended FP use in Benin.
Conceptual Model and Hypotheses
For this analysis, we developed a conceptual model based on the socio-ecological framework, which highlights FP influences at the individual, couple, and village levels (Figure 1) (Bronfenbrenner, 1979). The items we focus on in this analysis operate at the village level but are measured at the individual level (i.e., men’s social networks and social norms). Building on TJ’s social network diffusion approach, we hypothesize that men with networks that are more supportive of FP and men who believe that social norms around FP are more supportive of FP use will report greater current and intended FP use.
Figure 1:
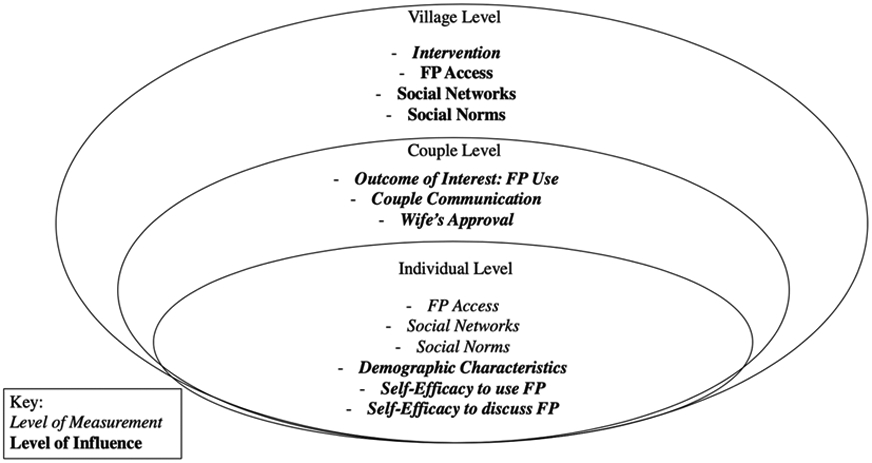
Conceptual Model for Couple FP Use
We operationalized supportive social networks and social norms in multiple ways. For example, we considered the size of men’s networks and how much of their network is outside of their village, as we expect that both factors may spark more FP communication and serve as a bridge to new, outside ideas (Madhavan et al., 2005). We also hypothesized, based on research done with women, that the higher the percentage of men’s networks that include male relatives, the more likely men are to adhere to traditional FP norms unsupportive of FP (Madhavan et al., 2005). Related to social norms, we hypothesized that if FP use is normative and expected by the village, men’s social networks will be supportive of FP use, and men’s FP current and intended use will increase. Similarly, we hypothesize that if the perceived sanctions that would arise from using FP are weak, men’s networks would embrace rather than sanction potential and actual FP users, and men’s FP current and intended use will be higher.
We also considered demographic characteristics related to individuals’ FP use (i.e., age, education, number of wives, number of children, religion, ethnicity). Younger age groups have been shown to be more open to FP use, as prior work has found age-specific effects on FP use (Madhavan et al., 2005). Those with more living children may be more supportive of FP, but only if they want to space or limit childbearing (Bankole & Singh, 1998). Those with more education are more likely to be supportive of FP, but the association between education and FP may be less strong for men than for women (Cochrane, 1979). Prior work has found that among women, having a co-wife may lead to less FP use, but it is unclear how having multiple wives affects men’s FP decisions (Bankole & Singh, 1998; Madhavan et al., 2005).
II. Materials and Methods
Data and Sample
Data come from men’s surveys conducted in 2015 prior to the TJ intervention. We have 32 villages in this analysis, all located in the Ouémé Department in southern Benin. TJ stratified sampling by region and village size and based sampling on the 2012 Beninese Demographic and Health Survey (INSAE & ICF International, 2013). TJ conducted sampling with a probability proportional to the adult population (15-59 years) according to the 2015 Benin census (IRH, 2017). Of the 1,030 men interviewed at baseline, 145 were missing data on whether or not their wife approved of FP use, resulting in an analytic sample of 885.
Men’s surveys included egocentric social network questions in which participants were asked to separately give the first name of up to 12 people that they relied on for material (i.e., money, food), practical (i.e., childcare, chores), and/or emotional (i.e., advice, guidance) support. These questions were open-ended and not linked to fertility and FP-related support. If a person had the same name and relation to the respondent and was listed more than once (e.g., Eunice, wife), they were considered a duplicate and removed from the dataset. After removing duplicate entries, we created a summed score of the number of people in each man’s egocentric network. The survey also asked questions related to FP social norms, self-efficacy for FP use and discussion, couple communication, and current and intended FP use.
One man and one woman per household were interviewed. While the women and men interviewed are likely spouses, data are not matched. Participating men were over the age of 18 years and had a wife ages 18-44 years. Response rates for men were 97%. As most were illiterate, participants were presented with informed consent information in conjunction with a short form written consent document, which states that the elements of consent have been presented orally. The written informed consent document was in French, the official language of Benin. The Institutional Review Board (IRB) of Georgetown University and le Comité d’Ethique de la Recherche, Institut des Science Biomédicales Appliquées en Santé in Benin approved the study protocol. This secondary data analysis was deemed exempt by the IRB at the University of North Carolina at Chapel Hill.
Key Indicators
Village Factors for FP (Table 1)
Table 1:
Village Factors for FP
| Variable Descriptions | Category |
|---|---|
| Number of network contacts | Network Size |
| % of Network living in their household or village | Network Outside of Village |
| % of Network that is not a Male Relative | Network Non-Male Relative |
| % of Network they believe approves of FP | Network FP Approval |
| % of Network they communicate about FP with | Network FP Communication |
| In this village, it is acceptable to discuss FP | FP Acceptability |
| Do you think you'd be criticized by community if used MC? | FP Sanctions |
| Do you think you'd be excluded from social gatherings if used MC? | FP Sanctions |
| If a man finds out his wife is using FP, would he yell or beat her? | FP Sanctions |
As stated above, men were asked to give the first name of people that they relied on for support. We created five network measures to assess different aspects of the structure and content of men’s egocentric networks (Kohler et al., 2001). First, we calculated the size or number of unique contacts in each man’s network (Network Size). While this variable was a count, all other network variables were assessed as percentages of the total personal network. For instance, for residence, we created an indicator for whether or not each network contact lived within their household or village. We created a variable for the percent of each man’s network living outside of their village as opposed to in their household or village (Network Outside of Village). We created a variable to assess the percentage of each male respondent’s network that were not male relatives (i.e., father, brother, or other male relative) (Network Non- Male Relative). To do this, for each male respondent we summed network contacts who were not male relatives and divided by their total network size to determine a percentage of each respondent’s network that was not a male relative. We analogously examined the content of men’s interactions within their network, including their perception of network members’ approval of FP and their communication about FP. To do this, we created a measure indicating the percent of network members each male respondent believed approved of FP (Network FP Approval) and a measure indicating the percentage of network members with whom each male respondent communicated about FP (Network FP Communication).
To examine the influence of social norms and related sanctions at the village level on men’s reported FP use, we used four variables that asked about perceptions of what was acceptable and what would be sanctioned. Men were asked their level of agreement with four statements reflecting either a descriptive norm or a sanction related to violating a norm. Men were asked their level of agreement with the statement: ‘In this village, it is acceptable to discuss FP’ (FP Acceptability). Similarly, men were asked if they agreed with the statements: ‘Do you think you'd be criticized by community if used MC; Do you think you'd be excluded from social gatherings if used MC?’; ‘If a man finds out his wife is using FP, would he yell or beat her?’. For each statement, if they agreed, we coded them as perceiving that the village FP sanction existed. We created an average for each man’s agreement (i.e., if he agreed with one of the three questions, his score was 0.33) and reverse coded it so that a higher score indicated lower perceived levels of sanctions for FP use in the Village (Disagree that FP Sanctions exist).
Couple and Individual Factors for FP
In our multivariable model, we controlled for variables at the couple and individual levels known to be related to FP use. At the couple level, this included men’s perception of wives’ FP approval and men’s reported couple communication on FP and childbearing in the last 12 months. At the individual level, this included men’s self-efficacy to use FP, men’s self-efficacy to discuss FP, and men’s perceived FP access. Men’s self-efficacy to use FP was measured by the man’s confidence in being able to use MC at all times (yes/no). Men’s self-efficacy to discuss FP was comprised of items asking about men’s comfort discussing FP with six different people in a six-item index. Men’s FP access was assessed in a summed four-item index (yes/no for each indicator). We included demographic variables known to be influential in individuals’ FP decisions: age, education, number of wives, number of living children, religion, and ethnicity. Age, education, and number of living children were made into categorical indicators. Number of wives was dichotomized as ‘one’ or ‘more than one;’ religion was dichotomized as ‘Christian’ or ‘non-Christian;’ and ethnicity was dichotomized as ‘Fon’ or ‘other.’
FP Use
For our first outcome of interest, we used men’s reports of whether they or at least one of their wives was using MC. This was defined as using at least one of the following methods: sterilization, oral contraceptive, intrauterine device, injectable, implant, condoms, diaphragm/mousse/gel, lactational amenorrhea, or cycle beads. If men reported them or their wife used both MC and a traditional method (withdrawal, periodic abstinence, traditional tea, traditional belt), they were coded as using MC. Intention to use FP in the future was our second outcome of interest; we used men’s reports of if they thought themselves or at least one of their wives would use any FP (i.e., modern or traditional) in the future. This question was asked to all men, both those using and not using FP.
Statistical Analyses
This analysis created indicators for and explored men’s social networks and norms related to MC, and subsequently assessed the relationship between men’s social networks, social norms, and FP current and intended use. Our first aim was to describe men’s egocentric social networks and social norms related to discussion and approval of FP use.
Our second aim was to determine the association between men’s FP-related social network and norm measures and men’s reported and intended future FP use. We first assessed the pairwise correlations amongst network and norm indicators, relevant couple and individual level indicators, demographic characteristics, and FP current and intended use. We then conducted logistic regression analysis. Logistic regression has commonly been used to assess the relationship between social factors and FP use (Kohler et al., 2001; Madhavan et al., 2005). We assessed outcomes at the individual level. However, in keeping with our socioecological conceptual model and as data were collected in distinct villages, we accounted for clustering of individuals within villages and created several village-level variables. For all of the variables at the village level, individuals were assigned the mean covariate value of all respondents from their village. Variables were added into multivariable models based on our conceptual model (Figure 1) and pairwise correlations being below 0.80. In analyses, indicators for age and number of living children were collapsed further due to few men being 18-24 years old and few men having no or few children. We used margins to create predicted probabilities of current MC use and intended future FP use at the 25th and 75th percentiles for all village-level variables as well.
III. Results
Descriptive Statistics (Tables 2-4)
Table 2:
Men’s Demographic Characteristics
| (N=885) | ||
|---|---|---|
| n | % | |
| Age Group | ||
| 18-24 | 29 | 3.28 |
| 25-34 | 314 | 35.48 |
| >34 | 542 | 61.24 |
| Education Status | ||
| None | 286 | 32.32 |
| Primary | 353 | 39.89 |
| Secondary or More | 246 | 27.8 |
| Number of Wives | ||
| 1 | 594 | 67.12 |
| More than 1 | 291 | 32.88 |
| Number of Living Children | ||
| None | 29 | 3.28 |
| 1 | 107 | 12.09 |
| 2 | 138 | 15.59 |
| 3 | 138 | 15.59 |
| 4 | 122 | 13.79 |
| 5 or more | 351 | 39.66 |
| Religion | ||
| Christian | 687 | 77.63 |
| Other | 198 | 22.37 |
| Ethnicity | ||
| Fon | 855 | 96.61 |
| Other | 30 | 3.39 |
Table 4.
Social, Couple, and Individual Factors Related to Men’s FP Use, Aggregated at the Village Level
| N=885 | |||
|---|---|---|---|
| Mean | SD | ||
| FP Networks | Network Size (individual) | 2.18 | 1.45 |
| Network Outside of Village | 0.34 | 0.38 | |
| Network Non-Relative | 0.63 | 0.39 | |
| Network FP Approval | 0.36 | 0.42 | |
| Network FP Communication | 0.15 | 0.31 | |
| FP Social Norms | FP Acceptability | 0.86 | 0.34 |
| Disagree that FP Sanctions exist (3 items) + | 0.65 | 0.32 | |
| n | % | ||
| Couple Level Factors for FP | At least one wife approves of FP | 602 | 68.02 |
| Wife listed in social network | 328 | 37.06 | |
| Mean | SD | ||
| Couple Communication about FP (3 items) + | 0.31 | 0.41 | |
| n | % | ||
| Individual Level Factors for FP | Self-Efficacy to Use FP | 560 | 63.28 |
| Mean | SD | ||
| Self-Efficacy to Discuss FP (6 items) + | 0.50 | 0.38 | |
| FP Access (4 items) + | 0.59 | 0.43 | |
index of multiple items on a scale of 0-1
The majority of men are over 34 years old, have at least a primary education, and have only one wife. Over one-third have at least five children, most are Christian, and they are almost exclusively of Fon ethnicity. Twenty-two percent reported current use of modern contraception and 54% reported intended future use. Notably, the majority of current MC users (70%) reported intention to use in the future while only 45% of non-users reported an intention to use.
Men’s Village Level FP Factors (Table 4)
The social network mapping activity elicited a small number of network contacts (mean of 2) with 11% of men listing no network contacts in any network. On average, around one-third of men’s network contacts lived outside of their village. Over 60% of men’s contacts were not male relatives. On average, the percent of men’s network contacts that they believe approved of FP was about one-third and men talked with a small percentage of network members (15%) about FP.
Regarding social norms, while men believed that most of their individual network contacts did not approve of FP and they did not communicate with most of their network about FP, they believed their village supported FP. Eighty-six percent believed it was acceptable to discuss MC in their village. The majority of men disagreed with statements that sanctions exist for using FP, with men disagreeing, on average, with roughly two of the three sanction related questions.
Men’s Couple and Individual Level FP Factors (Table 4)
At the couple level, most men believed that at least one of their wives approved of FP (68%). However, only 37% of men listed their wife in their social network. The percentage of men discussing FP and childbearing with at least one wife was relatively low but varied by indicator. With their wife, over one-third discussed their opinion about having children, one-quarter discussed which MC method to use, and one-quarter discussed how to obtain MC. In the couple communication index, men on average agreed with 31% of the items (less than one out of three).
At the individual level, 63% of men were confident in being able to use MC all the time. On average, men were comfortable discussing FP with half of their network contacts. Men agreed with, on average, 59% of the four questions (two out of four) around having FP access.
Multilevel Logistic Regression for Men’s Current MC Use and Intention to Use FP (Tables 5 and 6)
Table 5:
Bivariate Logistic Regressions for Men’s Current MC Use and Future FP Use (N=885)
| Current MC | Future FP | |||
|---|---|---|---|---|
| Odds Ratio | 95% CI | Odds Ratio | 95% CI | |
| Village | 1.43 | 0.74, 2.75 | 0.55 | 0.34, 0.87 |
| Men’s Village Factors for FP | ||||
| Network Size | 0.61 | 0.37, 1.02 | 1.50 | 1.01, 2.21 |
| Network Outside of Village | 0.99 | 0.96, 1.01 | 1.02 | 1.00, 1.04 |
| Network Non-Relative | 1.01 | 0.98, 1.04 | 1.01 | 0.99, 1.04 |
| Network FP Approval | 0.98 | 0.96, 1.00 | 1.03 | 1.01, 1.04 |
| Network FP Communication | 1.05 | 1.01, 1.09 | 0.97 | 0.94, 0.99 |
| FP Acceptability | 1.01 | 0.97, 1.04 | 1.04 | 1.01, 1.06 |
| Disagree that FP Sanctions exist | 1.23 | 0.84, 1.82 | 0.68 | 0.52, 0.88 |
| Men’s Couple & Individual Factors for FP | ||||
| At least one wife approves of FP | 3.89 | 2.48, 6.10 | 15.14 | 10.23, 22.40 |
| Wife in Network | 1.61 | 1.05, 2.46 | 1.73 | 1.23, 2.43 |
| Couple Communication about FP | 2.10 | 1.77, 2.49 | 3.07 | 2.52, 3.74 |
| Self-Efficacy to Discuss FP | 1.44 | 1.20, 1.72 | 2.79 | 2.37, 3.29 |
| Self-Efficacy to Use FP | 3.81 | 2.49, 5.84 | 6.30 | 4.57, 8.69 |
| FP Access | 3.24 | 2.49, 4.20 | 3.02 | 2.55, 3.57 |
| Covariates | ||||
| Age Group (>34 ref) | ||||
| 18-34 | 0.66 | 0.46, 0.94 | 1.39 | 1.04, 1.85 |
| Education (None ref) | ||||
| Primary | 1.61 | 1.04, 2.48 | 1.83 | 1.30, 2.57 |
| Secondary or more | 2.11 | 1.33, 3.34 | 2.52 | 1.72, 3.69 |
| Number of Living Children (5 or more ref) | ||||
| None or 1 | 0.27 | 0.14, 0.51 | 1.31 | 0.85, 2.00 |
| 2-4 | 0.68 | 0.48, 0.98 | 0.95 | 0.70, 1,28 |
| Multiple Wives | 1.50 | 1.05, 2.15 | 1.25 | 0.92, 1.69 |
| Non-Christian Religion | 0.96 | 0.62, 1.50 | 0.54 | 0.37, 0.79 |
Table 6:
Multivariable Logistic Regressions for Men’s Current MC Use and Future FP Use (N=885)
| Current MC | Future FP | |||
|---|---|---|---|---|
| Wald Chi-Squared Test (17) | 137.07 | 234.97 | ||
| Odds Ratio | 95% CI | Odds Ratio | 95% CI | |
| Village | 0.89 | 0.32, 2.51 | 0.90 | 0.39, 2.11 |
| Men’s Village Factors for FP | ||||
| Network Size | 0.65 | 0.33, 1.28 | 1.16 | 0.65, 2.07 |
| Network Outside of Village | 0.96 | 0.94, 0.99 | 1.01 | 0.98, 1.03 |
| Network Non-Relative | 0.99 | 0.97, 1.02 | 1.03 | 1.00, 1.05 |
| Network FP Approval | 0.97 | 0.95, 0.99 | 1.02 | 1.00, 1.04 |
| Network FP Communication | 1.03 | 0.98, 1.08 | 1.00 | 0.96, 1.04 |
| FP Acceptability | 1.02 | 0.98, 1.05 | 1.02 | 1.00, 1.05 |
| Disagree that FP Sanctions exist | 0.91 | 0.65, 1.28 | 1.14 | 0.87, 1.50 |
| Men’s Couple & Individual Factors for FP | ||||
| At least one wife approves of FP | 1.60 | 0.93, 2.75 | 4.96 | 3.17, 7.77 |
| Wife in Network | 1.19 | 0.73, 1.93 | 0.83 | 0.51, 1.37 |
| Couple Communication about FP | 1.39 | 1.13, 1.70 | 1.93 | 1.54, 2.43 |
| Self-Efficacy to Discuss FP | 0.96 | 0.76, 1.20 | 1.76 | 1.43, 2.18 |
| Self-Efficacy to Use FP | 0.73 | 0.40, 1.32 | 1.22 | 0.75, 1.96 |
| FP Access | 2.93 | 2.10, 4.10 | 1.75 | 1.37, 2.23 |
| Covariates | ||||
| Age Group (>34 ref) | ||||
| 18-34 | 0.96 | 0.59, 1.55 | 1.42 | 0.90, 2.24 |
| Education (None ref) | ||||
| Primary | 1.23 | 0.75, 2.00 | 1.14 | 0.73, 1.77 |
| Secondary or more | 1.71 | 1.01, 2.90 | 1.08 | 0.65, 1.80 |
| Number of Living Children (5 or more ref) | ||||
| None or 1 | 0.24 | 0.10, 0.57 | 1.33 | 0.65, 2.74 |
| 2-4 | 0.65 | 0.38, 1.11 | 1.05 | 0.62, 1.76 |
| Multiple Wives | 1.00 | 0.61, 1.66 | 1.64 | 1.00, 2.72 |
| Non-Christian Religion | 1.17 | 0.69, 1.98 | 0.67 | 0.41, 1.09 |
We had 885 men in the analysis clustered into 32 villages after dropping men missing data on their wife’s approval of modern FP use. Table 5 presents the bivariate and multivariable results examining how village level factors (i.e., the network and social norms variables) are associated with men’s reported current use of MC, controlling for couple-level and individual-level factors. Table 6 is the comparable table for the association with men’s intended use of FP in the future.
In bivariate models (Table 5), most network variables were not closely related to current MC use or intention to use FP in the future. However, those with larger networks had a lower odds of using MC (OR: 0.61; 95% CI: 0.37, 1.02) but a higher odds of intention to use FP in the future (OR: 1.39; 95% CI: 0.95, 2.03) compared to those with smaller networks. Additionally, men disagreeing with FP sanctions had a higher odds of currently using MC than those that agreed with FP sanctions (OR: 1.23; 95% CI: 0.84, 1.82) but a lower odds of future FP use intention (OR: 0.68; 95% CI: 0.52, 0.88) compared to men that agreed that FP sanctions exist. Most network variable associations were not statistically significant. Couple-level variables were significantly related to current MC use with, for example, those communicating with their wife about FP having a higher odds of currently using MC (OR: 2.10; 95% CI: 1.77, 2.49) and of intending to use FP in the future (OR: 3.07; 95% CI: 2.52, 3.74) than those not communicating with their wife. Individual level factors were also significantly related to current MC use and intention to use FP in the future with, for example, those with high self-efficacy to discuss FP having a higher odds of using MC (OR: 1.44; 95% CI: 1.20, 1.72) and of intending to use FP (OR: 2.79; 95% CI: 2.37, 3.29) than those with low self-efficacy.
In multivariable models (Table 6), village level network and norm variables’ associations were close to an OR of 1.00, the null value. For example, men with a larger percentage of their network from outside of their village had an odds that were near the null value of 1.00 for both current MC use (OR=0.96; 95% CI=0.94, 0.99) and future FP use (OR=1.01; 95% CI=0.98, 1.03). We obtained predicted probabilities for those at the 25th and 75th percentiles on the scale of the covariate of each of the village-level network and norm variables and we did not see significant differences in predicted margins for either current MC or future FP use.
Regarding couple variables, results were similar in both multivariable and bivariate models. However, once network and individual FP and demographic factors were included in the multivariable model, the strength of the relationship between couple level variables and FP decreased and some relationships were no longer statistically significant. Men who believed their wife approved of FP had a higher odds of both current (OR=1.60; 95% CI=0.93, 2.75), though this relationship is not statistically significant, and intended FP use (OR=4.96; 95% CI=3.17, 7.77). Men who communicated with their wife about FP also had a higher odds of current and intended FP use (Current MC: OR=1.39; 95% CI=1.13,1.70) (Future FP: OR=1.93; 95% CI=1.54, 2.43). Men listing their wife in their network had a higher odds of current use (OR: 1.19; 95% CI: 0.73, 1.93) and a lower odds of intended use (OR: 0.83; 95% CI: 0.51, 1.37); neither of these were significant.
Similar to couple level variables, results for individual factors related to FP had a similar relationship in bivariate and multivariable models but the strength of the relationship between these variables and FP was attenuated in multivariable models and some relationships were no longer statistically significant. Self-efficacy to discuss FP was not significantly related to current use (OR: 0.96; 95% CI: 0.76, 1.20) but those with higher self-efficacy to discuss FP did have a higher odds of future FP use (OR=1.76; 95% CI=1.43, 2.18). Those with more FP access had a higher odds of both current MC (OR=2.93; 95% CI=2.10, 4.10) and future FP use (OR=1.75; 95% CI=1.37, 2.23).
IV. Discussion
This study explored associations between men’s social networks and social norms related to FP use among men in Benin. It provides insights into the composition of men’s networks and how FP use may be related to men’s social networks and norms in sub-Saharan Africa given the prior focus on women’s networks. Our work has three main findings related to network and normative factors affecting men’s FP use: (1) men’s networks are small; (2) more men believe that discussing and using FP is acceptable in their villages than have actually spoken about FP; and, (3) couple-level factors remain associated with men’s use of FP after accounting for village-level indicators.
First, we find that men have small networks and that about 11% of men listed zero network contacts. This contrasts with literature on women’s networks in sub-Saharan Africa, which finds that women have, on average, between four and 18 network members and speak with a high proportion of network members about FP (Alvergne et al., 2011; Behrman et al., 2002; Madhavan et al., 2005). Men’s network size has been found to increase the probability of talking with their wife about FP in Kenya, which points towards the influence of social network size on a couples’ dialogue (Musalia, 2003). The size of men’s networks and their engagement in FP-related conversation with network members is also likely context specific and steeped in gender norms, as research in high-income countries has found that men talk to a higher proportion of their social network about condom use than women do (Choi & Gregorich, 2009). However, men’s small network size may indicate that social network questions were not well-phrased (i.e., men may not think of their social network as people they rely on for support) or that data collectors did not probe sufficiently with men about their network contacts. It is important for future work to co-create a definition for social network members with men in this context.
Our second finding is that more men believe that FP discussion is acceptable in their village than believe that their network members or spouse approve of FP use. At the village level, 86% of men believe it is acceptable to discuss FP in their village, while, on average, men believe that only one-third of their networks approve of FP. Additionally, more men perceive that others approve of FP use than actually communicate about FP at the village level. Prior work finds that men make assumptions about their network members’ FP use, meaning that they report their network members’ approval of FP based on their friends’ child spacing or family size (Paz Soldan, 2004). In contrast, women tend to talk with their network about FP directly and then use this information to decipher their perception of their networks’ approval of FP (Alvergne et al., 2011; Paz Soldan, 2004). At the couple level, more men also believe that their wives approve of FP than have discussed childbearing, FP method choice, or obtaining FP with their wives. Likely due to this lack of communication with their wives, men’s perceived opposition to FP continues to serve as a key barrier to FP use as reported by women in Benin (Guttmacher Institute, 2018). In sum, at both the village and couple level, a larger percentage of men think that FP is acceptable to discuss than think others approve of its use or actually discuss FP. These findings indicate both a need and opportunity for increased FP related dialogue in these villages and among couples. They also may indicate that social norms are important, as more men believe there is a norm that supports FP use than have communicated about FP use.
Our third main finding is that couple-level factors have a strong relationship to FP use even when accounting for village-level factors. This corroborates decades of research showing that the husband-wife dyad is important in FP decision-making (Lasee & Becker, 1997; Rimal et al., 2015; Wegs et al., 2016), and recent work in Benin that found both couple-level and village-level factors are crucial for achieving FP need (Igras et al., 2021). Most studies with women participants find that couple-level factors are important, namely that a woman’s perception of her partner’s approval is influential in her FP decision-making (Alvergne et al., 2011; Samandari et al., 2010). We find this connection to be salient even after controlling for social and individual characteristics, as a spouse’s perceived approval and couple communication remain associated with FP use. At the same time, prior work in Kenya has found that larger social networks among men increase the probability of FP discussions amongst couples, indicating that the village level may remain important for FP even if it manifests in FP communication and dialogue at the couple level (Musalia, 2003).
Interestingly, although couple communication about FP and perceived wife’s approval of FP are influential, few men listed their wife in their material, practical, or emotional support networks, some have not communicated with their wives about FP, and over 40% do not believe their spouse approves of FP. As one level of FP decision-making takes place at the couple level, it is important that programs consider strategies that support men in engaging their partners in FP conversations. Simultaneously, and related to our conceptual model, it is important that programs continue to emphasize men’s networks discussing FP, as this dialogue can then diffuse down to the couple level and affect change (Musalia, 2003). Lastly, it is important to explore why men’s wives were infrequently mentioned as part of their husbands networks (e.g., gender roles, difficulty of network questions).
This analysis provides a rich description of men’s networks and norms related to FP and re-emphasizes the importance of the husband-wife dyad in FP decision-making. Building on our socio-ecological model and TJ’s unique design, we were able to assess a number of variables of interest and related covariates at the village, couple, and individual levels that have been shown to influence FP use. However, future research is needed. For instance, the socio-ecological framework extends beyond the village level and into the societal and policy level (i.e., investments in national FP programs) (Igras et al., 2021; Schölmerich & Kawachi, 2016). Future work should include indicators at this additional level in analyses that focus on men. The relationship between the factors in our model and FP use may also change over time as Benin’s MC prevalence rate increases in future years (Alvergne et al., 2011). Thus, the MC prevalence rate itself may affect how strongly indicators such as social norms are related to FP use, indicating the need for this research to be ongoing. Another possibility is that an individual’s parity or age may modify the relationship between FP factors and FP use (Madhavan et al., 2005; Samandari et al., 2010). Future research should also further explore men’s networks, the barriers to discussing FP with those in the network, and how these networks and barriers related to them change throughout the life course.
Limitations
Multiple limitations warrant discussion. First, we are unable to match men and women’s data from households to confirm if men’s perceptions of their wives’ beliefs or behaviors are concordant (i.e., if their wife does use FP). Thus, we are unable to confirm that our measures of FP use align with actual use. It is also possible that men do not always know if their wives' use FP. Second, network data is more difficult to collect than traditional survey data in several respects. For example, the boundaries of social networks are often unknown and respondents may have experienced fatigue with naming all network members. Further, many men (N=145) did not answer the question as to whether or not their wife approved of FP. This high missingness had implications for our multivariable model, as incomplete data were dropped from further analysis. Additionally, men may have had differing conceptions of what “network” was referring to. While many men may did not list their wives in their network, this may because they were conceptualizing their network outside of the home. Third, our question related to the acceptability of FP discussions and FP sanctions in the man’s village did not specify a referent group. The acceptability to discuss FP likely varies based on whether men are talking with, for example, their wives, with each other, or with elders. Men may also have answered sanction-related questions differently by referent group (e.g., village chief, male relative). Fourth, our findings at the couple level have one caveat. Men were asked about their own or their wives’ FP use, as the majority of methods are woman-directed, rather than men’s own use alone. This specific question may be more influenced by interactions within the husband-wife dyad than by men’s personal use, which may be more influenced by village level factors. Fifth, the outcome for intention to use asked about any future intended use rather than imminent use, which may have produced different results. Future studies should obtain information on intention to use in the next year or ever and see if and how the association between network and norm variables and these FP intention-related outcomes changes. Lastly, it is possible that endogeneity is present, as FP use itself may affect village-level or couple communication about FP. However, the study design is not equipped to address this issue and thus the results should be interpreted with caution.
Conclusions
In our sample in Benin, men had few social network contacts and even fewer contacts with whom they discussed FP or that they perceived approve of FP use. Yet, there is high social acceptability for FP discussion. Social network-based approaches that harness men and women’s social networks hold promise for accelerating FP communication and uptake. Additionally, surveys conducted post-TJ intervention have found that networks have influenced FP use and couple communication, further indicating that these social network-based approaches ignite change (IRH, 2016). Through unpacking men’s social networks and norms and their relationship to FP use in addition to couple-level indicators, this analysis enables researchers and development organizations to strategize how to better engage Beninese men and men throughout sub-Saharan Africa in FP programs. These findings emphasize the need to increase FP-related dialogue to encourage greater information flow among men’s networks and within the husband-wife dyad to better reach villages in Benin where MC rates are low and unmet need for FP is high.
Table 3:
Current and Future Intended FP Use as Reported by Men
| (N=885) | ||
|---|---|---|
| n | % | |
| Future FP Use | ||
| Intended Future Use of FP | 476 | 53.79 |
| Current FP Use | ||
| Current Use of Family Planning | 308 | 34.8 |
| Traditional methods | 115 | 12.99 |
| Modern contraception | 193 | 21.81 |
Acknowledgments
Funding Details: Tékponon Jikuagou was supported by the United States Agency for International Development (USAID) [AID-OAA-A-10_00066]. The Carolina Population Center provided general and training support (P2C-HD050924; T32-HD091058) from the NIH.
Footnotes
Declaration of Interest: No potential competing interest was reported by the authors.
Data Availability:
The data that support the findings of this study are available from the Institute of Reproductive Health at Georgetown University.
References
- Agadjanian V (2001). Religion, social milieu, and the contraceptive revolution. Population Studies, 55(2), 135–148. [Google Scholar]
- Alvergne A, Gibson MA, Gurmu E, & Mace R (2011). Social Transmission and the Spread of Modern Contraception in Rural Ethiopia. PLOS ONE, 6(7), 1–10. 10.1371/journal.pone.0022515 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bankole A, & Singh S (1998). Couples’ Fertility and Contraceptive Decision-Making in Developing Countries: Hearing the Man’s Voice. International Family Planning Perspectives, 24(1), 15–24. [Google Scholar]
- Behrman JR, Kohler H-P, & Watkins SC (2002). Social networks and changes in contraceptive use over time: Evidence from a longitudinal study in rural Kenya. Demography, 39(4), 713–738. 10.1353/dem.2002.0033 [DOI] [PubMed] [Google Scholar]
- Bicchieri C (2016). Norms in the Wild. How to Diagnose, Measure, and Change Social Norms. Oxford University Press. [Google Scholar]
- Blackstone SR, Nwaozuru U, & Iwelunmor J (2017). Factors Influencing Contraceptive Use in Sub-Saharan Africa: A Systematic Review. International Quarterly of Community Health Education, 37(2), 79–91. 10.1177/0272684X16685254 [DOI] [PubMed] [Google Scholar]
- Bronfenbrenner U (1979). Ecological Models of Human Development. In Gauvain M & Cole M (Eds.), Readings on the Development of Children (4th ed., pp. 3–8). Worth Publishers. [Google Scholar]
- Buesseler H, & Diakité M (2013). Topline Results of a Rapid Assessment of Barriers to Family Planning Use. https://www.thecompassforsbc.org/Project-Examples/Topline-Results-Rapid-Assessment-Barriers-Family-Planning-Use
- Casterline J, & Sinding S (2000). Unmet Need for Family Planning in Developing Countries and Implications. Population and Development Review, 26(4), 691–723. [Google Scholar]
- Choi K-H, & Gregorich SE (2009). Social network influences on male and female condom use among women attending family planning clinics in the United States. Sexually Transmitted Diseases, 36(12), 757–762. 10.1097/OLQ.0b013e3181afefc1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chung A, & Rimal RN (2016). Social Norms: A Review. Review of Communication Research, 4, 1–28. 10.12840/issn.2255-4165.2016.04.01.008 [DOI] [Google Scholar]
- Cislaghi B, & Heise L (2019). Using social norms theory for health promotion in low-income countries. Health Promotion International, 34(3), 616–623. 10.1093/heapro/day017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cleland J, Bernstein S, Ezeh A, Faundes A, Glasier A, & Innis J (2006). Family planning: the unfinished agenda. Lancet, 368(9549), 1810–1827. 10.1016/S0140-6736(06)69480-4 [DOI] [PubMed] [Google Scholar]
- Cochrane S (1979). Fertility and education: what do we really know? In Johns Hopkins University Press. World Bank Staff Occasional Papers. [Google Scholar]
- Costenbader E, Lenzi R, Hershow RB, Ashburn K, & McCarraher DR (2017). Measurement of Social Norms Affecting Modern Contraceptive Use: A Literature Review. Studies in Family Planning, 48(4), 377–389. [DOI] [PubMed] [Google Scholar]
- Figueroa M, Kincaid D, Rani M, & Lewis G (2002). Communication for Social Change: An Integrated Model for Measuring the Process and Its Outcomes. [Google Scholar]
- FP2020. (2016). 2016 Fp2020 Annual Commitment Update Questionnaire Response.
- Government of Benin. (2018). Engagments FP2020.
- Guttmacher Institute. (2018). Contraceptive Use in Benin. https://www.guttmacher.org/fact-sheet/contraceptive-use-benin
- Herbert S (2015). Social norms, contraception and family planning. [Google Scholar]
- Igras S, Burgess S, Chantelois-Kashal H, Diakité M, Giuffrida M, & Lundgren R (2021). Pathways to Modern Family Planning: A Longitudinal Study on Social Influence among Men and Women in Benin. Studies in Family Planning, 52(1), 59–76. 10.1111/sifp.12145 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Igras S, Diakité M, & Lundgren R (2017). Moving from theory to practice: A participatory social network mapping approach to address unmet need for family planning in Benin. Global Public Health, 12(7), 909–926. 10.1080/17441692.2016.1147589 [DOI] [PubMed] [Google Scholar]
- INSAE, & ICF International. (2013). Enquête Démographique et de Santé du Bénin 2011-2012.
- IRH. (2016). Projet Tékponon Jikuagou Répondre aux Besoins Non Satisfaits de Planification Familiale : Résultats de la Phase d’Extension: Ouémé, Atlantique.
- IRH. (2017). Tékponon Jikuagou: Final Report.
- Kadushin C (2012). Understanding Social Networks: Theories, Concepts, and Findings. Oxford University Press. [Google Scholar]
- Khan S, Mishra V, Arnold F, & Abderrahim N (2007). Contraceptive Trends in Developing Countries. In DHS Comparative Reports. [Google Scholar]
- Kohler H-P, Behrman JR, & Watkins SC (2001). The density of social networks and fertility decisions: Evidence from South Nyanza District, Kenya. Demography, 38(1), 43–58. 10.1353/dem.2001.0005 [DOI] [PubMed] [Google Scholar]
- Lasee A, & Becker S (1997). Husband-Wife Communication About Family Planning and Contraceptive Use in Kenya. International Family Planning Perspectives, 23(1), 15–33. 10.2307/2950781 [DOI] [Google Scholar]
- Madhavan S, Adams A, Simon D, & Adams AA (2005). Women’ s Networks and the Social World Of Fertility Behavior. International Family Planning Perspectives, 29(2), 58–68. [DOI] [PubMed] [Google Scholar]
- Musalia JM (2003). Extraconjugal Determinants of Spousal Communication About Family Planning in Kenya. Sex Roles, 49(11), 597–607. 10.1023/B:SERS.0000003130.04774.a1 [DOI] [Google Scholar]
- Nöstlinger C, Nideröst S, Gredig D, Platteau T, Gordillo V, Roulin C, Rickenbach M, Dias SF, & Rojas D (2010). Condom use with steady partners among heterosexual people living with HIV in Europe: testing the information-motivation-behavioral skills model. AIDS Patient Care and STDs, 24(12), 771–780. [DOI] [PubMed] [Google Scholar]
- Oheneba-Sakyi Y, & Takyi B (1997). Effects of couples’ characteristics on contraceptive use in sub-Saharan Africa: the Ghanaian example. J Biosoc Sci, 29, 33–49. [DOI] [PubMed] [Google Scholar]
- Parker R, & Sommer M (Eds.). (2010). Routledge Handbook of Global Public Health (1st ed.). Routledge. [Google Scholar]
- Paz Soldan VA (2004). How family planning ideas are spread within social groups in rural Malawi. Studies in Family Planning, 35(4), 275–290. [DOI] [PubMed] [Google Scholar]
- Rimal RN, Sripad P, Speizer IS, & Calhoun LM (2015). Interpersonal communication as an agent of normative influence: a mixed method study among the urban poor in India. Reproductive Health, 12(1), 71. 10.1186/s12978-015-0061-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Samandari G, Speizer IS, & O’Connell K (2010). The Role of Social Support and Parity On Contraceptive Use in Cambodia. International Perspectives on Sexual and Reproductive Health, 36(3), 122–131. [DOI] [PubMed] [Google Scholar]
- Sanusi A, Akinyemi O, & Onoviran O (2014). Do knowledge and cultural perceptions of modern female contraceptives predict male involvement in Ayete, Nigeria? African Journal of Reproductive Health, 18, 105–114. [PubMed] [Google Scholar]
- Schölmerich VLN, & Kawachi I (2016). Translating the Social-Ecological Perspective Into Multilevel Interventions for Family Planning: How Far Are We? Health Education & Behavior, 43(3), 246–255. 10.1177/1090198116629442 [DOI] [PubMed] [Google Scholar]
- Sedgh G, & Hussain R (2014). Reasons for Contraceptive Nonuse among Women Having Unmet Need for Contraception in Developing Countries. Studies in Family Planning, 45(2), 151–169. 10.1111/j.1728-4465.2014.00382.x [DOI] [PubMed] [Google Scholar]
- Shah NM (1974). The Role of Interspousal Communication in Adoption of Family Planning Methods: A Couple Approach. The Pakistan Development Review, 13(4), 452–469. http://www.jstor.org/stable/41258259 [PubMed] [Google Scholar]
- Shakya HB, Challa S, Nouhou AM, Vera-Monroy R, Carter N, & Silverman J (2020). Social network and social normative characteristics of married female adolescents in Dosso, Niger: Associations with modern contraceptive use. Global Public Health, 1–17. 10.1080/17441692.2020.1836245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shattuck D, Kerner B, Gilles K, Hartmann M, Ng’ombe T, & Guest G (2011). Encouraging contraceptive uptake by motivating men to communicate about family planning: The Malawi Male Motivator project. American Journal of Public Health, 101(6), 1089–1095. 10.2105/AJPH.2010.300091 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stefanik L, & Hwang T (2017). Applying Theory to Practice: CARE’s Journey Piloting Social Norms Measures for Gender Programming. [Google Scholar]
- The Learning Collaborative to Advance Normative Change. (2019). Social Norms and AYSRH: Building a Bridge from Theory to Program Design.
- The World Bank. (2015a). Infant Mortality Rate.
- The World Bank. (2015b). Maternal Mortality Ratio.
- Udry JR (1982). The effect of normative pressures on fertility. Population and Environment, 5(2), 109–122. 10.1007/BF01367490 [DOI] [Google Scholar]
- UNFPA. (2014). The Global Programme to Enhance Reproductive Health Commodity Security Annual Report 2013.
- Valente T (2010). Social Networks and Health: Models, Methods, and Applications. Oxford Scholarship. [Google Scholar]
- Wang R, & Wang H (2005). Prebirth psychosocial factors as predictors of consistency in contraceptive use among Taiwanese adolescent mothers at 6 months postpartum. Public Health Nursing, 22(4), 271–279. [DOI] [PubMed] [Google Scholar]
- Wegs C, Creanga AA, Galavotti C, & Wamalwa E (2016). Community Dialogue to Shift Social Norms and Enable Family Planning: An Evaluation of the Family Planning Results Initiative in Kenya. PLOS ONE, 11(4), 1–23. 10.1371/journal.pone.0153907 [DOI] [PMC free article] [PubMed] [Google Scholar]
- WHO. (2007). Report of a WHO Technical Consultation on Birth Spacing. World Health Organization. [Google Scholar]
- WHO. (2014). WHO ∣ Unsafe abortion: global and regional estimates of the incidence of unsafe abortion and associated mortality in 2008. Who, 5th editio, 1–67. 10.1017/CBO9781107415324.004 [DOI] [Google Scholar]
- WHO. (2017). Family planning/Contraception.
- Yzer M (2012). The integrative model of behavioral prediction as a tool for designing health messages. In Cho H (Ed.), Health Communication Message Design: Theory and Practice. Sage Publications. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the Institute of Reproductive Health at Georgetown University.