

Abstract
The ongoing coronavirus pandemic threatens physical and psychological health. We examined whether social dominance orientation (SDO), a preference for inequality among social groups, contributes to mental health during the pandemic. In particular, we predicted that people high in SDO would experience higher levels of depression than others low in SDO. Our results (N = 2008) showed that SDO was positively associated with depression. In addition, participants' perceived lifestyle changes moderated the association between SDO and depression. We also discuss the theoretical and practical implications of the current work.
Keywords: Social dominance orientation, Depression, Lifestyle change, Mental health, COVID-19
For much as men differ with regard to places in which they live, or in the law of their daily life, or in natural bent, or in active pursuits, or in whatever else man differs from man, in the case of this disease alone the difference availed naught.
—Procopius, History of the War
1. Introduction
During the prevalence of a disease, nearly everyone is at risk of being infected. As Procopius observed during the Plague of Justinian, no matter where you live and no matter who you are, everyone is equal when facing the plague. Similarly, the ongoing outbreak of the 2019 coronavirus disease (COVID-19) seriously threatens people's physical and psychological health, interrupts people's regular work and life, and generates other economic and social issues such as unemployment across the globe. More importantly, with the extremely high infection rate of the COVID-19, not only ordinary people but many well-known ones have also been reported to get sick (e.g., Tom Hanks and Boris Johnson), convincing people that everyone is equally at risk of infection. During the outbreak, people naturally experienced poor well-being (e.g., feeling depressed), but some people are indeed influenced more. It is crucial to understand who might be at higher risk for depression in the ongoing pandemic. Intuitively, the perceived risk of infection should induce depression. However, this study aimed to explore this issue with a factor that seems unrelated to the outbreak, that is, social dominance orientation (SDO), and test whether people with higher SDO experience a reduced level of well-being (i.e., depression in the current case).
1.1. Social dominance orientation
Social dominance orientation reflects the extent to which an individual prefers intergroup relationships to be equal or hierarchical (Pratto et al., 1994). SDO is grounded in the social dominance theory, which postulates that people have a fundamental individual orientation to accept and justify different forms of social inequality (e.g., Racism; Sidanius, 1993). SDO is a predisposition toward anti-egalitarianism within and between groups; in general, people with higher SDO may favor their in-group members before the out-group members, whereas those with lower SDO may expect equality between the two groups. Empirically, Pratto and colleagues developed the Social Dominance Orientation Scale to measure the SDO level (Pratto et al., 1994); indeed, it is a powerful predictor of social and political attitudes. Previous studies have found that individuals with higher SDO exhibit stronger negative attitudes toward others regarding their gender (Pratto et al., 1994), ethnicity (Pratto et al., 1994), social class (Guimond et al., 2003), sexual orientation (Whitley & Lee, 2000), and among others. In addition to this interpersonal dominance phenomenon, what are the personal outcomes for those higher in SDO? Can this be harmful to others but beneficial for the self?
Compared to other right-wing ideological attitudes (e.g., right-wing authoritarianism), relatively few studies have focused on the relationship between SDO and well-being, with inconsistent findings (Onraet et al., 2013). For example, Van Hiel and Kossowska (2006) found that SDO was negatively associated with well-being, as measured by emotion expression. However, De Cremer et al. (2008) found that higher SDO can increase positive affect when people have the voice. In the study by de Zavala et al. (2009), a null relationship was found. A more recent meta-analysis suggests that the mixed findings may be due to different well-being indicators (Onraet et al., 2013). Specifically, there was a moderate and significant effect between SDO and intrinsic goals (e.g., self-development and affiliation with others), but no significant SDO effects on positive and negative affect and life satisfaction. Since very few studies have investigated this issue, and specifically, to our knowledge, no previous studies have examined the association between SDO and depression, the current work aimed to fill this research gap. We argue that SDO is positively associated with depression and elaborate on our thinking as follows.
The high infection rate of the COVID-19 forces nearly everyone to face the risk of being infected. Obviously, acquiring an infection of COVID-19 does not depend on someone's SDO; that is, regardless of whether one is higher or lower in SDO, ordinary people should have a similar infectious risk. Specifically, many famous people have been reported to be infected, which suggests that everyone is equal before the virus. The equality of health versus illness, or even life versus death, conflicts with individuals' beliefs in hierarchy and inequality, and thus might result in poor well-being experience. Indeed, many studies have suggested that conflicting beliefs impair well-being. For example, in an individual's value system, a few individual-oriented beliefs (e.g., materialism) stand in conflict with other collective-oriented beliefs, which reduces individuals' well-being (Burroughs & Rindfleisch, 2002). As the current outbreak can induce the perception of equality, which seems to conflict with the view of accepting and justifying social inequality, we hypothesized that participants scoring high in SDO would report poor well-being (i.e., more depression in this case). We also examined a moderator that might influence the relationship between SDO and depression and lifestyle changes.
1.2. The moderating role of lifestyle changes
Self-quarantine, one of the most useful ways to fight the spread of COVID-19, has been recommended by the World Health Organization (https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public). Self-quarantine can cause lifestyle differences from regular days for most people. Previous studies have suggested that shifts in lifestyle negatively impact psychological health (Nea et al., 2018). While a deviation from the existing structured lifestyle could have a negative effect on psychological well-being for most people, such an effect should be more pronounced for people high in SDO. Although we do not have direct evidence to link SDO and lifestyle changes, indirect evidence supports SDO as being negatively associated with openness (Heaven & Bucci, 2001), characterized as the extent to which one accepts novel experiences. In addition, several political psychological studies suggest that people with higher SDO are more conservative, prefer to maintain the status quo, and are opposed to significant changes in their lives (e.g., protest; Carney et al., 2008; also see Becker, 2019, for a review). That one's regular lifestyle has been broken is treated as a novel experience and great changes; thus, people with higher SDO should be more affected.
1.3. The present research
The present study aimed to test two hypotheses: a) SDO can positively predict individuals' depression, and b) the association is moderated by lifestyle changes. The research design was approved by the institutional ethical committee of the first author's university (Ethics Approval: EA2003002).
2. Methods
2.1. Participants
We recruited 2008 participants from February 22nd to March 1st, 2020. The data were collected through a Chinese website (Wenjuanxing; www.wjx.com), similar to Amazon Mechanical Turk. Of the participants, 608 were men, and 1400 were women. Their mean age was 21.49 (SD = 5.23; range, 18–57 years). We conducted a sensitivity analysis with α = 0.05, β = 0.80, and the current sample size, showing that the minimum effect size (f 2) of 0.007 could be detected. Participants took part in the study voluntarily.
2.2. Procedures and measures
Participants were instructed to work on measures assessing their SDO, lifestyle changes, and depression. After completing these measures, participants reported their demographic information (i.e., gender and age). Finally, they were thanked and debriefed.
2.2.1. Social dominance orientation
SDO was assessed using four items taken from the Social Dominance Orientation Scale (SDOS; Pratto et al., 1994). An example item is “Some groups of people are simply inferior to other groups.” Responses were made on a 7-point Likert scale ranging from 1 (not at all) to 7 (very much). All scores were averaged to form an index to indicate the SDO level, with higher scores corresponding to higher levels of SDO (Cronbach's α = 0.603).
2.2.2. Lifestyle changes
We assessed participants' perceived lifestyle changes with one question, “How different is your present lifestyle from your past?” Participants responded on a 7-point Likert scale, ranging from 1 = not different at all to 7 = extremely different.
2.2.3. Depression
We used the Patient Health Questionnaire (PHQ; Spitzer et al., 1999), consisting of nine items, to measure participants' depression. A previous study suggested that it can be used in the general population (Kroenke et al., 2001). We modified the items slightly to adapt them to the current COVID-19 situation. Participants reported how often they had been bothered by the problems indicated for each item. For example, during the outbreak of COVID-19, “I am feeling down, depressed, or hopeless,” on a scale ranging from 0 (not at all) to 3 (very often). The scores were averaged to form one index of their depression level (α = 0.901).
2.2.4. Covariates
Participants then reported their perception of COVD-19 on two items. One item was used to measure the current disease's perceived mortality rate, “How high is the mortality rate of COVID-19?,” and the other perceived infection rate, “How high is the infection rate of COVID-19?” Participants responded to a 7-Likert scale (1 = extremely low to 7 = extremely high). Additionally, participants indicated their subjective social status on the MacArthur scale, which presents an image with a ladder containing ten rungs (Adler et al., 2000). Participants were informed that this ladder represented China's social status and were required to select one rung to represent their perceived status relative to others (M = 4.61, SD = 1.64).
3. Results
3.1. SDO positively predicted depression
Table 1 presents the descriptive statistics and intercorrelations between the study variables. The results showed that participants who perceived significant lifestyle changes reported stronger depression (r = 0.38); participants with higher SDO also felt greater depression (r = 0.20).
Table 1.
Descriptive statistics and correlations of each variable.
| Variables | M (SD) | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|---|
| 1. SSS | 4.61 (1.64) | − | ||||||
| 2. Age | 21.49 (5.23) | 0.06⁎⁎ | − | |||||
| 3. IR | 3.46 (2.06) | −0.08⁎⁎⁎ | 0.02 | − | ||||
| 4. MR | 4.57 (2.06) | −0.02 | −0.06⁎ | 0.33⁎⁎⁎ | − | |||
| 5. LC | 3.83 (1.65) | −0.04 | −0.01 | 0.08⁎⁎⁎ | 0.11⁎⁎⁎ | − | ||
| 6. SDO | 2.81 (1.10) | 0.02 | 0.04 | 0.02 | 0.00 | 0.07⁎⁎ | − | |
| 7. Depression | 1.63 (0.57) | −0.11⁎⁎⁎ | −0.02 | 0.13⁎⁎⁎ | 0.07⁎⁎ | 0.38⁎⁎⁎ | 0.20⁎⁎⁎ | − |
Note. SSS = subjective social status; IR = infection rate; MR = mortality rate; LC = lifestyle changes; SDO = social dominance orientation.
p < .05.
p < .01.
p < .001.
We conducted a regression analysis of the extent to which SDO predicted depression and found that SDO was positively related to depression (B = 0.10, SE = 0.01, p < .001). We controlled the perception of COVID-19 (IR: infection rate; MR: mortality rate) and demographic variables, including gender and subjective social status (SSS). Since 189 participants did not report their age, and there was no significant correlation between age and depression, we did not include age in the final regression. The association remained significant after controlling for these covariates (B = 0.11, p < .001).
3.2. The moderating effect of lifestyle changes
To examine the moderated effect of lifestyle changes (LC), we regressed LC (centered) and SDO (centered) in the first step and their interaction in the second step onto depression, controlling for the covariates mentioned above. All results are shown in Table 2 .
Table 2.
Regression results predicting depression (PHQ).
| Variables | B | SE | β | t | p |
|---|---|---|---|---|---|
| Gender (0 = women, 1 = men) | 0.02 | 0.02 | 0.01 | 0.70 | .486 |
| SSS | −0.03 | 0.01 | −0.10 | −4.86 | <.001 |
| IR | 0.02 | 0.01 | 0.09 | 4.14 | <.001 |
| MR | 0.00 | 0.01 | 0.00 | 0.07 | .948 |
| LC | 0.12 | 0.01 | 0.35 | 17.44 | <.001 |
| SDO | 0.09 | 0.01 | 0.18 | 8.54 | <.001 |
| LC × SDO | 0.02 | 0.01 | 0.05 | 2.49 | .013 |
| R2 = 0.19 | |||||
| F (7, 2000) = 68.19, p < .001 | |||||
Note. SSS = subjective social status; IR = infection rate; MR = mortality rate; LC = lifestyle changes; SDO = social dominance orientation.
As the interaction of SDO and LC on depression was significant, simple slope tests were performed, indicating that the positive effect of SDO on depression was stronger when the participants perceived more significant changes in their lifestyle (B = 0.16, p < .001) rather than less change (B = 0.07, p < .001). (see Fig. 1 ).
Fig. 1.
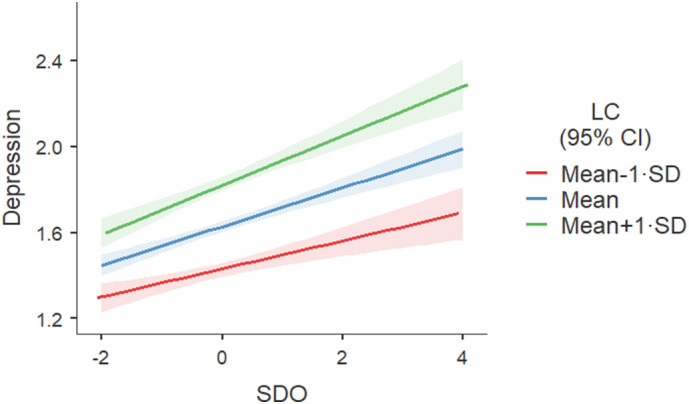
The moderating effect of lifestyle change (LC) and social dominance orientation (SDO) on depression.
These findings support our hypothesis that SDO is positively associated with depression. More importantly, this effect was stronger when people felt greater changes in their lifestyle.
4. Discussion
The current prevalence of COVID-19 threatens people's well-being. We predicted that those with high SDO would be more strongly affected, as their inequality belief toward people conflicts with the current situation in which everyone has an almost equal risk of infection. Supporting this prediction, our results revealed that people with higher SDO experienced stronger depression, even after controlling for the pandemic outbreak's perception. Moreover, greater lifestyle changes could also intensify the association between SDO and depression.
4.1. Contributions
Our study contributes to the literature on SDO. Based on social dominance theory, previous studies have mainly examined its adverse interpersonal outcomes (e.g., dehumanization; Hodson & Costello, 2007). Our study focused on its intrapersonal effect. Specifically, to our knowledge, this study is the first to examine the association between SDO and depression empirically, which broadens our understanding of SDO's dark side on well-being. This finding is consistent with Van Hiel and Kossowska (2006) but in contrast with MacInnis et al. (2013). This disagreement may be due to the indicators of well-being used. Well-being is a broad psychological construct that encompasses several components, such as subjective well-being (e.g., life satisfaction), self-evaluation (e.g., self-esteem), and others (e.g., anxiety and depression, Diener & Lucas, 1999; see also Dittmar et al., 2014). SDO may have different strengths and even directions with different components of well-being. The meta-analysis suggested that SDO has a significant negative relationship with self-esteem but a weak negative relationship with positive affect (Onraet et al., 2013). As SDO's empirical studies are limited, we urge that future studies further examine the association between SDO and different well-being components.
It should be noted that although our study took place during the COVID-19, it did not mean that the results would be different without the pandemic. Indeed, several similar beliefs, other than the perception of infection, may also strike those with high SDO, leading to stronger negative outcomes. For example, time is equal for everyone; each person has 24 h per day. Thus, perceiving time crawling may be frustrating everyone, but more on those scoring high in SDO. Likewise, in other situations where inequal beliefs were primed, people with higher SDO may experience positive well-being as there is no conflict. We acknowledge that this is our speculation, and thus, we call for future studies that can examine SDO's influence in other situations.
Our study also contributes to the literature on lifestyle. Consistent with previous studies (Goldsmith et al., 1997), we found that a significant change in lifestyle increases people's depression and has a more significant impact on individuals scoring high in SDO. Previous studies have shown that high SDO levels are opposed to support for progressive social change (see Becker, 2019, for a review). Our results indicate that the confrontation relationship between SDO and perceived change occurs at such a high level as social change, and at the individual's level of personal lifestyle change. The results suggest that people with high SDO become more vulnerable to adverse situations in an encounter with great change. Nevertheless, the current study merely examined the influence of COVID-19, and whether the findings could be expanded to other situations remains to be investigated.
We argue that our study has several practical implications. Specifically, COVID-19 continues to spread, and an increasing number of people may feel worse. Indeed, people's lives have changed dramatically. We have to embrace and learn to adapt to such a great change, which may help us reduce the outbreak's negative impact. Previous studies have examined a few helpful ways to increase well-being, such as spending money on others (Dunn et al., 2008). Our study suggests that changing our dominant belief may help us feel better.
4.2. Limitations and future directions
We acknowledge that this study has several limitations. First, although we found SDO to be positively associated with depression and argue that this is due to individuals' belief conflict, we did not directly test this argument. Future studies can examine this possibility by directly measuring their belief conflict. Second, as discussed above, we only included depression as a well-being indicator. Since well-being is a complicated construct that involves a wide array of different indicators (e.g., positive and negative affect, self-esteem, and life satisfaction), and relatively few studies have tested the effect of SDO on well-being (see Onraet et al., 2013, for a review), it would be interesting to investigate the relationships between SDO other well-being indicators in future studies. Third, it should be noted regarding the current findings that we cannot establish causality, as all the variables were measured at the same point in time. This is a desirable goal for future work, in which SDO and/or lifestyle changes are manipulated to examine their causal effect on well-being. Finally, since the current research was conducted in Chinese participants, whether the findings could be generalized in other countries remains unknown.
5. Conclusion
Despite several studies on the interpersonal effects of SDO, its intrapersonal outcome remains under-studied. Here, we examined this issue by testing the relationship between SDO and well-being during COVID-19. Our study showed that during COVID-19, people with higher SDO experienced reduced well-being (i.e., more depression), and lifestyle changes intensified this effect. These findings contribute to our understanding of SDO; that is, dominating others is not beneficial for the self. They also emphasize the importance of a stable lifestyle. Great change also hurts the self.
CRediT authorship contribution statement
J. Shi, Z. Chen, X. Wang, and T. Fei contributed to study conceptualization, Y. Yang, and H. Chen contributed to data collection, J. Shi, Z. Chen, X. Wang, and T. Fei contributed to data analysis. J. Shi and Z. Chen wrote the draft manuscript. All authors contributed to the editing and revising of the manuscript.
Footnotes
The current study was not pre-registered.
The data was opened at https://osf.io/bfqzh/.
References
- Adler N.E., Epel E.S., Castellazzo G., Ickovics J.R. Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy, White women. Health Psychology. 2000;19(6):586–592. doi: 10.1037/0278-6133.19.6.586. [DOI] [PubMed] [Google Scholar]
- Becker J.C. Ideology and the promotion of social change. Current Opinion in Behavioral Sciences. 2019;34:6–11. doi: 10.1016/j.cobeha.2019.10.005. [DOI] [Google Scholar]
- Burroughs J.E., Rindfleisch A. Materialism and well-being: A conflicting values perspective. Journal of Consumer Research. 2002;29(3):348–370. https://doi-org.eproxy.lib.hku.hk/10.1086/344429 [Google Scholar]
- Carney D.R., Jost J.T., Gosling S.D., Potter J. The secret lives of liberals and conservatives: Personality profiles, interaction styles, and the things they leave behind. Political Psychology. 2008;29(6):807–840. doi: 10.1111/j.1467-9221.2008.00668.x. [DOI] [Google Scholar]
- De Cremer D., Cornelis I., Van Hiel A. To whom does voice in groups matter? Effects of voice on affect and procedural fairness judgments as a function of social dominance orientation. Journal of Social Psychology. 2008;148(1):61–76. doi: 10.3200/SOCP.148.1.61-76. [DOI] [PubMed] [Google Scholar]
- Diener E., Lucas R.E. In: Well-being: The foundations of hedonic psychology. Kahneman D., Diener E., Schwarz N., editors. Russell Sage; New York: 1999. Personality and subjective well-being; pp. 213–229. [Google Scholar]
- Dittmar H., Bond R., Hurst M., Kasser T. The relationship between materialism and personal well-being: A meta-analysis. Journal of Personality and Social Psychology. 2014;107(5):879–924. doi: 10.1037/a0037409. [DOI] [PubMed] [Google Scholar]
- Dunn E.W., Aknin L.B., Norton M.I. Spending money on others promotes happiness. Science. 2008;319(5870):1687–1688. doi: 10.1126/science.1150952. [DOI] [PubMed] [Google Scholar]
- Goldsmith A.H., Veum J.R., Darity W., Jr. Unemployment, joblessness, psychological well-being and self-esteem: Theory and evidence. The Journal of Socio-Economics. 1997;26(2):133–158. doi: 10.1016/S1053-5357(97)90030-5. [DOI] [Google Scholar]
- Guimond S., Dambrun M., Michinov N., Duarte S. Does social dominance generate prejudice? Integrating individual and contextual determinants of intergroup cognitions. Journal of Personality and Social Psychology. 2003;84(4):697–721. doi: 10.1037/0022-3514.84.4.697. [DOI] [PubMed] [Google Scholar]
- Heaven P.C., Bucci S. Right-wing authoritarianism, social dominance orientation and personality: An analysis using the IPIP measure. European Journal of Personality. 2001;15(1):49–56. doi: 10.1002/per.389. [DOI] [Google Scholar]
- Hodson G., Costello K. Interpersonal Disgust, Ideological Orientations, and Dehumanization as Predictors of Intergroup Attitudes. Psychological Science. 2007;18(8):691–698. doi: 10.1111/j.1467-9280.2007.01962.x. [DOI] [PubMed] [Google Scholar]
- Kroenke K., Spitzer R.L., Williams J.B. The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine. 2001;16(9):606–613. doi: 10.1046/j.1525-1497.2001.016009606.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacInnis C.C., Busseri M.A., Choma B.L., Hodson G. The happy cyclist: Examining the association between generalized authoritarianism and subjective well-being. Personality and Individual Differences. 2013;55(7):789–793. doi: 10.1016/j.paid.2013.06.018. [DOI] [Google Scholar]
- Nea F.M., Pourshahidi L.K., Kearney J.M., Livingstone M.B.E., Bassul C., Corish C.A. A qualitative exploration of the shift work experience: The perceived effect on eating habits, lifestyle behaviours and psychosocial wellbeing. Journal of Public Health. 2018;40(4):e482–e492. doi: 10.1093/pubmed/fdy047. [DOI] [PubMed] [Google Scholar]
- Onraet E., Van Hiel A., Dhont K. The relationship between right-wing ideological attitudes and psychological well-being. Personality and Social Psychology Bulletin. 2013;39(4):509–522. doi: 10.1177/0146167213478199. [DOI] [PubMed] [Google Scholar]
- Pratto F., Sidanius J., Stallworth L.M., Malle B.F. Social dominance orientation: A personality variable predicting social and political attitudes. Journal of Personality and Social Psychology. 1994;67(4):741–763. doi: 10.1037/0022-3514.67.4.741. [DOI] [Google Scholar]
- Sidanius J. In: Duke studies in political psychology. Explorations in political psychology. Iyengar S., McGuire W.J., editors. Duke University Press; 1993. The psychology of group conflict and the dynamics of oppression: A social dominance perspective; pp. 183–219. [Google Scholar]
- Spitzer R.L., Kroenke K., Williams J.B.W., the Patient Health Questionnaire Primary Care Study Group Validation and utility of a self-report version of PRIME-MD: The PHQ Primary Care Study. Journal of the American Medical Association. 1999;282(18):1737–1744. doi: 10.1001/jama.282.18.1737. [DOI] [PubMed] [Google Scholar]
- Van Hiel A., Kossowska M. Having few positive emotions, or too many negative feelings? Emotions as moderating variables of authoritarianism effects on racism. Personality and Individual Differences. 2006;40(5):919–930. doi: 10.1016/j.paid.2005.09.014. [DOI] [Google Scholar]
- Whitley B.E., Jr., Lee S.E. The relationship of authoritarianism and related constructs to attitudes toward homosexuality. Journal of Applied Social Psychology. 2000;30(1):144–170. doi: 10.1111/j.1559-1816.2000.tb02309.x. [DOI] [Google Scholar]
- de Zavala A.G., Cichocka A., Eidelson R., Jayawickreme N. Collective narcissism and its social consequences. Journal of Personality and Social Psychology. 2009;97(6):1074–1096. doi: 10.1037/a0016904. [DOI] [PubMed] [Google Scholar]