

Abstract
Background:
Stone quarrying activities generate dust and fine particulate matters of silica and heavy metals. The prolonged exposure to suspended particulates leads to fatal respiratory complications. Occupational pulmonary complications are poorly characterized among quarry workers in Tamil Nadu.
Objectives:
This study aims to assess pulmonary function and determine the associated risk factors among quarry workers.
Materials and Methods:
A comparative, cross-sectional study was conducted from April 2014 to January 2015 among workers at seven stone quarries in Chennai and residents within a 5 Km radius. Pulmonary function tests (PFT) and sputum analysis were done.
Results:
Overall, 670 participants were enrolled in the study, with a median age of 37 years. Comparatively, the mean PFT measures were significantly lower in quarry workers with a higher proportion of airflow obstruction and tuberculosis infection.
Conclusion:
The risk of airflow obstruction among quarry workers increased with smoking and longer duration of work years in quarry.
KEY WORDS: India, quarry workers, radiography, spirometry, Tamil Nadu, tuberculosis
INTRODUCTION
Stone quarrying is a long-established industrial process of extracting rocks such as granite, sandstone, and limestone. Developments in the construction and infrastructure domains have led to increasing demand for building materials, resulting in a surge of quarrying activities.[1] Stone quarrying is a widely prevalent, export-oriented industry in India, Tamil Nadu,[2] with more than 1100 stone quarry units, of which nearly 985 are located in residential areas.[3] In stone quarries of Tamil Nadu, large blocks of metallic rock stones and granite are cut into stone slabs used as construction materials. The activities such as mining, crushing, and milling, stone cutting, and sandblasting carried out in quarries, generate dust and fine particulate matters (PMs) of silica and heavy metals that remain suspended in the air for long periods. Prolonged exposure to airborne PM poses serious health threats such as ocular injuries, skin diseases such as dermatoses, and lung disorders. Mainly, the particulates from stone quarries, when inhaled continuously, deposit in the lungs, eventually leading to respiratory conditions such as silicosis, tuberculosis (TB), and lung cancer.[4]
Despite being a thriving industry with a substantial presence in the country, the safety of the quarry workers and residents in the vicinity are least considered. The policies developed to prevent occupational and environmental hazards are not often followed, resulting in severe respiratory and skin ailments among the quarry workers.[5] Lung disorders such as silicosis and TB have been associated with mining and quarrying since the 1940s.[6] Following the first evidence of silicosis and TB occurrence among quarry workers in Delhi in 1949, many studies report the occupational health hazards of the quarry workers in India.[7,8,9,10] As silicosis and TB are significant occupational health hazards among quarry workers in India, and it has been suggested to undertake an occupational health survey with the relevant clinical investigations to facilitate a comprehensive policy framework on prevention, treatment, rehabilitation, compensation, and follow-up.[11] However, such studies in Tamil Nadu, are limited, and hence the quarry-related pulmonary complications are poorly characterized among quarry workers in Tamil Nadu.
On this background, this study was conducted to assess the pulmonary function and to determine the associated risk factors among quarry workers. The results were compared with the residents chosen from the population residing in 5 km radius from the group of quarry sites. Thiruneermalai and Kundrathur areas near Chennai city in Tamil Nadu are known for stone crusher quarrying works, and hence the available seven quarry sites from these regions were selected for the study.
METHODS
Study design and setting
A cross-sectional, comparative study was conducted among stone quarry workers and population residing within 5 Km radius of the selected quarry sites. The study period was from April 2014 to January 2015.
Study population
Inclusion criteria (quarry workers)
Male and female quarry employees aged above 18 years with a minimum exposure period of 1 year of quarry work and were involved in activities such as mining, crushing, milling, loading, and unloading (Residents): males and nonpregnant females aged above 18 years with a minimum residence period of 2 years in the study area.
Exclusion criteria (quarry workers)
Quarry workers not involved or employed in quarry-related specified activities for less than a year, and those who never consented for the study (Residents): males and nonpregnant females aged <18 years or those residing for <2 years in the study area and those who never consented for the study.
All eligible quarry workers available in the selected quarry sites during the field visit (7 A. M– 12 Noon IST) were enrolled after obtaining their consent [Figure 1]. Residents were selected randomly from the recruited residents of Thiruneermalai and Kundrathur areas, residing in 5 Km radius from the quarry sites.
Figure 1.

Participating study site and clinical examination
Sampling design
A convenience sampling approach was adopted for the selection of quarry workers. For all the recruited quarry workers, age (±1 year) and gender-matched residents were selected from the surrounding area using the grid sampling method, where the entire study area was divided into a small 30 × 30 meter grid cells to form a sampling frame.[12,13] Among them, the required number of grids falling on a household were selected.
Questionnaire development and data collection
A face-to-face interview was conducted by trained personnel using a structured, standardized questionnaire. Details on sociodemographic, anthropometric parameters (standing height and weight), smoking history, occupational history, and health-related information were recorded.
Lung function assessment (using spirometry)
Pulmonary functions were measured using an electronic spirometer (Model: Easy one) as per the guidelines of the American Thoracic Society/European Respiratory Society.[14] Details on the age, gender, standing height, weight, smoking status, and history of asthma of the participant were collected before spirometry test. Standard spirometric measures such as forced vital capacity (FVC), forced expiratory volume in one second (FEV1), and the ratio of FEV1/FVC were recorded. Pulmonary function variables were recorded as the percentage of the normal values predicted on reported height and age. Postbronchodilator (reversibility) testing was performed 10 min after the administration of the bronchodilator, asthalin. Based on the spirometric reading, the lung conditions were classified as normal, obstructive, and restrictive as per the global initiative for chronic obstructive lung disease classifications.[15]
Tuberculosis testing
Mass miniature radiography (MMR) was done on all the participants, to screen for TB testing. Sputum for TB was collected from those who showed MMR abnormality, and two sputum samples were collected, namely,(1) spot specimen and (2) overnight specimen were collected after their enrollment. The participants were well-instructed about the collection method before the specimen collection. Around 2–3 mL of sputum was collected in sterile, wide-mouthed, glass, leak-proof containers, and tested for TB by smear acid-fast bacilli (AFB) and M. tb culture.
Data analysis
The MMR films were read by standard X-ray reader, and spirometry curves were read independently by two medical doctors, formally trained in spirometry. The discrepancies in spirometry readings were referred to a senior doctor for the final decision. Matched paired t-test was used to compare the continuous variables such as systolic blood pressures (SBPs), diastolic blood pressure (DBP), pulse rate, and spirometry readings. Chi-square test and McNemar's test were used to compare the categorical variables. The conditional logistic regression was used to identify the associated risk factors. All statistical analyses were done using SPSS software IBM Corp. Released 2019. IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp. software Version 26.0.
Laboratory analysis
The sputum samples were processed on the same day of the collection, for AFB by fluorescent staining and M. tb culture. The samples were decontaminated using Petroff's method, stained with fluorescent auramine stain and were inoculated into Lowenstein-Jensen medium for growth of M. tb. The plates were incubated at 37°C for 8 weeks and were assessed for colony formation at every 1-week interval. The smear analysis test results were obtained after 24 h, while M. tb culture analysis results were obtained after 8 weeks. The samples measuring less than 0.5 mL in volume were not considered for testing.
RESULTS
A total of 670 participants (each of 335 quarry workers and residents) were enrolled in the study, with a median age of 37 (interquartile range: 20) years. The matched individuals from the residents were selected, such that the age and the gender matched with that of the quarry workers [Table 1]. About 23.6% of the participants were females. The distribution of the risk factors among the quarry workers and the residents is presented in Table 2. Among the quarry workers, 20.3% were underweight, whereas 12.2% were underweight among the residents. The mean body mass index among the quarry workers and residents was 21.9 and 24.0, respectively. The mean pulmonary function measures, FEV1, and FVC were significantly (P < 0.05) decreased in quarry workers compared to the residents [Table 2].
Table 1.
Characteristics and distribution of study participants
| Variables | Residents (n=335), n (%) | Quarry workers (n=335), n (%) |
|---|---|---|
| Gender | ||
| Female | 79 (23.6) | 79 (23.6) |
| Male | 256 (76.4) | 256 (76.4) |
| Age (years) | ||
| <25 | 68 (20.3) | 68 (20.3) |
| 25-34 | 69 (20.3) | 69 (20.3) |
| 35-44 | 87 (26.0) | 87 (26.0) |
| 45-54 | 58 (17.3) | 58 (17.3) |
| 55 and above | 54 (16.1) | 54 (16.1) |
| Median age (IQR) | 37 (20.0) | 37 (20.0) |
| BMI mean (range) | 24.0 (14.7-38.4) | 21.9 (12.7-38.2) |
IQR: Interquartile range, BMI: Body mass index
Table 2.
Health indicators and self-reported morbidities among two groups
| Factors | Mean (±SD) | P | |
|---|---|---|---|
|
| |||
| Residents | Quarry workers | ||
| SBP | 128.29 (±18.98) | 123.66 (±14.99) | 0.021* |
| DBP | 82.62 (±12.68) | 80.46 (±11.98) | 0.667 |
| Pulse rate | 76.23 (±11.93) | 78.96 (±12.79) | 0.048* |
| FVC | 3.22 (±0.94) | 2.90 (±0.88) | 0.002** |
| FEV1 | 2.53 (±0.78) | 2.28 (±0.71) | 0.003** |
| FEV1/FVC | 0.79 (±0.11) | 0.80 (±0.10) | 0.538 |
| BMI, n(%) | |||
| Normal | 167 (49.9) | 193 (57.6) | <0.001*** |
| Obese | 33 (9.9) | 8 (2.4) | |
| Over weight | 94 (28.1) | 66 (19.7) | |
| Under weight | 41 (12.2) | 68 (20.3) | |
| Smoking, n (%) | 88 (26.3) | 100 (29.9) | 0.304 |
| Having cough, n (%) | 24 (7.2) | 56 (16.7) | <0.001*** |
| Breathing problem, n (%) | 24 (7.2) | 49 (14.6) | <0.001*** |
| Respiratory issues, n (%) | 14 (4.2) | 69 (20.6) | <0.001*** |
| Eye irritation, n (%) | 15 (4.5) | 17 (5.1) | 0.717 |
| Skin problems, n (%) | 16 (4.8) | 5 (1.5) | 0.015* |
| Sputum positive@, n (%) | 1 (0.3) | 4 (1.2) | 0.375^ |
| Chest abnormality@, n (%) | 16 (4.8) | 59 (17.6) | <0.001***,^ |
| Airflow obstruction$, n (%) | 6 (5.3) | 16 (14.0) | <0.021*,^ |
Significant at *5% level (P<0.05), **0.5% level (P<0.005), ***Significant at 0.1% level (P<0.001), $Spirometry test (n=114, for each group), @Based on Chest X-ray, ^Used McNeamer test. SBP: Systolic blood pressure, DBP: Diastolic blood pressure, FVC: Forced vital capacity, FEV1: Forced expiratory volume in 1 s, SD: Standard deviation
The mean SBP, DBP, and the pulse rate of the quarry workers and residents were within the normal range. However, the FVC and FEV1 values obtained using spirometer were significantly lower among the quarry workers when compared to that of the residents. About 16.7% of the quarry workers were having cough, 14.6% had breathing problems, 20.6% had respiratory issues, and 17.6% presented abnormal X-ray, the proportion of which was significantly higher (P < 0.05) when compared to that of the residents [Table 2]. Based on the spirometric analysis, a higher proportion of quarry workers had obstructive or restrictive lung abnormality. The laboratory test done for those with abnormal X-ray had a higher positivity for TB (1.2%) among quarry workers than the residents (0.3%) [Figure 2]. Similarly, the proportion of those with airflow obstruction was significantly higher (P = 0.021) among the quarry workers (14.0%) when compared to the residents (5.3%).
Figure 2.
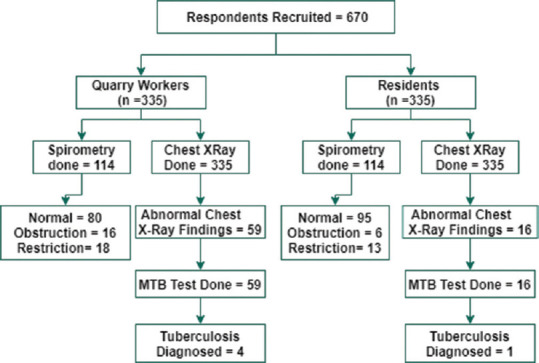
Consolidated representation of the investigations and study findings
The conditional logistic regression analyses of risk factors associated with quarry workers showed that the airflow obstruction (odds ratio [OR]: 4.33, 95% confidence interval [CI]: 1.23–15.21, P < 0.05) and chest abnormality (OR: 4.07, 95% CI: 2.27–7.31, P < 0.001) was significantly higher among quarry workers compared to the residents. Smoking significantly increased (adjusted odds ratio: 8.73, 95% CI: 1.20–63.68, P < 0.05) the risk of airflow obstruction in quarry workers [Table 3]. Figure 3 shows that the proportion exhibiting airflow obstruction increased with the duration of work years in quarry. About 50% of the workers working in quarry for more than 20 years had airflow obstruction, whereas it was 6.3% for workers with 1–5 years working experience [Figure 3].
Table 3.
Conditional logistic regression to identify the associated risk factors for quarry workers
| Matched OR (95% CI) | Adjusted matched OR (95% CI)^ | |
|---|---|---|
| Airflow obstruction$ | ||
| Residents | 1 | 1 |
| Quarry workers | 4.33 (1.23-15.21)* | 8.73 (1.20-63.68)* |
| Chest abnormality@ | ||
| Residents | 1 | |
| Quarry workers | 4.07 (2.27-7.31)*** |
*Significant at 5% level (P<0.05),***0.1% level (P<0.001), $Spirometry test (n=114, for each group), @Based on chest X-ray, ^AOR-Model is adjusted for smoking status “Smoker, nonsmoker”. CI: Confidence interval, OR: Odds ratio, AOR: Adjusted OR
Figure 3.
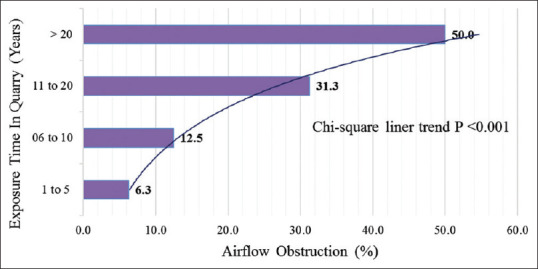
Airflow obstruction (%) and exposure years in quarry
DISCUSSION
Stone quarrying is an industrial process, in which rock stones are cut, crushed, and milled to produce manufactured sand, gravels, and slabs that are used for construction. These processes generate dust and respirable fine PMs made up of free silica, light, and heavy minerals[4] that lead to respiratory complications upon prolonged exposure. Hence, this study was conducted to assess the pulmonary function and to determine the associated risk factors among quarry workers of Chennai city. Overall, 335 quarry workers involved in operations such as crushing, loading, unloading, and laborers were enrolled in the study. Age- and gender-matched controls were selected from the residents within 5 km radius surrounding the quarry sites. Chest X-ray, pulmonary functions tests pulmonary function tests (PFT), and sputum analysis were done, and the mean PFT measures were significantly lower in quarry workers than the residents with a higher proportion of airflow obstruction and TB infection. In a study to measure the ambient air quality and occupational exposure levels in quarry units near Chennai city revealed that the concentration of total solid particles, PM10 and PM2.5 exceeded the Indian national standards. Accordingly, the pulmonary function tests (PFT) performed on the workers of the selected quarries suggested significantly lower mean PFT values as compared to those reported for normal South-Indian healthy males.[3] Figure 3 indicates that the proportion with airflow obstruction increased with the duration of work years in quarry. Studies show that long-term exposure and continued inhalation of dust and free silica are associated with lung diseases such as silicosis, mycobacterial diseases, airway obstruction, pneumoconiosis, and lung cancer.[16,17] Mining and quarry-related activities are risk factors for lung diseases such as silicosis and silica-induced TB that are often irreversible and fatal.[18,19] Several studies report the observation of both restrictive and obstructive patterns on spirometric evaluation as well as the occurrence of lung disorders among quarry workers in India. In our study, a significantly higher proportion of quarry workers self-reported to having a cough, shortness of breath and cold, and accordingly showed abnormalities in chest X-ray than the resident group. Early symptoms of lung disorders include difficulty in breathing, cough, and mucus production. Our findings suggest that quarry workers are at a higher risk of reduced pulmonary functions, which was aggravated with exposure time and smoking habits. Exposure time and smoking habits are prominent risk factors found to be associated with lung diseases.[9] The results suggest that quarry workers in Tamil Nadu are at a higher risk of developing pulmonary complications, including TB, which needs to be investigated for further details on lung complications and occupational hazards.
Studies show that the use of proper personal protective equipment (PPE) and pollution-control measure mitigate the risk of occupational hazards.[3,20,21] In many developing nations, poor utilization of PPE and nondecontamination of the work environment are found to be associated with increase the risk of health hazards. Further, inadequate awareness, under-utilization of PPE, and lack of safety protocols to control pollution in the work environments have been observed in several developing countries.[22,23,24,25,26] However, studies also indicate that periodic yet sustained educational and motivational sessions among laborers increase their compliance with PPE.[27] Hence, further research on employers' compliance of regulations, interventions carried out among the workers, level of awareness, and adherence to safety protocols will be instrumental in ensuring better facilities among quarry workers in Tamil Nadu.
CONCLUSION
Quarry workers are at an increased risk of pulmonary complications due to their prolonged exposure to dust. Our study shows a significantly lower mean PFT measures and a higher rate of chest abnormality among quarry workers compared to the residents surrounding the study area. The results suggest that the quarry workers had an increased risk of developing pulmonary disorders. However, more assessment and analysis are required for further details on lung complications due to occupational hazards and preventive measures.
Limitation
The individuals from the residents were selected randomly, whereas the quarry workers were selected by purposive sampling. Wind direction and seasonal variations were not accounted for. Information related to social economic status, hygiene, and housing-related factors of the workers and the residents were not included in the study and hence the effects of these factors on the presence of the pulmonary complications have not been reported.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The authors wish to thank the management of quarries, quarry workers, and the residents who consented to participate in the study. The authors also express their gratitude to all the technical staff involved in the field visit. Our special thanks to Dr. Soumya Swaminathan, Former Director, ICMR-National Institute for Research in Tuberculosis, Chennai; Dr. Sanjay Madhav Mehendale, Former Director, ICMR-National Institute of Epidemiology, Chennai; and Dr. Manoj Murhekar, Director, ICMR – National Institute of Epidemiology, Chennai for their continuous support toward successful completion of the study.
REFERENCES
- 1.Sharma A, Mishra AK, Choudhary BS. Sustainable exploitation of building stone in India–emerging issues. Curr Sci. 2018;115:838. [Google Scholar]
- 2.Suresh L, Maheswaran SU, Tamilarasan K, Kumar SR, Anbazhagan S. Quality assessment and grading of dimension stone in Krishnagiri district, Tamil Nadu, India. J Sci Technol. 2020;5:76–89. [Google Scholar]
- 3.Sivacoumar R, Jayabalou R, Swarnalatha S, Balakrishnan K. Particulate matter from stone crushing industry: Size distribution and health effects. J Environ Eng. 2006;132:405–14. [Google Scholar]
- 4.Ilahi I, Khan A, Ali M, Ullah U, Ali J, Khan M. Effects of stone dust exposure on some liver and kidney related serum parameters of stone crush plant workers. J Biol Life Sci. 2012;3:211–9. [Google Scholar]
- 5.Jobin P, Veparala AS, Varghese A, Jose AT, Walling KI, Sadan V. Assessment of occupational safety, hazards and related health problems among quarry workers at work places in India. Int J Nurs Educ Res. 2017;5:65–8. [Google Scholar]
- 6.Jindal SK. Silicosis in India: Past and present. Curr Opin Pulm Med. 2013;19:163–8. doi: 10.1097/MCP.0b013e32835bb19e. [DOI] [PubMed] [Google Scholar]
- 7.Rajavel S, Raghav P, Gupta MK, Muralidhar V. Silico-tuberculosis, silicosis and other respiratory morbidities among sandstone mine workers in Rajasthan – A cross-sectional study. PLoS One. 2020;15:e0230574. doi: 10.1371/journal.pone.0230574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dey D, Kumar S, Chakraborty S. Assessment of pulmonary health status among stone quarry workers at Kashipur, Silchar, Assam. Indian J Public Health Res Dev. 2017;8:382–6. [Google Scholar]
- 9.Sheikh JA, Khan ZA, Khan T, Chowdhary S. Pulmonary function among stone quarry workers in India: The effect of duration of exposure, smoking status and job profile on pulmonary function tests. J Health Soc Sci. 2018;3:137–46. [Google Scholar]
- 10.Prasad M, Wagh V. A study of pulmonary function test in stone quarry industry workers in Wardha district. J Acad Ind Res. 2019;8:52. [Google Scholar]
- 11.Sharma N, Kundu D, Dhaked S, Das A. Silicosis and silicotuberculosis in India. Bull World Health Organ. 2016;94:777–8. doi: 10.2471/BLT.15.163550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Elangovan A, Elavarsu G, Ezhil R, Prabu R, Yuvaraj J. Geospatial techniques in health survey to overcome the lack of sampling Frame. Int J Adv Remo Sen GIS. 2016;5:1908–14. [Google Scholar]
- 13.Gyapong JO, Remme JH. The use of grid sampling methodology for rapid assessment of the distribution of bancroftian filariasis. Trans R Soc Trop Med Hyg. 2001;95:681–6. doi: 10.1016/s0035-9203(01)90115-4. [DOI] [PubMed] [Google Scholar]
- 14.Graham BL, Steenbruggen I, Miller MR, Barjaktarevic IZ, Cooper BG, Hall GL, et al. Standardization of spirometry 2019 Update.An official American Thoracic Society and European Respiratory Society Technical statement. Am J Respir Crit Care Med. 2019;200:e70–88. doi: 10.1164/rccm.201908-1590ST. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med. 1999;159:179–87. doi: 10.1164/ajrccm.159.1.9712108. [DOI] [PubMed] [Google Scholar]
- 16.Leung CC, Yu IT, Chen W. Silicosis. Lancet. 2012;379:2008–18. doi: 10.1016/S0140-6736(12)60235-9. [DOI] [PubMed] [Google Scholar]
- 17.Yarahmadi A, Zahmatkesh MM, Ghaffari M, Mohammadi S, Labbafinejad Y, Seyedmehdi SM, et al. Correlation between silica exposure and risk of tuberculosis in Lorestan province of Iran. Tanaffos. 2013;12:34–40. [PMC free article] [PubMed] [Google Scholar]
- 18.Ehrlich RI. Tuberculosis, mining and silica. Occup Environ Med. 2018;75:763–4. doi: 10.1136/oemed-2018-105318. [DOI] [PubMed] [Google Scholar]
- 19.Hoy RF, Chambers DC. Silica related diseases in the modern world. Allergy. 2020;75:2805–17. doi: 10.1111/all.14202. [DOI] [PubMed] [Google Scholar]
- 20.Rav AP, Sivasankar S, Razali NK, Karmegam K, Velu P, Kulanthayan S, et al. A review of occupational safety and health problems among quarry plant workers. Malaysian J Med Health Sci. 2020;16:194–200. [Google Scholar]
- 21.Hedges K, Reed S, Mulley RC, Djukic W, Tiernan G. Exposure, health effects and control of respirable crystalline silica in Queensland quarries. J Health Safety Environ. 2010;2010:109–21. [Google Scholar]
- 22.Ahmad A. Awareness of workplace hazards and preventive measures among sandstone mineworkers in Rajasthan, India: A cross-sectional study. J Health Soc Sci. 2017;2:69–82. [Google Scholar]
- 23.Kaoje AU, Haliru L, Raji MO, Ango UM, Ango JT. Knowledge, perception and practice of safety measures related to workplace hazards among manual stone crushing workers in Sokoto, Nigeria. Int J Occup Safety Health. 2018;8:8–18. [Google Scholar]
- 24.Azuamah YC, Nwazunku A, Amadi AN, Esenwah EC, Ikoro NC, Megwas AU. Major ocular problems found among quarry workers and residents of quarrying communities in Abakaliki, Southeastern Nigeria. Int J Res. 2019;6:129–36. [Google Scholar]
- 25.Tagurum YO, Gwomson MD, Yakubu PM, Igbita JA, Chingle MP, Chirdan OO. Awareness of occupational hazards and utilization of PPE amongst welders in Jos metropolis, Nigeria. Int J Res Med Sci. 2018;6:2227–33. [Google Scholar]
- 26.Deshmukh AA, Kulkarni NP, Dhatrak SV, Nandi SS. Assessment of occupational dust and silica exposure in Indian stone mining and crushing unit – A case study. Curr World Environ. 2017;12:663. [Google Scholar]
- 27.Adams JS, Raju R, Solomon V, Samuel P, Dutta AK, Rose JS, et al. Increasing compliance with protective eyewear to reduce ocular injuries in stone-quarry workers in Tamil Nadu, India: A pragmatic, cluster randomised trial of a single education session versus an enhanced education package delivered over six months. Injury. 2013;44:118–25. doi: 10.1016/j.injury.2011.10.001. [DOI] [PubMed] [Google Scholar]