

Abstract
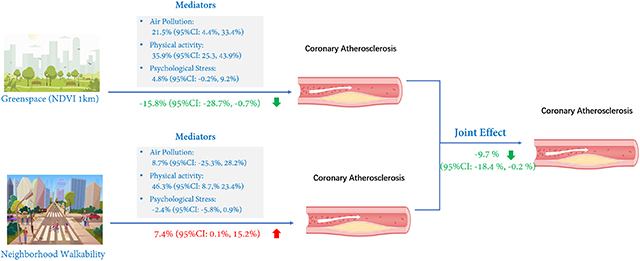
Residential green space and neighborhood walkability are important foundations of a healthy and sustainable city. Yet, their associations with atherosclerosis, the disease underlying clinical coronary heart disease (CHD), is unknown, especially in susceptible populations. We aim to explore the associations of exposure to residential green space and neighborhood walkability with coronary atherosclerosis. In this study of 2021 adults with suspected CHD, we evaluated the associations of exposure to green space (using Normalized Difference Vegetation Index [NDVI] and enhanced vegetation index [EVI] surrounding each participant’s home) and neighborhood walkability (using walkability index and number of parks near home) with atherosclerosis (using coronary artery calcium score, CAC) using linear regression model adjusted for individual-level characteristics. Mediation analysis was further applied to explore potential mechanisms through the pathways of physical activity, air pollution, and psychological stress. In the primary model, an interquartile increase in annual mean NDVI and EVI within the 1-km area was associated with −15.8% (95%CI: −28.7%, −0.7%), and −18.6% (95%Cl: −31.3%, −3.6%) lower CAC score, respectively. However, an interquartile increase in the walkability index near home was associated with a 7.4% (95% CI: 0.1%, 15.2%) higher CAC score. The combined exposure to a green space area in a 1-km area and the walkability index were inversely associated with atherosclerosis, albeit with a smaller magnitude than a single-exposure model. The findings from a mediation analysis suggested that increased physical exercise and ameliorated particulate matter < 2.5 μm (PM2.5) may partially contribute to the relationship between green space and atherosclerosis, and for walkability index, partially explained by increased PM2.5 exposure. Our study suggested a beneficial association between green space and atherosclerosis, but an adverse association between neighborhood walkability and atherosclerosis. Therefore, urban development that aims to improve neighborhood walkability should jointly account for enhancing green space properties from a public health perspective.
Keywords: green space, neighborhood walkability, physical activity, air pollution, coronary atherosclerosis
Graphical Abstract
INTRODUCTION
Cardiovascular diseases (CVD) are the leading cause of death worldwide (Collaborators, 2017). In China, more than 290 million residents were affected by CVD in 2016 (Zhao et al., 2019); over 70% of the burden of the disease is attributable to modifiable risk factors, such as environmental stressors, lifestyle behaviors, and characteristics of built environment (eg, green space). These factors may initiate or accelerate coronary atherosclerosis, which is a chronic process and the most common form of clinical CVD. People with suspected CVD may be especially susceptible to modifiable factors that influence both atherosclerosis progression and clinical CVD event rates. Thus, they are most likely to benefit from disease prevention strategies prior to its clinical manifestations by way of community-level efforts to improve the urban environment and promote healthy behaviors.
Greenness is a key determinant of a healthy urban environment and an effective mitigation strategy for air pollution (Deng et al., 2019; Ren et al., 2017). It is linked to more physical exercise, better performance behaviors, and reduced risk of disease morbidity and mortality (de Bont et al., 2020; Markevych et al., 2019; Xiao et al., 2020). A recent systematic review of 13 cohorts found a negative association between neighborhood green space and natural mortality and, thus, suggested to consider green spaces as a key public health prevention strategy (Gascon et al., 2016). Greenness is speculated to provide the beneficial effects on cardiovascular health in the following ways: mitigation of environmental pollution hazards (eg, air pollutants and noise), provision of accessible space for recreational physical exercises, increased social cohesion, and alleviation of psychophysiological stress (Yeager et al., 2020). Recent studies have observed associations of exposure to several air pollutants with initiation and progression of atherosclerosis both cross-sectionally and longitudinally (Kalsch et al., 2014; Kaufman et al., 2016; Wang et al., 2019b). Moreover, built environment factors, such as access to green space area (referred as proximity to parks) and walkable environment (referred as walkability), are composite indices that have recently been suggested as predictors for physical activity and were also linked to residential greenness levels (de Keijzer et al., 2020b; Frank et al., 2010; Jones et al., 2009). Areas with high walkability may provide benefits in mobility, physical activity, psychological pleasure, and social connection (Carr et al., 2010), and thus are closely related to the concepts of city sustainability and livability. The American Heart Association recently published a science advisory on built environment approaches to improve physical activity and cardiovascular health metrics (Omura et al., 2020). However, few studies have examined the associations of residential surrounding green space and built environment factors with subclinical CVD outcomes, such as coronary atherosclerosis, and the pathways underlying the relationships are not well understood.
Beijing, China is one of the largest metropolitan cities in the world and is currently experiencing tremendous growth in urban greenness and improvement of walkability to promote green physical activity opportunities and healthy lifestyles for local residents (Tang et al., 2018). However, due to the rapid urbanization in the past decades, Beijing is also historically plagued by high pollution issues (Hammer et al., 2020). Frequent air pollution episodes may prevent residents (especially susceptible populations, such as those with existing cardiopulmonary conditions and the elderly) from taking part in outdoor physical activity, even though their residential areas are surrounded by a high density of green space. Therefore, in developing countries with heavy air pollution, the observed impact of green space and walking behaviors on residents’ health may differ from most studies on green space, which have mostly been conducted in developed countries.
This study aims to explore the research gaps regarding the impact of urban green space and neighborhood walkability in Beijing, a metropolitan city with high air pollution levels on coronary atherosclerosis in a susceptible population with suspected coronary heart disease (CHD). We hypothesized that urban green space and variables of neighborhood walkability are associated with less coronary atherosclerosis, and that these associations are mediated through enhanced physical activity, air pollution mitigation, or reduced psychological stress.
METHODS
Study population
This study obtained the population data from the CREATION cohort in Beijing Fuwai Hospital, China. Detailed information on the study design and population was described previously (Wang et al., 2020; Wang et al., 2019b) and in section 1 of the Supplemental Information. Between 2015 and 2017, the study originally enrolled patients nationwide who were suspected to have CHD, the predominant form of atherosclerotic CVD in adults, and had cardiac computed tomography (CT). Participants were not included if they have a history of coronary events: myocardial infarction, coronary revascularization, and other CHD. In the present study, the data analysis was focused on urban residences in the Beijing metropolitan area (Figure 1) to 1) ensure availability of all the exposure variables, and 2) to reduce possible influence of selection bias due to heterogeneity in rural-urban areas during recruitment. For example, rural areas in China are usually covered by a high density of green space that may not be predictive to increased accessible space for physical activities, a potential mediator we will explore in this study. Research ethics were approved by the Chinese Academy of Medical Sciences’ Review Committee at Fuwai Hospital. We received written informed consent from each participant during the recruitment interviews. We followed standard protocols to collect cardiovascular risk factors using self-reported questionnaires, face-to-face interviews, clinical investigation, and biomarker analyses (Wang et al., 2019b).
Figure 1.
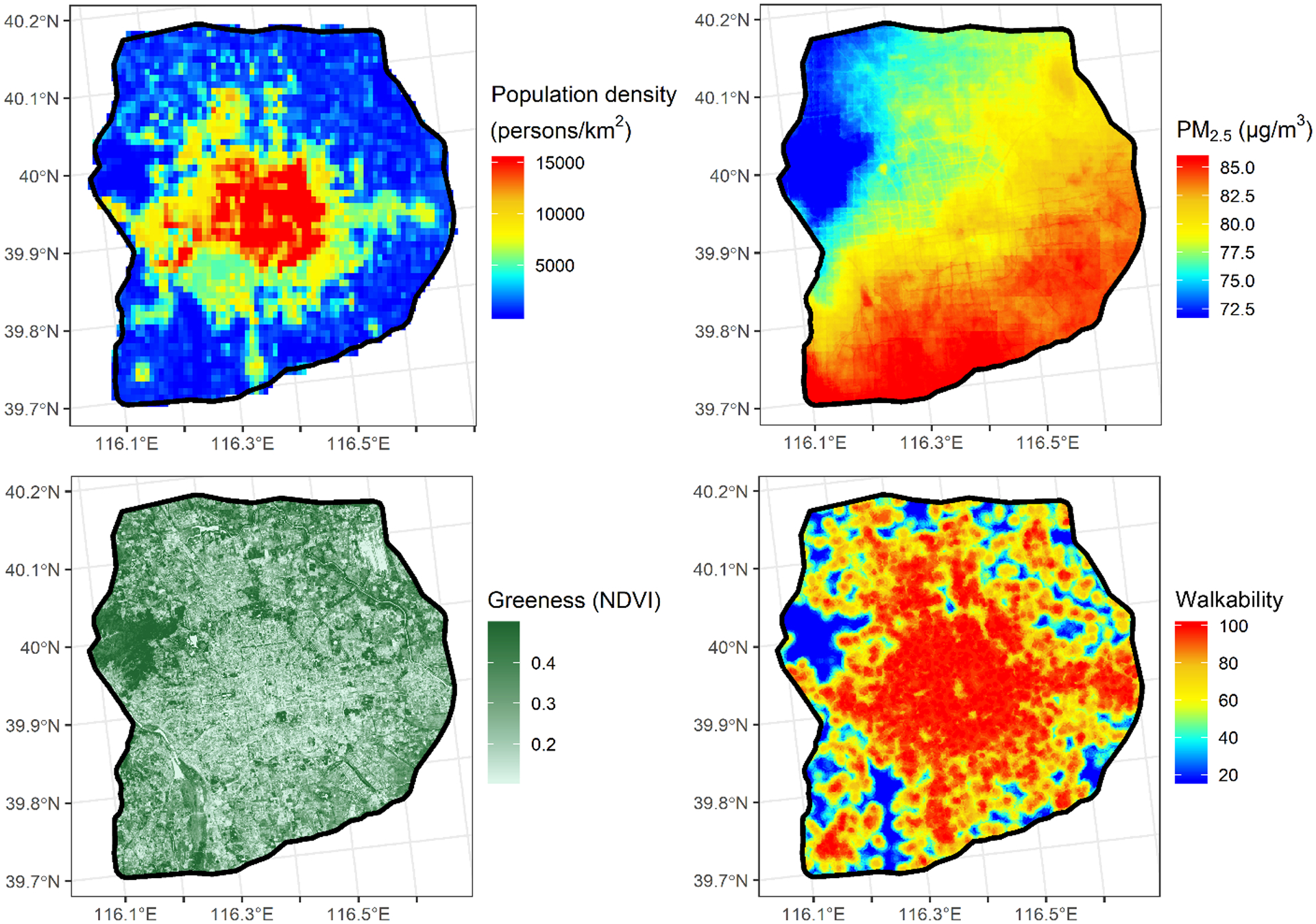
Spatial distribution of population density, PM2.5 concentrations and greenness measured with satellite-derived NDVI during the study period, and neighborhood walkability in the Beijing city area (within the 6th ring road).
Coronary artery calcium (CAC)
Standard procedures for CAC measurement are described elsewhere (Hou et al., 2012). Participants were examined with a second-generation dual-source CT system (SOMATOM Definition Flash; Siemens Healthcare, Forchheim, Germany) with a standardized scanning protocol, using 128×3mm section collimation, 75 ms rotation time, 120 kV tube voltage. A calcified lesion was determined by a threshold ≥ 130 Hounsfield units (HUs) and an area ≥ 1 mm2. Coronary artery calcification was assessed by summing up all calcified lesions using the method designed by Agatston and colleagues (Agatston et al., 1990). Specifically, we quantified the total CAC score by the summation of the area of each calcified plaque for the left main coronary artery, left anterior descending coronary artery, left circumflex coronary artery, and right coronary artery.
Exposure assessment
Residential green space indices.
Exposure to green space was assessed by outdoor green space surrounding the participants’ homes at local (250m × 250m resolution) and neighborhood (1km × 1km resolution; ie, walking distance area) scales. Each participant provided a detailed home address and was geocoded using the Baidu API platform with manual correction for errors. Residential green space was determined by two major satellite-based indicators: 1) normalized difference vegetation index (NDVI); and 2) the enhanced vegetation index (EVI). NDVI is an indicator of greenness based on land surface reflectance of visible (red) and near-infrared parts of the spectrum. NDVI varies between −0.2 and 1, with higher positive values indicating more intensity of green. EVI is considered an improvement on NDVI due to minimized oil background influences and higher responsiveness to canopy structural variations (Weier and Herring, 2011). The NDVI and EVI data used in this study was derived from the Terra Moderate Resolution Imaging Spectroradiometer (MODIS) vegetation indices product (MOD13Q1 V6) produced by NASA (https://lpdaac.usgs.gov/products/mod13q1v006/). The data has a spatial resolution of 250m and a temporal resolution of 16-day. We aggregated the data to monthly mean for further analysis from 2015 to 2017. The satellite image processing was performed on the Google Earth Engine platform. We estimate two exposure metrics: contemporaneous NDVI and EVI, to assess short-term exposure to green space; cumulative NDVI and EVI, to reflect year-long exposure to green space. Contemporaneous NDVI and EVI were their monthly average values at the time closest to the CT measurement, and cumulative exposures were calculated as the annual average values prior to the baseline CT.
Walkability.
Walkability can be assessed from the perspective of accessibility to daily facilities in proximity to each participant’s residential location (Lo, 2009). The methodology to assess walkability was developed using the Street Smart Walk Score,™ which estimates walking distances from a given location to various surrounding amenities (such as shopping malls, restaurants, schools, parks, libraries, entertainment centers) (Carr et al., 2011). Points for each type of amenity are added and then normalized to yield a score from 0 to 100 with higher values reflecting an urban setting that encourages walking. The Walk Score has been documented as a useful indicator for predicting community walkability in several cities and in various spatial scales (Carr et al., 2011; Duncan et al., 2011). However, the commercial database for Walk Score is restricted to use in US and Canadian cities. In this study, we adapted the Walk Score using a specific algorithm developed locally from a highly urbanized city (Shenzhen) in China and termed it as “walkability index” (Zhang et al., 2019). Walkability index was a modification of the weights of some key proximity facilities for Chinese cities without changes of the main algorithm from the original walk score estimate.
Apart from the calculation of walkability index, we also assessed accessibility to neighborhood parks based on the total number of urban parks surrounding the participants’ homes (at 250-m and 1-km resolution respectively). It was considered as an alternative indicator for walkability used to characterize additional potential impacts on leisure physical exercises and psychological pleasure opportunities.
Air pollution exposure.
To explore potential pathways through air pollution mitigation, we estimated air pollutant concentrations [fine particulate matter (PM2.5), nitrogen dioxide (NO2), and ozone (O3)] at residential locations using high-resolution geo-statistical modeling approach developed previously for this study. Detailed information about the model development and evaluations have been described previously (Xu et al., 2018) and are summarized in Supplemental Table 1 and 2. Annual mean air pollution concentrations over the year of the CT exam were calculated for each address (smaller than 100 m × 100 m) to match the resolution of green space. The model prediction ability varied from good to excellent for PM2.5 (R2=0.88), NO2 (R2=0.75) and O3 (R2=0.49) according to the cross-validated analysis across the monitoring stations.
Statistical analyses
We used multiple linear regression models to estimate the associations of residential green space (NDVI, EVI) and built environment (walkability index and number of parks) exposure with the CAC score. CAC was treated as dependent variable with a ln (CAC+1) transformation to account for the skewed distribution. The regression models were fit by stages and adjusted for several covariates that were selected according to established or presumed influence on the proposed associations (Wang et al., 2020; Wang et al., 2019b). The primary model included individual-level demographic and risk factor variables: age, gender, smoking status, duration and intensity, body mass index (BMI), alcohol uses, education levels, and meat consumption. We further adjusted for urbanization variable Beijing (≥2500 vs < 2500 population per 1 square km grid) to account for potential behavioral confounders that differed by geography (eg, urban vs suburban areas).
In sensitivity analyses, the main model was further extended by: 1) including self-reported hypertension SBP ≥ 140 mm Hg or DBP ≥ 90 mm Hg), diabetes mellitus, statin and CVD-related medications; 2) adding biochemical markers: high-sensitivity C-reactive protein, total cholesterol, high-density lipoprotein, low-density lipoprotein, and triglycerides in a sub-population (n=1842); 3) adding multi-pollutants (PM2.5, NO2, O3) in a model to evaluate the independent associations of the green space exposure and walkability index with ln (CAC+1); 4) excluding the patients who responded to have breathlessness or chest pain when doing moderate-vigorous exercises (n=1233); 5) using annual average EVI and NDVI values within 500m buffer size; and 6) adding individual socioeconomic status (eg, income and employment status) in subpopulation (n=450). To control for spatial clustering of the outcome, a linear mixed effects model was used with a random intercept to account for area-level postal code numbers.
Moreover, we investigated whether the observed associations were modified by previously suggested effect modifiers, such as ages (≤60 vs >60 years), gender, education, disease risk factors [BMI (≤25 vs >25), diabetes mellitus and hypertension (yes vs no)], physical activity and air pollution exposure (11,20). Physical activity was collected as continuous variable from self-reported questionnaire using “how many times of a week do you have 1 hour or more outdoor aerobic exercise regularly?” and categorized as never, <3, and ≥3 times per week for effect modification analysis. Exposure to PM2.5, NO2, and O3 were categorized as low-exposure versus high-exposure groups based on median values of concentration levels (cutpoint: PM2.5: 83.9 μg/m3; NO2: 54.2 μg/m3; O3: 101.0 μg/m3). We coded psychological stress based on whether participants reported a stressful life or concern about their health status as degree in 0 (least stressed), 1, or 2 (most stressed). Data analyses were implemented using SAS 9.4 (SAS Institute Inc., Cary, NC).
We conducted mediation analysis to examine whether physical exercises, air pollution, and psychological stress are potential underlying pathways for associations of residential green space and walkable environment on coronary atherosclerosis. We only performed the mediation analysis when the exposure variables were significantly associated with CAC score. The mediation analysis fit two models: one modeling the exposure-mediator(Mi) associations (Mi = β0 + β1Exposurei + β2Confoundersi + ε0), and the other modeling the mediator-outcome (CACi) associations (CACi = γ0 + γ1Mi + γ2Exposurei + γ3Confoundersi + ε1); where, γ2 is the direct effect from exposure noted in the exposure assessment section to CAC score while controlling for the mediator Mit, noted as air pollution exposure and physical activity. The indirect effect describes the pathway from exposure to CAC score through the mediator Mi. The proportion mediated is calculated as: . We assessed 95% confidence interval by 1000 bootstrap simulations. We used built-in function in R package to perform the mediation analysis (Imai et al., 2010).
A healthy and sustainable city aims to promote both a greener and more walkable environment. Thus, to investigate the joint effects of both green space and walkability on atherosclerosis, we established a linear combination statistical model using the cumulative risk index (CRI) method based on estimates from the primary models that included green space and walkability index simultaneously (Wang et al., 2019a), as secondary analysis. The CRI refers to where is the estimates of effects for green space and walkability index xp from the primary models. The CRI confidence interval (95%CI) is estimated by . In addition, we used categories of differently exposed groups of the population by dichotomizing the exposure variables according to their median exposure levels, and then examined the additive interaction between green space and walkability index by calculating the relative excess risk due to interaction (RERI) (Zou, 2008). The 95% CI of RERI contains 0 if no interaction is detected.
RESULTS
Population characteristics
Table 1 summarizes the population statistics with respect to the demographics, lifestyle, and socioeconomic status, and outcome information stratified by NDVI quartiles. Of the 2021 participants with CT measurement who resided in Beijing in the past 5 years, 2000 were successfully geocoded with valid outdoor residential exposure estimates for the year of their baseline exam. The participants were on average 57±12 years’ old; 59% were male. Over 33% were current smokers, 72% had lower than college education, 85% did regular outdoor exercises (self-reported) at least once per week for over 1 hour. Moreover, 48% of the participants had hypertension, 18% had diabetes mellitus, and nearly 75% had medication history. The mean CAC score is 92.6±325.9 Agatston units with a declining trend seen over incrementally better NDVI quartiles. Participants living in an area with higher levels of NDVI were more likely to be younger, male, current smokers, better educated, have slightly higher BMI, drink more alcohols, exercise more, and have less statin uses and less psychological stress than those who lived in an area with lower levels of NDVI.
Table 1.
Characteristics of the participants and exposure metrics by quantiles of NDVI1000-1year
| Total | Greenness Quartile 1 |
Greenness Quartile 2 |
Greenness Quartile 3 |
Greenness Quartile 4 |
P value | |
|---|---|---|---|---|---|---|
| Population size | 2000 | 500 | 500 | 500 | 500 | |
| CAC (Agtation unit) | 92.6 (325.9) | 120.2 (391.8) | 102.7 (359.6) | 70.3 (253.2) | 77.3 (277.5) | <0.001 |
| Demographics | ||||||
| Age (year) | 57.3 (11.5) | 60.6 (10.1) | 58.1 (11.5) | 54.2 (10.9) | 56.0 (12.3) | <0.001 |
| Male (%) | 58.7 | 50.4 | 51.2 | 72.6 | 60.6 | <0.001 |
| Education (%) | <0.001 | |||||
| Lower than college | 71.6 | 84.2 | 79.0 | 51.8 | 71.7 | |
| College | 25.0 | 13.6 | 15.4 | 45.4 | 25.5 | |
| Higher than college | 3.4 | 2.2 | 5.6 | 2.8 | 2.8 | |
| Risk factors | ||||||
| BMI | 25.7 (3.3) | 25 (3) | 25.5 (3.4) | 26.4 (3.3) | 25.7 (3.3) | <0.001 |
| Smoking Status (%) | <0.001 | |||||
| Never & former smokers | 67.1 | 75.4 | 74.4 | 54.2 | 64.2 | |
| Current smokers | 33.0 | 24.6 | 25.6 | 45.8 | 35.8 | |
| Cigarettes per day (in smokers) | <0.001 | |||||
| ≤ 10 | 17.0 | 13.8 | 21.1 | 10.9 | 24.0 | |
| 10–20 | 61.6 | 57.7 | 56.3 | 71.2 | 55.9 | |
| ≥ 20 | 21.4 | 28.5 | 22.7 | 17.9 | 20.1 | |
| Smoking years (in smokers) | 28.1 (10.6) | 31.6 (11.3) | 29.7 (11.8) | 26.0 (8.9) | 27.3 (10.4) | <0.001 |
| Alcohol uses (%) | 24.8 | 20.7 | 18.2 | 36.3 | 23.8 | <0.001 |
| Physical activity (%) | <0.001 | |||||
| Never | 15.4 | 15.5 | 14.8 | 15.5 | 15.8 | |
| ≤3 times per week | 49.3 | 59.9 | 56.4 | 39.2 | 42.3 | |
| >3 times per week | 35.3 | 24.6 | 28.8 | 45.4 | 41.9 | |
| Hypertension (%) | 48.4 | 48.8 | 48.8 | 48.4 | 47.6 | 0.97 |
| Diabetes mellitus (%) | 18.7 | 15.6 | 16.6 | 22.6 | 20.0 | 0.02 |
| Medication (%) | ||||||
| Antihypertensive | 45.4 | 46.6 | 48.0 | 42.8 | 44.0 | 0.33 |
| Statin | 29.4 | 34.0 | 30.6 | 22.6 | 30.4 | <0.001 |
| Psychological stress (%) | <0.001 | |||||
| Low | 54.5 | 41.0 | 40.9 | 67.4 | 52.8 | |
| Moderate | 16.6 | 23.5 | 19.0 | 13.0 | 16.5 | |
| High | 28.9 | 35.5 | 40.1 | 19.6 | 30.7 | |
Exposure to green space and walkable environment
Figure 1 shows the spatial distribution of selected exposure variables for green space (NDVI), air pollution (PM2.5), and walkability index, as well as for population density. Supplemental Table 3 summarizes statistical distribution of the residential green space and walkability variables as well as air pollution exposure at homes. For instance, the mean annual levels for NDVI1000m, EVI1000m are 0.22 and 0.12, respectively. Mean walkability index was 89.1, and mean total parks within a 1-km residential buffer was 9, indicting high accessibility to all facilities and leisure. The levels of NDVI and EVI were highly correlated with each other (Pearson R > 0.8) but weakly and negatively correlated with the walkability index (Pearson correlation −0.11 – −0.01) (Supplemental Table 4). Moreover, air pollutants (PM2.5, NO2) showed low-moderately negative correlations with the levels of green space variables, and positive correlations with walkability index and park numbers within both 250m and 1km buffers.
Main analysis
The results of the age- and sex-adjusted models and the primary models are presented in Table 2. In the base models, residential surrounding green space (ie, NDVI, EVI) and walkability index were associated with degree of CAC score. In the primary model, an interquartile increase in annual mean NDVI and EVI in the 250-m buffer was associated with −17.1% (95%CI: −29.7%, −2.2%), and −16.4% (95%CI: −28.7%, −2.0%) lower degree of CAC score, respectively. The magnitude of the associations was consistent regardless of the choice of buffer size (eg, 250 m and 1 km) or the exposure duration (ie, contemporaneous versus cumulative for NDVI and EVI) (Supplemental Table 6 and 7). On the contrary, higher walkability index near residential address was associated with 7.4% (95%CI: 0.1%, 15.2%) higher degree of CAC score. No associations were found between the number of parks around the home and CAC, although the directions were consistently positive, eg, 1.0% (−4.7%, 6.9%) and 4.6% (−2.9%, 12.8%) in the 250-m and 1-km buffers, respectively.
Table 2.
Associations between (interquartile increase) annual average greenness (in 250m and 1000m), built environment variables and coronary artery calcium score with incremental adjustment for risk factors.
| Exposure (interquartile increase) | Base Model | Fully-adjusted Model |
|---|---|---|
| NDVI250m (0.17) | −17.4 (−29.9, −2.6) | −17.1 (−29.7, −2.2) |
| NDVI1000m (0.17) | −16.3 (−29.0, −1.3) | −15.8 (−28.7, −0.7) |
| EVI250m (0.10) | −16.8 (−29.0, −2.6) | −16.4 (−28.7, −2.0) |
| EVI1000m (0.10) | −19.1 (−31.6, −4.4) | −18.6 (−31.3, −3.6) |
| Walkability index (10) | 7.3 (0.6, 14.4) | 7.4 (0.1, 15.2) |
| Npark_250m (1) | 1.3 (−4.4, 7.2) | 1.0 (−4.7, 6.9) |
| Npark_1000m (7) | 5.0 (−2.6, 13.1) | 4.6 (−2.9, 12.8) |
Base model adjusted for age, gender.
Fully adjusted model adjusted for age, sex, body mass index, smoking (status, duration and intensity), alcohol consumption, education, meat consumption and urbanization.
The combined exposure to higher green space area in 1-km buffer and higher walkability index were associated with lower CAC scores (Supplemental Table 8) using the CRI model. There were small negative interactions (ie, RERI<0) on the additive scale, which indicated a smaller magnitude of the combined effects than effects of the single exposure variables.
Sensitivity analysis
The associations in models were generally robust when we additionally adjusted for medications, blood biomarkers, socioeconomic status, and neighborhood-level zip-code variables, or excluded the participants who may have symptoms with mild exercises, or use of annual average green space variables (ie, EVI and NDVI) within a 500 m buffer of the residential areas (Supplemental Table 6, 7, 9). Similarly, the effect estimates in multiple-exposure models including all the air pollutant variables were not meaningfully different from the results of single-exposure model.
Effect modifications
We found potential effect modification in the relationship between annual mean NDVI and CAC score by physical activity (Pinteraction<0.001) (Table 3). Stronger association between green space (ie, NDVI1000m-1year) and CAC score were seen in participants who exercised more than 3 times per week outdoors than those who did not exercise at all or exercised less. For the walkability index, we observed stronger associations with CAC score among male adults. There was no evidence of effect modification for green spaces and walkability index by other personal characteristics or environmental exposure.
Table 3.
Effect modification analysis for associations between (interquartile range increase) greenness variables (in 1000m) and coronary artery calcium score stratified by potential modifiers.
| NDVI1000m-1year | P-value | Walkability index | P-value | |
|---|---|---|---|---|
| Gender | 0.69 | 0.001 | ||
| Female | −12.8 (−31.6, 11.1) | −4.1 (−12.9, 5.7) | ||
| Male | −18.3 (−34.6, 2) | 19.3 (8.6, 31.1) | ||
| Age | 0.96 | 0.86 | ||
| ≤60 | −20.9 (−36.2, −2) | 9.2 (−0.5, 19.9) | ||
| >60 | −20.2 (−38.6, 3.6) | 7.9 (−2.3, 19.3) | ||
| BMI | 0.46 | 0.85 | ||
| ≤25 | −10.7 (−29.2, 12.7) | 8.5 (−3.6, 22) | ||
| >25 | −20.8 (−36.9, −0.7) | 7.1 (−1.3, 16.2) | ||
| Education | 0.27 | 0.66 | ||
| Lower than college | −11.1 (−26.1, 6.9) | 8.3 (0.7, 16.5) | ||
| College | −35.7 (−56.0, −6.0) | −4.1 (−28.0, 27.7) | ||
| Higher than college | 0.7 (−61.5, 163.6) | −4.6 (−45.9, 68.2) | ||
| Hypertension | 0.71 | 0.42 | ||
| No | −13.4 (−30.7, 8.3) | 4.5 (−5, 15.1) | ||
| Yes | −18.5 (−35.6, 3.1) | 10.1 (0.3, 20.9) | ||
| Diabetes | 0.62 | 0.24 | ||
| No | −14.3 (−28.5, 2.8) | 9.3 (1.2, 17.9) | ||
| Yes | −22.9 (−47.4, 13.1) | −0.6 (−14.3, 15.3) | ||
| Physical exercise | <0.001 | 0.57 | ||
| Never | 12.6 (−10, 40.9) | −0.3 (−17.4, 20.5) | ||
| ≤3 times per week | −16.4 (−34, 5.9) | 10.3 (0.7, 20.8) | ||
| >3 times per week | −45 (−60.8, −22.6) | 5.3 (−5.8, 17.9) | ||
| PM2.5 | 0.36 | 0.24 | ||
| ≤ median | −16.8 (−29.7, −1.7) | 6.5 (−0.8, 14.4) | ||
| > median | −11.8 (−27.3, 7.2) | 7.3 (0.0, 15.1) | ||
| NO2 | 0.94 | 0.45 | ||
| ≤ median | −16.1 (−30.3, 1.0) | 8.3 (0.6, 16.5) | ||
| > median | −15.7 (−28.9, −0.1) | 7.8 (0.4, 15.7) | ||
| O3 | 0.55 | 0.89 | ||
| ≤ median | −18.3 (−32.5, −1.0) | 7.3 (0, 15.2) | ||
| > median | −15.1 (−28.2, 0.5) | 7.4 (0.1, 15.2) |
Model adjusted for age, sex, body mass index, smoking (status, duration, and intensity), alcohol consumption, education, meat consumption and urbanization.
Mediation analysis
We found that the associations between green space and atherosclerosis were partially mediated through more physical activity and lower exposure to PM2.5, but not explained by psychological stress (Table 4). Specifically, the increased outdoor physical activity explained the largest proportion [35.9% (95%CI: 25.3%, 43.9%)] of the association between annual mean green space (ie, NDVI level in 1km buffer) and the degree of CAC score, followed by reduced PM2.5 exposure with a proportion of mediation by 23.4% (95%CI: 35.0%, 6.8%) of this association. In contrast, self-reported psychological stress explained only 3.7% to 4.8% of the associations. For the association between the walkability index and CAC score, 46.3% (95%CI: 23.4%, 58.7%) could be explained by increased PM2.5 concentration.
Table 4.
Estimated proportion of association between greenness and coronary artery calcium score mediated by air pollutants and physical activity.
| Proportion (%) mediated by physical activity (95%CI) | Proportion (%) mediated by annual mean PM2.5 (95%CI) | Proportion (%) mediated by psychological stress (95%CI) | |
|---|---|---|---|
| NDVI250m-1year | 26.3 (14.2, 35.3) | 19.9 (4.2, 31.1) | 3.7 (−0.2, 7.3) |
| NDVI1000m-1year | 35.9 (25.3, 43.9) | 21.5 (4.4, 33.4) | 4.8 (−0.2, 9.2) |
| EVI250m-1year | 21.1 (7.5, 31.2) | 23.4 (6.8, 35.0) | 4.5 (−0.2, 8.8) |
| EVI1000m-1year | 29.4 (18.9, 37.5) | 21.0 (5.5, 32.2) | 4.2 (−0.3, 8.2) |
| Walkability index | 8.7 (−25.3, 28.2) | 46.3 (8.7, 23.4) | −2.4 (−5.8, 0.9) |
Model adjusted for age, sex, body mass index, smoking (status, duration and intensity), alcohol consumption, education, meat consumption and urbanization.
DISCUSSION
The findings of our cross-sectional study supported our hypothesis that living in urban areas surrounded by more green space was associated with less coronary atherosclerosis, as measured by coronary arterial calcification score from cardiac CT scanning, in subjects with suspected CHD after adjustment for various confounder variables including air pollution exposure. The associations were robust when focusing on the surrounding residential area (250-m radius) versus walkable area in a larger buffer (1-km radius), and regardless of the choice of exposure durations (contemporaneous vs cumulative). The beneficial association between exposure to green space and atherosclerosis appeared to be greater among the participants who had more outdoor physical exercise. Unexpectedly, we observed that a higher walkability index in residential areas was associated with greater atherosclerosis (higher CAC score), although the finding suggested that the additive effect of both green space and walkability index was still dominated by the beneficial inverse association for green space and atherosclerosis. Furthermore, our study results suggested that a major proportion of the association between green space and atherosclerosis was partially explained through pathways of physical exercise, followed by the air pollution reduction, but was not explained by self-reported psychological stress. For the walkability index, the association was mainly explained through the impact of air pollution exposure. Because atherosclerosis is the major cause of CHD, the progression of which may be lifelong (Gidding and Allen, 2019), our findings provide important nuance regarding the prevention strategies to reduce possible CHD risks, especially for susceptible populations with suspected CHD. Mitigation of air pollution and enhanced green space availability could be key determinants of effective primary CVD prevention strategies targeting healthy lifestyles in large industrialized urban settings.
To our knowledge, no study has investigated the relationships between greenness and atherosclerosis. However, accumulating evidence has supported the protective associations between green space and natural and CVD mortality in many countries, including studies conducted in China (de Keijzer et al., 2020a; Rojas-Rueda et al., 2019). For instance, Ji and colleagues (Ji et al., 2019) reported that residences surrounded by the highest quartile of greenness (NDVI within a 250m buffer) were associated with 27% lower risk of mortality than those in the lowest quartile in 23,754 Chinese older adults with a mean age of 93 years across the country. Another study conducted in an urban area in China found a 77% lower CHD prevalence in people who lived in higher NDVI neighborhoods (Jia et al., 2018). Furthermore, there are many studies that have explored the associations of green space variables with CVD risk factors, including blood pressure and hypertension, incidence or prevalence of diabetes mellites, blood lipids, and metabolic syndrome of a set of cardiometabolic disorders (de Keijzer et al., 2020a; Fong et al., 2018; Yang et al., 2020). Most of the existing findings, albeit inconsistent, generally support the hypothesis that higher coverage of green space is associated with lower levels of CVD risk factors. However, few studies have focused on the association in a susceptible population, defined as high-risk adults due to existing evidence of subclinical CHD, who may gain more primary prevention benefits from green space exposure. In comparison, a recent study in Great Britain assessed the association of green space with longitudinal changes in subclinical markers of arterial stiffness, which seems more relevant to our study (de Keijzer et al., 2020b). However, no associations were found in that study regardless of the green space variables that were used. Collectively, although our study supported the inverse association between green space exposure and coronary atherosclerosis, existing published studies on the same topic are limited and thus, worthy of further investigation.
Our findings support some proposed hypotheses on the underlying mechanisms of the beneficial association of green space with cardiovascular health by motivating people toward physical activity and/or ameliorating air pollution exposure. Physical exercise may protect patients from atherosclerosis and CHD via multiple potential pathways, including attenuated plaque progression and outward remodeling, stabilization of vulnerable plaques, and improved endothelial function (Bowles and Laughlin, 2011). However, some studies have suggested that only one third of the beneficial effects of physical activity on CVD were attributed to favorable changes in CVD risk factors, such as lipid and cholesterol levels and hypertension (Mora et al., 2007). Therefore, most of the exercise-induced improvements may be directly attributed to the beneficial effects on vascular structure and function, independent of the impact of exercise on traditional CV risk factors (Thijssen et al., 2010). This speculation is supported by the result of our study in which the proportions of the association mediated through physical exercise was substantially higher than those observed in other studies conducted in northern China that focused on cardiovascular risk factors (Yang et al., 2020). Hence, the benefits of physical exercise derived by proximity to neighborhood green spaces may be more related to the treatment of atherosclerosis than the traditional risk factors giving rise to the onset of atherosclerosis.
Previous studies, mainly from the United States and Canada, have increasingly examined the relationships between walkability index and health outcomes, but findings remain largely inconclusive. Compared to our result which implied an adverse association between a more walkable neighborhood on higher CAC score, there were other studies that suggest highly walkable communities are associated with better cardiometabolic health (Howell et al., 2019; Jia et al., 2018; Meline et al., 2017).The discrepancy among findings might be attributed to two factors. First, highly walkable neighborhoods are commonly associated with high residential density and street connectivity (Figure 1), which may also be affected by increased air pollution levels, seen as the positive correlation between walkability index and air pollution exposure in our study (Supplemental Table 5). Compared to the latter studies with opposite findings, our study focused on susceptible populations (participants with suspected CHD) who were more vulnerable to poor air quality and inclined to exercise less than the healthy population used in the latter studies. We did not observe an association between walkability index and physical activity, suggesting that the walkability index may not directly show patients’ perceptions of their community environment and the actual physical exercise levels in metropolitan cities. Indeed, our walkability index ignores other features (ie, aesthetics, sidewalks, crime, perceived safety, etc) relevant to physical activity based on the premise that facilities proximity makes a place walkable. Second, the Walk Score™ (www.walkscore.com), which has been widely used in many studies, primarily represents the walkability lifestyle in the United States and Canada rather than those in China. For example, a large commercial center that integrates a variety of facilities such as restaurants, supermarkets, movie theatres, is an important motivator for neighborhood walkability in China but was not included in the Walk Score™ calculation; in contrast, individual groceries and shops are more popularly seen in US and Canadian cities. Our study adapted the Walk Score™ algorithm by assigning high weights to large commercial complex destinations to reflect the unique perception of walkable environments in Chinese cities. The modified version on the score calculation may increase the correlation of the walk score with road networks, which further contributed to the higher probability of exposure to traffic air pollutants than the use of the traditional walk score for exposure assessment. Indeed, we identified that over 46.3% of the relationship between walkability index and CAC score was explained through increased air pollution exposure rather than physical activity and psychological stress. To our knowledge, this is the first study that explored underlying pathways for walkability assessment and cardiovascular health. Future studies are needed to assess the validity of the walkability index locally in Chinese cities.
Improving neighborhood green space and walkability is equally essential for maintaining sustainable and livable cities in China, even though our study showed that their independent association with subclinical CHD may be contradictory. In this study, the combined effect of both exposure factors appeared to be beneficial to atherosclerosis, despite the attenuated magnitude after additivity. Although the competing effect between augmented air pollution exposure and enhanced physical exercise on cardiovascular disease is unclear, recent emerging studies increasingly support the cardioprotective effect exerted through physical activity when the adverse effects of exposure to air pollution have been jointly assessed (Andersen et al., 2015; Guo et al., 2020; Kim et al., 2020). Therefore, sustainable Chinese cities that aim to improve neighborhood walkability should jointly account for enhancing green space properties from a public health perspective. This conclusion is consistent with the recently published science advisory by the American Heart Association that calls for greater emphasis on improving the built environment as an effort to enhance cardiovascular health globally (Omura et al., 2020).
The major strength of our study is that it is the first rigorous assessment of the independent and joint associations of both residential green space and walkability with a measure of subclinical atherosclerosis, giving insight into potential underlying mechanistic pathways in a large susceptible population. However, this study has several limitations. First, our study focused on susceptible populations, and, thus, the results were mostly relevant to at-risk populations regarding the effects of exposure on CHD. Nevertheless, the burden of heart disease in China is growing rapidly, leading to an incidence of approximately 3 million CHD diagnoses and 1.7 million deaths in 2016 (Zhao et al., 2019). Hence, there is still a great potential for disease prevention intervention in this population by improving neighborhood green space. Second, our results may be skewed by selection bias of the population due to refusal of eligible participants. However, this impact may be minimal, as the estimated refusal rate was relatively small (<15%, see Supplemental Information, section 1). Third, although air pollution exposure seems an important mediator in the association between green space and CAC, it is noted that these predictions also contained green space information (e.g. NDVI and green land cover such as crop, forest and grass) as predictor variables from the air pollution models. This issue appears common in recent studies given that geostatistical model (that include green space as predictor variables) remains the major method for predicting air pollution exposure in epidemiological studies. Therefore, future studies are recommended to use deterministic model (e.g. chemical transport model or dispersion model) for air pollution exposure to avoid duplicated use of green space in the mediation analysis. Fourth, the cross-sectional study design restricted our ability for causal inferences, especially when interpreting the mediation analysis results, based on our findings that deserve further evaluation in a longitudinal analysis with additional future information in this cohort. Fifth, the questionnaire related to physical activity is not comprehensive enough to represent the outdoor physical activity, and thus may misclassify the associations in the mediation analyses. Use of a more comprehensive assessment scored as physical activity metabolic equivalents (METs) may be an optimal approach in this analysis. Moreover, our study did not account for physical activity performed beyond the residential area, nor that was associated to transportation, such as biking and walking on daily trips, which may lead to exposure misclassification. Similarly, we did not find any role played through psychological stress for the observed association of green space and walkability with atherosclerosis, probably due to the use of crucial assessment with dichotomized questionnaire information. Sixth, accessibility to parks near residential area (eg, Npark_250m and Npark_1000m) may not well reflect residents’ willingness to exercise in China, as compared to more favorable locations such as community or city park squares. Moreover, some park features such as aesthetics and area sizes may be more conductive to exercise than the number of parks near residential areas. However, obtaining these data are difficult in this study. Lastly, we acknowledge some neighborhood-level socio-economic status confounders, such as the inclusion of manual workers (%) and illiterate participants (%), which were not spatially resolved over the study area and may potentially affect our results.
CONCLUSION
In this study of participants with suspected CHD, we found that increased exposure to green space is associated with smaller degree of CAC (less atherosclerosis), independent of traditional atherosclerotic risk factors, indicating potential benefit of environmental green space for prevention of atherosclerosis. Moreover, neighborhood walkability was adversely associated with higher CAC scores in a single-exposure model. However, the integrated analysis that assessed the exposure to a combination of the residential green space and neighborhood walkability still suggested a beneficial association between the joint-exposure and coronary atherosclerosis. Mediation analysis indicated that the relationship between green space and coronary atherosclerosis was mainly attributed through the increment of physical activity, followed by air pollution reduction; whereas the association between walkability index and atherosclerosis was mediated by the increase in air pollution levels. As China undergoes rapid urbanization for better neighborhood walkability, our findings provide important implication to urban planners and health policy makers aimed at increasing greenness in urbanized cities as part of a comprehensive strategy to promote physical activity and enhance cardiovascular health for urban populations.
Supplementary Material
HIGHLIGHTS:
Exposure to green space was inversely associated with coronary artery calcium
Neighborhood walkability was positively associated with coronary artery calcium
Physical activity and fine particulate matter partially mediated the green space-atherosclerosis association
Increased air pollution partially mediated the walkability-atherosclerosis association
ACKNOWLEDGEMENT
The authors thank Elizabeth Marshall Metcalfe at University at Buffalo for proofreading the manuscript. This study was supported by the Ministry of Science and Technology of China (Grant No. 2016YFC1300400) and Chinese national key research and development project (2016-CXGC05-1) and the National Institutes of Health (ES031986). The authors have no conflicts of interest. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Footnotes
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
REFERENCES
- Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr., Detrano R, 1990. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 15, 827–832. [DOI] [PubMed] [Google Scholar]
- Andersen ZJ, de Nazelle A, Mendez MA, Garcia-Aymerich J, Hertel O, Tjonneland A, Overvad K, Raaschou-Nielsen O, Nieuwenhuijsen MJ, 2015. A study of the combined effects of physical activity and air pollution on mortality in elderly urban residents: the Danish Diet, Cancer, and Health Cohort. Environ Health Perspect 123, 557–563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bowles DK, Laughlin MH, 2011. Mechanism of beneficial effects of physical activity on atherosclerosis and coronary heart disease. J Appl Physiol (1985) 111, 308–310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carr LJ, Dunsiger SI, Marcus BH, 2010. Walk score as a global estimate of neighborhood walkability. Am J Prev Med 39, 460–463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carr LJ, Dunsiger SI, Marcus BH, 2011. Validation of Walk Score for estimating access to walkable amenities. Br J Sports Med 45, 1144–1148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collaborators GBDRF, 2017. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 390, 1345–1422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Bont J, Hughes R, Tilling K, Diaz Y, de Castro M, Cirach M, Fossati S, Nieuwenhuijsen M, Duarte-Salles T, Vrijheid M, 2020. Early life exposure to air pollution, green spaces and built environment, and body mass index growth trajectories during the first 5 years of life: A large longitudinal study. Environ Pollut 266, 115266. [DOI] [PubMed] [Google Scholar]
- de Keijzer C, Bauwelinck M, Dadvand P, 2020a. Long-Term Exposure to Residential Greenspace and Healthy Ageing: a Systematic Review. Curr Environ Health Rep 7, 65–88. [DOI] [PubMed] [Google Scholar]
- de Keijzer C, Foraster M, Basagana X, Tonne C, Garcia LA, Valentin A, Kivimaki M, Nieuwenhuijsen MJ, Alonso J, Anto JM, Singh-Manoux A, Sunyer J, Dadvand P, 2020b. Long-Term Greenspace Exposure and Progression of Arterial Stiffness: The Whitehall II Cohort Study. Environ Health Perspect 128, 67014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deng S, Ma J, Zhang L, Jia Z, Ma L, 2019. Microclimate simulation and model optimization of the effect of roadway green space on atmospheric particulate matter. Environ Pollut 246, 932–944. [DOI] [PubMed] [Google Scholar]
- Duncan DT, Aldstadt J, Whalen J, Melly SJ, Gortmaker SL, 2011. Validation of walk score for estimating neighborhood walkability: an analysis of four US metropolitan areas. Int J Environ Res Public Health 8, 4160–4179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fong KC, Hart JE, James P, 2018. A Review of Epidemiologic Studies on Greenness and Health: Updated Literature Through 2017. Curr Environ Health Rep 5, 77–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frank LD, Sallis JF, Saelens BE, Leary L, Cain K, Conway TL, Hess PM, 2010. The development of a walkability index: application to the Neighborhood Quality of Life Study. Br J Sports Med 44, 924–933. [DOI] [PubMed] [Google Scholar]
- Gascon M, Triguero-Mas M, Martinez D, Dadvand P, Rojas-Rueda D, Plasencia A, Nieuwenhuijsen MJ, 2016. Residential green spaces and mortality: A systematic review. Environ Int 86, 60–67. [DOI] [PubMed] [Google Scholar]
- Gidding SS, Allen NB, 2019. Cholesterol and Atherosclerotic Cardiovascular Disease: A Lifelong Problem. J Am Heart Assoc 8, e012924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guo C, Zeng Y, Chang LY, Yu Z, Bo Y, Lin C, Lau AK, Tam T, Lao XQ, 2020. Independent and Opposing Associations of Habitual Exercise and Chronic PM2.5 Exposures on Hypertension Incidence. Circulation 142, 645–656. [DOI] [PubMed] [Google Scholar]
- Hammer MS, van Donkelaar A, Li C, Lyapustin A, Sayer AM, Hsu NC, Levy RC, Garay MJ, Kalashnikova OV, Kahn RA, Brauer M, Apte JS, Henze DK, Zhang L, Zhang Q, Ford B, Pierce JR, Martin RV, 2020. Global Estimates and Long-Term Trends of Fine Particulate Matter Concentrations (1998–2018). Environ Sci Technol 54, 7879–7890. [DOI] [PubMed] [Google Scholar]
- Hou ZH, Lu B, Gao Y, Jiang SL, Wang Y, Li W, Budoff MJ, 2012. Prognostic value of coronary CT angiography and calcium score for major adverse cardiac events in outpatients. JACC Cardiovasc Imaging 5, 990–999. [DOI] [PubMed] [Google Scholar]
- Howell NA, Tu JV, Moineddin R, Chu A, Booth GL, 2019. Association Between Neighborhood Walkability and Predicted 10-Year Cardiovascular Disease Risk: The CANHEART (Cardiovascular Health in Ambulatory Care Research Team) Cohort. J Am Heart Assoc 8, e013146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Imai K, Keele L, Tingley D, 2010. A general approach to causal mediation analysis. Psychol Methods 15, 309–334. [DOI] [PubMed] [Google Scholar]
- Ji JS, Zhu A, Bai C, Wu CD, Yan L, Tang S, Zeng Y, James P, 2019. Residential greenness and mortality in oldest-old women and men in China: a longitudinal cohort study. Lancet Planet Health 3, e17–e25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jia X, Yu Y, Xia W, Masri S, Sami M, Hu Z, Yu Z, Wu J, 2018. Cardiovascular diseases in middle aged and older adults in China: the joint effects and mediation of different types of physical exercise and neighborhood greenness and walkability. Environ Res 167, 175–183. [DOI] [PubMed] [Google Scholar]
- Jones A, Hillsdon M, Coombes E, 2009. Greenspace access, use, and physical activity: understanding the effects of area deprivation. Prev Med 49, 500–505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kalsch H, Hennig F, Moebus S, Mohlenkamp S, Dragano N, Jakobs H, Memmesheimer M, Erbel R, Jockel KH, Hoffmann B, Heinz Nixdorf Recall Study Investigative, G., 2014. Are air pollution and traffic noise independently associated with atherosclerosis: the Heinz Nixdorf Recall Study. Eur Heart J 35, 853–860. [DOI] [PubMed] [Google Scholar]
- Kaufman JD, Adar SD, Barr RG, Budoff M, Burke GL, Curl CL, Daviglus ML, Diez Roux AV, Gassett AJ, Jacobs DR Jr., Kronmal R, Larson TV, Navas-Acien A, Olives C, Sampson PD, Sheppard L, Siscovick DS, Stein JH, Szpiro AA, Watson KE, 2016. Association between air pollution and coronary artery calcification within six metropolitan areas in the USA (the Multi-Ethnic Study of Atherosclerosis and Air Pollution): a longitudinal cohort study. Lancet 388, 696–704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim SR, Choi S, Keum N, Park SM, 2020. Combined Effects of Physical Activity and Air Pollution on Cardiovascular Disease: A Population-Based Study. J Am Heart Assoc 9, e013611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lo RH, 2009. Walkability: What is it? Journal of Urbanism 2, 145–166. [Google Scholar]
- Markevych I, Feng X, Astell-Burt T, Standl M, Sugiri D, Schikowski T, Koletzko S, Herberth G, Bauer CP, von Berg A, Berdel D, Heinrich J, 2019. Residential and school greenspace and academic performance: Evidence from the GINIplus and LISA longitudinal studies of German adolescents. Environ Pollut 245, 71–76. [DOI] [PubMed] [Google Scholar]
- Meline J, Chaix B, Pannier B, Ogedegbe G, Trasande L, Athens J, Duncan DT, 2017. Neighborhood walk score and selected Cardiometabolic factors in the French RECORD cohort study. BMC Public Health 17, 960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mora S, Cook N, Buring JE, Ridker PM, Lee IM, 2007. Physical activity and reduced risk of cardiovascular events: potential mediating mechanisms. Circulation 116, 2110–2118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Omura JD, Carlson SA, Brown DR, Hopkins DP, Kraus WE, Staffileno BA, Thomas RJ, Lobelo F, Fulton JE, American Heart Association Physical Activity Committee of the Council on, L., Cardiometabolic, H., Council on, C., Stroke, N., Council on Clinical, C., 2020. Built Environment Approaches to Increase Physical Activity: A Science Advisory From the American Heart Association. Circulation 142, e160–e166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ren Y, Qu Z, Du Y, Xu R, Ma D, Yang G, Shi Y, Fan X, Tani A, Guo P, Ge Y, Chang J, 2017. Air quality and health effects of biogenic volatile organic compounds emissions from urban green spaces and the mitigation strategies. Environ Pollut 230, 849–861. [DOI] [PubMed] [Google Scholar]
- Rojas-Rueda D, Nieuwenhuijsen MJ, Gascon M, Perez-Leon D, Mudu P, 2019. Green spaces and mortality: a systematic review and meta-analysis of cohort studies. Lancet Planet Health 3, e469–e477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tang HZ, Liu WP, Yun WJ, 2018. Spatiotemporal Dynamics of Green Spaces in the Beijing–Tianjin–Hebei Region in the Past 20 Years. Sustainability 10, 2949. [Google Scholar]
- Thijssen DH, Maiorana AJ, O’Driscoll G, Cable NT, Hopman MT, Green DJ, 2010. Impact of inactivity and exercise on the vasculature in humans. Eur J Appl Physiol 108, 845–875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang M, Aaron CP, Madrigano J, Hoffman EA, Angelini E, Yang J, Laine A, Vetterli TM, Kinney PL, Sampson PD, Sheppard LE, Szpiro AA, Adar SD, Kirwa K, Smith B, Lederer DJ, Diez-Roux AV, Vedal S, Kaufman JD, Barr RG, 2019a. Association Between Long-term Exposure to Ambient Air Pollution and Change in Quantitatively Assessed Emphysema and Lung Function. JAMA 322, 546–556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang M, Hou ZH, Xu H, Budoff MJ, Szpiro AA, Vedal S, Kaufman JD, Lu B, 2020. Ambient air pollution, traffic proximity and coronary atherosclerotic phenotype in China. Environ Res 188, 109841. [DOI] [PubMed] [Google Scholar]
- Wang M, Hou ZH, Xu H, Liu Y, Budoff MJ, Szpiro AA, Kaufman JD, Vedal S, Lu B, 2019b. Association of Estimated Long-term Exposure to Air Pollution and Traffic Proximity With a Marker for Coronary Atherosclerosis in a Nationwide Study in China. JAMA Netw Open 2, e196553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weier J, Herring D, 2011. Measuring Vegetation (NDVI & EVI; ) Available: https://earthobservatory.nasa.gov/features/MeasuringVegetation (accessed 30 June, 2020). [Google Scholar]
- Xiao X, Yang BY, Hu LW, Markevych I, Bloom MS, Dharmage SC, Jalaludin B, Knibbs LD, Heinrich J, Morawska L, Lin S, Roponen M, Guo Y, Lam Yim SH, Leskinen A, Komppula M, Jalava P, Yu HY, Zeeshan M, Zeng XW, Dong GH, 2020. Greenness around schools associated with lower risk of hypertension among children: Findings from the Seven Northeastern Cities Study in China. Environ Pollut 256, 113422. [DOI] [PubMed] [Google Scholar]
- Xu H, Bechle MJ, Wang M, Szpiro AA, Vedal S, Bai Y, Marshall JD, 2018. National PM2.5 and NO2 exposure models for China based on land use regression, satellite measurements, and universal kriging. Sci Total Environ 655, 423–433. [DOI] [PubMed] [Google Scholar]
- Yang BY, Liu KK, Markevych I, Knibbs LD, Bloom MS, Dharmage SC, Lin S, Morawska L, Heinrich J, Jalaludin B, Gao M, Guo Y, Zhou Y, Huang WZ, Yu HY, Zeng XW, Hu LW, Hu Q, Dong GH, 2020. Association between residential greenness and metabolic syndrome in Chinese adults. Environ Int 135, 105388. [DOI] [PubMed] [Google Scholar]
- Yeager RA, Smith TR, Bhatnagar A, 2020. Green environments and cardiovascular health. Trends Cardiovasc Med 30, 241–246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang JY, Tan PY, Zeng H, Zhang Y, 2019. Walkability Assessment in a Rapidly Urbanizing City and Its Relationship with Residential Estate Value. Sustainability 11, 1–20. [Google Scholar]
- Zhao D, Liu J, Wang M, Zhang X, Zhou M, 2019. Epidemiology of cardiovascular disease in China: current features and implications. Nat Rev Cardiol 16, 203–212. [DOI] [PubMed] [Google Scholar]
- Zou GY, 2008. On the estimation of additive interaction by use of the four-by-two table and beyond. Am J Epidemiol 168, 212–224. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.