

Abstract
Aim:
The Aim of the study was to evaluate the reproducibility of condylar inclination values obtained using three different interocclusal recording materials in Hanau Wide-Vue semi-adjustable articulator and to compare those values of condylar inclination with panoramic radiographic images.
Settings and Design:
In Vivo Comparative study.
Materials and Methods:
The clinical trial was carried out in the Department of Prosthodontics, M. R Ambedkar Dental College and Hospital, Bengaluru. A total of 30 dentulous subjects aged between 20 and 40 years were selected, without any signs and symptoms of temporomandibular joint disorders. With the help of a custom-made protrusive guide, protrusive records for three materials were made. These records were used for programming the articulator and the respective horizontal condylar inclination (HCI) value, and panoramic radiographs were made. The values obtained were statistically analyzed.
Statistical Analysis Used:
Independent t-test, multiple comparisons using Bonferroni method followed by Analysis of variances (ANOVA) were used.
Results:
Among each pair of groups there exists a significant difference, i.e., the mean condylar inclination (degree) was found to be statistically significant between wax and polyvinyl siloxane (P < 0.01) as well as between wax and polyether (P < 0.01). No significant difference was observed between polyvinyl siloxane and polyether (P > 0.05).
Conclusion:
HCI values differed depending on the type of material employed. The study concluded that the protrusive condylar guidance angles obtained by panoramic radiograph can be used in programming the semi-adjustable articulator and among the materials polyether gave the highest Condylar Guidance values with less variability and wax gave lowest values with greater variation.
Keywords: Condylar guidance, interocclusal records, panoramic radiograph, semi-adjustable articulator
INTRODUCTION
An analog of the condylar guidance on an articulator is considered to be a necessary requisite in prosthodontics. Condylar guidance is described as mandibular guidance generated by the condyle and articular disc traversing the contour of the articular eminence.[1] If condylar guidance is not recorded accurately, it will lead to occlusal interferences during mandibular movements. This may also increase chairside denture adjustment time, which can be frustrating for both the patient and the dentist.[2] For this reason, it is necessary to record the maxillomandibular relationship accurately.
Articulators attempt to simulate mandibular movement. The ability to simulate mandibular movement in the articulator is dependent on design of the articulator, ability in recording condylar guidance determinants, and programming of the articulator to those determinants.[3]
The condylar inclinations provided in semi-adjustable articulators are horizontal and lateral condylar inclinations. Horizontal condylar inclination (HCI) is usually obtained with protrusive interocclusal record and the lateral condylar inclination can be calculated either from HCI using Hanau's formula or with individual lateral records.
There has been unreliability of recording and reproducing the condylar guidance on semi-adjustable articulators. Consecutive condylar guidance angles recorded showed variation between operators, between recording materials, and between articulators.[4] Apart from the previously mentioned methods, condylar guidance can also be measured from radiographs. Compared to clinical methods, radiographic measurement involves stable bony landmarks and can be standardized.[5]
Recently, digital panoramic radiography has made them safer, more accurate, and comparatively cheaper resulting in their widespread application in many areas of dentistry. It can be argued that the application of advanced imaging is unwarranted in prosthodontics. Yet, the higher levels of safety, accuracy, and ultimate patient benefit from advanced digital imaging suggest that time may be ripe for its introduction into prosthodontics. However, evidence-based adoption of digital panoramic radiography for stomatognathic measurements and calibration of the dental articulators calls for definitive comparative studies in this area.[2] Currently, high quality panoramic machines are being manufactured which have much greater versatility than the conventional panoramic machines. Such machines have a capability for adding on a cephalometric attachment to allow exposure of standardized skull views.[6] This study, therefore, aimed at comparing condylar guidance measurements made using panoramic radiography and interocclusal wax records with interocclusal jig in healthy adults and also comparatively assess the accuracy and reproducibility of three commonly employed interocclusal recording materials, namely interocclusal wax, polyvinylsiloxane, and polyether in obtaining the condylar inclination values in semi-adjustable articulators.
MATERIALS AND METHODS
The study was conducted in the Department of Prosthodontics, M R Ambedkar Dental College and Hospital, Bangalore, Karnataka, India. Written consent was obtained from all the patients. Thirty patients aged between 20 and 40 years with a full complement of dentition fulfilling the following criteria were selected MRADC&H/ECIRB/0827/2016-17.
Inclusion criteria
Inclusion criteria were Angle's Class I molar and incisal relations, absence of crowded or malaligned teeth, good oral hygiene, and periodontal status.
Exclusion criteria
Exclusion criteria were completely edentulous patients, subjects with missing anterior teeth, subjects with any temporomandibular disorder, subjects with restricted mandibular movement, subjects with gross attrition, abrasion or erosion of teeth, lack of adequate neuromuscular control of jaw movements, and pregnancy.
Obtaining panoramic radiograph of the patient
The images were acquired at 74 kVp and 10 mA. All images were made with digital unit KODAK-Trophy 8000c Digital Panoramic and Cephalometric system.
Obtaining sagittal condylar guidance angles from panoramic radiograph tracing
Two radio-opaque lines are consistently apparent on the panoramic radiographs in the region of the temporal bone.One depicts the outline of the articular eminence and fossa and the second depicts the inferior border of the zygomatic arch. Radiographic tracings of the right and left side condylar guidance angle, were made [Figure 1a and b]. A horizontal reference line was marked by joining the orbitale and porion. The most superior and the most inferior points of the curvatures were identified. These two lines were connected by a straight line representing the mean curvature line. Angles made by the intersection of the mean curvature line and the horizontal reference line were measured [Figure 2a and b]. The same procedure was followed for 30 patients and 60 condylar guidance values (30 right sides and 30 left side of the condyle) were obtained. The mean of 60 Condylar Guidance (CG) angle value was calculated and tabulated.
Figure 1.
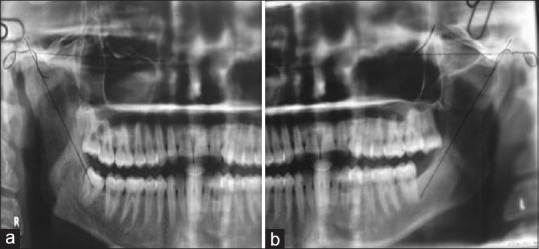
Panoramic radiographic image, (a) right side with overlapped tracing of condylar guidance angle, (b) left side with overlapped tracing of condylar guidance angle
Figure 2.
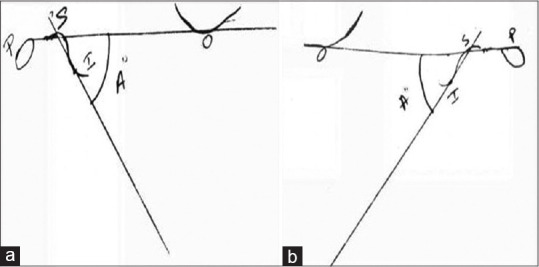
Tracing obtained on the transparent sheet, (a) Right side tracing, (b) Left side
Two sets of maxillary and mandibular impressions were made with irreversible hydrocolloid impression material (Algitex, Dental products of India) for each patient and poured immediately with Type III dental stone (Kalabhai, Karskarson Pvt. Ltd.). The set casts were retrieved, inspected, trimmed, and finished.
Relating the casts to the articulators
Facebow transfer records were made to relate the maxillary casts to the semi-adjustable articulator.
Facebow transfer
Low fusing impression compound was conditioned in a hot water bath in a rubber bowl; it was uniformly softened and was placed over the bite fork of the facebow, and the fork was placed into the patient mouth. The patient midline was aligned with the index notch of the bite fork so that it is parallel with the patient's coronal and horizontal plane. The impression of maxillary cusp tip was made on the low fusing impression compound , soft tissue registration and excess registration materials were trimmed away. After trimming the impression material from the bite fork, it was checked in the patient mouth for accuracy and stability. With the bite fork of facebow related to maxillary arch by means of occlusal indentations, the stem of the fork slides through the opening in the clamp of the bow. The patient was asked to grasp both arms of the facebow and bring them backward to position the earpieces of the facebow in external auditory meatus and hold them in place with a firm forward pressure. The orbital pointer of the facebow is positioned to align with orbitale of the patient [Figure 3a and b]. The bow was adjusted parallel to the line between the pupils of the eye. The locking device was grasped to resist torquing and the three thumbscrews were tightened in the following order, i.e., 1, 2, and 3 from left to right.
Figure 3.

Hanau springbow used for facebow recording (orbitale is used as the third reference point), (a) frontal view, (b) lateral view
The entire face bow assembly was removed by advising the patient to pull the earpiece out of their ears while helping them to remove the bite fork from the mouth. The facebow record was then transferred to the articulator. Maxillary cast was securely seated on maxillary occlusal index of the supported bite fork and the maxillary cast was mounted [Figure 4].
Figure 4.

Facebow transfer done to orient maxillary cast in Hanau articulator
Obtaining interocclusal record at maximum intercuspal position (MICP)
The baseplate wax was softened, adapted to the mandibular arch, and the patient was instructed to bite in MICP. The record was then removed from the patient mouth, washed, and placed in ice cold water. The articulator was inverted and interocclusal record at MICP was carefully seated onto the maxillary casts and the mandibular cast was positioned on the record and checked for stability of the cast. Mandibular cast was mounted with dental plaster.
Fabrication of the protrusive guide
A custom-made protrusive guide was fabricated prior to obtaining protrusive interocclusal record. Autopolymerizing clear acrylic resin (DPI – RR cold cure, Dental products India Ltd., Mumbai, India) was used to make a custom-made anterior jig [Figure 5a]. The autopolymerizing acrylic resin was sprinkled on to the labial surface of the cast to cover the anterior teeth along with an extension of 1 mm incisal to the two central incisors. The palatal surface of the jig was trimmed into a flat platform. After polymerization, the protrusive guide was retrieved from the model, trimmed, and adjusted in the patient's mouth to guide the mandibular anterior teeth to the same protrusive edge-to-edge position. Softened impression compound was placed at the incisal edge of the jig and the patient was asked to bite in the same protrusive position [Figure 5b]. The jig was removed, washed, and placed in ice cold water. The indentation of lower teeth on the incisal edge of the jig will help in positioning the mandibular anterior teeth to the same protrusive edge-to-edge position during impression making.
Figure 5.
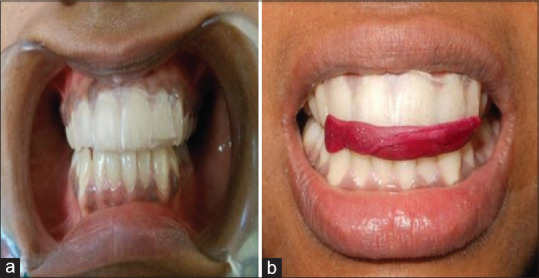
Protrusive jig, (a) frontal view, (b) jig with impression compound in the incisal edge (indentation on compound help in repeatedly placing teeth in the same position)
Making of protrusive interocclusal records
The customized protrusive jig was placed over the maxillary anterior teeth and the patient was trained to protrude the mandible as guided by the jig. Three interocclusal record materials were used.
Protrusive interocclusal records with Aluwax
The Aluwax was softened and was placed over the mandiblular arch. The patient was made to bite in protrusion (edge-to-edge position) as guided by a protrusive jig [Figure 6a]. The record was cooled, removed from the patient mouth, and placed in ice cold water.
Figure 6.
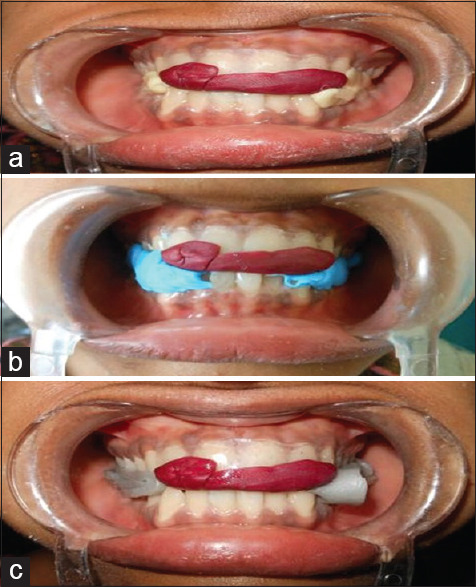
(a) Interocclusal bite registered with Aluwax in protrusive, (b) interocclusal bite registered with polyvinyl siloxane in protrusive, (c) interocclusal bite registered with polyether in protrusive
Protrusive interocclusal record with polyvinyl siloxane polyether
Polyvinyl siloxane and polyether interocclusal recording material was injected on the occlusal surface of mandibular teeth. The patient was asked to close in protrusive edge-to-edge position as guided by jig [Figure 6b and c]. Set material is removed from the patient mouth and washed. The excess is trimmed and stored in a clean dry area.
Centric lock and thumb nut for horizontal inclination of the condylar guidance of the Hanau articulator were loosened. Protrusive interocclusal record which was obtained by Aluwax was placed on the lower cast and stabilized. The maxillary cast was carefully guided into protrusion, slightly engaging the cast into indentation of the Aluwax protrusive record. The right and left condylar guides were rotated back and forth to accurately seat the maxillary cast into the protrusive relation record. The thumb nuts for horizontal inclination of the condylar guide were tightened and readings shown on right and left side of the condylar guide of the articulator were recorded. Similarly, other two records (polyvinyl and polyether) were used for programming the articulator and three readings of different interocculsal materials for protrusive condylar angle were obtained. The same procedure was repeated for all 30 patients and the mean protrusive condylar guidance angle was calculated and tabulated.
Statistical analysis
The data were analyzed by ANOVA. When a significant difference was detected among the means, Bonferroni test (post hoc test) was applied.
RESULTS
Mean CG's angle measurement values obtained from each interocclusal material were 34.85°, 39.27°, 39.58°, and 38.77°, respectively, for wax, polyvinyl siloxane, polyether, and panoramic radiograph [Table 1].
Table 1.
Estimation of mean and standard deviation of condylar guidance angle values for wax, polyvinyl siloxane, and polyether and panoramic radiograph
| Methods | Mean | SD |
|---|---|---|
| Wax | 34.85 | 4.85 |
| Polyvinyl siloxane | 39.27 | 3.61 |
| Polyether | 39.58 | 5.88 |
| OPG | 38.77 | 2.56 |
SD: Standard deviation, OPG: Orthopantomograph
Independent t-test and multiple comparisons using the Bonferroni method followed by ANOVA are used in this study to compare the reproducibility of horizontal condylar guidance values using three different interocclusal recording materials in a semi-adjustable articulator and a panoramic radiograph.
In this study, P ≤ 0.001 was considered as the level of significance. ANOVA test was used to compare the means of horizontal condylar guidance values obtained among three interocclusal materials. Higher mean condylar inclination (degree) was recorded in polyether method followed by polyvinyl siloxane and wax methods respectively. The difference in mean condylar inclination (degree) was found to be statistically significant among the groups (p<0.001) [Table 2].
Table 2.
ANOVA
| Source of variation | df | SS | Mean SS | F | P |
|---|---|---|---|---|---|
| Between groups | 2 | 420.117 | 210.058 | 8.865 | <0.001* |
| Within groups | 87 | 2061.483 | 23.695 | - | - |
| Total | 89 | 2481.600 | - | - | - |
*Denotes significant difference. SS: Sum of squares
The difference in mean condylar inclination (degree) was found to be statistically significant between wax and polyvinyl siloxane (P < 0.01) as well as between wax and polyether (P < 0.01). No significant difference was observed between polyvinyl siloxane and polyether (P > 0.05) [Table 3 and Graph 1].
Table 3.
Comparisons using Bonferroni method
| (I) Method | (J) Method | Mean difference (I-J) | P |
|---|---|---|---|
| Wax | Polyvinyl siloxane | −4.417 | 0.002* |
| Polyether | −4.733 | 0.001* | |
| Polyvinyl siloxane | Wax | 4.417 | 0.002* |
| Polyether | −0.317 | 1.000 | |
| Polyether | Wax | 4.733 | 0.001* |
| Polyvinyl siloxane | 0.317 | 1.000 |
*Denotes significant difference
Graph 1.
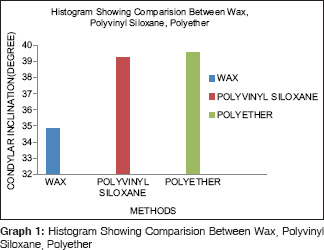
Histogram Showing Comparision Between Wax, Polyvinyl Siloxane, Polyether
Independent samples t-test was done as results showed that the difference in mean condylar inclination (degree) between Wax and Orthopantomograph was found to be statistically significant (P < 0.001) [Graph 2].
Graph 2.
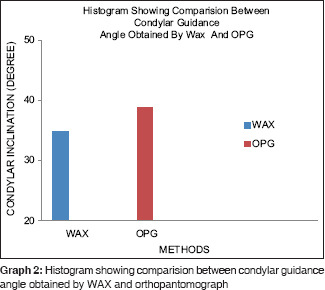
Histogram showing comparision between condylar guidance angle obtained by WAX and orthopantomograph
The difference in mean condylar inclination (degree) between polyvinyl siloxane and Orthopantomograph (OPG) was not statistically significant (P > 0.05) [Graph 3]. The difference in mean condylar inclination (degree) between polyether and OPG was not statistically significant (P > 0.05) [Table 4 and Graph 4].
Graph 3.
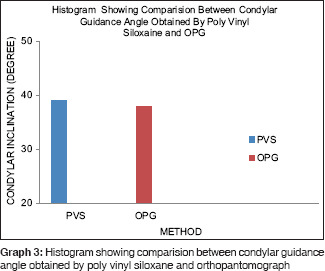
Histogram showing comparision between condylar guidance angle obtained by poly vinyl siloxane and orthopantomograph
Table 4.
Comparison of condylar inclination (deg) of each method with OPG
| Method | Mean | SD | Mean difference | T | P |
|---|---|---|---|---|---|
| Wax | 34.85 | 4.85 | −3.917 | −3.911 | <0.001* |
| OPG | 38.77 | 2.56 | |||
| Polyvinyl siloxane | 39.27 | 3.61 | 0.500 | 0.619 | 0.538 |
| OPG | 38.77 | 2.56 | |||
| Polyether | 39.58 | 5.88 | 0.817 | 0.698 | 0.490 |
| OPG | 38.77 | 2.56 |
*Denotes significant difference. SD: Standard deviation, OPG: Orthopantomograph
Graph 4.
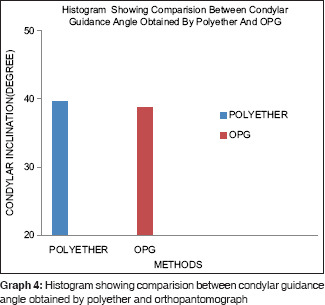
Histogram showing comparision between condylar guidance angle obtained by polyether and orthopantomograph
The mean condylar guidance angles obtained by all three different interocclusal materials are compared with Orthopantomograph and have been represented in [Graph 5].
Graph 5.
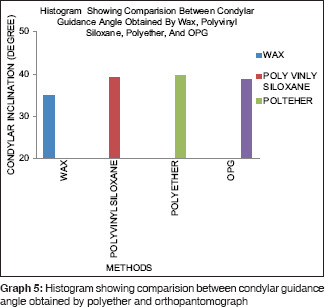
Histogram showing comparision between condylar guidance angle obtained by polyether and orthopantomograph
DISCUSSION
The importance of condylar guidance has been stressed upon by many researchers with their main concern to record condylar guidance accurately and transfer the same to the articulator. Condylar guidance depends on the steepness of the glenoid fossae. The steeper the contour of glenoid fossae, more will be the condylar force on the anterior region during protrusion. Many practitioners rely on average values of condylar guidance, which range from 22° to 65°.[7,8,9]
For dentate patients, the paths which the condyles follow in the glenoid fossae are determined by (1) bony limitations which comprise the joint, (2) direction and tonicity of the attaching muscles, and (3) limitation of movement imposed by attaching ligaments. When a natural dentition is present, the leading role in the dictation of the condylar path is played by the teeth.[10]
The accuracy of an interocclusal record is influenced not only by the material properties but also by the recording technique, as well as the reliability of the mandibular position influenced by the occlusal contacts, muscular action, or tissue changes within the joints. Moreover, the accuracy of fit of the recording material on the study or working casts seems to be a critical factor in the whole procedure.[11]
Elastomers as interocclusal record materials consistently yielded the least error among the materials studied.[12,13,14] They are easy to manipulate and do not need a carrier when used in the mouth. They offer little or no resistance to closure, set to a consistency that makes them easy to trim without distortion, and accurately reproduce tooth details.[12]
Most of the studies comparing the efficiency of interocclusal recording materials were done on the laboratory simulated models at MICP. Clinical studies comparing the effects of different interocclusal recording materials as to the levels of their accuracy and reproducibility of horizontal condylar registrations in semi-adjustable articulators have not been studied adequately.
In view of the above, the present clinical study was conducted to comparatively assess the effects of three commonly employed interocclusal recording materials, namely interocclusal wax, polyvinyl siloxanes, and polyether in obtaining the condylar guidance angle values in a semi-adjustable arcon articulator for their reproducibility of protrusive condylar guidance and their evaluation with panoramic radiographic method.
In this study, 30 patients aged between 20 and 40 years with a full complement of dentition were selected. Two sets of maxillary and mandibular impression were made and poured with Type III dental stone. One set was used for mounting on articulator and the other one for fabrication of protrusive jig.[15] Articulation was done in MICP via bite registration records. A custom-made protrusive guide was fabricated to allow edge-to-edge contact of anterior teeth with 6 mm of protrusion.[15] The use of the anterior jig provided the desired amount of interocclusal space for the recording material and practically eliminated the risk of mandibular deviation due to muscle fatigue. The amount of protrusion has a direct influence on the amount of separation between the posterior teeth and on stomatognathic apparatus.[16]
A total of 30 (3 × 30 = 90) protrusive records obtained using anterior jig were used to program the articulator which gave 180 condylar guidance values (right and left). Many methods are used to determine the sagittal condylar guidance such as wear facets,[17] intraoral protrusive record, extraoral method such as mandibular motion analyzer,[18] tracing method,[9] and electronic pantography.[19] However, the most frequently used method in the articular individualization is eccentric interocclusal records.[20] The procedure is simple and quick, and applicable in daily clinical practice.
During the study, all the interocclusal records were handled carefully and were used immediately to program the articulator to reduce any time dependant distortion. Abrupt withdrawal of interoccusal material might produce dimensional changes in both horizontal and vertical planes.[12]
Data obtained from 30 patients were tabulated and analyzed. The mean sagittal condylar guidance angle from panoramic radiograph was calculated. Table 2 shows that higher mean condylar inclination (deg) was recorded in polyether method followed by polyvinyl siloxane and wax methods. The difference in mean condylar inclination (deg) was found to be statistically significant among the groups (P < 0.001).
Bonferroni method was carried out to find out significant difference between groups [Table 3]. Shows the difference in mean condylar inclination (deg) and was found to be statistically significant between wax and polyvinyl siloxane (P < 0.01) as well as between wax and polyether (P < 0.01). No significant difference was observed between polyvinyl siloxane and polyether (P > 0.05).
Among all the three interocclusal materials, wax was found to be statistically significant and thus found to be highly variable and unreliable as interocclusal recording material. Literature shows protrusive condylar guidance registration using waxes which shows greater variation with ranges up to l0° between articulators.[11,18,21] Polyvinyl siloxane exhibited the greatest resistance to compression,[11] and polyether and polyvinyl siloxane produced the lowest vertical discrepancy in mounted casts with greatest by wax.[16,22]
In this study the angles which were recorded by interocclusal materials and OPG were between 30° and 50° which was in accordance to other studies by various authors where they found variations in condylar guidance angles ranging from 5° to 55°.[7,15,20,23] A review stated that “no radiographically determined sagittal condylar guidance angle coincided with that obtained with the use of intra-oral records. The radiographically determined angle showed a greater mean value than that determined by intra-oral records.”[2]
In this study, the mean CG angle value obtained by OPG is compared [Table 4] with mean CG angle value obtained by all three different interoccusal materials. It was found that there were statistically significant values (deg) between OPG (38.77) and Aluwax (34.85) with P < 0.001) and there was no statistically significant value between OPG and polyvinyl siloxane and polyether P > 0.05).
Studies have stated that Whip Mix consistently gave the highest angulations and Hanau the lowest, in the same patients.[15,24] The present study supports previous studies showing intraoral methods of recording condylar guidance angles have lower levels of reproducibility and are subject to variations of instrument, operator, and occlusal records.[15]
Semi-adjustable articulator was used in this study which is limited in their capabilities to accurately simulate the temporomandibular joints (TMJs) and the jaws and their movements because of the fixed intercondylar distances and the straight condylar pathways, which are reported to cause errors especially in the horizontal and frontal plane.[8] Arbitrary hinge axis is being used to transfer the facebow record to the articulator might be the reason for variance between the radiograph and rest of the methods. Future studies should investigate the possible effect that TMJ disorders which might have on clinical methods. It may be beneficial to employ a panoramic radiograph for condylar measurements, especially for complex oral rehabilitations. However, further studies with larger sample sizes are required to confirm the results of the present study. Human errors count is neglected as a limitation because it has been proved that the method of recording interocclusal relations and interpretation of condylar guidance values from the articulator is subjected to vary between examiners.
The parallax effect due to positioning errors when making a panoramic radiograph may lead to a relative change in positions of two radio-opaque lines, i.e., outline of the articular eminence and fossa, which can be confusing.
CONCLUSION
Within limitations of this in vivo study, the following conclusions were drawn:
Polyether and polyvinyl siloxanes interocclusal recording materials exhibited very minimal variation in recording condylar guidance angle values
Wax exhibited wide variation in recording condylar guidance angle values.
Comparative evaluation of the mean condylar guidance angle values obtained using three different interocclusal recording materials in a semi-adjustable articulator and panoramic radiograph revealed that protrusive condylar guidance angles obtained by panoramic radiograph may be used in programming semi-adjustable articulators.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Gilboa I, Cardash HS, Kaffe I, Gross MD. Condylar guidance: Correlation between articular morphology and panoramic radiographic images in dry human skulls. J Prosthet Dent. 2008;99:477–82. doi: 10.1016/S0022-3913(08)60112-2. [DOI] [PubMed] [Google Scholar]
- 2.Shreshta P, Jain V, Bhalla A, Pruthi G. A comparative study to measure the condylar guidance by the radiographic and clinical methods. J Adv Prosthodont. 2012;4:153–7. doi: 10.4047/jap.2012.4.3.153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Payne JA. Condylar determinants in a patient population: Electronic pantograph assessment. J Oral Rehabil. 1997;24:157–63. doi: 10.1046/j.1365-2842.1997.00452.x. [DOI] [PubMed] [Google Scholar]
- 4.Tannamala PK, Pulagam M, Pottem SR, Swapna B. Condylar guidance: Correlation between protrusive interocclusal record and panoramic radiographic image: A pilot study. J Prosthodont. 2012;21:181–4. doi: 10.1111/j.1532-849X.2011.00811.x. [DOI] [PubMed] [Google Scholar]
- 5.Sharma LA, Azhagarasan NS, Shankar C, Sharma A. A comparative study of the effect of three different interocclusal recording materials on reproducibility of horizontal condylar registrations in two different semiadjustable articulators: A clinical study. Int J Prosthodont Rest Dent. 2011;1:155–62. [Google Scholar]
- 6.Gupta S, Jain S. Orthopantomographic analysis for assessment of mandibular asymmetry. J Indian Orthod Soc. 2012;46:33–7. [Google Scholar]
- 7.Isaacson D. A clinical study of the condyle path. J Prosthet Dent. 1959;9:927–35. [Google Scholar]
- 8.Kurth LE. Discussion of condylar determinants of occlusal patterns: Part I. Statistical report on condylar path variations. Part II. Condylar movements may affect the occlusal patterns of teeth. J Prosthet Dent. 1965;15:847–9. [Google Scholar]
- 9.Woelfel JB, Winter CM, Igarashi T. Five-year cephalometric study of mandibular ridge resorption with different posterior occlusal forms. Part I. Denture construction and initial comparison. J Prosthet Dent. 1976;36:602–23. doi: 10.1016/0022-3913(76)90025-1. [DOI] [PubMed] [Google Scholar]
- 10.Trapozzano VR. An analysis of current concepts of occlusion. J Prosthet Dent. 1955;5:764–82. [Google Scholar]
- 11.Nooji D, Sajjan SM. The third point of reference and its effect on the protrusive condylar guidance angles obtained in semi-adjustable articulator. J Indian Prosthodont Soc. 2008;8:71. [Google Scholar]
- 12.Mullick SC, Stackhouse JA, Jr, Vincent GR. A study of interocclusal record materials. J Prosthet Dent. 1981;46:304–7. doi: 10.1016/0022-3913(81)90219-5. [DOI] [PubMed] [Google Scholar]
- 13.Fattore L, Malone WF, Sandrik JL, Mazur B, Hart T. Clinical evaluation of the accuracy of interocclusal recording materials. J Prosthet Dent. 1984;51:152–7. doi: 10.1016/0022-3913(84)90251-8. [DOI] [PubMed] [Google Scholar]
- 14.Campos AA, Nathanson D. Compressibility of two polyvinyl siloxane interocclusal record materials and its effect on mounted cast relationships. J Prosthet Dent. 1999;82:456–61. doi: 10.1016/s0022-3913(99)70034-x. [DOI] [PubMed] [Google Scholar]
- 15.Gross M, Nemcovsky C, Friedlander LD. Comparative study of condylar settings of three semiadjustable articulators. Int J Prosthodont. 1990;3:135–41. [PubMed] [Google Scholar]
- 16.Posselt U, Nevstedt P. Registration of the condyle path inclination by intraoral wax records – Its practical value. J Prosthet Dent. 1961;11:43–7. [Google Scholar]
- 17.Goyal MK, Goyal S. A comparative study to evaluate the discrepancy in condylar guidance values between two commercially available arcon and non-arcon articulators: A clinical study. Indian J Dent Res. 2011;22:880. doi: 10.4103/0970-9290.94695. [DOI] [PubMed] [Google Scholar]
- 18.Hobo S, Shillingburg HT, Jr, Whitsett LD. Articulator selection for restorative dentistry. J Prosthet Dent. 1976;36:35–43. doi: 10.1016/0022-3913(76)90231-6. [DOI] [PubMed] [Google Scholar]
- 19.Wilkie ND. The anterior point of reference. J Prosthet Dent. 1979;41:488–96. doi: 10.1016/0022-3913(79)90079-9. [DOI] [PubMed] [Google Scholar]
- 20.Craddock FW. The accuracy and practical value of records of condyle path inclination. J Am Dent Assoc. 1949;38:697–710. doi: 10.14219/jada.archive.1949.0066. [DOI] [PubMed] [Google Scholar]
- 21.Müller J, Götz G, Bruckner G, Kraft E. An experimental study of vertical deviations induced by different interocclusal recording materials. J Prosthet Dent. 1991;65:43–50. doi: 10.1016/0022-3913(91)90045-x. [DOI] [PubMed] [Google Scholar]
- 22.Ecker GA, Goodacre CJ, Dykema RW. A comparison of condylar control settings obtained from wax interocclusal records and simplified mandibular motion analyzers. J Prosthet Dent. 1984;51:404–6. doi: 10.1016/0022-3913(84)90231-2. [DOI] [PubMed] [Google Scholar]
- 23.dos Santos J, Jr, Nelson S, Nowlin T. Comparison of condylar guidance setting obtained from a wax record versus an extraoral tracing: A pilot study. J Prosthet Dent. 2003;89:54–9. doi: 10.1067/mpr.2003.11. [DOI] [PubMed] [Google Scholar]
- 24.Gross M, Nemcovsky C, Tabibian Y, Gazit E. The effect of three different recording materials on the reproducibility of condylar guidance registrations in three semi-adjustable articulators. J Oral Rehabil. 1998;25:204–8. doi: 10.1046/j.1365-2842.1998.00225.x. [DOI] [PubMed] [Google Scholar]