

Abstract
Background and objective
Evaluation of the stage and severity of the chronic diabetic foot ulcer (CDFU) is vital to increase the healing rate and to select the suitable treatment. We aim to assess the influence of low-intensity laser irradiation (LILI) and hyperbaric oxygenation therapy (HBOT) to accelerate the CDFU healing thru the transcutaneous oxygen tension (TcPO2) measurements.
Materials and methods
Seventy-five diabetic patients (type 2) of both genders, their ages ranged from 40–65 years with CDFUs (duration of ulcer < 6 weeks). All patients were randomly assigned into LILI, HBOT, and the control group. Measurement of TcPO2 using transcutaneous oximetry was performed for all patients once in the baseline and consequently in the second, fourth, and sixth- weeks duration. LILI utilized by a 33-diode cluster contact applicator with output power 1440 mW, energy density (fluency) was adjusted for 4 J/Cm2 at 10 kHz, and for 8 min per session, three times per week for a total of consecutive 6 weeks. HBOT was pressurized up to 2.5 ATA and patients delivered 100% oxygen for 60 min per session for 30 sessions. The Control group received conventional wound care only, twice daily, with saline and apply a new bandage after cleaning.
Results
MANOVA revealed a statistically insignificant difference in the control group, while statistically significant improvement in both the LILI and HBOT groups. The intergroup comparisons showed an insignificant statistical difference in the pre-test, while highly statistically significant differences for the three post-measures in favor of HBOT and LILI groups. The percentage of improvement of the HBOT group was higher than LILI. Post-hoc test using the least significant difference (LSD) revealed statistically significant differences of HBOT in favor of the LILI group.
Conclusion
Both LILI and HBOT may be used as adjunctive methods to improve TcPO2 that accelerate healing in CDFUs. HBOT may be favorable in the improvement of TcPO2 than LILI.
Keywords: Transcutaneous oxygen tension, Diode laser irradiation, Hyperbaric oxygen therapy, Diabetic foot ulceration
Introduction
Diabetic foot ulcers are a significant complication that affects 4 ~ 10% of the diabetic population [1]. Furthermore, foot problems represent one of the foremost common reasons for hospitalization with diabetic patients. It's estimated that fifty diabetic amputees necessitate amputation of the contralateral limb thru the primary four years after the amputation of the primary limb [2, 3]. Chronic diabetic foot ulcers (CDFUs) are remarkably hypoxic, thru transcutaneous oxygen tensions (TcPO2) measured from 5 mm Hg to 25 mm Hg, compared to manage to tissue values of 30 mmHg to 55 mm Hg [4].
The drop of healing rates due to the imbalance between low oxygen delivery/availability, and the high tissue demand during recovery from tissue injury [5]. Chronic low TcPO2 and perfusion pressure could also be related to an accumulation of necrotic tissue and poor formation of the granulation and should contribute to the buildup of harmful substances within the peri-wound microenvironment like carboxylic acid (from hypoxia-induced anaerobic metabolism) that are further deleterious to wound healing [6].
Measurement of TcPO2 was used as a helpful tool to assess tissue oxygen supply and microperfusion directly at the wound site [7]. This makes it possible to predict the severity of ischemia and chances for healing and to pick a suitable treatment [8]. Oxygen is important for wound healing progression since it is engaged in cell production, collagen production, re-epithelization, and defense versus bacteria. Therapeutic strategies to correct this include local delivery of oxygen to the wound and systemic oxygen administration [9]. A review study presents the TcPO2 measurement as a technique to evaluate the delay of chronic wound healing and the fact of its complications [10]. The conventional TcPO2 values are greater than 55 mmHg and wound healing may be significantly impaired if the worth drops to < 30 mm Hg [11]. It'd now be possible to detect clinically relevant ischemia earlier, predict the long-run healing process, and choose a more appropriate treatment schedule [8–11].
Low-Intensity Laser Irradiation (LILI) has been presented to accelerate the speed of wound healing and tissue contracture of diabetic foot ulcers [12]. The treatment principle for LILI relies on photo-biomodulation effects which influence the components within the respiratory chain as primary photon acceptors [13]. Among other things, LILI may increase cell proliferation and have a positive impact on energy metabolism, additionally improving microcirculation and releasing growth factors [13–17].
Henry's Law states that the quantity of a perfect gas dissolved in the solution is directly proportional to its partial pressure. The principal impact of HBOT is to extend the oxygen absorption in tissues by developing the oxygen dissolved in circulating plasma and particularly into areas of relative hypoxia [18]. On a cellular level, HBO obviates the detrimental effects of ischemia‐reperfusion injury by inducing a sway over the amount of circulating reactive oxygen species [19–21]. Following Boyle's law (pressure of a gas are inversely proportional to its volume) [22–24], HBO reduces nitrogen bubbles in vessels in addition to decreasing the harmful effects of ischemia‐reperfusion effects [25].
Utilizing HBOT, the hemoglobin within the circulating blood becomes fully oxygenated and, additionally, oxygen physically dissolves in plasma in direct proportion to the partial pressure of oxygen. Through HBOT, the oxygen dissolved in the plasma to fulfill tissue necessities from oxygen without the aid from hemoglobin [26]. At 2 ~ 2.5 ATA oxygen pressure, physically dissolved oxygen in plasma increases by quite 10 folds. This primary effect of hyperbaric oxygenation generates a good gradient for oxygen diffusion from functioning capillaries to ischemic tissue sites [27].
HBOT is utilized in chronic wounds to extend oxygen delivery to ischemic tissue. Added benefits include reduced edema through hyperoxia‐induced vasospasm and reduced inflammation [25].
Wounds often have reduced oxygen supply (hypoxia) which impairs leukocyte bactericidal activities and wound healing. The good thing about HBO relies on the premise that raising tissue oxygen levels will enhance wound healing ability. Adjunctive HBO therapy is used within the management of DFUs [25, 27].
However, no investigations are distributed heretofore into whether an improvement within the tissue circulation or the transcutaneous oxygen tension occurs, which might be key to wound healing [28]. Hyperbaric Oxygenation Therapy (HBOT) is a very important therapeutic adjunct within the management of chronic diabetic foot ulcers because it increases transcutaneous oxygen tensions [29, 30]. The best advantage of HBOT is achieved in circumstances where the nourishing flow and oxygen supply to repair tissue are compromised, but within which the regional vascular network, a prerequisite for oxygen to succeed in tissues, is barely partially impaired [31]. The most effects of HBOT on the healing of diabetic foot ulcers include stimulus of fibroblast proliferation and diversity, increased collagen formation and cross-linking, augmented neovascularization, stimulation of leukocyte microbial killing, lethal effects on certain anaerobic bacteria, and inhibition of toxin formation by certain pathogenic microorganisms [29–31].
So, the presented study is a randomized controlled trial to analyze the influence of LILI versus HBOT on TcPO2 in CDFUs' healing rate, and it was hypothesized that there was an insignificant influence of both modalities.
Materials and methods
Design of the study
A randomized controlled experimental study design was conducted during the period from May to October 2020 in the foot care center at “Kobri El Koba Military Complex Hospital”. The study was ethically approved by the Institutional Ethical Committee of the “Faculty of Physical Therapy, Cairo University, Egypt (No: P.T.REC/009/002144)” and was registered on PACTR (PACTR202005532154206). All patients read and signed two copies of a consent form before the beginning of data collection.
Subject criteria
Seventy-five patients with type 2 diabetes since < 10 years of both genders (45 males and 30 females) with ages ranging from (40–65 years) with CDFUs (duration of ulcer < 6 weeks) were recruited to participate in this study. All patients underwent a suitable assessment to ensure inclusion criteria that contain all patients had controlled blood glucose levels all over the whole duration of the study in which (HbA1C < 48 mmol/mol). All patients had grade II (according to Wagner grading system) CDFUs. All Patients had Cardiac Ejection Fraction (CEF) ≥ 50%, blood pressure (BP) ≤ 150/90 mmHg, Chest X-ray of all patients reported normal and all of them are clinically evaluated by a specialized ear, nose, and thorax (ENT) physician to ensure fitting for the hyperbaric chamber. Patients were excluded from the study if they had chronic obstructive pulmonary disease, malignancy, or cardiac pacemakers and patients with any disorder that lead to ulcers other than diabetes such as a history of chronic peripheral arterial disease.
The principal investigator randomly assigned all patients, who were blinded, into three groups (the LILI, HBOT, and control group) using the closed envelope method. Each group was composed of 25 patients, as displayed in Fig. 1. Measurement of TcPO2 was performed for all participated patients once in the baseline and consequently in the second, fourth, and sixth- weeks duration.
Fig. 1.

The study flowchart and allocation
Study equipments
-
I.
Transcutaneous Oximetry: The Fiber Optic Oximeter-Medical-Monitoring-System (HMMS 4.7) BA_HMMS_4.7e_1114, Germany.
-
II.
Hyperbaric Oxygen Therapy (HBOT): (Haux, Starmed 2300, Germany). Double-lock, divided into Main chamber and Antichamber, with omega Ω-shape and all safety and CE-Certificate, as more illustrated in Fig. 3 in the Appendix.
-
III.
Low-intensity Laser Therapy (Class 3B): (Chattanooga group of encores medical, Intellect Advanced Mobile Laser, USA) was applied in contact to the wound using cling film as an isolator between the device head and the ulcer site, as shown in Fig. 4 in the Appendix.
Fig. 3.

a The patient site inside the hyperbaric oxygen chamber highlighting the patient`s chairs and all the vital accessories to provide a proper session; b The hyperbaric oxygen room with its controller, (1) The main control console for the hyperbaric oxygen chamber with the monitors, (2) The omega Ω-shape chamber consists of the main and Antichamber (Haux, Starmed 2300, Germany), (3) patient site inside the hyperbaric oxygen chamber highlighting the Antichamber door, (4) The manual chamber controller
Fig. 4.

a The examination room highlighting the patient examination trolley and the exploited low-intensity laser irradiation (LILI) devices, b The LILI device (Chattanooga group of encores medical, Intellect Advanced Mobile Laser, USA), c The specialized person doing his routine measuring the ulcer each session and recording its patient data
Investigation practices
Measurements techniques
Transcutaneous oxygen tension (TcPO2): We apply initial baseline TcPO2 measurements were accomplished all participants at the beginning of the different therapies with additional measurements by pulse oximetry monitoring. The TcPO2 had been measured by an electrochemical transducer (Radiometer, TCM400 Monitor, Denmark) with special fixation rings and contact liquid from the same manufacture. The temperature of the transducer was settled at 44 °C to enhance the oxygen molecule's permeability to the skin at the measuring location. We calculated the difference of TcPO2 consequent to the variation of TcPO2 between the beginning and the end of the therapy [32, 33].
Calibration: It is a process of equalizing the probe signal by a known concentration of oxygen content. It is necessary before each measurement to calibrate the transducer electrode to normal air of PO2 159 mmHg to gain accurate measurements, with the following Calibration steps:
Connect the electrode into the socket of the calibration channel
Re-membrane: It is essential to the membrane of the electrode before each use.
Activate the calibration button by leaving the electrode in normal air.
The program recognizes automatically when values have stabilized
The message “Calibration Finished” shows you that the calibration is finished successfully.
Click the button “Close Calibration”. Now, the button “Apply” became active and the device is ready to measure the patient’s TcPO2.
Intervention’s procedures
Laser Group: LILI was applied using contact technique by 33 Diode Cluster Applicator, which was arranged to produce total power output 1440 mW with the following wavelengths: 5 × 850 nm 200 mW Lasers, 12 × 670 nm 10mW,8 × 880 nm 25 mW, 8 × 950 nm 15mW and energy density (fluency) was adjusted for 4 J/Cm2 with a pulse frequency of 10 kHz. The therapist and patients wore goggles to protect their eyes. Each session lasted 8 min three times per week (every other day) for a total of consecutive 6 weeks.
HBOT Group: HBOT started with a gradual increase of oxygen pressure to be approximately 2.5 ATA through 15 min in a 100% oxygen delivered for 60 min Then, gradual decompression through 15 min for a total of 90 min per each session for 30 sessions (5 sessions per week for 6 weeks).
Control Group: This group received conventional wound care only which consisted of wound cleansing to keep the wound surface moist. Clean the area twice daily with saline and apply a new bandage after cleaning. There is no need to use hydrogen peroxide or alcohol for cleaning.
Statistical analysis
All statistical calculations were carried out using a computer program IBM SPSS version 22 (IBM Corporation, USA). The sample size calculations were performed using the G*Power software (version 3.0.10). The TcPO2 was chosen as the primary outcome measure. Its effect size was estimated to be medium (0.25). A generated sample size of at least 20 patients per group would be required. Allowing for a 20% dropout rate, it was necessary to reach a total sample of a minimum of 75 patients. The test of homogeneity (Leven's test) showed that all data were homogenous. The test of normality (Shapiro- Wilk test) showed that data were normally distributed, so the parametric test was used (MANOVA) to compare the within and between groups results. Post-hoc test using the least significant difference (LSD) was used to detect the favorability between groups (multiple comparisons). A P-value of less than 0.05 was considered statistically significant.
Results
General demographic data
There were statistically insignificant differences between the groups regarding the duration of diabetes, duration of ulcer, initial TcPO2, as illustrated in Table 1.
Table 1.
General demographic data
| Variables | LILI group (X ± SD) |
HBOT group (X ± SD) |
Control Group (X ± SD) |
P-value |
|---|---|---|---|---|
| Age(year) | 59.1 ± 7.68 | 60.9 ± 8.3 | 60.1 ± 9.1 | 0.52 |
| DDM (year) | 16 ± 4.4 | 16.1 ± 3.4 | 15.9 ± 3.2 | 0.47 |
| DU (month) | 3.5 ± 1.7 | 3.3 ± 1.3 | 3.2 ± 1.5 | 0.11 |
| TcPO2 (mmHg) | 23.37 ± 5.28 | 20.26 ± 5.26 | 23.22 ± 6.13 | 0.98 |
X± SD, mean± standard deviation; DDM, Duration of Diabetes mellitus; TcPO2, Transcutaneous Oxygen Tension; Significant at P-value <0.05
The transcutaneous oxygen tension (TcPO2)
The within-group comparisons showed a statistically insignificant difference in the control group, while statistically significant improvement in both the LILI and HBOT groups. The intergroup comparisons showed an insignificant statistical difference in the pre-test, while highly statistically significant differences for the three post-measures in favor of HBOT and LILI groups. The percentage of improvement of the HBOT group was higher than LILI, as displayed in Fig. 2 and illustrated in Table 2.
Fig. 2.
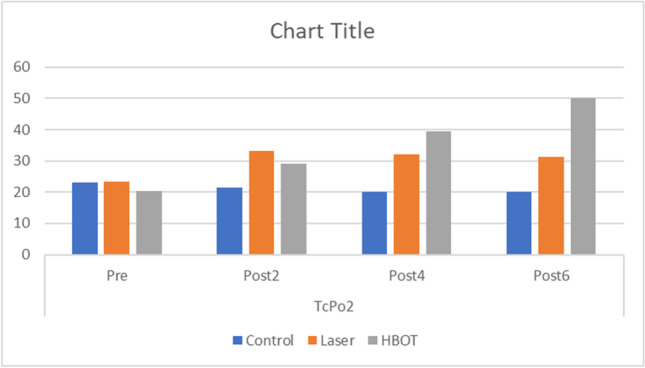
Transcutaneous oxygen tension (TcPO2) for hyperbaric oxygen therapy (HBOT- Grey Color), low-intensity laser irradiation group (LILI – Orange Color), and control group (Blue Color)
Table 2.
TcPO2 for HBOT, LILI, and control groups
| TcPo2 (mmHg) | ||||||
|---|---|---|---|---|---|---|
| Pre | Post2 | Post4 | Post6 | Within group comparison P-value |
Percentage of improvement | |
| Control | 23.22 ± 6.13 | 21.41 ± 9.77 | 20.22 ± 11.14 | 19.96 ± 10.88 | 0.59 | 14.04% |
| Laser | 23.37 ± 5.28 | 33.22 ± 5.41 | 32.22 ± 7.77 | 31.30 ± 11 | 0.000* | 33.93% |
| HBOT | 20.26 ± 5.26 | 29.15 ± 5.78 | 39.48 ± 8.43 | 50.15 ± 11.13 | 0.000* | 147.53% |
| In-Between Comparison | 0.075 | 0.000* | 0.000* | 0.000* | ||
Post-hoc test
There were statistically significant differences between both HBOT and LILI groups in favor of the control group, and statistically significant differences of HBOT in favor of the LILI group, as presented in Table 3.
Table 3.
Multiple comparisons between groups
| (I) Groups | (J) Groups | Mean difference (I-J) | Sig | |
|---|---|---|---|---|
| Post 2 | Control | Laser | -11.81* | 0.000 |
| HBO | -7.74* | 0.000 | ||
| Laser | Control | 11.81* | 0.000 | |
| HBO | 4.07* | 0.043 | ||
| HBO | Control | 7.74* | 0.000 | |
| Laser | -4.07* | 0.043 | ||
| Post 4 | Control | Laser | -12* | 0.000 |
| HBO | -19.26* | 0.000 | ||
| Laser | Control | 12* | 0.000 | |
| HBO | -7.26* | 0.005 | ||
| HBO | Control | 19.26* | 0.000 | |
| Laser | 7.26* | 0.005 | ||
| Post 6 | Control | Laser | -12* | 0.000 |
| HBO | -19.26* | 0.000 | ||
| Laser | Control | 12* | 0.000 | |
| HBO | -7.26* | 0.005 | ||
| HBO | Control | 19.26* | 0.000 | |
| Laser | 7.26* | 0.005 |
Discussion
The CDFUs` are quite possibly the most widely recognized and most genuine entanglements of diabetes mellitus and a typical reason for the requirement for hospitalization in diabetics [34]. Early evaluation of the CDFUs by TcPO2 measurements makes it possible to predict the severity of ischemia to increase chances for healing and pick up the suitable treatment [8].
We aim in this study to measure the improvements of TcPO2 in CDFUs to evaluate which technique is better LILI or HBOT. Both techniques reported statistically significant improvements of TcPO2 in CDFUs, regarding the proportion of improvement, it was 33.93% within the LILI group and 147.53% within the HBOT group within the 6th –week.
The rationale of this study was to turn on the evidence that oxygen demand and utilization rates are increased during tissue repair and wound healing. O2 is not stored within the tissue, therefore, adequate and continuous O2 supply to the location of the injury is critical for wound healing and repair [4]. This hypothesis is upheld by clinical perceptions that conveyance of oxygen to persistent injuries winds up in inordinate exudates age and subsequently, the fast development of granulation in these treated injuries [35–37].
In the concurrent study, the LILI group reported a statistical improvement in TcPO2 that was agreed by Kaviani et.al. who concluded that LILI contains a significant effect in the acceleration of diabetic foot ulcer healing by improving microcirculation and increasing transcutaneous oxygen saturation to the ulcer region [38]. But the precise and initial mechanism of laser-induced biomodulation remains to be elucidated. The rise of the local blood flow is additionally important in other areas of the clinical application of laser-induced biomodulation. Because the loco-regional increase of blood flow also contributes to local oxygenation [15].
Bio-stimulation effects of low-level laser therapy (LLLT) are extensively reported. There is great evidence that the applying of LLLT improves microcirculation and oxygen supply [39]. D.G. Minatel et.al. demonstrated a major enhancement of the oxygenation induced by a LILI. However, the mechanisms by which photo-stimulation influences microcirculation and oxygenation are still unclear [40]. Laser irradiation is additionally thought to extend the amount of oxygen content of the tissue. Low-level laser emission increased tissue oxygenation, morpho-functional activity, and substantial expansion of the microcirculatory bed. They, in turn, accelerated the restoration of functions, stimulation of adaptation ability, and stabilization of the hormonal status [41].
From the work of M. Dadpay et.al., it's clear that the importance of excellent oxygen tension in an exceedingly healing wound isn't limited to the nutritive effects of oxygen alone. The formation of a decent oxygen gradient may be a pathway along which mast cells, leukocytes, and macrophage cells, can make their way into the wound [42]. Vasodilation combined with the direct photo-effects of laser energy causes changes within the permeability of the walls of irradiated blood vessels, and platelets are stimulated to release platelet-derived protein (PDGF) which reinforces fibroblast chemotaxis, cell proliferation and contraction factors in new collagen fibers [40–42].
LLLT having an influence on perfusion or oxygenation simply after a period delay, after rehashed radiation, or with pathological starting conditions. While the postulated consequences of the LLLT, like countless cell proliferation, enhanced ATP convenience. Also, to wrap things up improved microcirculation, are supported changes within the cellular metabolism, an enhancement in perfusion or oxygenation will only occur after a given stage. It might be sensible if further studies on the oxygen saturation following LLLT including patients with chronic wounds seem to be worth recommending may influence the accelerated wound healing which is commonly observed [43]. Concerning the HBOT group the results were surprising to favor the LILT group, this comes to coincide with A 2015 Cochrane review that pooled data from 10 RCTs showed a major increase rate in healing with HBOT at 6 weeks. HBOT treatment for 90 minutes per day, 4 or 5 days per week supported developed protocols [44].
RCTs were identified that measured tissue oxygen level on diabetic wounds. Complete wound healing, clinical improvement, amputation, and transcutaneous oxygen levels were the outcomes. All studies reported that HBO treatment enhanced the whole healing rate of wounds [45]. RCT reported that comparison between transcutaneous oxygen measurements in normal air and at 2.5 ATA HBO could even be a reliable test to predict outcome in DFUs. Raised peri-wound transcutaneous oxygen estimations at 2.4 ATA and decreased peri-wound oxygen estimations at 1 ATA were related to a more quick reaction to HBO treatment in patients with chronic leg wounds [46].
Conclusion
Both LILI and HBOT may be used as adjunctive methods to improve TcPO2 that accelerate healing in CDFUs. To the extent of our knowledge, HBOT may be favorable in the improvement of TcPO2 than LILI. It is recommended to examine the combined application that may have dual beneficial effects and may enhance TcPO2 more.
Appendix
Data availability
The authors stated and declare that all data is exist and available.
Code availability
The authors stated and declare that all code is exist and available.
Declarations
Ethics approval
All experimental and investigation trails was conducted during the period from May to October 2020 in the foot care center at “Kobri El Koba Military Complex Hospital”. The study was ethically approved by the Institutional Ethical Committee of the “Faculty of Physical Therapy, Cairo University, Egypt (No: P.T.REC/009/002144)” and was registered on PACTR (PACTR202005532154206) at 22 May 2020.
Consent to participate
All patients read and signed two copies of a consent form before the beginning of data collection and within this research study.
Consent for publication
All the co-authors are agreed for the research study publication.
Conflicts of interest/Competing interests
The authors stated and declare that No conflict or competing of interests.
Limitations
The researchers were aware of the study limitations. It was the psycho-physiological factors for patients at the time of examination and treatment, which was assumed to be the same for patients all over the study.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Amir N. Wadee, Email: anazih@cu.edu.eg
Mohamed Hisham Fouad Aref, Email: MH-Aref@ieee.org.
Ayman A. Nassar, Email: ayman_nassar@knights.ucf.edu
Ibrahim H. Aboughaleb, Email: ehe43@hotmail.com
Siham M. Fahmy, Email: Fahmysiham@gmail.com
References
- 1.Guest JF, Fuller GW, Vowden P. Diabetic foot ulcer management in clinical practice in the UK: costs and outcomes. Int Wound J. 2018;15:43–52. doi: 10.1111/iwj.12816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lanting SM, Barwick AL, Twigg SM, Johnson NA, Baker MK, Chiu SK, et al. Journal of Diabetes and Its Complications Post-occlusive reactive hyperaemia of skin microvasculature and foot complications in type 2 diabetes. J Diabetes Complications [Internet]. Elsevier Inc.; 2017;31:1305–10. Available from: 10.1016/j.jdiacomp.2017.05.005. [DOI] [PubMed]
- 3.Lowry D, Saeed M, Uk M, Uk F, Narendran P, Tiwari A. The Difference Between the Healing and the Nonhealing Diabetic Foot Ulcer : A Review of the Role of the Microcirculation. 2017; [DOI] [PMC free article] [PubMed]
- 4.Lapi D, Di Maro M, Mastantuono T, Starita N, Ursino M, Colantuoni A. Arterial Network Geometric Characteristics and Regulation of Capillary Blood Flow in Hamster Skeletal Muscle Microcirculation. Front Physiol. Frontiers; 2019;9:1953. [DOI] [PMC free article] [PubMed]
- 5.Hu H-F, Hsiu H, Sung C-J, Lee C-H. Combining laser-Doppler flowmetry measurements with spectral analysis to study different microcirculatory effects in human prediabetic and diabetic subjects. Lasers Med Sci Springer. 2017;32:327–334. doi: 10.1007/s10103-016-2117-2. [DOI] [PubMed] [Google Scholar]
- 6.Perwitasari DA, Urbayatun S, Faridah IN, Amelia R, Lelo A. Relationship between emotional distress and quality of life on type 2 diabetes mellitus patients in Meranti island regency hospital Relationship between emotional distress and quality of life on type 2 diabetes mellitus patients in Meranti island regency . 2017;
- 7.Values M. Transcutaneous Oxygen Pressure Measurement in Diabetic Foot Ulcers Mean Values and Cut-Point for Wound Healing. 2013;40:585–9. [DOI] [PubMed]
- 8.Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med. Mass Medical Soc; 2017;376:2367–75. [DOI] [PubMed]
- 9.Jeffcoate WJ, Vileikyte L, Boyko EJ, Armstrong DG, Boulton AJM. Current challenges and opportunities in the prevention and management of diabetic foot ulcers. Diabetes Care Am Diabetes Assoc. 2018;41:645–652. doi: 10.2337/dc17-1836. [DOI] [PubMed] [Google Scholar]
- 10.Arsenault KA, McDonald J, Devereaux PJ, Thorlund K, Tittley JG, Whitlock RP. The use of transcutaneous oximetry to predict complications of chronic wound healing: A systematic review and meta-analysis. Wound Repair Regen Wiley Online Library. 2011;19:657–663. doi: 10.1111/j.1524-475X.2011.00731.x. [DOI] [PubMed] [Google Scholar]
- 11.Wang Z, Hasan R, Firwana B, Elraiyah T. A systematic review and meta-analysis of tests to predict wound healing in diabetic foot. J Vasc Surg [Internet]. Elsevier; 2011;63:29S-36S.e2. Available from: 10.1016/j.jvs.2015.10.004. [DOI] [PubMed]
- 12.Heu F, Forster C, Namer B, Dragu A, Lang W. Effect of low-level laser therapy on blood flow and oxygen-hemoglobin saturation of the foot skin in healthy subjects: a pilot study. Laser Ther International Phototherapy Association. 2013;22:21–30. doi: 10.5978/islsm.13-OR-03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mj LP, Ep KB. Effect of low level laser therapy on diabetic foot ulcers: a randomized control trial. Int Surg J. 2018;5:1008–1015. doi: 10.18203/2349-2902.isj20180821. [DOI] [Google Scholar]
- 14.Tchanque-fossuo CN, Ho D, Dahle SE, Koo E, Li C, Isseroff RR, et al. A systematic review of low-level light therapy for treatment of diabetic foot ulcer. 2016; [DOI] [PubMed]
- 15.Kajagar BM, Godhi AS, Pandit A, Khatri S. Efficacy of low level laser therapy on wound healing in patients with chronic diabetic foot ulcers—a randomised control trial. Indian J Surg Springer. 2012;74:359–363. doi: 10.1007/s12262-011-0393-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kajagar BM, Godhi AS, Pandit A, Khatri S. Efficacy of low level laser therapy on wound healing in patients with chronic diabetic foot ulcers-a randomised control trial. Indian J Surg. 2012;74:359–363. doi: 10.1007/s12262-011-0393-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Dogan SK, Ay S, Evcik D. The effectiveness of low laser therapy in subacromial impingement syndrome: a randomized placebo controlled double-blind prospective study. Clinics SciELO Brasil. 2010;65:1019–1022. doi: 10.1590/S1807-59322010001000016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Gunes AE. Hyperbaric Oxygen Therapy. 2019;
- 19.Golledge J, Singh TP. Systematic review and meta-analysis of clinical trials examining the effect of hyperbaric oxygen therapy in people with diabetes-related lower limb ulcers. Diabet Med Wiley Online Library. 2019;36:813–826. doi: 10.1111/dme.13975. [DOI] [PubMed] [Google Scholar]
- 20.Kusnanto K, Dismalyansa D, Pradanie R, Arifin H. Quality of life of diabetic foot ulcer patients with hyperbaric oxygen therapy. Folia Medica Indones. 2019;55:127–133. doi: 10.20473/fmi.v55i2.14344. [DOI] [Google Scholar]
- 21.ur Rahman M, Khan MRK, Ahmed T, Islam MS Bin, Nayeem R, Kalam MA. Hyperbaric Oxygen Therapy in Non Healing Wounds in a Referral Hospital of Bangladesh. J Bangladesh Coll Physicians Surg. 2019;37:109–18.
- 22.Pra AMA. E X Tra. 2012;25:38–44.
- 23.Guide S. Introduction to Ventilation. Mallinckrodt.
- 24.Bhutani S, Vishwanath G. Review Article Hyperbaric oxygen and wound healing. 2019;45. [DOI] [PMC free article] [PubMed]
- 25.Jukic I, Mišir M, Mihalj M, Mihaljevic Z, Unfirer S, Kibel D, et al. Mechanisms of HBO-Induced Vascular Functional Changes in Diabetic Animal Models. Hyperb Oxyg Treat Res Clin Pract Mech Action Focus. BoD–Books on Demand; 2018;87.
- 26.Abdelrahman AA. Hyperbaric oxygen therapy : A review. 2020;
- 27.Vinkel J, Lohse N, Hyldegaard O. The clinical use of hyperbaric oxygen in the treatment of Danish patients with diabetic foot ulcers. Dan Med J. 2019;66. [PubMed]
- 28.Tubachi P. Antibacterial effect of low level laser therapy in infective diabetic foot ulcers. IOSR J Dent Med Sci. 2015;14:110–114. [Google Scholar]
- 29.Fahmy SM, Aref MH, Aboughaleb IH, Rabie M, Abdlaty R. Hyperbaric Oxygen Therapy for Healing Diabetic Lower Extremity Ulcers. 2020 12th Int Conf Electr Eng ICEENG 2020. 2020;135–9.
- 30.Andrea K, Dávid B, Peter S, Martin Č, Elena L, Andrej D, et al. VASOMOTION CHANGES AFTER HYPERBARIC OXYGEN THERAPY IN DIABETIC PATIENTS. Indian J Appl Res. 2019;9.
- 31.Ennis WJ, Huang ET, Gordon H. Impact of hyperbaric oxygen on more advanced wagner grades 3 and 4 diabetic foot ulcers: matching therapy to specific wound conditions. Adv Wound Care. Mary Ann Liebert, Inc., publishers 140 Huguenot Street, 3rd Floor New …; 2018;7:397–407. [DOI] [PMC free article] [PubMed]
- 32.Catella J, Long A, Mazzolai L. What is currently the role of tcpo2 in the choice of the amputation level of lower limbs? A comprehensive review. J Clin Med. 2021;10:1413. doi: 10.3390/jcm10071413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Benhamou Y, Begarin L, David N, Cailleux N, Bessin C, Lévesque H, et al. Detection of microcirculatory impairment by transcutaneous oxymetry monitoring during hemodialysis: An observational study. BMC Nephrol. 2014;15. [DOI] [PMC free article] [PubMed]
- 34.Hornberger C, Herrmann BH, Daeschlein G, Von PS, Sicher C, Kuhn J, et al. Detecting bacteria on wounds with hyperspectral imaging in fluorescence mode. Curr Dir Biomed Eng. 2020;6:6–9. [Google Scholar]
- 35.Schaper NC, Van Netten JJ, Apelqvist J, Lipsky BA, Bakker K, (IWGDF) IWG on the DF. Prevention and management of foot problems in diabetes: a Summary Guidance for Daily Practice 2015, based on the IWGDF Guidance Documents. Diabetes Metab Res Rev. Wiley Online Library; 2016;32:7–15. [DOI] [PubMed]
- 36.Bakker K, Apelqvist J, Lipsky BA, Van Netten JJ, Schaper NC, (IWGDF) IWG on the DF. The 2015 IWGDF guidance documents on prevention and management of foot problems in diabetes: development of an evidence‐based global consensus. Diabetes Metab Res Rev. Wiley Online Library; 2016;32:2–6. [DOI] [PubMed]
- 37.Chen G, Gu J, Lou W, He X, Chen L, Su H, et al. Diabetic peripheral arterial disease: lower limb angiography results and one year outcomes of interventional treatment. Chinese J Radiol. 2010;44:1189–1193. [Google Scholar]
- 38.Kaviani A, Djavid GE, Ataie-Fashtami L, Fateh M, Ghodsi M, Salami M, et al. A randomized clinical trial on the effect of low-level laser therapy on chronic diabetic foot wound healing: a preliminary report. Photomed Laser Surg. Mary Ann Liebert, Inc. 140 Huguenot Street, 3rd Floor New Rochelle, NY 10801 USA; 2011;29:109–14. [DOI] [PubMed]
- 39.Kwan RL, Cheing GL, Vong SK, Lo SK. Electrophysical therapy for managing diabetic foot ulcers: a systematic review. Int Wound J Wiley Online Library. 2013;10:121–131. doi: 10.1111/j.1742-481X.2012.01085.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Minatel DG, Frade MAC, França SC, Enwemeka CS. Phototherapy promotes healing of chronic diabetic leg ulcers that failed to respond to other therapies. Lasers Surg Med Off J Am Soc Laser Med Surg. Wiley Online Library; 2009;41:433–41. [DOI] [PubMed]
- 41.Basso FG, Oliveira CF, Kurachi C, Hebling J, de Souza Costa CA. Biostimulatory effect of low-level laser therapy on keratinocytes in vitro. Lasers Med Sci Springer. 2013;28:367–374. doi: 10.1007/s10103-012-1057-8. [DOI] [PubMed] [Google Scholar]
- 42.Dadpay M, Sharifian Z, Bayat M, Bayat M, Dabbagh A. Effects of pulsed infra-red low level-laser irradiation on open skin wound healing of healthy and streptozotocin-induced diabetic rats by biomechanical evaluation. J Photochem Photobiol B Biol Elsevier. 2012;111:1–8. doi: 10.1016/j.jphotobiol.2012.03.001. [DOI] [PubMed] [Google Scholar]
- 43.AlGhamdi KM, Kumar A, Moussa NA. Low-level laser therapy: a useful technique for enhancing the proliferation of various cultured cells. Lasers Med Sci Springer. 2012;27:237–249. doi: 10.1007/s10103-011-0885-2. [DOI] [PubMed] [Google Scholar]
- 44.Whinfield AL, Aitkenhead I. The light revival: does phototherapy promote wound healing? A review foot Elsevier. 2009;19:117–124. doi: 10.1016/j.foot.2009.01.004. [DOI] [PubMed] [Google Scholar]
- 45.Zhao D, Luo S, Xu W, Hu J, Lin S, Wang N. Efficacy and safety of hyperbaric oxygen therapy used in patients with diabetic foot: a meta-analysis of randomized clinical trials. Clin Ther Elsevier. 2017;39:2088–2094. doi: 10.1016/j.clinthera.2017.08.014. [DOI] [PubMed] [Google Scholar]
- 46.Ontario HQ. Hyperbaric oxygen therapy for the treatment of diabetic foot ulcers: a health technology assessment. Ont Health Technol Assess Ser. Health Quality Ontario; 2017;17:1. [PMC free article] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The authors stated and declare that all data is exist and available.
The authors stated and declare that all code is exist and available.