

Abstract
Total hip arthroplasty is performed more frequently in younger patients nowadays, making long-term bone stock preservation an important topic. A mechanism for late implant failure is periprosthetic bone loss, caused by stress shielding around the hip stem due to different load distribution. Short stems are designed to keep the physical loading in the proximal part of the femur to reduce stress shielding. The aim of this review is to give more insight into how short and anatomic stems behave and whether they succeed in preservation of proximal bone stock.
A systematic literature search was performed to find all published studies on bone mineral density in short and anatomic hip stems. Results on periprosthetic femoral bone mineral density, measured with dual-energy X-ray absorptiometry (DEXA), were compiled and analysed per Gruen zone in percentual change.
A total of 29 studies were included. In short stems, Gruen 1 showed bone loss of 5% after one year (n = 855) and 5% after two years (n = 266). Gruen 7 showed bone loss of 10% after one year and –11% after two years. In anatomic stems, Gruen 1 showed bone loss of 8% after one year (n = 731) and 11% after two years (n = 227). Gruen 7 showed bone loss of 14% after one year and 15% after two years.
Short stems are capable of preserving proximal bone stock and have slightly less proximal bone loss in the first years, compared to anatomic stems.
Cite this article: EFORT Open Rev 2021;6:1040-1051. DOI: 10.1302/2058-5241.6.210030
Keywords: anatomic stem, bone mineral density, bone stock loss, DEXA, periprosthetic bone loss, short stem, total hip arthroplasty
Introduction
Nowadays, there is a higher incidence of younger and more active patients undergoing total hip arthroplasty (THA). In the Netherlands, between 17% and 19% of the patients receiving total hip arthroplasty are younger than 60 years.1,2 Their biomechanical forces on the hip implant are higher compared to the more elderly with THA, increasing the long-term failure rate of hip implants.3–6 Failure of hip implants can be caused by periprosthetic bone loss, leading to aseptic loosening or periprosthetic fractures. Stress shielding is one of the reasons for periprosthetic bone loss in cementless total hip arthroplasty,7,8 as bone resorption occurs through changed physical loading in the femur.9,10 Loss of bone stock can compromise the stability of hip stems,11 emphasizing the importance of bone stock preservation around hip stems. Physical loading in most conventional hip stems is transferred from the proximal region of the femur to the femur shaft, decreasing bone mass around the greater trochanter and calcar region.12,13
Other types of implants, such as short and anatomical stem designs, are based on a more proximal anchoring principle. Short stems in total hip arthroplasty were designed to restrict the physical loading to the proximal part of the femur, thereby reducing periprosthetic bone loss.14 However, there are a lot of designs with different implant characteristics. A clear definition of a short stem still lacks. A classification based on the osteotomy level is currently used,15 but neglects the anchoring principle of the stem. Hip stems that are classified as short do not necessarily yield better proximal bone stock preservation compared to anatomical or conventional hip stems.
Dual-energy X-ray absorptiometry (DEXA) is a reliable and widely accepted tool to determine bone mineral density (BMD).16–18 Measuring BMD around the total hip prosthesis provides information on the redistribution of the biomechanical forces in the femur as a result of implanted hip stems.19 A review by Knutsen et al13 gave insight into stress shielding around cemented and uncemented conventional hip stems, as all available data on bone remodelling were pooled. For uncemented conventional stems, the area of the greater trochanter and calcar region are most prone to bone loss. Results of proximal bone stock preservation for different types of short and anatomic stems have been published in recent years, with diverse outcomes, but there are no global data on their outcome. In this review, short-term results on BMD surrounding short stems were assessed in comparison with anatomic stems.
Methods
Inclusion criteria
Studies
A systematic literature search was performed to obtain all published data on bone mineral density (BMD) in total hip arthroplasty. Inclusion was limited to studies on BMD measurements surrounding proximal anchored femoral hip stems, with a follow-up period of at least one year after surgery. Studies on hip resurfacing and conventional hip stems were excluded. Prospective and retrospective cohorts, as well as comparative studies, were included.
Outcome measurement
Primary outcome was BMD loss in Gruen zone 1 (calcar region) and Gruen zone 7 (greater trochanter),20 representing proximal loading zones, as these zones can be compared per different stem design. The outcome was described as the relative percentual change in BMD per follow-up moment relative to baseline. Baseline value was defined as the direct postoperative BMD (< 3 weeks). Data on BMD were collected for all Gruen zones (as mean BMD g/cm2 or percentual change in BMD, with or without standard deviation). The studies that presented their data in mg/cm2 or g/cm2 were converted into percentual change of baseline BMD in each Gruen zone.
Gruen zones are defined areas around the hip stem to assess osteolysis. Originally, they were divided into seven zones for conventional stems, but are also appliable for short stems (Fig. 1). Gruen 1 begins on the proximal lateral side (greater trochanter) and Gruen 7 ends on the proximal medial side (calcar region). If studies used a different Gruen zone numbering, this was converted to the zones as depicted in Fig. 1.
Fig. 1.
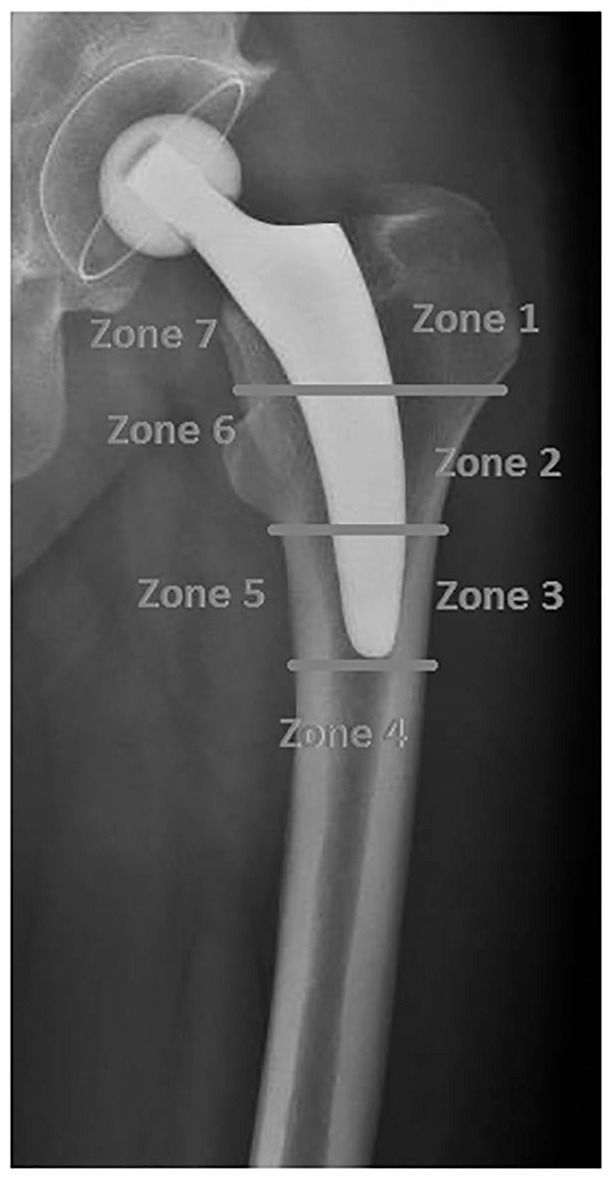
Gruen zones in short hip stems.
Search strategy
To identify all suitable studies, the following search terms were used in Medline, PubMed and Embase: “hip arthroplasty OR hip replacement” and “short stem OR anatomic stem” and “dual-energy OR DEXA” between January 1990 and June 2020. More details of the search can be requested from the authors. The search was performed by two reviewers (PV and DH), independently. Language was restricted to English, German, French and Spanish. References of retrieved studies, potentially meeting the criteria, were also screened. Abstracts from congress, scientific meetings and unpublished reports were excluded.
Methods of review
Selection of studies
Studies were selected by reviewing the title and abstract to identify potentially relevant articles by two reviewers (PV and DH). Disagreement was resolved through discussion by the two reviewers, with a third reviewer (SW) as final vote with remaining discussions. The full text was retrieved and evaluated for definitive inclusion, when the title, keywords or abstract showed information on bone mineral density or DEXA in total hip arthroplasty.
Data extraction
Two authors (SW and JV) independently performed the data extraction. Predefined extraction forms were used to collect the following data from each study: author, year of publication, type of implant, manufacturer, whether the implant is still on the market, number of patients/hips, years of follow-up, and the patient demographics (such as age, gender and BMI). BMD data were collected in mg/cm2, g/cm2 or percentual change of BMD at baseline, all with the standard deviation if described. When available, additional Harris Hip Scores (HHS) were collected. In case of non-numerical presentation of BMD, the authors were contacted to retrieve numerical data.
All hip implants were defined as either short or anatomical hip stems. According to the classification system as used by van Oldenrijk et al21 and described by Falez et al,15 the short stems were classified as partial collum or trochanter sparing, and the anatomic stems as trochanter sparing or trochanter harming. Additionally, all stem types were categorized based on anchoring site as metaphyseal, metadiaphyseal or diaphyseal anchoring.22 Follow-up was categorized as 1–3 months, six months, one year, two years, 3–5 years and 5–10 years.
Methodological quality
Methodological quality was assessed by use of the Methodological Index for Non-Randomized Studies (MINORS) criteria for quality assessment of the studies23 by two authors (SW and PV) independently. Discrepancies were resolved by consensus.
Analysis
Descriptive statistics were used to present study details. BMD data were converted into overall weighted mean of bone loss, expressed in percentages, for short and anatomic stems. The standard error (SE) was calculated using the pooled standard deviations in percentages. A threshold of ten percent was defined by the authors as the clinically relevant cut-off value for bone loss in the proximal Gruen zones (G1 and G7); however, there is no known threshold. The review of Knutsen et al showed in different types of conventional hip stems a wide range of percentual bone loss, where after two years in non-cemented femoral stems there was bone loss of at least 10%. A hip stem was classified as bone stock preserving in case the bone loss was less than this threshold. Additionally, all short stems that are still on the market were selected and their course of bone loss during a two-year follow-up period was investigated.
Results
Selection procedure
In total, 681 references were found in the online databases, all published between January 1997 and June 2020. After removal, a total of 470 articles remained for reviewing titles, abstracts and keywords. Finally, 29 studies were included in this review (Fig. 2).
Fig. 2.

Flowchart with selection of included studies.
Note. BMD, bone mineral density; DEXA, dual-energy X-ray absorptiometry; CT, computerized tomography; FU, follow-up.
Study characteristics
The 29 included studies contained a total of 2095 patients (2265 hips). Details of the included studies are presented in Table 1. The population consisted of 56% male and 44% female patients, with an average age of 55 years (range, 17–83 years) and a mean body mass index (BMI) of 28.4 (range, 16.9–49.6). Eighteen different stem designs were found, of which nine were short stems and nine anatomic stems (Table 2). According to the level of osteotomy, the stems were classified as trochanter harming (seven stems),24–30 trochanter sparing (seven stems)25,26,31–40 and partial collum (four stems).41–50According to site of anchoring, the stems were classified as metaphyseal (three stems),25,26,36,41,43,44,46,47 metadiaphyseal (seven stems)24,26,37–42,45,48,51 or diaphyseal (eight stems)25,27–30,33–36,52 anchoring. After patients who were lost to follow-up were excluded, 1796 hips remained to analyse. All included hip stems with their respective bone loss are depicted in Table 2. The bone loss in short and anatomic stems at one year follow-up is comparable in Gruen 7; however, there appears to be a difference in Gruen 1 at two-year follow-up (Fig. 3). The bone loss in all Gruen zones stabilized after three months, except for Gruen 7 which displayed a continuous bone loss until six months in the anatomic stems (Table 3).
Table 1.
Summary of included studies
| Author, year | Patients/hips (n) | Age (mean) | M/F (n) |
Body mass index (mean) | Follow-up (years) | Design | MINORS |
|---|---|---|---|---|---|---|---|
| Arabmotlag, 200352 | 15/15 | 48 | 7/8 | – | 2 | CTX | 17/22 |
| Boller, 201950 | 39/39 | 51 | 13/26 | 28 | 2 | Metha | 12/16 |
| 28/28 | 66 | 16/12 | 27 | 2 | Metha | ||
| Brinkmann, 201541 | 24/24 | 59 | 12/12 | 27 | 1 | Metha | 16/22 |
| 26/26 | 60 | 16/10 | 27 | Nanos | |||
| Ercan, 201642 | 62/62 | 57 | 28/34 | 29 | 1 | Minihip | 10/16 |
| Fokter, 201524 | 19/19 | 60 | 8/11 | 28 | 1 | Unibionix | 16/22 |
| Freitag, 201633 | 57/57 | 57 | 36/21 | 30 | 1 | Fitmore | 19/22 |
| Gasbarra, 201434 | 33/33 | 62 | 15/18 | 24 | 1 | Fitmore | 16/22 |
| Hayashi, 201670 | 21/21 | 68 | 11/56 | 23 | 2 | Trilock | 12/16 |
| Jahnke, 201443 | 40/40 | 55 | 20/20 | 27 | 1 | Metha | 13/16 |
| Kim, 201125 | 50/60 | 54 | 22/28 | 26 | 3 | Proxima | 16/22 |
| 50/60 | 52 | 24/26 | 25 | Profile | |||
| Kim, 201626 | 201/221 | 53 | 118/83 | 30 | 10 | Proxima | 19/22 |
| 400/530 | 53 | 264/136 | 29 | IPS | |||
| Kim, 201636 | 200/200 | 53 | 138/62 | 30 | 12 | Proxima | 19/22 |
| 200/200 | 53 | 138/62 | 30 | Profile | |||
| Leali, 200427 | 10/10 | 65 | 4/6 | – | 3 | Revelation | 10/16 |
| Lerch, 201244 | 25/25 | 59 | 16/9 | 25 | 2 | Metha | 13/16 |
| Meyer, 201932* | 54/54 | – | – | – | 5 | Fitmore | – |
| Nysted, 201151 | 43/43 | 55 | 18/28 | – | 5 | Unique | 16/22 |
| 35/35 | 53 | 13/28 | – | ABG-I | |||
| Panisello, 200937 | 56/56 | 60 | 27/29 | 28 | 5 | ABG-I | 19/22 |
| 54/54 | 59 | 26/28 | 27 | ABG-II | |||
| Parchi, 201749 | 20/20 | 54 | 11/9 | – | 4 | Metha | 12/16 |
| Rahmy, 200438 | 24/24 | 62 | 11/18 | 28 | 3 | ABG-I | 18/22 |
| Salemyr, 201531 | 26/26 | 62 | 11/15 | 27 | 4 | Proxima | 21/22 |
| Shafy, 201645 | 26/26 | 43 | 20/6 | 27 | 2 | Minihip | 12/16 |
| Sluimer, 200628 | 40/40 | 53 | 15/25 | – | 2 | Omnifit-HA 1090 | 18/22 |
| Steens, 201546 | 20/20 | 49 | 12/8 | 26 | 5 | ESKA cut 2000 | 14/16 |
| Synder, 201547 | 36/36 | 50 | 18/18 | – | 1 | Metha | 12/16 |
| Vd Wal, 200640 | 25/25 | 62 | 17/8 | – | 2 | ABG-I | 16/22 |
| 26/26 | 60 | 12/14 | – | 2 | ABG-II | ||
| Vd Wal, 200839 | 24/24 | 60 | 11/13 | – | 2 | ABG-I | 15/22 |
| White, 200829 | 27/27 | 37 | 14/13 | 25 | 5 | Epoch | 9/16 |
| Wixson, 199730 | 35/35 | 50 | 16/19 | – | 2 | Custom made | 9/16 |
| Zeh, 201348 | 25/25 | 60 | 15/10 | 29 | 1 | Nanos | 11/16 |
Note. MINORS, Methodological Index for Non-Randomized Studies.
*Study between two age groups.
**follow-up of Freitag et al, 201633.
Table 2.
Classification and course of bone loss per hip stem design from baseline in Gruen 1 and 7 (in %)
| Gruen 1 | Type | Osteotomy | Anchoring | Studies (n) | N | 3M | 6M | 1Y | 2Y |
|---|---|---|---|---|---|---|---|---|---|
| ABG-I35–38,51 | Anatomic | Trochanter sparing | Metadiaphyseal | 5 | 164 | –11 | –11 | –13 | –12 |
| ABG-II35,38 | Anatomic | Trochanter sparing | Metadiaphyseal | 2 | 80 | –5 | –7 | –8 | –9 |
| Custom made Biomet30 | Anatomic | Trochanter harming | Diaphyseal | 1 | 31 | –10 | –17 | –8 | |
| CTX52 | Anatomic | Trochanter sparing | Diaphyseal | 1 | 15 | –2 | |||
| Epoch29 | Anatomic | Trochanter harming | Diaphyseal | 1 | 12 | –17 | –19 | ||
| ESKA cut 200046 | Short | Partial collum | Metaphyseal | 1 | 30 | –3 | –1 | ||
| Fitmore31,32,40 | Short | Trochanter sparing | Diaphyseal | 3 | 90* | –3 | 0 | –4 | |
| IPS33 | Anatomic | Trochanter harming | Metadiaphyseal | 1 | 385 | 0 | |||
| Metha41,43,44,47,49, 50 | Short | Partial collum | Metaphyseal | 6 | 206 | –9 | –9 | –8 | –5 |
| Minihip42,45 | Short | Partial collum | Metadiaphyseal | 2 | 88 | –11 | –12 | –8 | –3 |
| Nanos41,48 | Short | Partial collum | Metadiaphyseal | 2 | 51 | –9 | –14 | ||
| Omnifit-HA 109028 | Anatomic | Trochanter harming | Diaphyseal | 1 | 35 | –11 | –13 | –14 | –13 |
| Profile25,26 | Anatomic | Trochanter harming | Diaphyseal | 2 | 60 | –27 | |||
| Proxima25,26,34, 39 | Short | Trochanter sparing | Metaphyseal | 4 | 333 | –6 | –3 | –1 | –3 |
| Revelation27 | Anatomic | Trochanter harming | Diaphyseal | 1 | 10 | –1 | –2 | –4 | |
| Trilock33 | Short | Trochanter sparing | Diaphyseal | 1 | 65 | –6 | –5 | –3 | |
| Unibionix24 | Short | Trochanter harming | Metadiaphyseal | 1 | 19 | 0 | 5 | 10 | |
| Unique51 | Short | Trochanter sparing | Metadiaphyseal | 1 | 43 | –10 | –9 | –10 | –11 |
| Gruen 7 | Type | Osteotomy | Anchoring | Studies (n) | N | 3M | 6M | 1Y | 2Y |
| ABG-I 35–38,51 | Anatomic | Trochanter sparing | Metadiaphyseal | 5 | 164 | –12 | –22 | –23 | –15 |
| ABG-II35,38 | Anatomic | Trochanter sparing | Metadiaphyseal | 2 | 80 | –5 | –10 | –16 | –12 |
| Custom made Biomet30 | Anatomic | Trochanter harming | Diaphyseal | 1 | 31 | –17 | –19 | 15 | |
| CTX52 | Anatomic | Trochanter sparing | Diaphyseal | 1 | 15 | –34 | |||
| Epoch29 | Anatomic | Trochanter harming | Diaphyseal | 1 | 12 | –10 | –12 | ||
| ESKA cut 200046 | Short | Partial collum | Metaphyseal | 1 | 30 | –3 | 1 | ||
| Fitmore31,32,40 | Short | Trochanter sparing | Diaphyseal | 3 | 90* | –14 | –6 | –8 | |
| IPS33 | Anatomic | Trochanter harming | Metadiaphyseal | 1 | 385 | –6 | |||
| Metha41,43,44,47,49, 50 | Short | Partial collum | Metaphyseal | 6 | 206 | –15 | –11 | –13 | –3 |
| Minihip42,45 | Short | Partial collum | Metadiaphyseal | 2 | 88 | –11 | –12 | –9 | –3 |
| Nanos41,48 | Short | Partial collum | Metadiaphyseal | 2 | 51 | –9 | –8 | ||
| Omnifit-HA 109028 | Anatomic | Trochanter harming | Diaphyseal | 1 | 35 | –11 | –13 | –14 | –13 |
| Profile25,26 | Anatomic | Trochanter harming | Diaphyseal | 2 | 60 | –33 | |||
| Proxima25,26,34,39 | Short | Trochanter sparing | Metaphyseal | 4 | 333 | –11 | –12 | –7 | –13 |
| Revelation27 | Anatomic | Trochanter harming | Diaphyseal | 1 | 10 | –4 | –5 | –5 | |
| Trilock33 | Short | Trochanter sparing | Diaphyseal | 1 | 65 | –9 | –9 | –14 | |
| Unibionix24 | Short | Trochanter harming | Metadiaphyseal | 1 | 19 | –12 | –12 | –15 | |
| Unique51 | Short | Trochanter sparing | Metadiaphyseal | 1 | 43 | –17 | –20 | –21 | –24 |
Fig. 3.

Percentual bone loss per type of hip stem in Gruen 1 and 7, with pooled standard error.
Note. BMD, bone mineral density.
Table 3.
Mean percentual change in bone mineral density in short and anatomic stems as a proportion from baseline (< 3 weeks postoperative)
| Short | Time (months) | 3 | 6 | 12 | 24 | 36–60 | 60–120 |
|---|---|---|---|---|---|---|---|
| Nr of hips (G1, G7) | 397 (12) | 456 (12) | 855 (18) | 266 (7) | 335 (4) | 221 (3) | |
| Nr of hips (G2–G6) | 371 (11) | 430 (11) | 582 (16) | 240 (6) | 117 (3) | 63 (2) | |
| Gruen 1 | –7 | –8 | –5 | –5 | 1 | –2 | |
| Gruen 2 | –7 | –5 | –4 | –1 | –9 | –7 | |
| Gruen 3 | –1 | –1 | 0 | 1 | –2 | –4 | |
| Gruen 4 | –4 | –4 | –2 | –1 | –5 | –6 | |
| Gruen 5 | –3 | –2 | –2 | 0 | 0 | –3 | |
| Gruen 6 | –5 | –1 | 1 | 2 | –4 | 0 | |
| Gruen 7 | –12 | –11 | –10 | –11 | –13 | –15 | |
| Anatomic | Time (months) | 3 | 6 | 12 | 24 | 36–60 | 60–120 |
| Nr of hips (G1, G7) | 155 (5) | 245 (6) | 731 (9) | 227 (8) | 504 (4) | 631 (5) | |
| Nr of hips (G2–G6) | 155 (5) | 245 (6) | 257 (7) | 227 (8) | 59 (2) | 157 (3) | |
| Gruen 1 | –9 | –10 | –8 | –11 | –13 | –2 | |
| Gruen 2 | –7 | –4 | –5 | –6 | –7 | 4 | |
| Gruen 3 | –5 | –4 | –2 | –2 | –5 | –1 | |
| Gruen 4 | –4 | –5 | –1 | –1 | –2 | –1 | |
| Gruen 5 | –4 | –1 | –2 | –1 | –1 | 3 | |
| Gruen 6 | –6 | –4 | –4 | –3 | –5 | 3 | |
| Gruen 7 | –10 | –17 | –14 | –15 | –13 | –25 |
Between brackets number of studies.
Short stem
A total number of 1068 patients (1098 hips) were included in 19 studies (not including Meyer et al,32 of whom 53.7% were male (n = 574/1068) and 46.3% were female (n = 494/1068). The average age was 55 years with a mean BMI of 25. Once patients who were lost to follow-up were excluded, a total of 915 hips remained. A mean total value in HHS of 94 at a minimal follow-up of one year (range, 1–10 years) was reported.
Gruen 1 showed a bone loss of 5% after one year (n = 855) and 5% after two years (n = 266). Gruen 7 was the most affected zone, with a bone loss of 10% after one year and 11% after two years (Table 3).
Anatomic stem
A total of 1027 patients (1167 hips) were included in 13 studies, of whom 56% were male (n = 597/1027) and 44% female (n = 430/1027). In this population, the mean age was 54 years with a mean BMI of 23. Lost to follow-up patients were excluded, leaving a total of 881 hips in this subgroup. The HHS had a mean total value of 96 points at a minimal follow-up of one year (range, 1–10 years).
Gruen 1 showed bone loss of 8% after one year (n = 731) and 11% after two years (n = 227). Bone loss in Gruen 7 was 14% after one year and 15% after two years (Table 3).
Osteotomy levels (Fig. 4)
Fig. 4.

Percentual bone loss in type of osteotomy in Gruen 1 and 7 (short and anatomic), with pooled standard error.
Note. BMD, bone mineral density.
Bone loss in Gruen 1 was, in both trochanter sparing and partial collum hip stems, less than 10%, with a slightly better preservation in trochanter sparing hip stems at one year follow-up. This was not seen at two-year follow-up. A difference of > 10% bone loss was found at two-year follow-up between trochanter sparing and partial collum hip stems in Gruen 7.
In anatomic stems, the trochanter harming stems were bone stock preserving at one-year follow-up in Gruen 1, but this preservation was not seen at two-year follow-up. There is a difference between trochanter sparing stems in short and anatomic stems, in favour of the short stems.
Anchoring types (Fig. 5)
Fig. 5.

Percentual bone loss in type of anchoring in Gruen 1 and 7 (short and anatomic), with pooled standard error.
Note. BMD, bone mineral density.
In short stems, metaphyseal anchoring was bone stock preserving in the two Gruen zones at one- and two-year follow-up. Metadiaphyseal anchoring also achieves this in Gruen 1, but not in Gruen 7. Comparing metadiaphyseal short stems and anatomic stems, both stems had equal bone loss in Gruen 1 and 7.
Short stem types (Fig. 6)
Fig. 6.

Bone loss in % per short stem design (still on the market) in Gruen 1 and 7 over time, with the total mean per stem included. Threshold of 10% bone loss added.
Note. BMD, bone mineral density.
The progress of the different types of short stems that are still on the market in Gruen 1 and Gruen 7 over time varies. The total mean percentual changes in BMD of the short and anatomic stems were included as reference line, with the threshold of 10%.
At two years follow-up, the Metha (Braun, Hessen, Germany), Fitmore (ZimmerBiomet, Warsaw, USA) and Minihip (Corin group PLC, Circencester, United Kingdom) were bone stock preserving in Gruen 1 and 7. The Trilock (DePuy, Warsaw, IN) was bone stock preserving in Gruen 1,but this was not achieved in Gruen 7. The Nanos (Smith & Nephew, Marl, Germany) is bone stock preserving in Gruen 7 at one-year follow-up, but did have more than 10% bone loss in Gruen 1.
Discussion
This review compiled the available data on periprosthetic bone loss in short and anatomic hip stems and defined which type of stem is best capable of preserving bone stock. Overall one-year follow-up results revealed that short and anatomic stems are bone stock preserving in Gruen 1. Furthermore, only the short stem was bone stock preserving in Gruen 7 at one-year follow-up. In the rest of the follow-up moments, in both short and anatomic stems, there was more than 10% bone loss. Bone stock was preserved in the remaining Gruen zones in short and anatomic stems.
This review was restricted to short stems and anatomic stems; hip resurfacing stems were not included due to different physical loading and anchoring principles. Uncemented conventional hip stems were covered in the review by Knutsen et al.13 All measurements were obtained with DEXA scans, a widely used and reliable technique for measurement of periprosthetic bone loss.17,53 The focus of interest in this review were Gruen 1and 7, as these two zones are most representative for proximal loading of the femur and where periprosthetic bone loss is mainly observed.13,54,55 These two zones are also the most comparable between different stem designs, as stem length defines the length of the Gruen zone for Gruen 2 until Gruen 6, but is less important for Gruen 7 (the calcar/lesser trochanter region) and Gruen 1 (greater trochanter region).
By maintaining a greater part of the postoperative physical loading in the metaphysis, the trochanter region has less bone stock loss in short (-5%) and anatomic (-8%) stems one-year postoperatively than uncemented conventional stems (–9.8%), as shown in the review by Knutsen et al.13 In the calcar region it is more difficult to preserve bone stock in uncemented conventional stems (–19%).13 Short stems (-10%) show better bone stock preservation one year after implantation compared to uncemented conventional stems. The more proximal anchoring anatomic stems (-14%) also provide a smaller amount of bone loss than uncemented conventional stems in the calcar region.
The present study had some limitations. This review has focused only on the classification of the hip stem, thereby neglecting implant-specific characteristics such as geometry, coating, stiffness and material that are also associated with BMD.13 The IPS (anatomic) and Unibionix stem (short) both show remarkable bone stock preservation in Gruen 1, the Unique stem (short) displays bone loss of more than 20% in Gruen 7 and the Profile stem (anatomic) has bone loss of more than 20% in both Gruen zones. These results are not in line with other results of the same type of hip stems in their category, indicating that other implant-specific characteristics play an important role. Unfortunately, stem positioning and osteotomy level were not mentioned in most studies, therefore their effect on BMD could not be assessed in this review. But it could be an explanation between two different results in the same type of hip stem (Metha), where one study describes bone loss of 23% in Gruen 7 and another 8%. A study by Brinkmann et al56 showed a different straining distribution in stems which were placed in a varus or valgus alignment.
Most studies reported data on BMD direct postoperatively in both Gruen zones 1 and 7; however, 19 studies did not. They compared follow-up BMD to the preoperative BMD (n = 5), the BMD of the contralateral side (n = 3), the BMD value without Gruen zones (n = 4) or made no comparison at all (n = 7). Therefore, these studies were excluded from this review. A threshold of 10% bone loss was chosen as clinically relevant in this review as reference value for all short hip stems, thereby making a stem bone stock preserving when it shows less than 10% bone loss. However, there is no known threshold for how much bone loss is of clinical significance for implant failure. Long-term survival in hip stems can be affected by bone loss in Gruen 1 and 7, but in case of sufficient anchoring in the other (more distal) Gruen zones, implant stability can be maintained. As conventional stems have a higher percentage of bone loss, most stems also have excellent long-term survival, as seen with the 13A Orthopaedic Data Evaluation Panel (ODEP) rating for the CLS and Exeter for example. However, if the femoral component fails in the long term due to aseptic loosening, this is often accompanied with (proximal) bone stock loss and mostly seen in Gruen 1 and Gruen 7. As revision surgery in total hip arthroplasty is rising, due to a higher incidence of younger and more active patients with total hip arthroplasty,57–61 this loss can pose more difficulty during revision surgery62 and influence the type of hip stem as femoral replacement.63 The chance of complications, such as fractures, and the difficulty of the revision is theoretical lower when there is still sufficient bone stock.64 Especially in patients who have a chance of re-revision in THA, maintaining bone stock seems to play an important role.65
The majority of the studies concerned follow-up data limited to the first postoperative year. Since bone activity is a continuous process, medium- and long-term bone remodelling is important for better understanding of the effect that short stems have on the physical loading.26,66,67 Especially since the patient population is in a stage of life where bone stock will naturally decline due to age, reduced activity and hormonal shifts.68 Nevertheless, the promising course of bone remodelling in this review around the short stem during the first two postoperative years could yield information on bone stock preservation in the long term.12,69
Both classification systems based on osteotomy level as well as anchoring site revealed varying amounts of bone loss within their classification among short and anatomical stems. This could indicate that positioning of the stem can play a role in bone remodelling.56,70 For instance, the Nanos stem can be placed in a varus or valgus position, depending on the hip anatomy of the individual patient in terms of the femoral offset. Osteotomy level can therefore be either partial collum or trochanter sparing while maintaining the anchoring site. Classification on just osteotomy level could not be accurate enough. Therefore, classification according to type of anchoring should be described in further research when describing the effect of the hip stem on femoral bone loss.
Conclusion
This study contributes to the understanding of periprosthetic bone mineral density in short stem hip arthroplasty. Short stems are capable of preserving bone stock by maintaining the postoperative physical loading in the metaphysis. Though there is still loss of bone, this is slightly reduced in short stems compared to anatomic stems. Whether this effect is clinically relevant and remains in the long term is yet to be established.
Footnotes
ICMJE Conflict of interest statement: The author declares no conflict of interest relevant to this work.
Social media: [Twitter: SheryldeWaard, Linkedin: Sheryl de Waard]
OA licence text: This article is distributed under the terms of the Creative Commons Attribution-Non Commercial 4.0 International (CC BY-NC 4.0) licence (https://creativecommons.org/licenses/by-nc/4.0/) which permits non-commercial use, reproduction and distribution of the work without further permission provided the original work is attributed.
Funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
References
- 1. Arthroplasty in the Picture Annual Report of the Dutch Arthroplasty Register (Landelijke Registratie Orthopedische Implantaten) 2014. www.lroi-rapportage.nl (date last accessed 21 October 2021).
- 2. Landelijke Registratie Orthopedische Implantaten (LROI) ©2016 Online LROI-Rapportage 2015. www.lroi-rapportage.nl (date last accessed 21 October 2021).
- 3. Swarup I, Marshall AC, Lee YY, Figgie MP. Implant survival and patient-reported outcomes after total hip arthroplasty in young patients with developmental dysplasia of the hip. Hip Int 2017;26:367–373. [DOI] [PubMed] [Google Scholar]
- 4. Swarup I, Sutherland R, Jayme C, Burket JC, Figgie MP. Total hip arthroplasty in young patients with post-traumatic arthritis of the hip. Hip Int 2017;27:546–550. [DOI] [PubMed] [Google Scholar]
- 5. Swarup I, Shields M, Mayer EN, Hendow CJ, Burket JC, Figgie MP. Outcomes after total hip arthroplasty in young patients with osteonecrosis of the hip. Hip Int 2017;27:286–292. [DOI] [PubMed] [Google Scholar]
- 6. Santaguida PL, Hawker GA, Hudak PL, Glazier R, Mahomed NN, et al. Patient characteristics affecting the prognosis of total hip and knee joint arthroplasty: a systematic review. Can J Surg 2008;51:428–436. [PMC free article] [PubMed] [Google Scholar]
- 7. Alm JJ, Mäkinen TJ, Lankinen P, Moritz N, Vahlberg T, Aro HT. Female patients with low systemic BMD are prone to bone loss in Gruen zone 7 after cementless total hip arthroplasty. Acta Orthop 2009;80:531–537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Sköldenberg OG, Bodén HSG, Salemyr MO, Ahl TE, Adolphson PY. Periprosthetic proximal bone loss after uncemented hip arthroplasty is related to stem size: DXA measurements in 138 patients followed for 2–7 years. Acta Orthop 2006;77:386–392. [DOI] [PubMed] [Google Scholar]
- 9. Rosenthall L, Bobyn JD, Tanzer M. Bone densitometry: influence of prosthetic design and hydroxyapatite coating on regional adaptive bone remodelling. Int Orthop 1999;23:325–329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Tanzer M, Kantor S, Rosenthall L, Bobyn JD. Femoral remodeling after porous-coated total hip arthroplasty with and without hydroxyapatite-tricalcium phosphate coating: a prospective randomized trial. J Arthroplasty 2001;16:552–558. [DOI] [PubMed] [Google Scholar]
- 11. Parchi PD, Cervi V, Piolanti N, et al. Densitometric evaluation of periprosthetic bone remodeling. Clin Cases Miner Bone Metab 2014;11:226–231. [PMC free article] [PubMed] [Google Scholar]
- 12. Roth A, Richartz G, Sander K, et al. Verlauf der periprothetischen Knochendichte nach Hüfttotalendoprothesenimplantation. Abhängigkeit von Prothesentyp und knöcherner Ausgangssituation. Orthopade 2005;34:334–344. [DOI] [PubMed] [Google Scholar]
- 13. Knutsen AR, Lau N, Longjohn DB, Ebramzadeh E, Sangiorgio SN. Periprosthetic femoral bone loss in total hip arthroplasty: systematic analysis of the effect of stem design. Hip Int 2017;27:26–34. [DOI] [PubMed] [Google Scholar]
- 14. Albanese CV, Santori FS, Pavan L, Learmonth ID, Passariello R. Periprosthetic DXA after total hip arthroplasty with short vs. ultra-short custom-made femoral stems: 37 patients followed for 3 years. Acta Orthop 2009;80:291–297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Falez F, Casella F, Papalia M. Current concepts, classification, and results in short stem hip arthroplasty. Orthopedics 2015;38:S6–S13. [DOI] [PubMed] [Google Scholar]
- 16. Cohen B, Rushton N. Accuracy of DEXA measurement of bone mineral density after total hip arthroplasty. J Bone Joint Surg [Br] 1995;77-B:479–483. [PubMed] [Google Scholar]
- 17. Bloebaum RD, Liau DW, Lester DK, Rosenbaum TG. Dual-energy X-ray absorptiometry measurement and accuracy of bone mineral after unilateral total hip arthroplasty. J Arthroplasty 2006;21:612–622. [DOI] [PubMed] [Google Scholar]
- 18. Martini F, Lebherz C, Mayer F, Leichtle U, Kremling E, Sell S. Precision of the measurements of periprosthetic bone mineral density in hips with a custom-made femoral stem. J Bone Joint Surg [Br] 2000;82-B:1065–1071. [DOI] [PubMed] [Google Scholar]
- 19. Kroger H, Miettinen H, Arnala I, Koski E, Rushton N, Suomalainen O.Evaluation of periprosthetic bone using dual-energy X-ray absorptiometry: precision of the method and effect of operation on bone mineral density. J Bone Miner Res 1996;11:1526–1530. [DOI] [PubMed] [Google Scholar]
- 20. Gruen T, McNeice G, Amstutz H. ‘Modes of failure’ of cemented stem-type femoral components: a radiographic analysis of loosening. Clin Orthop Relat Res 1979;141:17–27. [PubMed] [Google Scholar]
- 21. van Oldenrijk J, Molleman J, Klaver M, Poolman RW, Haverkamp D. Revision rate after short-stem total hip arthroplasty: a systematic review of 49 studies. Acta Orthop 2014;85:250–258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. McTighe T, Keggi J, David Stulberg S, Keppler L, Brazil D, McPherson EJ. Total hip stem classification system. Reconstr Rev 2014;4:24–28. [Google Scholar]
- 23. Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological Index for Non-Randomized Studies (MINORS): development and validation of a new instrument. ANZ J Surg 2003;73:712–716. [DOI] [PubMed] [Google Scholar]
- 24. Fokter SK, Sarler T, Strahovnik A, Repše-Fokter A. Results of total hip arthroplasty using a bionic hip stem. Int Orthop 2015;39:1065–1071. [DOI] [PubMed] [Google Scholar]
- 25. Kim YH, Choi Y, Kim JS. Comparison of bone mineral density changes around short, metaphyseal-fitting, and conventional cementless anatomical femoral components. J Arthroplasty 2011;26:931–940.e1. [DOI] [PubMed] [Google Scholar]
- 26. Kim YH, Park JW, Kim JS. Metaphyseal engaging short and ultra-short anatomic cementless stems in young and active patients. J Arthroplasty 2016;31:180–185. [DOI] [PubMed] [Google Scholar]
- 27. Leali A, Fetto JF. Preservation of femoral bone mass after total hip replacements with a lateral flare stem. Int Orthop 2004;28:151–154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Sluimer JC, Hoefnagels NHM, Emans PJ, Kuijer R, Geesink RGT. Comparison of two hydroxyapatite-coated femoral stems: clinical, functional, and bone densitometry evaluation of patients randomized to a regular or modified hydroxyapatite-coated stem aimed at proximal fixation. J Arthroplasty 2006;21:344–352. [DOI] [PubMed] [Google Scholar]
- 29. White SP, Lee MB, Galpin J, Learmonth ID. Ten-year results of a bone-preserving low-modulus composite total hip replacement stem. Hip Int 2008;18:81–87. [DOI] [PubMed] [Google Scholar]
- 30. Wixson RL, Stulberg SD, Van Flandern GJ, Puri L. Maintenance of proximal bone mass with an uncemented femoral stem analysis with dual-energy x-ray absorptiometry. J Arthroplasty 1997;12:365–372. [DOI] [PubMed] [Google Scholar]
- 31. Salemyr M, Muren O, Ahl T, et al. Lower periprosthetic bone loss and good fixation of an ultra-short stem compared to a conventional stem in uncemented total hip arthroplasty. Acta Orthop 2015;86:659–666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Meyer JS, Freitag T, Reichel H, Bieger R. Periprosthetic bone mineral density changes after implantation of a curved bone preserving hip stem compared to a standard length straight stem: 5-yr results of a prospective, randomized DXA-analysis. J Clin Densitom 2019;22:96–103. [DOI] [PubMed] [Google Scholar]
- 33. Freitag T, Hein MA, Wernerus D, Reichel H, Bieger R. Bone remodelling after femoral short stem implantation in total hip arthroplasty: 1-year results from a randomized DEXA study. Arch Orthop Trauma Surg 2016;136:125–130. [DOI] [PubMed] [Google Scholar]
- 34. Gasbarra E, Celi M, Perrone FL, et al. Osseointegration of Fitmore stem in total hip arthroplasty. J Clin Densitom 2014;17:307–313. [DOI] [PubMed] [Google Scholar]
- 35. Hayashi S, Nishiyama T, Fujishiro T, et al. Maintenance of periprosthetic bone mineral density with a cementless three dimensional straight tapered stem. Hip Int 2011;21:163–167. [DOI] [PubMed] [Google Scholar]
- 36. Kim YH, Park JW, Kim JS. Ultrashort versus conventional anatomic cementless femoral stems in the same patients younger than 55 years. Clin Orthop Relat Res 2016;474:2008–2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Panisello JJ, Canales V, Herrero L, Herrera A, Mateo J, Caballero MJ. Changes in periprosthetic bone remodelling after redesigning an anatomic cementless stem. Int Orthop 2009;33:373–379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Rahmy AIA, Gosens T, Blake GM, Tonino A, Fogelman I. Periprosthetic bone remodelling of two types of uncemented femoral implant with proximal hydroxyapatite coating: a 3-year follow-up study addressing the influence of prosthesis design and preoperative bone density on periprosthetic bone loss. Osteoporos Int 2004;15:281–289. [DOI] [PubMed] [Google Scholar]
- 39. van der Wal BCH, Rahmy AIA, Grimm B, Heyligers IC, Tonino AJ. Preoperative bone quality as a factor in dual-energy X-ray absorptiometry analysis comparing bone remodelling between two implant types. Int Orthop 2008;32:39–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. van der Wal BCH, Rahmy AIA, Grimm B, Blake GM, Heyligers IC, Tonino AJ. The influence of implant design on periprosthetic bone remodelling of two types hip stems. Hip Int 2006;16:8–17. [PubMed] [Google Scholar]
- 41. Brinkmann V, Radetzki F, Delank KS, Wohlrab D, Zeh A. A prospective randomized radiographic and dual-energy X-ray absorptiometric study of migration and bone remodeling after implantation of two modern short-stemmed femoral prostheses. J Orthop Traumatol 2015;16:237–243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Ercan A, Sokkar SM, Schmid G, Filler TJ, Abdelkafy A, Jerosch J. Periprosthetic bone density changes after MiniHip TM cementless femoral short stem: one-year results of dual-energy X-ray absorptiometry study. SICOT J 2016;2:40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Jahnke A, Engl S, Altmeyer C, et al. Changes of periprosthetic bone density after a cementless short hip stem: a clinical and radiological analysis. Int Orthop 2014;38:2045–2050. [DOI] [PubMed] [Google Scholar]
- 44. Lerch M, von der Haar-Tran A, Windhagen H, Behrens BA, Wefstaedt P, Stukenborg-Colsman CM. Bone remodelling around the Metha short stem in total hip arthroplasty: a prospective dual-energy X-ray absorptiometry study. Int Orthop 2012;36:533–538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Shafy TA, Sayed A, Abdelazeem AH. Study of the bone behavior around a neck preserving short stem implant: bone densitometric analysis over a span of two years. SICOT J 2016;2:31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Steens W, Boettner F, Bader R, Skripitz R, Schneeberger A. Bone mineral density after implantation of a femoral neck hip prosthesis: a prospective 5 year follow-up. BMC Musculoskelet Disord 2015;16:192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Synder M, Krajewski K, Sibinski M, Drobniewski M. Periprosthetic bone remodeling around short stem. Orthopedics 2015;38:S40–S45. [DOI] [PubMed] [Google Scholar]
- 48. Zeh A, Pankow F, Röllinhoff M, Delank S, Wohlrab D. A prospective dual-energy X-ray absorptiometry study of bone remodeling after implantation of the Nanos short-stemmed prosthesis. Acta Orthop Belg 2013;79:174–180. [PubMed] [Google Scholar]
- 49. Parchi PD, Ciapini G, Castellini I, Mannucci C, Nucci A-M, Piolanti N, Maffei S, Lisanti M. Evaluation of the effects of the Metha® short stem on periprosthetic bone remodelling in total hip arthroplasties: results at 48 months. Surg Technol Int 2017;30:346–351. [PubMed] [Google Scholar]
- 50. Boller S, Jahnke A, Augustin L, Ahmed G, Rickert M, Alexander B. Age-related osseointegration of a short hip stem: a clinical and radiological 24 months follow-up. Arch Orthop Trauma Surg 2019;139:405–410. [DOI] [PubMed] [Google Scholar]
- 51. Nysted M, Benum P, Klaksvik J, Foss O, Aamodt A. Periprosthetic bone loss after insertion of an uncemented, customized femoral stem and an uncemented anatomical stem: a randomized DXA study with 5-year follow-up. Acta Orthop 2011;82:410–416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Arabmotlagh M, Hennigs T, Rittmeister M. Femoral periprosthetic bone remodelling after implantation of custom made anatomic and standard straight stem hip prostheses. Z Orthop Ihre Grenzgeb 2003;141:519–525. [DOI] [PubMed] [Google Scholar]
- 53. Cohen B, Rushton N. Accuracy of DEXA measurement of bone mineral density after total hip arthroplasty. J Bone Joint Surg [Br] 1995;77-B:77–479. [PubMed] [Google Scholar]
- 54. Grochola LF, Habermann B, Mastrodomenico N, Kurth A. Comparison of periprosthetic bone remodelling after implantation of anatomic and straight stem prostheses in total hip arthroplasty. Arch Orthop Trauma Surg 2008;128:383–392. [DOI] [PubMed] [Google Scholar]
- 55. Boyle C, Kim IY. Comparison of different hip prosthesis shapes considering micro-level bone remodeling and stress-shielding criteria using three-dimensional design space topology optimization. J Biomech 2011;44:1722–1728. [DOI] [PubMed] [Google Scholar]
- 56. Brinkmann V, Radetzki F, Gutteck N, Delank S, Zeh A. Influence of varus/valgus positioning of the Nanos® and Metha® short-stemmed prostheses on stress shielding of metaphyseal bone. Acta Orthop Belg 2017;83:57–66. [PubMed] [Google Scholar]
- 57. Duncan CP, Masterson EL, Masri BA. Impaction allografting with cement for the management of femoral bone loss. Orthop Clin North Am 1998;29:297–305. [DOI] [PubMed] [Google Scholar]
- 58. Goff TAJ, Bobak P. Femoral impaction allografting for significant bone loss in revision hip arthroplasty. Hip Int 2017;27:281–285. [DOI] [PubMed] [Google Scholar]
- 59. Abdel MP, Roth PV, Harmsen WS, Berry DJ. What is the lifetime risk of revision for patients undergoing total hip arthroplasty? A 40-year observational study of patients treated with the Charnley cemented total hip arthroplasty. J Bone Joint Surg [Br] 2016;98-B:1436–1440. [DOI] [PubMed] [Google Scholar]
- 60. Cnudde PHJ, Nemes S, Bülow E, Timperley AJ, Whitehouse SL, Kärrholm J, et al. Risk of further surgery on the same or opposite side and mortality after primary total hip arthroplasty: a multi-state analysis of 133,654 patients from the Swedish Hip Arthroplasty Register. Acta Orthop 2018;89:386–393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Kärrholm J, Mohaddes M, Odin D, Vinblad J, Rogmark C, Rolfson O. Swedish Hip Arthroplasty Register annual report 2017. Gothenburg: Swedish Hip Arthroplasty Register, 2018. [Google Scholar]
- 62. DeRogatis MJ, Issack PS. Total femoral replacement as a salvage operation for the treatment of massive femoral bone loss during revision total hip arthroplasty. JBJS Rev 2018;6:e9. [DOI] [PubMed] [Google Scholar]
- 63. Sculco PK, Abdel MP, Lewallen DG. Management of femoral bone loss in revision total hip arthroplasty. Hip Int 2015;25:380–387. [DOI] [PubMed] [Google Scholar]
- 64. Glassman AH, Bobyn JD, Tanzer M. New femoral designs: do they influence stress shielding? Clin Orthop Relat Res 2006;453:64–74. [DOI] [PubMed] [Google Scholar]
- 65. Sheth NP, Melnic CM, Rozell JC, Paprosky WG. Management of severe femoral bone loss in revision total hip arthroplasty. Orthop Clin North Am 2015;46:329–342, ix. [DOI] [PubMed] [Google Scholar]
- 66. Götze C, Ehrenbrink J, Ehrenbrink H. Bleibt der Krafteinfluss der Kurzschaftprothese auf den methaphysären proximalen Femur begrenzt? Osteodensitometrische Analysen der NANOS®-Schaftendoprothese. Z Orthop Unfall 2010;148:398–405. [DOI] [PubMed] [Google Scholar]
- 67. Thorey F, Hoefer C, Abdi-Tabari N, Lerch M, Budde S, Windhagen H. Clinical results of the Metha short hip stem: a perspective for younger patients? Orthop Rev (Pavia) 2013;5:e34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. Boskey AL, Coleman R. Critical reviews in oral biology and medicine. J Dent Res 2010;89:1333–1348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Venesmaa PK, Ger HPJK, Miettinen HJA, Jurvelin JS, Suomalainen OT, Alhava EM. Monitoring of periprosthetic BMD after uncemented total hip arthroplasty with dual-energy X-ray absorptiometry: a 3-year follow-up study. J Bone Miner Res 2001;16:1056–1061. [DOI] [PubMed] [Google Scholar]
- 70. Hayashi S, Hashimoto S, Kanzaki N, Kuroda R, Kurosaka M. Stem anteversion affects periprosthetic bone mineral density after total hip arthroplasty. Hip Int 2016;26:260–264. [DOI] [PubMed] [Google Scholar]