

Abstract
Objective:
To investigate if there are any significant differences in the final inclination of the upper and lower anterior teeth of patients treated with a Roth or an MBT bracket prescription.
Materials and Methods:
Forty sets of posttreatment study models from patients treated using a preadjusted edgewise appliance (20 Roth and 20 MBT) were selected using predetermined inclusion and exclusion criteria. The models were masked and laser-scanned, and the final crown inclinations of UL1, UR3, and LR1 were assessed from the digital images. A two-way analysis of variance was undertaken with the dependent variable of final crown inclination and independent variables of bracket prescription (Roth or MBT) and tooth type.
Results:
There were no statistically significant differences in terms of the final inclination of the anterior teeth between the two bracket prescriptions (P = .132). Statistically significant differences were found between the final inclinations of different tooth types investigated (P < .001).
Conclusion:
In this group of selected patient records, the differences in torque values between the two bracket prescriptions did not lead to any real clinically detectable differences in the final inclination of teeth.
Keywords: Bracket prescription; MBT, Roth; Torque; Three-dimensional digital dental models
INTRODUCTION
The preadjusted edgewise Straight Wire Appliance was introduced in the 1970s.1 Since then, there have been many suggested modifications to the bracket prescriptions in terms of torque and tip values, often differing by only a few degrees. Differences in the torque prescription of the various preadjusted edgewise appliance systems are often the reason given for choosing one prescription over another. It is known that torque expression is affected by the amount of play between the archwire and the bracket slot2 and by variations in tooth anatomy,3–5 variations in bracket placement,3 inaccuracies in the bracket slot and archwire dimensions,6–8 mode of ligation of an archwire,7,9 and stiffness of the archwire.10
The MBT and Roth bracket prescriptions are the two commonly used preadjusted edgewise appliance systems in the United Kingdom. In the orthodontic literature, one previous study has compared the subjective outcome of the two appliances (MBT and Roth); the results of that study showed that the bracket prescription had no effect on the subjective esthetic judgments of posttreatment study models made by nine experienced orthodontists.11
Traditionally, incisor inclination has been assessed by lateral cephalometric radiograph; however, this technique is known to be less than ideal12 and has the disadvantage of subjecting the participant to ionizing radiation. A more recent method is using three-dimensional (3D) digital dental models obtained from laser scanning, which has been shown to be as reliable as cephalometric superimpositions for assessing orthodontic tooth movement.13,14
The aim of this study was to determine if there were any significant differences in the final crown inclination of the anterior teeth in patients treated with a Roth or an MBT bracket prescription. The null hypothesis tested was that there is no difference in the final crown inclination of the maxillary central incisor, maxillary canine, and mandibular central incisor between patients treated using a Roth or an MBT prescription.
MATERIAL AND METHODS
The project was registered with the Clinical Effectiveness Unit of the Sheffield Teaching Hospitals NHS Foundation Trust, which reviewed the protocol. The committee agreed that because the records included in the study were collected as a normal part of the patient's treatment and were fully anonymized, the project constituted a service evaluation and formal review by an ethics committee was not required.
Forty sets of posttreatment study models from patients treated using a preadjusted edgewise appliance (20 Roth and 20 MBT) were selected using predetermined inclusion and exclusion criteria. These patients were treated in the Orthodontic Department of the Charles Clifford Dental Hospital, Sheffield, UK. This was a convenience sample, chosen retrospectively, to represent a common type of orthodontic patient, treated to a good occlusal result, in a UK postgraduate teaching hospital.
The following inclusion criteria were applied:
Treated with upper and lower preadjusted edgewise appliances with a Roth (Ovation, Dentsplay GAC, Bohemia, NY) or an MBT prescription (Victory, 3M, St Paul, Minn)
Younger than 20 years of age at the start of treatment
Bilateral upper arch premolar extractions
A Peer Assessment Rating Index score of 5 or less from the posttreatment study models
A 0.019 × 0.025-inch stainless steel working archwire in a 0.022 × 0.028-inch bracket slot
An ANB angle between 1° and 5° inclusive.
The following exclusion criteria were applied:
A nonextraction approach
Extractions other than premolars
Functional appliance treatment
Headgear treatment
Orthognathic surgery
Several operators treated the patients, but the archwires were standardized within the department (Sentalloy and Neo-Sentalloy nickel-titanium aligning archwires, Dentsply GAC, and 0.019 × 0.025-inch stainless steel working archwires, DB Orthodontics, Silsden, West Yorkshire, UK). The torque values of MBT bracket prescription used were +17° for maxillary central incisors, −7° for maxillary canines, and −6° for mandibular incisors. The torque values of Roth bracket prescription used were +12° for maxillary central incisors, −2° for maxillary canines, and −1° for mandibular incisors.
Laser Scanning of Study Models and Torque Analysis on 3D Digital Image
The system used for this study was a 3D surface laser scanner (Vivid 910i, Konica Minolta Sensing, Tokyo, Japan) with a rotating stage, a tripod set, an exchangeable lens, a personal computer, and Rapidform 2006 software (INUS Technology Inc and Rapidform Inc, Seoul, South Korea). The reliability and accuracy of this equipment for orthodontic investigations has been tested in a previous study, which showed that the scanner was accurate to 0.023 mm for anteroposterior tooth movements and to 0.007 mm for buccopalatal movements.14 Although the present study did not measure anteroposterior or buccopalatal tooth movement, the repeatability of the point identification on digital dental models was the fundamental basis for the crown inclination analysis.
To conduct the laser scanning of dental study models and to analyze the crown inclination of the labial segment teeth, the following method was developed: The study models were placed at an angle of 45° to the horizontal on the rotating stage so that the laser beam hit the horizontal part of the hard palate at right angles. The model was then scanned and the surface was converted to a lattice of 300,000 connected points. The 3D image was captured by a computer and then viewed and manipulated using Rapidform 2006 software.
The faciolingual crown inclination. or “torque analysis.” was conducted on the 3D digital images for three labial segment teeth: maxillary left central incisor (UL1), maxillary right canine (UR3), and mandibular right central incisor (LR1). To analyze the crown inclination of the maxillary left central incisor, the following procedure was developed: The mesiobuccal cusp tip of both maxillary first molars and the midpoint of the incisal edge of the maxillary left central incisor were marked on the 3D digital image of a maxillary study model. The 3D digital images were manipulated by rotating or magnifying the image to improve point identification. The maxillary occlusal plane was drawn using the software (Figure 1). The midpoint of the facial axis of the clinical crown of the maxillary left central incisor was identified and marked on the digital dental model by the operator and a tangent plane to this point was drawn using the software (Figure 2). The software then calculated the angle formed between the tangent plane and a plane perpendicular to the maxillary occlusal plane. This angle signifies the faciolingual crown inclination of the tooth. The same procedure was conducted to determine the crown inclination of the maxillary right canine and the mandibular right central incisor.
Figure 1.
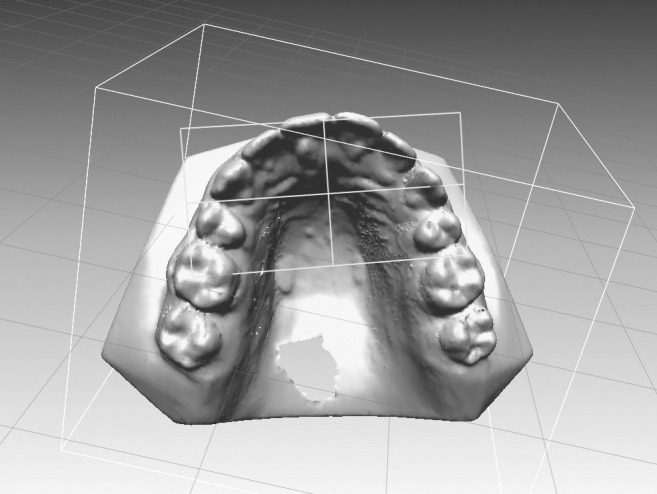
Three-dimensional image of a model with the occlusal plane marked.
Figure 2.

Tangent plane to the midpoint of the facial axis of clinical crown of the upper central incisor.
Reliability Test
To test the reliability of the laser scanning process and the crown inclination analysis method, 10 sets of study models (five from the Roth and five from the MBT group) were masked and the crown inclination values calculated for the three teeth under investigation. These study models were then re-masked, and the investigator repeated the whole process of laser scanning and crown inclination analysis after an interval of at least 3 weeks. For the main study, all the study models were masked, and the investigator was blinded to the prescription used for treating each patient.
Statistics
To test reliability, the data obtained were entered in the PASW Statistics for Windows version 18.0.0 (SPSS Inc, Chicago, Ill) and analyzed for any systematic error (paired t-test) or random error (intraclass correlation coefficient). Bland-Altman plots15 were also used to assess the limits of agreement between the crown inclination values measured on the two occasions. To test the null hypothesis that there was no difference in crown inclination between the patients treated using the two bracket prescriptions, the normality of the data distribution was first checked using the Shapiro-Wilk test. This was found to be normal; therefore, a two-way analysis of variance (ANOVA) test was conducted. The dependent variable was the inclination of the teeth measured using the 3D laser technique and the two independent variables were bracket prescription and tooth type. The significance level was set at P < .05.
RESULTS
The random error was low (intraclass correlation coefficient = 0.98). and there was no evidence of a systematic error (P = .66). The mean differences for all repeated measurements were less than 0.1°. An example of Bland-Altman plots for repeat readings of 20 sets of study models is shown in Figure 3, where the difference between the two readings has been plotted against the mean of the two readings.
Figure 3.

Bland and Altman plot for the upper central incisor.
Table 1 shows the descriptive statistics for the three teeth by bracket prescription. The Shapiro-Wilk test, used to test normality of distribution of data, showed the data to be normally distributed. This was also confirmed from Q-Q plots drawn for both MBT and Roth prescription data. The results of the two-way ANOVA tests (Table 2) showed that there was no statistically significant interaction between the bracket prescription and tooth type on the final crown inclination (P = .330) and no statistically significant difference in the final inclination of the teeth between the patients treated using MBT or Roth bracket prescriptions (P = .130); however, there was a statistically significant difference in the final inclination between different tooth types (P < .001).
Table 1.
Descriptive Statistics for the Three Tooth Type by Bracket Prescription

Table 2.
Two-Way Analysis of Variance Results

Table 6 shows the Tukey post hoc test results for the different tooth types. In terms of the torque expressed by the brackets for different tooth types, there was a statistically significant difference in the final crown inclination between the upper left central incisor and upper right canine (P < .001). There was also a statistically significant difference in the final crown inclination between the upper left central incisor and lower right central incisor (P < .001). There was no significant difference in the final crown inclination between the upper right canine and lower right central incisor (P = .160).
Table 3.
Tukey Post Hoc Testsa

DISCUSSION
This study found no significant difference between the MBT and Roth bracket prescriptions in terms of the final crown inclination of labial segment teeth of patients treated using these appliances. The results suggest a statistically significant difference in the final crown inclination between different tooth types, which is as we would expect, because the brackets for the three tooth types investigated here have different degrees of built-in labial and lingual torque. With regard to the faciolingual inclination of labial segment teeth, therefore, it appears that for treating patients with skeletal Class I and at least two premolar extractions, it does not matter whether a patient is treated with the MBT or Roth prescription as the stated difference in torque between the two bracket prescriptions does not seem to exist clinically.
This study is in agreement with the findings of Moesi et al.,11 who carried out a retrospective observational assessment to determine if using the MBT or Roth prescription has any effect on the subjective outcome of treatment, as judged by professionals. They showed that the ability to determine which bracket prescription has been used was no better than chance for most clinicians. In addition, Moesi et al.11 found that the choice of bracket prescription had no effect on the subjective esthetic judgments of posttreatment study models made by nine experienced orthodontists.
Germane et al.3 examined the facial surface contours of teeth and the effects of variations in facial surface on the faciolingual tooth angulation. These authors reported that the facial surface contours are not consistent among teeth of the same type between different persons, and this variability increases progressively between teeth from anterior to posterior in both arches. Additionally, van Loenan et al.5 reported that placing a bracket between 2 and 4.5 mm from the incisal edge of the maxillary central incisor and canine may result in an average torque expression difference of 10° at the end of treatment in the same patient using one type of bracket system. This was due to the variable labial crown morphology. These factors might have contributed to the wide range of standard deviations in expressed torque values noticed in the present study.
An additional source of loss of torque control is the forced relaxation of elastomeric ligatures. Elastomeric ligatures show a force degradation pattern characterized by an initial exponential decrease reaching 40% in the first 24 hours.16 The use of steel ligatures has been found to diminish slot-wire clearance, even with large dimensional slot-wire differences;17 however, the present study was a real-world study where steel ligatures were only used when absolutely required.
Torque expression is also affected by the stiffness of the archwire; stainless steel is known to have the largest torque expression, followed by TMA (titanium molybdenum alloy) and then nickel-titanium wire.10 The final working archwire used to treat patients in our study was a 0.019 × 0.025-inch stainless steel in a stainless steel bracket with a slot dimension of 0.022 × 0.028-inch. With this combination of bracket slot and archwire dimension, a theoretical torque loss of 10.5° has been reported.2 The results of theoretical torque loss, however, do not always represent the actual play between the slot and the wire. It is possible that if the patients had been treated with a full-sized 0.021 × 0.025-inch stainless steel or TMA archwire with a greater potential for full torque expression, differences between the two bracket prescriptions could have been detected; however, we wanted this study to be a real-world study, where we treated our patients as we routinely do in the clinic.
One criticism of this investigation is that no calculation was made to determine a suitable sample size needed to detect a clinically significant difference if one truly exists. This was not undertaken because there were no data upon which to base the calculation. It is, however, possible to carry out a post hoc power calculation based on the actual data from the study to determine what might be an appropriate sample size to detect a significant difference.
The largest mean difference in torque measurements between the MBT and Roth brackets was 3.6° for the upper left central incisor. The standard deviation of the differences can be estimated to be 11.3° ( ); therefore, the standardized difference (mean difference/standard deviation) can be calculated to be 0.32. Using the Altman nomogram18 it can be estimated that a sample size of 300 would be required to detect a significant difference with a power of 0.85 and significance level of .05. Using the nominal torque difference between the MBT and Roth brackets, a sample size of approximately 180 would be required to detect a significant difference of 5° with a power of 0.85 and significance level of .05.
); therefore, the standardized difference (mean difference/standard deviation) can be calculated to be 0.32. Using the Altman nomogram18 it can be estimated that a sample size of 300 would be required to detect a significant difference with a power of 0.85 and significance level of .05. Using the nominal torque difference between the MBT and Roth brackets, a sample size of approximately 180 would be required to detect a significant difference of 5° with a power of 0.85 and significance level of .05.
A further potential criticism of the study is that the patients were treated by different clinicians, although all were from one center, and therefore operator variability might have masked any differences between the two prescriptions; however, an original objective of the preadjusted edgewise appliance was to reduce the amount of wire bending required and promote more consistent treatment outcomes both within and between individual operators.
Overall, bearing in mind the limitations of this study, the results raise the question whether there is actually a need for having various preadjusted appliance systems with only a few degrees of difference between the prescriptions.
CONCLUSIONS
The results of this study show that there is insufficient evidence to reject the null hypothesis and it can therefore be concluded that, in our selected sample of patients:
There is no difference in the final inclinations of the upper central incisor, lower central incisor, and upper canine in patients treated with either the MBT or Roth prescription preadjusted edgewise appliances.
ACKNOWLEDGMENT
We would like to thank Miss Zoe Rusk, information analyst at the Royal Derby Hospital, for her help with the statistical tests.
REFERENCES
- 1.Andrews LF. The straight-wire appliance. Br J Orthod. 1979;6:125–143. doi: 10.1179/bjo.6.3.125. [DOI] [PubMed] [Google Scholar]
- 2.Sebanc J, Brantley WA, Pincsak JJ, Conover JP. Variability of effective root torque as a function of edge bevel on orthodontic arch wires. Am J Orthod. 1984;86:43–51. doi: 10.1016/0002-9416(84)90275-6. [DOI] [PubMed] [Google Scholar]
- 3.Germane N, Bentley BE, Jr, Isaacson RJ. Three biologic variables modifying faciolingual tooth angulation by straight-wire appliances. Am J Orthod Dentofacial Orthop. 1989;96:312–319. doi: 10.1016/0889-5406(89)90350-8. [DOI] [PubMed] [Google Scholar]
- 4.Smith RN, Karmo M, Russell J, Brook AH. The variability of the curvature of the labial surface of the upper anterior teeth along the facial axis of the clinical crown. Arch Oral Biol. 2007;52:1037–1042. doi: 10.1016/j.archoralbio.2007.04.017. [DOI] [PubMed] [Google Scholar]
- 5.van Loenen M, Degrieck J, De Pauw G, Dermaut L. Anterior tooth morphology and its effect on torque. Eur J Orthod. 2005;27:258–262. doi: 10.1093/ejo/cji007. [DOI] [PubMed] [Google Scholar]
- 6.Cash AC, Good SA, Curtis RV, McDonald F. An evaluation of slot size in orthodontic brackets—are standards as expected. Angle Orthod. 2004;74:450–453. doi: 10.1043/0003-3219(2004)074<0450:AEOSSI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 7.Gioka C, Eliades T. Materials-induced variation in the torque expression of preadjusted appliances. Am J Orthod Dentofacial Orthop. 2004;125:323–328. doi: 10.1016/j.ajodo.2003.02.007. [DOI] [PubMed] [Google Scholar]
- 8.Joch A, Pichelmayer M, Weiland F. Bracket slot and archwire dimensions: manufacturing precision and third order clearance. J Orthod. 2010;37:241–249. doi: 10.1179/14653121043182. [DOI] [PubMed] [Google Scholar]
- 9.Badawi HM, Toogood RW, Carey JP, Heo G, Major PW. Torque expression of self-ligating brackets. Am J Orthod Dentofacial Orthop. 2008;133:721–728. doi: 10.1016/j.ajodo.2006.01.051. [DOI] [PubMed] [Google Scholar]
- 10.Archambault A, Major TW, Carey JP, Heo G, Badawi H, Major PW. A comparison of torque expression between stainless steel, titanium molybdenum alloy, and copper nickel titanium wires in metallic self-ligating brackets. Angle Orthod. 2010;80:884–889. doi: 10.2319/102809-604.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Moesi B, Dyer F, Benson PE. Roth versus MBT: does bracket prescription have an effect on the subjective outcome of pre-adjusted edgewise treatment. Eur J Orthod. 2013;35:236–243. doi: 10.1093/ejo/cjr126. [DOI] [PubMed] [Google Scholar]
- 12.Richmond S, Klufas ML, Sywanyk M. Assessing incisor inclination: a non-invasive technique. Eur J Orthod. 1998;20:721–726. doi: 10.1093/ejo/20.6.721. [DOI] [PubMed] [Google Scholar]
- 13.Cha BK, Lee JY, Jost-Brinkmann PG, Yoshida N. Analysis of tooth movement in extraction cases using three-dimensional reverse engineering technology. Eur J Orthod. 2007;29:325–331. doi: 10.1093/ejo/cjm019. [DOI] [PubMed] [Google Scholar]
- 14.Thiruvenkatachari B, Al-Abdallah M, Akram NC, Sandler J, O'Brien K. Measuring 3-dimensional tooth movement with a 3-dimensional surface laser scanner. Am J Orthod Dentofacial Orthop. 2009;135:480–485. doi: 10.1016/j.ajodo.2007.03.040. [DOI] [PubMed] [Google Scholar]
- 15.Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–310. [PubMed] [Google Scholar]
- 16.Taloumis LJ, Smith TM, Hondrum SO, Lorton L. Force decay and deformation of orthodontic elastomeric ligatures. Am J Orthod Dentofacial Orthop. 1997;111:1–11. doi: 10.1016/s0889-5406(97)70295-6. [DOI] [PubMed] [Google Scholar]
- 17.Fischer-Brandies H, Orthuber W, Es-Souni M, Meyer S. Torque transmission between square wire and bracket as a function of measurement, form and hardness parameters. J Orofac Orthop. 2000;61:258–265. doi: 10.1007/s000560050011. [DOI] [PubMed] [Google Scholar]
- 18.Altman DG. Practical statistics for medical research. London, UK: Chapman and Hill; 1991. [Google Scholar]