

Abstract
Abstract thinking is a cognitive process that involves the assimilation of concepts reduced from diffuse sensory input, organized, and interpreted in a manner beyond the obvious. There are multiple facets by which abstraction is measured that include semantic, visual-spatial and social comprehension. This study examined the prevalence and course of abstract and concrete responses to semantic proverbs and aberrant abstraction (composite score of semantic, visual-spatial, and social comprehension) over 20 years in 352 participants diagnosed with schizophrenia spectrum, affective psychosis, and unipolar non-psychotic depression. We utilized linear models, two-way ANOVA and contrasts to compare groups and change over time. Linear models with Generalized Estimation Equation (GEE) to determine association. Our findings show that regardless of diagnosis, semantic proverb interpretation improves over time. Participants with schizophrenia give more concrete responses to proverbs when compared to affective psychosis and unipolar depressed without psychosis. We also show that the underlying structure of concretism encompasses increased conceptual overinclusion at index hospitalization and idiosyncratic associations at follow-up; whereas, abstract thinking overtime encompasses increased visual-spatial abstraction at index and rich associations with increased social comprehension scores at follow-up. Regardless of diagnosis, premorbid functioning, descriptive characteristics, and IQ, were not associated with aberrant abstraction. Delusions are highly and positively related to aberrant abstraction scores, while hallucinations are mildly and positively related to this score. Lastly, our data point to the importance of examining the underlying interconnected structures of ‘established’ constructs vis-a-vis mixed methods to provide a description of the rich interior world that may not always map onto current quantitative measures.
Introduction
Originally appearing in the English language in the fourteenth century, as a borrowing from the Latin “abstractus” meaning “to have been drawn away,” the term abstract was first applied to a thought process that “draws away” the more common attributes from the less common attributes of a group of sensory experiences, perceptual objects, or mental ideations into a unitary concept, symbol, idea, belief, or other cognitive aspect as in the idealist philosopher, Bishop George Berkeley’s famous observation, “Can there be a finer strain of abstraction than to distinguish the existence of sensible objects from their being perceived? (Dictionary, 1989).” The modern use of the word has been broadened to designate a more complex thought process that involves the assimilation of concepts reduced from a broad range of diffuse sensory inputs, organized, and interpreted through other mental representations in a manner beyond the obvious. This assimilation of concepts in normal abstraction is the developmental product of multiple stages of childhood cognitive development as first described in Piaget’s foundational studies. When this abstractive process becomes aberrant in psychosis features of Piaget’s sensorimotor, preoperational and concrete operational cognitive developmental stages re-emerge (Torres, Olivares, Rodriguez, Vaamonde, & Berrios, 2007).
Disturbance in abstract thinking, which is most often expressed in concrete or literal forms of cognition and speech, has been recognized as a characteristic of schizophrenia for over 100 years (Finckh, 1906; Harrow, Martin, Tucker, & Adler, 1972; Vigotsky & Kasanin, 1934). Constructs of either concrete or abstract thinking represent end points on a continuum characterizing the ability to shift one’s thinking about specific stimuli into less specific and more symbolic modes. In semantic interpretation, ‘concrete thinking’ refers to the tendency to use key words and ideas in a phrase from a proverb in their original form without translating the proverb into another phrase with a more conceptual interpretation. ‘Abstract thinking’ refers to the ability to synthesize concepts, principles, and relationships based on concepts, principles, and relationships between ideas and objects.
Heinrich Neuman, 1814–1884 and the unitary psychosis school of thought claimed that there was only one kind of ‘insanity’ that was caused by a “loosening of togetherness” and that the heterogeneity within psychosis was attributed to individual characteristics (Neuman, 1999; Torous & Keshavan, 2014). The first descriptions of concretism, or the “disorder of associative processes”, as a primary symptom of schizophrenia are attributed to Eugen Bleuler (Bleuler, 1950; Roche, Creed, MacMahon, Brennan, & Clarke, 2015). Bleuler further claimed that the core “fundamental” symptom of schizophrenia is a disintegration which results in a “loosening of associations (Bleuler, 1950)”; that are entangled in a diffusion of intrapsychic and interpersonal boundaries (Bleuler, 1950; Nordgaard, Gravesen-Jensen, Buch-Pedersen, & Parnas, 2021a). Bleuler described a “splitting” in the foundation of perception, affect, memory, and thought as the conceptual core of schizophrenia in which associations lose their connection resulting in unusual and often logically false interpretations (Bleuler, 1950; Bleuler, 2013; Rapaport, 1951). These unusual and logically false interpretations contribute to the belief formation within the context of delusional reality. Disturbances in associative processes are considered a fundamental component of formal thought disorder which are associated with the concrete responses in people given a diagnosis of schizophrenia (Bleuler, 2013; Harrow, Martin, Adler, & Hanf, 1974; Roche et al., 2015). There are multiple theories and reviews dealing with abstract and concrete thinking that extend beyond the scope of this article (Glucksberg & McGlone, 2001; Lakoff & Johnson, 2004; Thoma & Daum, 2006).
Proverb interpretation is often used to assess thought disturbances and cognitive processes in schizophrenia (Goldstein, K., 1939; Harrow, Martin & Quinlan, 1985). The degree of concreteness has also been associated with overall IQ, executive functions, attention, memory, socio-cultural features, and positive or negative symptom severity (Harrow, Martin et al., 1972; Sponheim, Surerus-Johnson, Leskela, & Dieperink, 2003). Our earlier work show that difficulties in providing abstract proverb interpretations are not uniquely distinguishable in schizophrenia but are also present in affective psychosis subgroups when compared to controls (Harrow, Martin & Quinlan, 1977). Research of semantic abstraction reported that participant performance included the “inability to maintain adequate boundaries, to restrict, eliminate and focus on the task in hand.” In place of a precise answer “a cluster of more or less related elements or imprecise approximations” were offered, and elements from problems outside the test situation were woven into answers to test questions (Cameron, 1944). Semantic abstraction is only one facet of abstract thinking. There are multiple facets by which the plasticity of abstraction is measured which extend into the visual-spatial realm and social comprehension (Thoma & Daum, 2006).
Object sorting test, as a measure of visual-spatial abstraction, was initially introduced by Vigotsky to study thought disorder in schizophrenia (Vigotsky & Kasanin, 1934). Its rationale is described by Rapaport (1945): “Sorting behaviour, in response to instructions to ‘put together those objects which belong together’ is an expression of concept formation. Sorting behavior, wherein participants compare objects that belong to the realm and objects that do not belong to the realm, gives the examiner an opportunity to assess how rigid and concrete (narrow), or how fluid, vague, and over-generalized (loose or multidimensional complex associations), the concept formation of the subject is (Rapaport, Gill, & Schafer, 1945).” Object sorting test results have been considered a measure of abstract and concrete thinking (Harrow, Martin & Quinlan, 1985; McConaghy, 1959). In general, object sorting provides an evaluation of visual-spatial abstraction.
Social comprehension has also been considered a form of abstraction associated with social cognitive abilities that involve understanding and interpreting mental representation and processes that contribute to human social judgments, social behavior and ways people perceive and evaluate other people and social groups and act toward them (Bambini, Bertini, Schaeken, Stella, & Di Russo, 2016; Marengo, Joanne T., Harrow, Lanin-Kettering, & Wilson, 1986; Smith & Semin, 2007). Ability to infer mental states in a social context has been shown to be highly correlated with abstract thinking (Braine & Bodenstein, 2005).
The overall process of abstract thinking, regardless of form (e.g., semantic, visual-spatial, and social comprehension) involves assimilation of “partial conformities of several objects of perception that are preceded by a stage in which these precepts are experientially present as definite objects with a definite number of well-defined given properties. The actual feat of abstraction consists in either voluntarily or involuntarily singling out from all the given contents (Weigl, 1941).”
Longitudinal research examining the course of abstract and concrete thinking in schizophrenia is rare and associations between abstract thinking and factors considered to influence abstraction remain in question, in addition to the relationship between abstraction and delusional reality and hallucinations. The current research addresses these questions in a prospective 20-year multi-follow-up longitudinal study of course of abstract thinking and other prognostic features in relation to symptoms and outcome in individuals with schizophrenia, affective psychosis, or non-psychotic unipolar depression. Research aims for this study sought to investigate four primary questions:
What is the prevalence and course of abstract and concrete responses to semantic proverbs and aberrant abstraction (composite score of semantic, visual-spatial and social comprehension) over time in schizophrenia spectrum, affective psychosis, and unipolar non-psychotic depression?
Is there a relationship between abstract and concrete responses to semantic proverbs, visual-spatial abstraction, and social comprehension by diagnostic group?
Are descriptive characteristics (sex, race, level of education, social economic status, IQ etc), or factors contributing to premorbid functioning associated with aberrant abstraction?
Is there a relationship between aberrant abstraction and hallucination or delusions in persons with schizophrenia?
Method
Participants and measures
Our sample consisted of 352 participants with one or more follow-up and who met diagnostic criteria for either schizophrenia (n=142), affective psychosis (n=102) or unipolar depressed nonpsychotic (n=108) and were evaluated on all three dimensions of abstract thinking. Total number of follow-up observations were 1256 in the original data and 1401 after imputation, which indicates an average of 3.57 (and 3.98 after imputation) follow-ups for each patient (Kim & Sherry, 2010). All participants were evaluated at index hospitalization as part of the Chicago Longitudinal study, a prospective research program designed to study major symptoms including psychopathology, abstract and concrete thinking, neurocognition, and recovery in schizophrenia and primary mood disorders (Harrow, Martin et al., 1974; Harrow, Martin & Jobe, 2005; Luther et al., 2020; Rosen, Grossman, Harrow, Bonner-Jackson, & Faull, 2011; Strauss, Harrow, Grossman, & Rosen, 2010). Participants were reassessed at 6 subsequent follow-ups over a 20-years. Follow-ups occurred at approximately 2, 4.5, 7.5, 10, 15, and 20 years after index hospitalization. The study was approved by the University of Illinois at Chicago (IRB# 1997–0053), and all participants signed an informed consent prior to initiation of study procedures at index hospitalization and at each subsequent follow-up.
Assessments were conducted by trained research assistants who were blind to diagnosis and previous ratings. Participants were diagnosed at index hospitalization using the Diagnostic and Statistical Manual Version III criteria (American Psychiatric Association, 1980). The Schedule for Affective Disorders and Schizophrenia (SADS) (Endicott & Spitzer, 1978), and Schizophrenia State Inventory (Grinker Sr, Roy Richard Ed & Harrow, 1987) were administered as part of diagnostic determination. At index, the Vaillant (Vaillant, 1962; Vaillant, 1978) and Stephen’s symptomatic Prognostic Index (Stephens, Richard, & McHugh, 1997; Westermeyer & Harrow, 1984) were administered to predict poor prognostic potential versus moderate prognostic potential. We also administered Zigler’s Prognostic Index (Zigler & Glick, 2001) based on developmental characteristics (e.g. graduated from high school). Positive and negative symptoms at index hospitalization and at each subsequent visit were assessed using the SADS (Endicott & Spitzer, 1978). Gorham Proverbs Test (Gorham, 1956a; Gorham, 1956b; Gorham, 1963) was used in assessment of participants’ spontaneous responses and interpretation to proverbs over time. For examples from our participant sample, when asked what the saying “when the cat’s away the mice will play” means rather than just say more about it, a participant who utilized abstract thinking responded, “when the boss is gone, the employees will do what they want, fool around” whereas a participant who utilized concrete thinking responded, “when the cat’s there the mice won’t play.” Goldstein-Scheerer Object Sorting Test was used to evaluate abstract and concrete thinking using visual-spatial parameters (O’Brien Jr, 1987). A subtest of the Wechsler Adult Intelligence Scale Comprehension subtest was used to measure social comprehension (WAIS; (Wechsler, 1955)). A composite index measure was used to evaluate multidimensional aspects of abstraction (aberrant abstraction) were derived from Goldstein-Scheerer Object Sorting Test (Goldstein, K. & Scheerer, 1941), Gorham Proverbs test (Gorham, 1956a), and Social Comprehension Subtest of the Wechsler Adult Intelligence Scale (WAIS; (Wechsler, 1955)). See Supplemental materials 1 for detailed description of study measures.
Statistical Analyses
Analyses were carried out using SPSS version 21 and SAS 9.4. Pearson’s chi-squares and one-way ANOVA were used to compare demographic variables across groups at index hospitalization. Linear models, two-way ANOVA and contrasts were used to compare proverb abstract, concrete and aberrant abstraction composite scores at both index hospitalization and follow-ups among diagnosis groups and over time. Linear models with Generalized Estimation Equation (GEE) were used to handle repeated measures in analysis focusing on association between variables, instead of trend over time. Autoregressive covariance structure was used for the GEE models due to the consideration on temporal repeated observations over time. To increase robustness of GEE models, missing measures in the middle (available before and after the current follow-up) on psychopathology, semantic abstraction, visual-spatial abstraction, social comprehension and aberrant abstraction were imputed by carrying over the value from previous observation (Kim & Sherry, 2010). Missing measures at index hospitalization or after the last non-missing follow-up were not imputed. Data with imputation were used only in GEE models.
Results
Demographic Characteristics
Table 1 lists demographic characteristics of study sample at index hospitalization. See Supplemental materials 2 for text description of demographic characteristics.
Table 1:
Index Demographic and Descriptive Table
| Schizoph renia | Affective Psychosis | Unipolar Depressed (non-psychotic | p-values | ||||
|---|---|---|---|---|---|---|---|
| n=142 | n=102 | n=108 | |||||
| Sex (Male/Female) | 87/55 | 43/59 | 37/71 | X2 (2) = 19.56, p ≤ .001 | |||
| Race (White/Black) | 96/46 | 72/29 | 86/21 | X2 (2) = 5.12, p = 0.08 | |||
| Age at first episode (≤23/≥24) | 121/14 | 88/14 | 68/37 | X2 (2) = 26.30, p ≤ .001 | |||
| M | SD | M | SD | M | SD | ||
| Age at index hospitalization | 23.18 | 4.16 | 22.72 | 5.34 | 23.62 | 4.14 | F(2, 349) = 1.05, p = .35 |
| Educational level at index hospitalization | 12.69 | 1.93 | 13.36 | 2.05 | 13.75 | 2.10 | F(2, 343) = 8.60, p ≤ .001 |
| IQ at index hospitalization | 10.19 | 2.95 | 11.09 | 2.93 | 11.04 | 2.58 | F(2, 232) = 2.73, p = .07 |
| SES (Hollingshead Index) | 3.12 | 1.44 | 2.95 | 1.38 | 2.95 | 1.26 | F(2, 323) = .58, p = .56 |
| Number of previous hospitalizations | 1.50 | 1.82 | 1.69 | 2.36 | .69 | 1.29 | F(2, 349) = 8.76, p ≤ .001 |
| Number of follow-up evaluations in original data | 3.42 | 1.85 | 3.65 | 1.86 | 3.69 | 1.86 | F(2, 349) = 0.82, p = .44 |
| Number of follow-up evaluations with imputation | 4.01 | 1.95 | 3.91 | 1.94 | 4.00 | 1.97 | F(2, 349) = 0.09, p = .91 |
| Aberrant Abstraction | 3.21 | 1.24 | 3.05 | 1.29 | 2.13 | 0.90 | F(2, 248) = 19.83, p ≤ .001 |
| Delusions | 2.69 | 0.69 | 2.43 | 0.85 | 1.09 | 0.34 | F(2, 326) = 127.96, p ≤ .001 |
| Hallucinations | 2.40 | 0.89 | 1.79 | 0.93 | 1.07 | 0.29 | F(2, 327) = 88.53, p ≤ .001 |
M = Mean; S.D. = Standard deviation
Diagnostic differences in the longitudinal trajectory of abstract thinking
Figure 1a reports the longitudinal trajectory of abstract thinking at index hospitalization and six follow-up evaluations over 20 years in participants with schizophrenia, affective psychosis, and non-psychotic unipolar depression. Linear model results show significant main effects for groups (F(2,1240)=72.74, p<0.001) and time (F(6,1240)=7.25, p<0.001), which indicates a significant variation of abstract thinking among groups and over time. Pairwise comparison among groups are all significant (p-values<0.001). On average, participants with schizophrenia have the lowest abstract score, participants with non-psychotic unipolar depression have the highest scores and participants with affective psychosis’ scores are in the middle. Abstract scores were the lowest at index. Longitudinal trajectory of abstraction show a decreased score at 4.5-year follow-up compared to other follow-ups. Differences between 4.5-year follow-up and 2-year, 7.5-year and 10-year are not significant (p=0.1567, 0.2624 and 0.1162 respectively); while scores are significantly higher at 15-year and 20-year follow-ups compared to 4.5-year (p=0.0355 and 0.0138 respectively). Differences of abstract scores for all other pairwise time period comparison are not significant (all p-values<0.05).
Figure 1a.
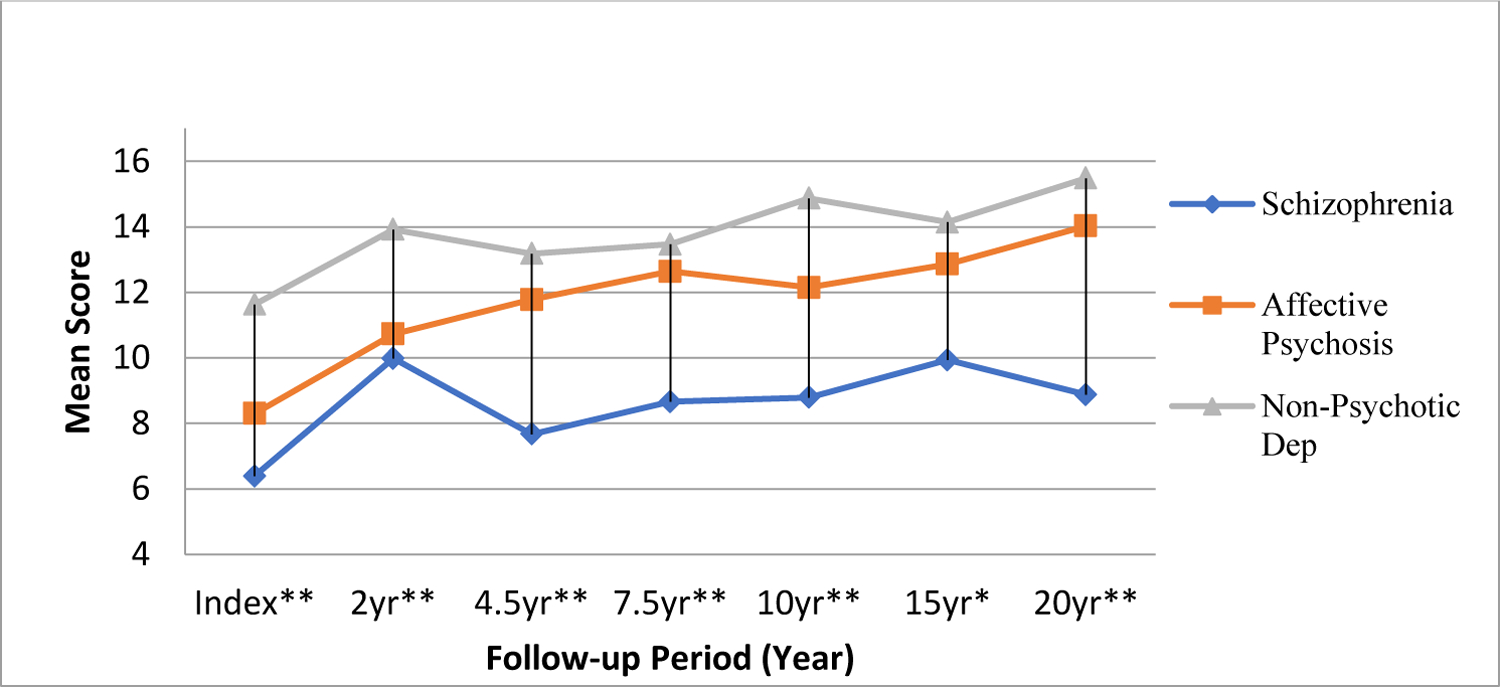
Diagnostic Compairson of Abstract Thinking Six Follow-ups over 20 years
Pairwise comparisons between diagnosis groups and between time points were also done by defining appropriate contrasts in the fitted linear models. Results show that at all 7 time points, from index hospitalization to follow-up at 20 years, the average values of abstract thinking in these three groups are significantly different (p-values<0.05). The value of abstract thinking for participants with schizophrenia is always significantly lower than those for participants with affective psychosis (p-values≤0.05 except at year-2, p=0.4241) and those participants with non-psychotic unipolar depression (p-values≤0.001). However, the difference between participants with affective psychosis and non-psychotic unipolar depression are significant only at index (p=0.0012) and year-2 (p=0.0011), but not significant at year-4.5 (p=0.2143), year-7.5 (p=0.5008), year-10 (p=0.0533), year-15 (p=0.4067) or year-20 (p=0.346). The pattern of abstraction values at year-2 were not consistent for the three diagnosis groups: higher than all the later follow-up measures for Schizophrenia, lower than all the later follow-up measures for Affective Psychosis and in the middle comparing to later follow-up measures for Non-Psychotic Unipolar Depression. Patterns of abstract values after 2 years are similar for all three groups: a decreased score at year 4.5 and then a gradual increase in abstraction thereafter, a greater number of participants show increased abstraction scores during the 20 years compared to all previous follow-ups (p≤0.001), however, there was no significant difference between the 15 year and 20 year follow-up (p=.10).
Diagnostic differences in the longitudinal trajectory of concrete thinking
Figure 1b shows the trajectory of concrete thinking as measured using proverbs at index hospitalization and over the six follow-up evaluations spanning 20 years in participants with psychotic and non-psychotic disorders. Two way ANOVA shows significant group (F(2,1186)=63.37, p<0.001) and time (F(6,1186)=6.63, p<0.001) effect on the variation of concrete scores. In addition, participants with schizophrenia, collapsing across all follow-ups, had a greater rate of concrete thinking than participants with affective psychosis (p<0.001) and participants with non-psychotic depression (p<0.001). Participants with affective psychosis had a greater rate of concrete thinking than participants with non-psychotic depression (p<0.001).
Figure 1b.
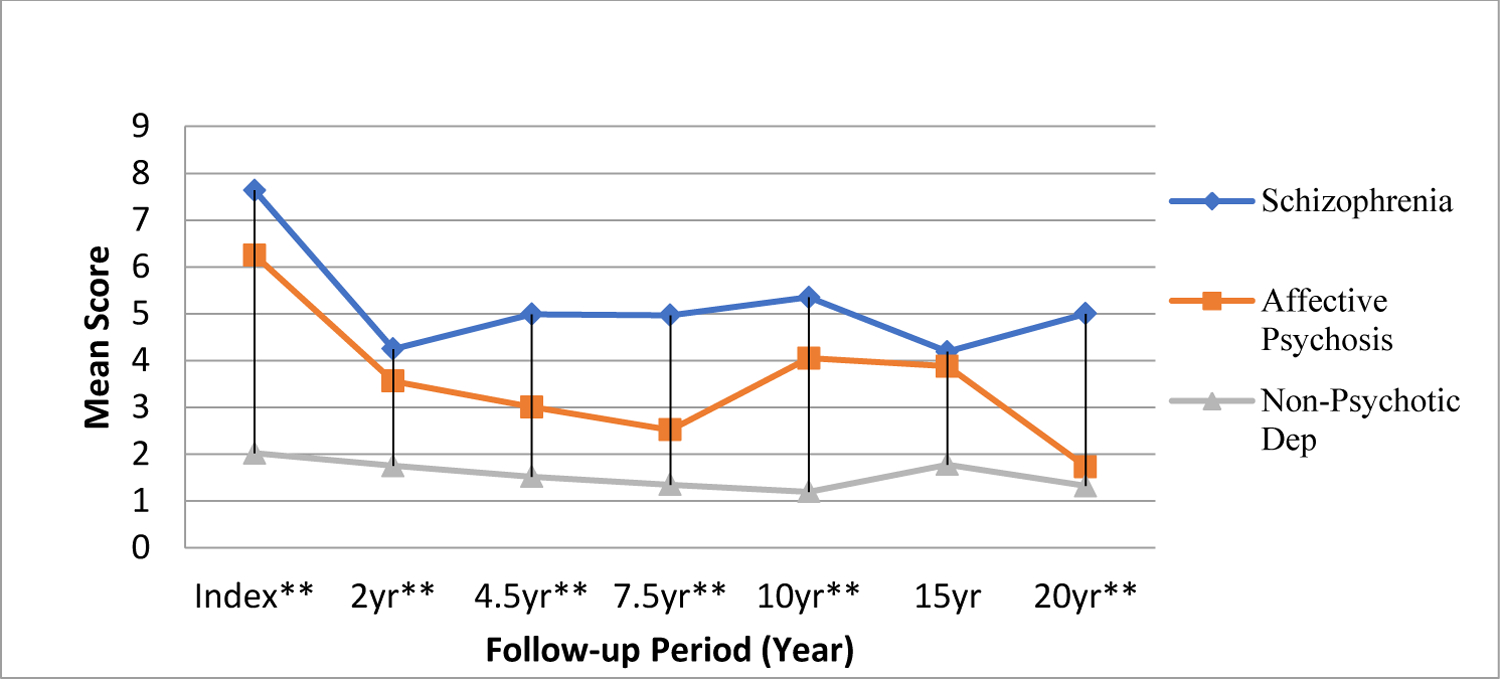
Diagnostic Compairson of Concrete Thinking Six Follow-ups over 20 years
Similar to the analysis for abstract thinking, ANOVA and contrasts from fitted linear models are performed to understand the longitudinal trajectory of concrete thinking among diagnosis groups and over time. A greater number of participants show increased concrete thinking in their response to proverbs questions during follow-ups (p-values<0.001). Concrete thinking scores at follow-up are not significant different from each other (p-values<0.05). Participants with schizophrenia show higher scores in concrete thinking at all follow-up points, with the exception of the 15 year follow-up, when compared to participants with non-psychotic depression and at 7.5, and 20 year follow-up when compared to participants with affective psychosis. Participants with affective psychosis show increased proverbs concrete scores of concrete response to proverbs by follow-up at 2, 10 year follow-up when compared to participants with non-psychotic depression.
Diagnostic differences in the longitudinal trajectory of aberrant abstraction
As a measure of the underlying construct of thought disturbance we utilized a composite score of aberrant abstraction established by Harrow and Marengo (Harrow, M., King, Marengo, Rattenbury, & Silverstein, 1985; Harrow, Martin & Quinlan, 1977; Marengo, Joanne T. & Harrow, 1987). Scores were derived from the Goldstein-Scheerer Object Sorting Test (Goldstein, K. & Scheerer, 1941), Gorham Proverbs test (Gorham, 1956a), and Social Comprehension Subtest of the Wechsler Adult Intelligence Scale (WAIS; (Wechsler, 1955)).
A Two way ANOVA shows significant group (F(2,1445)=65.18, p<0.001) and time (F(6,1445)=2.66, p=0.014) effect on variation of aberrant abstraction composite scores. Participants with schizophrenia had a higher aberrant abstraction score than participants with affective psychosis (p<0.001) and participants with non-psychotic depression (p<0.001). Participants with affective psychosis had a higher aberrant abstraction score than participants with non-psychotic depression (p<0.001). Aberrant abstraction scores decreased from index hospitalization at all later follow-ups (p-values<0.05) except year 20 (p=0.20). Further analysis by separate groups indicates that participants with schizophrenia have the highest aberrant abstraction score at index hospitalization. Then significantly decrease at 2-year (p=0.028) and 15-year (p=0.0157), but not significantly lower at other follow-ups (p-values<0.05). Participants with affective psychosis have a significantly lower aberrant abstraction score than at index and all follow-ups (p-values<0.05) with the exception of year-7.5 (p=0.1282). Participants with non-psychotic depression the aberrant abstraction scores did not change significantly over time since all pairwise comparisons have p-values greater than 0.05.
Longitudinal and diagnostic interrelatedness of semantic abstraction, visual-spatial abstraction, and abstraction in social comprehension
We next conducted a linear model with GEE to examine longitudinal diagnostic differences in the interrelationship between abstract and concrete responses to proverbs, visual-spatial abstraction and social comprehension (Table 2). Our data show that overall semantic proverbs scores at follow-up can be explained by index overall semantic proverbs, conceptual overinclusion, and concrete visual-spatial abstraction. Additionally, idiosyncratic associations, rich associations, and social comprehension at follow-up are also associated with overall semantic abstraction at follow-up showing that increased conceptual overinclusion at index and idiosyncratic associations at follow-up predicts concrete thinking or overall lower proverb abstraction scores. Whereas, increased index concrete visual-spatial abstraction and follow-up rich associations in addition to social comprehension scores predicts abstract thinking or higher overall proverb scores regardless of diagnostic groups.
Table 2:
Longitudinal and diagnostic interrelatedness of semantic abstraction, visual-spatial abstraction, and abstraction in social comprehension
| Analysis Of GEE Parameter Estimates | |||||||
|---|---|---|---|---|---|---|---|
| Empirical Standard Error Estimates | |||||||
| Parameter | Construct | Estimate | Standard Error | 95% Confidence Limits | Z | Pr > |Z| | |
| Intercept | 2.6447 | 0.9268 | 0.8282 | 4.4612 | 2.85 | 0.0043 | |
| Proverb abstraction overall (Index) | Semantic abstraction | 0.6419 | 0.0434 | 0.5568 | 0.7269 | 14.80 | <.0001 |
| Conceptual overinclusion (Index) | Visual-spatial abstraction | −0.3181 | 0.1089 | −0.5316 | −0.1047 | −2.92 | 0.0035 |
| Concrete visual-spatial abstraction (Index) | Visual-spatial abstraction | 0.2436 | 0.1282 | −0.0077 | 0.4950 | 1.90 | 0.0574 |
| Idiosyncratic associations (Follow-up) | Visual-spatial abstraction | −0.1941 | 0.1015 | −0.3932 | 0.0049 | −1.91 | 0.0559 |
| Rich associations (Follow-up) | Visual-spatial abstraction | 1.0583 | 0.3824 | 0.3088 | 1.8078 | 2.77 | 0.0056 |
| Social comprehension (Follow-up) | Social Comprehension | 0.4222 | 0.0735 | 0.2781 | 0.5663 | 5.74 | <.0001 |
Longitudinal and diagnostic association between premorbid functioning, descriptive characteristics and aberrant abstraction
We also conducted a linear model with GEE to examine longitudinal diagnostic differences and associations between Valliant and Stephen’s and Zigler’s Prognostic Index as a measure of premorbid functioning, descriptive characteristics (sex, race, level of education, social economic status, marital status etc), and aberrant abstraction and show that regardless of diagnosis neither premorbid functioning nor descriptive characteristics were associated with aberrant abstraction (p-values<0.05; Table 3).
Table 3:
Longitudinal and diagnostic association between premorbid functioning, descriptive characteristics, and aberrant abstraction
| Analysis Of GEE Parameter Estimates | ||||||
|---|---|---|---|---|---|---|
| Parameter | Estimate | Standard Error | 95% Confidence Limits | Z | Pr > |Z| | |
| Intercept | 1.0874 | 0.5272 | 0.0541 | 2.1208 | 2.06 | 0.0392 |
| Aberrant abstraction (Index) | 0.3789 | 0.0471 | 0.2867 | 0.4711 | 8.05 | <.0001 |
| Affective Psychosis | −0.1477 | 0.1326 | −0.4075 | 0.1121 | −1.11 | 0.2652 |
| Unipolar Depressed (non-psychotic) | −0.3714 | 0.1353 | −0.6365 | −0.1063 | −2.75 | 0.0060 |
| Schizophrenia | 0.0000 | 0.0000 | 0.0000 | 0.0000 | . | . |
| Valliant & Stevens Prognostic Index | 0.1959 | 0.1162 | −0.0319 | 0.4237 | 1.69 | 0.0919 |
| Zigler Prognostic Index | 0.2024 | 0.1275 | −0.0476 | 0.4524 | 1.59 | 0.1125 |
| Sex | −0.0756 | 0.1072 | −0.2856 | 0.1344 | −0.71 | 0.4805 |
| Race | −0.1287 | 0.1133 | −0.3507 | 0.0933 | −1.14 | 0.2560 |
| Age | 0.0128 | 0.0127 | −0.0122 | 0.0377 | 1.00 | 0.3156 |
Note: The response variable in this model is aberrant abstraction at follow-up.
Longitudinal association between hallucinations and delusions and aberrant abstraction in schizophrenia
Lastly, we examined the longitudinal relationship between hallucinations and delusions and aberrant abstraction composite score in schizophrenia over 20 years. Fitted linear model on time, delusion and hallucination indicates that after adjusting the effect of other variables, time is no longer a significant factor on variation of aberrant abstraction (F(5,348)=1.66, p=0.1441) (Table 4). But delusion is very closely and positively related to aberrant abstraction score (p<0.001); while hallucination is mildly and positively related to this score (p=0.0786) (Table 4).
Table 4:
Longitudinal association between hallucinations and delusions and aberrant abstraction in schizophrenia
| Parameter | Estimate | Standard Error | t Value | Pr > |t| | |
|---|---|---|---|---|---|
| Intercept | 1.653629213 | B | 0.29788778 | 5.55 | <.0001 |
| Aberrant abstraction (Index) | 0.182930603 | 0.05347960 | 3.42 | 0.0007 | |
| 02-year follow-up | −0.490926471 | B | 0.24134044 | −2.03 | 0.0427 |
| 05-year follow-up | −0.082418707 | B | 0.24843147 | −0.33 | 0.7403 |
| 08-year follow-up | −0.322006993 | B | 0.25298113 | −1.27 | 0.2039 |
| 10-year follow-up | −0.387988483 | B | 0.25904226 | −1.50 | 0.1351 |
| 15-year follow-up | −0.522930978 | B | 0.26723512 | −1.96 | 0.0512 |
| 20-year follow-up | 0.000000000 | B | . | . | . |
| Delusion follow-up | 0.391484797 | 0.09048601 | 4.33 | <.0001 | |
| Hallucination follow-up | 0.153905055 | 0.08725422 | 1.76 | 0.0786 |
Note: The response variable in this model is aberrant abstraction at follow-up.
Discussion
The goal of this study was to examine the trajectory of abstraction as a multidimensional construct that includes semantic abstraction, dimensions of visual-spatial abstraction, and social comprehension over 20-years, for six follow-ups in participants diagnosed with schizophrenia, affective psychosis, and non-psychotic depression. This is the first study to examine the longitudinal trajectory of aberrant abstraction (a composite score of semantic, visual-spatial, and social comprehension) as an underlying construct of thought disturbances to introduce a more integrated model of its potential underlying etiology and course.
As mentioned earlier, theorist considered concreteness as one of the essential features of schizophrenia (Arieti, 1955; Benjamin, 1944; Bleuler, 1950; Goldstein, K., 1964; Vygotsky, 2012). Thus, the presumed loss of ability to abstract successfully occupies a key place in theoretical conceptualizations and has been considered an important diagnostic marker for schizophrenia. Proverbs test remains one of the primary measures in neurocognitive and clinical measures developed to evaluate the continuum of abstract and concrete thinking (Goldstein, G., 1998; Gorham, 1956a; Harrow, Martin & Quinlan, 1985; Kay, Fiszbein, & Opler, 1987). Systematic investigations of the course of abstract and concrete thinking in a longitudinal framework are rare. However, there are studies that have investigated the short term course of abstract thinking which show a decrease in concreteness over a period of five weeks (Shimkunas, Algimantas M., Gynther, & Smith, 1966; Shimkunas, Aligimantas M., Gynther, & Smith, 1967). Similarly, our research demonstrated that the longitudinal course of sematic abstraction or proverb interpretation improves over time regardless of diagnosis. Participants with schizophrenia scored higher in concrete interpretation of proverbs when compared to affective psychosis and non-psychotic unipolar depression. Participants with affective psychosis and unipolar depressed were not significantly different over time in proverb interpretation. This data clearly demonstrates that in the groups studied the measure of semantic abstraction over time shows a progression from concrete responses at index to increased abstract responses of proverbs at follow-ups over 20 years, and that although concrete responses are more prevalent in participants with schizophrenia, it is not uniquely indicative of a core differential marker. Our findings also show aberrant abstraction are associated with the expression of psychosis (e.g., hallucinations and delusions) at index and during periods of psychosis at follow-up which may serve as an explanatory factor contributing to the improvement in abstraction overtime. Tangled in aberrant abstraction and psychosis is the self-dissolution of intrapsychic/interpersonal boundaries that are also prominent at the onset and during the exacerbation of psychosis (Pienkos et al., 2019; Rosen et al., 2016; Rosen et al., 2018). The association between disturbances or alterations of self-experience in psychosis and thought disorder further supports the hypothesis of a “unifying psychopathological core beneath the apparently heterogeneous symptoms of schizophrenia (Nordgaard, Gravesen-Jensen, Buch-Pedersen, & Parnas, 2021b).” Our results are associated with considerable improvement in other areas of psychopathology at the same time, indicating that the reduction in concrete thinking during recovery should be viewed as part of a more general picture involving improvement in a number of areas. However, it is important to note that “normal thinking” on the abstract-concrete dimension and other aspects of thinking in general are not well defined. Also important to note is that although the quantitative data show increased concrete thinking during episodes of increased psychosis, the qualitative literature describes a phenomenon of increased, at times overwhelming, expansion and intensification of abstraction.
The ability to engage in abstract thinking involves complex cognitive abilities. Dimensions of aberrant abstraction identified a core framework that included proverb interpretation, bizarre idiosyncratic thinking, rich associations, conceptual overinclusion, concrete visual-spatial abstraction and social comprehension. Overinclusive thinking has been described as a difficulty in maintaining usual conceptual boundaries and is primarily associated with rich associations and/or idiosyncratic (bizarre) thinking (Cameron, 1939; Harrow, Martin, Himmelhoch, Tucker, Hersh, & Quinlan, 1972). Idiosyncratic thinking and rich associations have shown to be more prevalent with delusions in acute episodes in individuals with schizophrenia (Cameron, 1939; Harrow, Martin et al., 1972), which was consistent with our findings showing that increased aberrant abstraction was consistently associated with the presence of delusions in participants with schizophrenia overtime. Associations between increased aberrant abstraction and presence of hallucinations, although present intermittently over-time, were not as consistent compared to associations between aberrant abstraction and delusions.
Loose associations are currently assessed by various metrics applied to computationally generated normed association tables and include associational distance, point-wise mutual information, and Hamming distance (Church & Hanks, 1990; Estes, Golonka, & Jones, 2011; Gruenenfelder, Recchia, Rubin, & Jones, 2016; Just et al., 2020). The results of these studies are thought to access recall or working memory capacity for each of the test dimensions of association included, ie, logical, lexical, semantic, analogical, thematic, etc. and have shown that improbable associations (degrees of looseness) are not only characteristic of persons with schizophrenia but also highly creative people (Mohr, Graves, Gianotti, Pizzagalli, & Brugger, 2001; Stacy, Ames, & Grenard, 2006). Overinclusive thinking, on the other hand, derives from classification tasks and relies primarily on recognition memory capacity. Testing usually involves measuring the number of false positive and false negative membership decisions by the subject involving words, images, or objects as per correct inclusion in a category, class, or physical space (Chapman & Chapman, 1973). Overinclusive thinking appears to be most severe in persons with manic psychosis followed by schizophrenia (Grossman, Harrow, & Sands, 1986; Marengo, Joanne & Harrow, 1985). Finally, richness and sparseness of association are modeled and measured by neural network assessments of connection density and connection strength (Lanillos et al., 2020). Largely stimulated by Ralph Hoffman’s early work, in which he used fully interconnected Hopfield neural networks, undergoing Hebbian learning, to show that excessive connection density effectively modeled in both persons with manic and schizophrenia patterns of thought disorder (Hoffman, 1987; Hoffman & McGlashan, 2001; Jobe & Gaveria, 1998). The field of computational neuroscience has developed machine learning diagnostics to better diagnose thought disorder from samples of speech more accurately than human practitioners (Ratana, Sharifzadeh, Krishnan, & Pang, 2019; Rezaii, Walker, & Wolff, 2019).
Previous research has shown that factors such as socio-developmental background, premorbid functioning, and IQ influence domains of abstract thinking (Berg et al., 2017; Shimkunas, Algimantas M. et al., 1966; Sponheim et al., 2003). However, our findings report that when multiple domains of abstraction (semantic, visual-spatial, and social comprehension) are examined as a construct of aberrant abstraction it is not directly associated with sex, race, IQ, premorbid functioning or factors related to socio-developmental background, regardless of diagnosis.
Interestingly, in psychosis, concrete responses to quantitative measures of abstraction are quite different from qualitative description and/or narratives which describe a wildly abstract interior. For example, in an early qualitative study conducted by McGhie and Chapman (1961) twenty-six participants with early psychosis were asked to describe their thought process while experiencing present state psychosis (McGhie & Chapman, 1961). Categories consisted of disturbances in a) process of attention, b) perception (sensory, speech, movement), c) motility and bodily awareness, d) process of thinking, and e) affective process. Changes in the process of thinking have been described as such: “if I am reading, I may suddenly get bogged down at a word. It may be any word, even a simple word that I know well. When this happens I can’t get past it. It’s as if I am being hypnotized by it. It’s as if I am seeing the word for the first time and in a different way from anyone else. It’s not so much that I absorb it, it’s more like it is absorbing me” and “I wish I could think without interruption ~ not from others but from inside myself.” Subjective experience of psychotic thought has been described as an increase in the interconnectivity of environmental cues or internal thoughts not previously associated: “My trouble is that I’ve got too many thoughts. You might think about something, let’s say that ashtray and just think, oh! Yes, that’s for putting my cigarette in, but I would think of it and then I would think of a dozen different things connected with it at the same time (McGhie & Chapman, 1961).” Again, from a phenomenological perspective Wouter Kusters, 2020 also describes the interior process of abstraction as: “We sense double bottoms, which we drop through deeper, underground levels. Down in that subterranean space, hidden from almost everyone else, the meanings of words and sentences branch off at lightning speed. We shoot through an entire network, whizzing along underground corridors, and come back to the surface with an answer at a place far removed from where we began. So they don’t understand us. They can’t follow our speed. They think we can’t concentrate on “the conversation.” But we don’t have to follow their conversation! We’re creating our own path. And underground we find a whole new level below that, and another and another (Kusters, 2020).” The subjective experience of aberrant abstraction, particularly within delusional reality, describes an interior world that is rich in abstraction one in which the “possibilities and impossibilities intertwine like rotating sides of mirror, but never settles on one side only…a maze of endless reflections and abstractions,…detached from consensual reality (Humpston, 2021).” The loosening of associations can manifest as overinclusive thinking which in turn has been associated with the presence of delusive beliefs (Doughty, Lawrence, Al-Mousawi, Ashaye, & Done, 2009; Payne, 1962). Within the continuum of consensual beliefs and delusive beliefs, which at the core involves abstract thinking, research investigating delusive beliefs in the general population found that 91% endorsed bizarre and non-bizarre delusion-like-beliefs (Pechey & Halligan, 2011). Delusive beliefs tend to start out as interoceptive and idiosyncratic at their core, secondarily having exteroceptive references and associations (Bortolotti, 2018). Consensual beliefs start out as social and exteroceptive and are then adopted interoceptively. Consensual beliefs have a level of generality or abstraction that makes the individual believer only an exemplar of the category “disciple, advocate, believer, member, ideologue, proponent, partisan, etc.” Delusional reality is aberrantly abstract by focusing on the individual self as the center of the belief “where nothing is concrete and everything is contradictory. Thoughts merge with percepts, yet percepts cannot fully become thoughts; mental processes are simultaneously formed, loosened, constricted and indefinitely expanded (Humpston, 2021).”
Conclusions
In this study we present findings on the 20-year longitudinal trajectory of abstract and concrete semantic abstraction, and aberrant abstraction (composite score of semantic, visual-spatial and social comprehension) in participants with schizophrenia, affective psychosis and non-psychotic unipolar depression. Our findings show that regardless of diagnosis, abstract thinking as a measure of semantic proverb interpretation improves over time. We also show that participants with schizophrenia give more concrete responses to proverbs when compared to affective psychosis and unipolar depressed without psychosis. Importantly, our data show that overall low or concrete semantic proverbs scores at follow-up can be explained by index overall semantic proverbs, conceptual overinclusion, and concrete visual-spatial abstraction. Additionally, idiosyncratic associations, rich associations, and social comprehension at follow-up are also associated with overall semantic abstraction. Indicating that, regardless of diagnosis, the underlying structure of concretism (lower proverb abstraction overall scores) encompasses increased conceptual overinclusion at index and idiosyncratic associations at follow-up. The underlying structure of abstract thinking overtime encompasses increased visual-spatial abstraction during the acute phase and rich associations in addition to social comprehension scores at follow-up. We report that regardless of diagnosis neither premorbid functioning nor descriptive characteristics, including IQ were associated with aberrant abstraction. Interestingly, our data also reveal that delusions are very closely and positively related to aberrant abstraction scores, while hallucinations are mildly and positively related to this score. Finally, our data point to the importance of examining underlying interconnected structures of ‘established’ constructs vis a vis mixed methods that provide the rich descriptive interior world of the “subterranean space hidden from almost everyone else (Kusters, 2020)” where “language has abstract as well as concrete terms and uses them in many ways as if they referred to things which are parts of the relevant concrete entity. It also says of the abstraction that it is and is in the concrete thing (Kujundzic, 2012).”
Supplementary Material
Figure 1c.
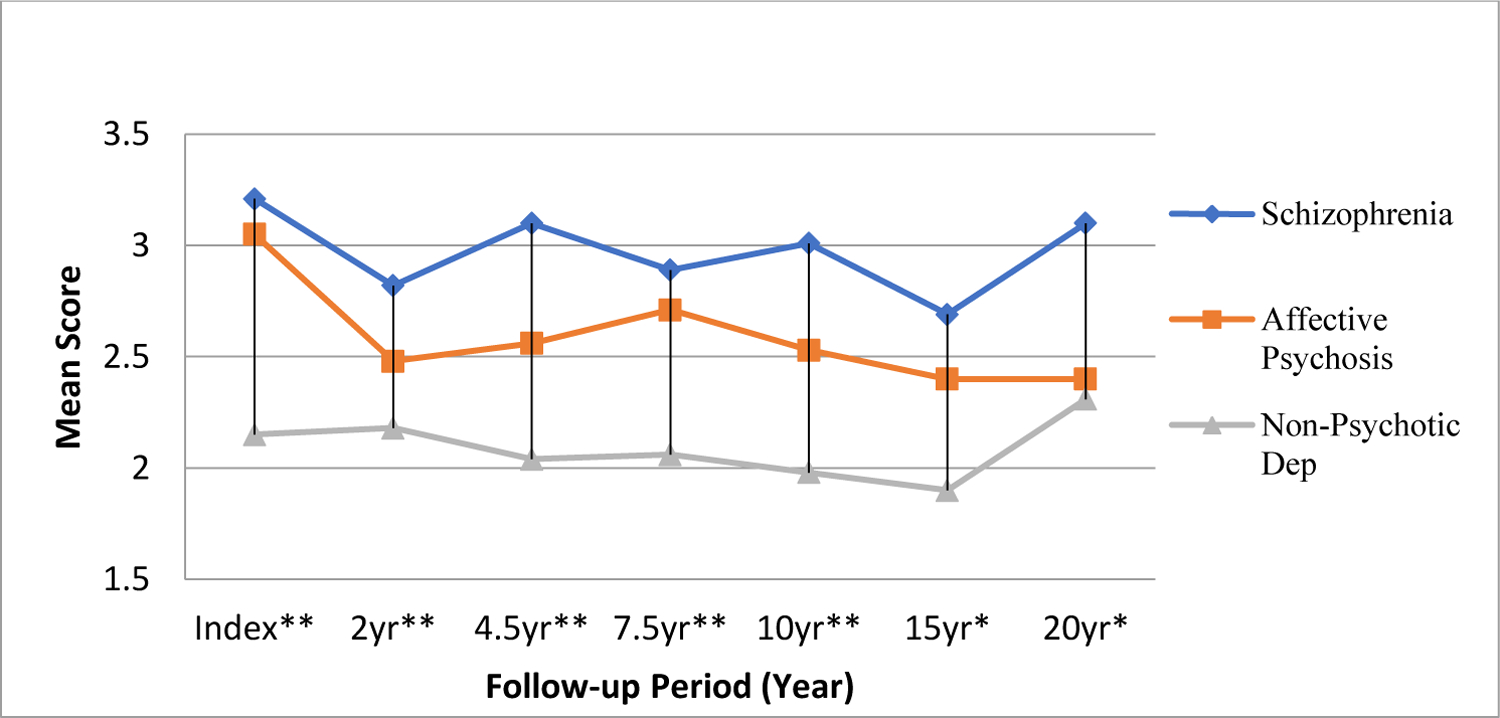
Diagnostic Compairson of Aberrant Abstraction Composit Score Semantic/visual spacial/social comprehension
P-values for group effect at each time point were recorded as very significant (p-value≤0.01, 2 stars), significant (0.01<p-value ≤0.05, 1 star) or insignificant (p-value>0.05, no star) in Figure 1.
Acknowledgement:
The authors would like to thank all the individuals who participated in this study as their contribution made this research possible.
Role of the funding source:
Supported, in part, by USPHS Grants MH-26341 andMH-068688 from the National Institute of Mental Health, USA (Dr. Harrow) and a Grant from the Foundation for Excellence in Mental Health Care G5014 (Dr. Harrow). The funding bodies had no other contribution to any part of the article.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declaration of competing interest: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- American Psychiatric Association. (1980). Quick reference to the diagnostic criteria from DSM-III The Association. [Google Scholar]
- Arieti S (1955). Interpretation of schizophrenia.
- Bambini V, Bertini C, Schaeken W, Stella A, & Di Russo F (2016). Disentangling metaphor from context: An ERP study. Frontiers in Psychology, 7, 559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benjamin JD (1944). A method for distinguishing and evaluating formal thinking disorders in schizophrenia. Language and Thought in Schizophrenia, 65, 90. [Google Scholar]
- Berg AO, Melle I, Zuber V, Simonsen C, Nerhus M, Ueland T, … Vaskinn A (2017). Modelling difficulties in abstract thinking in psychosis: The importance of socio-developmental background. Cognitive Neuropsychiatry, 22(1), 39–52. [DOI] [PubMed] [Google Scholar]
- Bleuler E Dementia Praecox, or the group of Schizophrenias, 1911. Translated by Zinkin J: International University Press, New York; 1950. [Google Scholar]
- Bleuler E (2013). Lehrbuch der psychiatrie Springer-Verlag. [Google Scholar]
- Bortolotti L (2018). Delusions in context Springer Nature. [Google Scholar]
- Braine M, & Bodenstein L (2005). Proverb comprehension reconsidered theory of mind and the pragmatic use of language in schizophrenia. Schizophrenia Research, 75(2–3), 233–239. [DOI] [PubMed] [Google Scholar]
- Cameron N (1939). Schizophrenic thinking in a problem-solving situation. Journal of Mental Science, 85(358), 1012–1035. [Google Scholar]
- Cameron N (1944). Experimental analysis of schizophrenic thinking. Language and Thought in Schizophrenia, , 50–64. [Google Scholar]
- Chapman LJ, & Chapman JP (1973). Disordered thought in schizophrenia. [DOI] [PubMed]
- Church K, & Hanks P (1990). Word association norms, mutual information, and lexicography. Computational Linguistics, 16(1), 22–29. [Google Scholar]
- Dictionary OE (1989). Oxford english dictionary. Simpson, Ja & Weiner, Esc, [Google Scholar]
- Doughty OJ, Lawrence VA, Al-Mousawi A, Ashaye K, & Done DJ (2009). Overinclusive thought and loosening of associations are not unique to schizophrenia and are produced in alzheimer’s dementia. Cognitive Neuropsychiatry, 14(3), 149–164. [DOI] [PubMed] [Google Scholar]
- Endicott J, & Spitzer RL (1978). A diagnostic interview: The schedule for affective disorders and schizophrenia. Archives of General Psychiatry, 35(7), 837–844. [DOI] [PubMed] [Google Scholar]
- Estes Z, Golonka S, & Jones LL (2011). Thematic thinking: The apprehension and consequences of thematic relations. Psychology of learning and motivation (pp. 249–294) Elsevier. [Google Scholar]
- Finckh J (1906). Zur frage der intelligenzprüfung
- Glucksberg S, & McGlone MS (2001). Understanding figurative language: From metaphor to idioms Oxford University Press on Demand. [Google Scholar]
- Goldstein G (1998). Neuropsychological assessment of abstract reasoning. Neuropsychology (pp. 317–331) Springer. [Google Scholar]
- Goldstein K (1939). The significance of special mental tests for diagnosis and prognosis in schizophrenia. American Journal of Psychiatry, 96(3), 575–588. [Google Scholar]
- Goldstein K (1964). Methodological approach to the study of schizophrenic thought disorder. Language and Thought in Schizophrenia, , 17–39. [Google Scholar]
- Goldstein K, & Scheerer M (1941). Abstract and concrete behavior an experimental study with special tests. Psychological Monographs, 53(2), i. [Google Scholar]
- Gorham DR (1956a). A proverbs test for clinical and experimental use. Psychological Reports, [Google Scholar]
- Gorham DR (1956b). Use of the proverbs test for differentiating schizophrenics from normals. Journal of Consulting Psychology, 20(6), 435. [DOI] [PubMed] [Google Scholar]
- Gorham DR (1963). Additional norms and scoring suggestions for the proverbs test. Psychological Reports, 13(2), 487–492. [Google Scholar]
- Grinker Roy Richard Sr Ed, & Harrow ME (1987). Clinical research in schizophrenia: A multidimensional approach. Charles C Thomas, Publisher. [Google Scholar]
- Grossman LS, Harrow M, & Sands JR (1986). Features associated with thought disorder in manic patients at 2–4-year follow-up. The American Journal of Psychiatry, [DOI] [PubMed] [Google Scholar]
- Gruenenfelder TM, Recchia G, Rubin T, & Jones MN (2016). Graph-theoretic properties of networks based on word association norms: Implications for models of lexical semantic memory. Cognitive Science, 40(6), 1460–1495. [DOI] [PubMed] [Google Scholar]
- Harrow M, King G, Marengo J, Rattenbury F, & Silverstein ML (1985). A manual to assess positive thought disorder, using the object sorting test. Unpublished Manual, [Google Scholar]
- Harrow M, Adler D, & Hanf E (1974). Abstract and concrete thinking in schizophrenia during the prechronic phases. Archives of General Psychiatry, 31(1), 27–33. [DOI] [PubMed] [Google Scholar]
- Harrow M, Himmelhoch J, Tucker G, Hersh J, & Quinlan D (1972). Overinclusive thinking in acute schizophrenic patients. Journal of Abnormal Psychology, 79(2), 161–168. [DOI] [PubMed] [Google Scholar]
- Harrow M, & Jobe TH (2005). No title. Longitudinal Studies of Outcome and Recovery in Schizophrenia and Early Intervention: Can they make a Difference?, [DOI] [PubMed]
- Harrow M, & Quinlan D (1977). Is disordered thinking unique to schizophrenia? Archives of General Psychiatry, 34(1), 15–21. [DOI] [PubMed] [Google Scholar]
- Harrow M, & Quinlan DM (1985). Disordered thinking and schizophrenic psychopathology. Gardner Press. [Google Scholar]
- Harrow M, Tucker GJ, & Adler D (1972). Concrete and idiosyncratic thinking in acute schizophrenic patients American Medical Association. [DOI] [PubMed] [Google Scholar]
- Hoffman RE (1987). Computer simulations of neural information processing and the schizophrenia-mania dichotomy. Archives of General Psychiatry, 44(2), 178–188. [DOI] [PubMed] [Google Scholar]
- Hoffman RE, & McGlashan TH (2001). Book review: Neural network models of schizophrenia. The Neuroscientist, 7(5), 441–454. [DOI] [PubMed] [Google Scholar]
- Humpston Clara Isolated by Oneself: Ontologically Impossible Experiences in Schizophrenia. In press: Philosophy, Psychiatry, & Psychology. [Google Scholar]
- Jobe TH, & Gaveria M (1998). On: Computer simulations of neural information processing and the schizophrenia-mania dichotomy. Journal of Psychosomatic Research, 44(6), 629–630. [DOI] [PubMed] [Google Scholar]
- Just SA, Haegert E, Kořánová N, Bröcker A, Nenchev I, Funcke J, … Montag C (2020). Modeling incoherent discourse in non-affective psychosis. Frontiers in Psychiatry, 11, 846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kay SR, Fiszbein A, & Opler LA (1987). The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophrenia Bulletin, 13(2), 261–276. [DOI] [PubMed] [Google Scholar]
- Kim SH, & Sherry A (2010). Descriptive discriminant analysis. Encyclopedia of Research Design, , 349–353. [Google Scholar]
- Kujundzic N (2012). (2012). The power of abstraction: Brentano, husserl and the göttingen students. Paper presented at the Symposium, , 16(2) 191–200. [Google Scholar]
- Kusters W (2020). A philosophy of madness: The experience of psychotic thinking MIT Press. [Google Scholar]
- Lakoff G, & Johnson M (2004). Metafory, kotorymi my zhivem [metaphors we live by]. Translated from English. Moscow: Editorial URSS, [Google Scholar]
- Lanillos P, Oliva D, Philippsen A, Yamashita Y, Nagai Y, & Cheng G (2020). A review on neural network models of schizophrenia and autism spectrum disorder. Neural Networks, 122, 338–363. [DOI] [PubMed] [Google Scholar]
- Luther L, Suor JH, Rosen C, Jobe TH, Faull RN, & Harrow M (2020). Clarifying the direction of impact of negative symptoms and neurocognition on prospective work functioning in psychosis: A 20-year longitudinal study. Schizophrenia Research, [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marengo JT, & Harrow M (1987). Schizophrenic thought disorder at follow-up: A persistent or episodic course? Archives of General Psychiatry, 44(7), 651–659. [DOI] [PubMed] [Google Scholar]
- Marengo JT, Harrow MM, Lanin-Kettering I, & Wilson A (1986). Evaluating bizarre-idiosyncratic thinking: A comprehensive index of positive thought disorder. Schizophrenia Bulletin, 12(3), 497–511. [DOI] [PubMed] [Google Scholar]
- Marengo J, & Harrow M (1985). Thought disorder: A function of schizophrenia, mania, or psychosis? Journal of Nervous and Mental Disease, [PubMed] [Google Scholar]
- McConaghy N (1959). The use of an object sorting test in elucidating the hereditary factor in schizophrenia. Journal of Neurology, Neurosurgery, and Psychiatry, 22(3), 243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGhie A, & Chapman J (1961). Disorders of attention and perception in early schizophrenia. British Journal of Medical Psychology, 34(2), 103–116. [DOI] [PubMed] [Google Scholar]
- Mohr C, Graves RE, Gianotti LR, Pizzagalli D, & Brugger P (2001). Loose but normal: A semantic association study. Journal of Psycholinguistic Research, 30(5), 475–483. [DOI] [PubMed] [Google Scholar]
- Neuman H (1999). Lehrbuch der psychiatrice.
- Nordgaard J, Gravesen-Jensen M, Buch-Pedersen M, & Parnas J (2021a). Formal thought disorder and self-disorder: An empirical study. Frontiers in Psychiatry, 12, 341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nordgaard J, Gravesen-Jensen M, Buch-Pedersen M, & Parnas J (2021b). Formal thought disorder and self-disorder: An empirical study. Frontiers in Psychiatry, 12, 341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Brien FJ Jr (1987). The goldstein-scheerer tests of abstract and concrete thinking. test review. [Google Scholar]
- Payne RW (1962). An object classification test as a measure of overinclusive thinking in schizophrenic patients. British Journal of Social and Clinical Psychology, 1(3), 213–221. [Google Scholar]
- Pechey R, & Halligan P (2011). The prevalence of delusion-like beliefs relative to sociocultural beliefs in the general population. Psychopathology, 44(2), 106–115. [DOI] [PubMed] [Google Scholar]
- Pienkos E, Giersch A, Hansen M, Humpston C, McCarthy-Jones S, Mishara A, … Sharma R (2019). Hallucinations beyond voices: A conceptual review of the phenomenology of altered perception in psychosis. Schizophrenia Bulletin, 45(Supplement_1), S67–S77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rapaport D (1951). Organization and pathology of thought: Selected sources.
- Rapaport D, Gill M, & Schafer R (1945). Diagnostic psychological testing, vol. 1. [Google Scholar]
- Ratana R, Sharifzadeh H, Krishnan J, & Pang S (2019). A comprehensive review of computational methods for automatic prediction of schizophrenia with insight into indigenous populations. Frontiers in Psychiatry, 10, 659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rezaii N, Walker E, & Wolff P (2019). A machine learning approach to predicting psychosis using semantic density and latent content analysis. NPJ Schizophrenia, 5(1), 1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roche E, Creed L, MacMahon D, Brennan D, & Clarke M (2015). The epidemiology and associated phenomenology of formal thought disorder: A systematic review. Schizophrenia Bulletin, 41(4), 951–962. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosen C, Grossman LS, Harrow M, Bonner-Jackson A, & Faull R (2011). Diagnostic and prognostic significance of schneiderian first-rank symptoms: A 20-year longitudinal study of schizophrenia and bipolar disorder. Comprehensive Psychiatry, 52(2), 126–131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosen C, Jones N, Chase KA, Gin H, Grossman LS, & Sharma RP (2016). The intrasubjectivity of self, voices and delusions: A phenomenological analysis. Psychosis, 8(4), 357–368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosen C, McCarthy-Jones S, Chase KA, Humpston CS, Melbourne JK, Kling L, & Sharma RP (2018). The tangled roots of inner speech, voices and delusions. Psychiatry Research, 264, 281–289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shimkunas AM, Gynther MD, & Smith K (1966). Abstracting ability of schizophrenics before and during phenothiazine therapy. Archives of General Psychiatry, 14(1), 79–83. [Google Scholar]
- Shimkunas AM, Gynther MD, & Smith K (1967). Schizophrenic responses to the proverbs test: Abstract, concrete, or autistic. Journal of Abnormal Psychology, 72(2), 128. [DOI] [PubMed] [Google Scholar]
- Smith ER, & Semin GR (2007). Situated social cognition. Current Directions in Psychological Science, 16(3), 132–135. [Google Scholar]
- Sponheim SR, Surerus-Johnson C, Leskela J, & Dieperink ME (2003). Proverb interpretation in schizophrenia: The significance of symptomatology and cognitive processes. Schizophrenia Research, 65(2–3), 117–123. [DOI] [PubMed] [Google Scholar]
- Stacy AW, Ames SL, & Grenard JL (2006). Of associative memory and implicit processes: Theoretical and assessment issues. Handbook of Implicit Cognition and Addiction, , 75. [Google Scholar]
- Stephens JH, Richard P, & McHugh PR (1997). Long-term follow-up of patients hospitalized for schizophrenia, 1913 to 1940. The Journal of Nervous and Mental Disease, 185(12), 715–721. [DOI] [PubMed] [Google Scholar]
- Strauss GP, Harrow M, Grossman LS, & Rosen C (2010). Periods of recovery in deficit syndrome schizophrenia: A 20-year multi—follow-up longitudinal study. Schizophrenia Bulletin, 36(4), 788–799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thoma P, & Daum I (2006). Neurocognitive mechanisms of figurative language processing—Evidence from clinical dysfunctions. Neuroscience & Biobehavioral Reviews, 30(8), 1182–1205. [DOI] [PubMed] [Google Scholar]
- Torous J, & Keshavan M (2014). The future of psychoses as seen from the history of its evolution. Current Behavioral Neuroscience Reports, 1(2), 94–99. [Google Scholar]
- Torres A, Olivares JM, Rodriguez A, Vaamonde A, & Berrios GE (2007). An analysis of the cognitive deficit of schizophrenia based on the piaget developmental theory. Comprehensive Psychiatry, 48(4), 376–379. [DOI] [PubMed] [Google Scholar]
- Vaillant GE (1962). The prediction of recovery in schizophrenia. The Journal of Nervous and Mental Disease, 135(6), 534–543. [DOI] [PubMed] [Google Scholar]
- Vaillant GE (1978). A 10-year followup of remitting schizophrenics. Schizophrenia Bulletin, 4(1), 78. [DOI] [PubMed] [Google Scholar]
- Vigotsky LS, & Kasanin J (1934). Thought in schizophrenia American Medical Association. [Google Scholar]
- Vygotsky LS (2012). Thought and language MIT press. [Google Scholar]
- Wechsler D (1955). Manual for the wechsler adult intelligence scale.
- Weigl E (1941). On the psychology of so-called processes of abstraction. The Journal of Abnormal and Social Psychology, 36(1), 3. [Google Scholar]
- Westermeyer JF, & Harrow M (1984). Prognosis and outcome using broad (DSM-II) and narrow (DSM-III) concepts of schizophrenia. Schizophrenia Bulletin, 10(4), 624–637. [DOI] [PubMed] [Google Scholar]
- Zigler EF, & Glick M (2001). A developmental approach to adult psychopathology John Wiley & Sons. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.