

Abstract
Background
Depressive symptoms has become an increasingly important public health issue, contributing to disability and disease burden around the world. Higher socioeconomic status (SES) has been found to be associated with lower prevalence of depression, but there are few studies about the older Chinese adults with long‐term follow up and rigorous prospective design. Meanwhile, there is little conclusive evidence about the mechanisms through which SES influences the onset of depressive symptoms.
Objective
To prospectively examine the association of baseline socioeconomic factors with the risks of developing depressive symptoms during 7‐year follow up in older Chinese population, and to study the mechanism by which SES impacts the prevalence of depressive symptoms.
Methods
A total of 5677 individuals over 45 years who participated in an ongoing nationally representative prospective cohort study, China Health and Retirement Longitudinal Study, were free from depressive symptoms at baseline, and completed 7‐year follow‐up were included. Depressive symptoms were assessed using the 10‐item Center for Epidemiological Studies Depression Scale score. Cox proportional hazards regression models were used to examine the association of SES and the incidence of depressive symptoms in 2011 to 2018. Generalized structural equation model was used to analyze the mediation effects of social support on the relation between SES and depressive symptoms.
Results
During the 7‐year follow‐up, 2398 (42.2%) cases were identified as depressive symptoms. Compared with the lowest level of household income, participants with the highest level of household income had a 20% reduction in risk (95% CI, 0.70–0.92, P < 0.001). Participants who had junior high school or above education had a 41% lower risk of depressive disorders compared with illiterate participants (95% CI, 0.52–0.69, P < 0.001). The relationship between SES and depressive symptoms was partially mediated by the social support, where higher social support was negatively associated with depressive symptoms. The proportion of mediation effect was even larger for women compared with men.
Conclusion
Socioeconomic factors were independently associated with the development of depressive symptoms, and the relationship was partially mediated by social support. Social support could be an effective intervention to alleviate the negative effects of lower SES on mental health. Multiple‐level policies should precisely target low‐SES groups, and timely intervention to promote social support for this group should be used to reduce the influence of depression on individuals, family as well as the whole society.
Keywords: depressive symptoms, longitudinal study, middle‐aged and older adults, social support, socioeconomic status
1. INTRODUCTION
Depression is a major mental health problem contributing to disability and the burden of disease globally (Mathers & Loncar, 2006; Whiteford et al., 2015). According to data issued by the World Health Organization data in 2017, more than 300 million people worldwide suffered from depression, with the prevalence rising by 18.4% over the past decade. In China, 54 million people suffered from depression, and the annual incidence had reached 4.2% (World Health Organization, 2017). Reports indicated that the incidence of depression increased by age and was particularly high among middle‐aged and elderly people (Liu et al., 2018). A nationally representative study showed that 30% of men and 43% of women aged 45 and over in China suffered depressive symptoms in 2011 and 2012 (Lei et al., 2014). With the increasing aging of China (UNFPA, 2020), the number of people suffering from depression is expected to rise dramatically in the middle‐aged and elderly. Individuals with depression have a 20‐time higher risks for suicide compared to that of general population (Osby et al., 2001), as well as a 60% increased risk of cardiovascular diseases (Barth et al., 2004). Furthermore, depression is associated with the loss in productivity and unemployment, placing a heavy burden on families and the whole society. For middle‐aged and older people, their body functions continue to deteriorate, and they may also face the risk of losing independence, financial troubles, and the coexistence of multiple chronic diseases (Boss & Seegmiller, 1981; Sivertsen et al., 2015).
The association between socioeconomic status (SES) and depressive symptoms has been reported in several studies (Freeman et al., 2016; Lotfaliany et al., 2019; Ng et al., 2014; Quashie et al., 2021; Wang et al., 2019). Lower SES may reduce the capacity to manage stress, and the long time exposure to the social stressors may result in higher depressive symptoms (Gallo & Matthews, 2003; Turner et al., 1995). However, the studies conducted among the older Chinese had been dubbed the “causation‐selection” issue, with most of the studies cross‐section designed or relative short time following up (Hu et al., 2019; Lei et al., 2014; Ruiz et al., 2019). On the other hand, the criticism of the previous work on SES and depressive symptoms includes the lack of control for confounding by sensory function (Harrison et al., 2019; Rong et al., 2020), housing conditions (Fang et al., 2019) and childhood deprivation (Ruiz et al., 2019) may partially explain the relationship.
Social support defined as “support accessible to an individual through social ties to other individuals, groups, and the larger community” (Fang et al., 2019), is negatively correlated with depressive symptoms (Faramarzi et al., 2015; Hu et al., 2018; Zhong et al., 2020). People with more social support tend to have more interpersonal resources when dealing with daily stress and are more likely to recover from stressful conditions (Mcdougall et al., 2016; Wang et al., 2016). Many studies confirmed that the distribution of social support was unequal among different socioeconomic classes and was more common in higher social classes (Matthews et al., 1999; Mickelson & Kubzansky, 2003). It has been found that social support mediates socioeconomic differences in health (Geckova et al., 2003; Matthews et al., 2008). However, studies with prospective design examining the role of social support in the relationship between SES and depression are quite scarce, particularly for the middle and low‐income countries.
This study aimed to prospectively examine the association between SES and the risks of developing depressive symptoms during 7‐year follow up from 2011 to 2018 in an older Chinese population. With few studies have examined the mechanisms and pathways through which SES impacts the prevalence of depressive symptoms, this study explored the mediation effect of social support on the relation between SES and depressive symptoms. We hypothesized that lower SES increased the risk of developing depressive symptoms and social support mediated the relationship between SES and depressive symptoms.
2. STUDY POPULATION AND METHODS
2.1. Data and study sample
The data for this study were derived from the China Health and Retirement Longitudinal Study (CHARLS), a nationally representative sample of Chinese adults aged 45 years or older and their spouses. The 2011 CHARLS baseline survey used multistage probability sampling to select 150 county‐level units in which 450 communities were chosen with 28 provinces in China. The interviewers were trained by Peking University before the survey and the participants were interviewed face‐to‐face in each household. A more detailed description about the study design and sampling procedure can be found in the cohort profile of CHARLS (Zhao et al., 2014). The data used in this study were followed up from the baseline survey to the latest CHARLS wave (2018). The 2011 baseline survey data included a total of 10,257 households and 17,708 individuals over 45. We excluded participants with missing data in depression (n = 1671), having depressive symptoms at baseline (n = 4504), those lost in follow‐up (n = 3250) and with missing critical data (n = 2606) from the analyses. In the end, the study included a total of 5677 participants over 45 years old without depressive symptoms at baseline and with completed 7‐year follow‐up. For the nonresponse group, the likelihood of nonresponses appeared to be uncorrelated with demographic, socioeconomic characteristics (Zhao et al., 2014). We further confirmed that there was no obvious correlation between social support and the likelihood of nonresponses. Figure 1 described the detailed information of the study flow chart.
FIGURE 1.
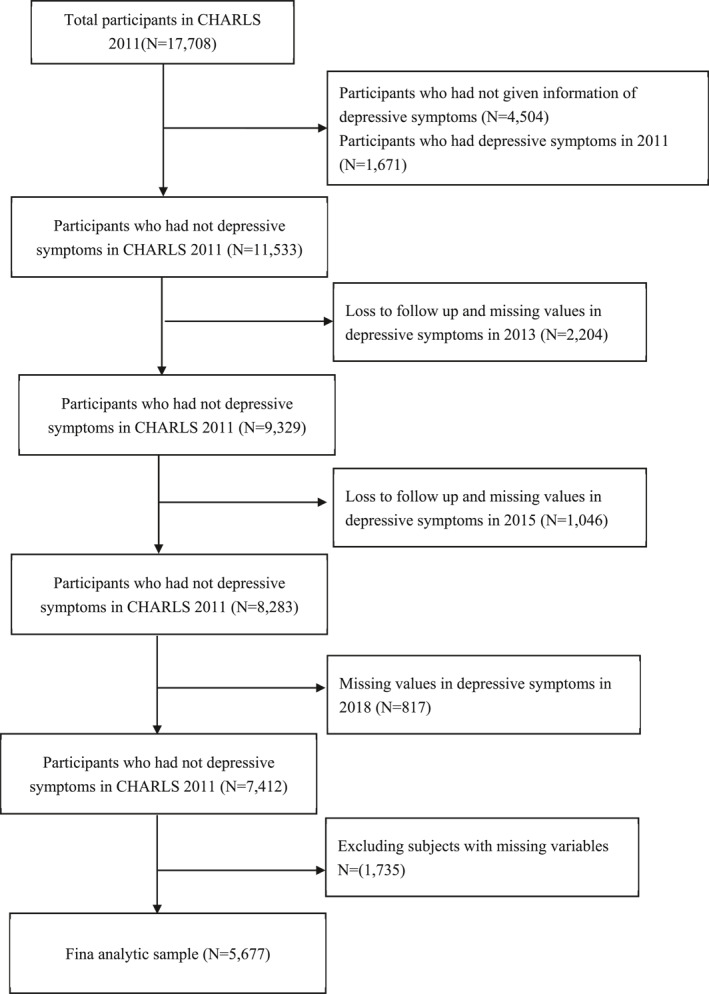
Flowchart of the study sample
The CHARLS study was ethically approved by the Peking University institutional review board (Zhao et al., 2014). This study was a secondary analysis of the CHARLS data sets and was waived from the ethical approval. The longitudinal study obtained written informed consent from all participants and was conducted following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline (von Elm et al., 2007).
2.2. Depressive symptoms
In the CHARLS survey, depressive symptoms were measured using a short form of the Center for Epidemiological Studies Depression Scale (CESD‐10), which contains 10 questions: (1) troubled by trivial matters, (2) troubled by inattention, (3) feeling frustrated, (4) laborious to do anything, (5) full of hope, (6) feeling fear; (7) poor sleep; (8) feeling happy; (9) feeling lonely, and (10) unable to continue living. Depressive symptoms over the past week were measured from 0 (little or no time [<1 day]) to 3 (most or all time [5–7 days]). Before summing the project scores, question 5 and 8 scores need to be converted. The CESD‐10, a useful mental health measure for the older people, has demonstrated satisfactory content and temporal validity and reliability among Chinese middle‐aged and older adults (Boey, 1999; Yang et al., 2015). The total score of CESD‐10 ranges from 0 to 30. A higher score indicates more depressive symptoms and previous studies show that a score of 12 or more have reasonable levels of sensitivity (0.76) and specificity (0.55) among older Chinese (Cheng & Chan, 2005; Li et al., 2015). We used 12 as the cut point for having elevated depressive symptoms (=1) and not depressed (=0; Chen & Mui, 2014; Li et al., 2019).
2.3. Socioeconomic status
We measured the SES by the participant's educational level and household annual income, as they have strong theoretical associations with depression (Lorant et al., 2003; Miech & Shanahan, 2000). Education level was classified as illiterate, primary school and below, and junior school and above. Quintiles for household annual income were used with household annual income ≤3000 RMB coded level 1, 3000−10,000 RMB coded level 2, 10,000−24,000 RMB coded level 3, 24,000−36,000 RMB coded level 4, >36,000 coded level 5. To examine the mediation effect of SES and depressive symptoms through social support, a composite score of SES was constructed by multiplying the education level and household annual income level (Katsarou et al., 2010).
2.4. Social support
A comprehensive index including family support, community support and public support were used to measure social support in our study (Hu et al., 2018; Zurlo et al., 2014). Family support referred to whether the participants live with a spouse (0 = no; 1 = yes), whether the participants weekly contact with their children in person (0 = no; 1 = yes), and whether the participants weekly contact with their children by phone or email (0 = no; 1 = yes). Community support included community infrastructure and resources, which was measured by the following questions: whether the village/community has outside exercising facilities (0 = no; 1 = yes); whether the village/community has dancing team or other exercise organizations (0 = no; 1 = yes); whether the village/community has organizations for helping the elderly and the handicapped (0 = no; 1 = yes); whether the village/community has activity center for the elderly (0 = no; 1 = yes); whether the village/community has elderly association (0 = no; 1 = yes). Public support was proxied by social security and welfare for the older people, referring to whether the participants have pensions (0 = no; 1 = yes), and whether the participants have medical insurance or welfare (0 = no; 1 = yes). By summing the 3 aspects of social support, the comprehensive index ranges from 0 to 10, with higher score reflecting higher level of social support.
2.5. Covariates
Information about other sociodemographic status, health behavior, health condition, household condition, and childhood deprivation of the participants were controlled in our study, including age, gender (male or female), smoking status (current, former of never), alcohol drinker (current, former, or never), number of non‐communicable diseases (0, 1–2, or ≥3), self‐assessment health (excellent, very good, good, moderate, or bad), body mass index (≤19, 20–24, 25–28, or ≥29), hearing function (good or poor). Activities of daily living (ADLs) were measured using a six‐item summary in CHARLS that included bathing, dressing, eating, getting in/out of bed, using the toilet and controlling urination with 0 for no difficulty and 1 for having difficulty in each activity (Zhou et al., 2020). Non‐communicable diseases included hypertension, dyslipidemia, diabetes, cancer, chronic lung diseases, liver diseases, heart diseases, stroke, kidney diseases, digestive diseases, psychiatric diseases, memory‐related diseases, arthritis and asthma. The household condition was measured by whether the residence has a telephone connection. Childhood deprivation referred to whether the participants ever lacked enough food to eat in the CHARLS.
2.6. Statistical analysis
Firstly, descriptive statistical analysis and the Pearson χ2 test were used to analyze the difference between the respondents who developed depressive symptoms during the seven‐year follow up and those who had no depressive symptoms by the end of the seven‐year follow up. To model the effect of SES on the incidence of depressive symptoms, cox proportional hazards regression was used to fit the longitudinal data. We calculated the follow‐up time as the number of months from the wave 1 interview date to follow‐up interview date where the first diagnosis of depressive symptoms occurred, or censoring (the date of the participant's last interview) took place. We fitted an unadjusted model and gradually adjusted for social support, demographic characteristics, health behaviors, health conditions, childhood deprivation, hearing function and telephone connection. The proportional hazards (PH) assumption was checked using statistical tests based on the scaled Schoenfeld residual, and all the models meet the assumption with P > 0.05. Structural equation model (SEM) is designed to test more intricate mediation models in a single analysis and can be used to extend a mediation process to multiple independent variables or outcomes (MacKinnon, 2008). We examined the mediation effect of social support on the relationship between SES and depressive symptoms through the generalize structural equation model after controlling for the all the covariates (Angkananard et al., 2019; Gunzler et al., 2013). We further evaluated whether the mediation effect differed between male and female.
To address concerns about selection bias, we conducted sensitivity analyses. The analyses were conducted as follows: (1) participants with missing income variable were included in model 1 to model 4 with a number of 6627 recipients; (2) binary mediation analysis with bootstrap standard errors and confidence intervals was used to explore the mediation effect of SES and depressive symptoms through social support. Individual weights in the CHARLS data were applied in the regression analysis to take into account selection probability, non‐response patterns and post‐stratification factors (Liu et al., 2017). We considered a two‐sided.
P < 0.05 statistically significant. The software Stata version 14.1 for Mac (Stata Corp) was used for statistical analysis.
3. RESULTS
Table 1 described the incidence of depressive symptoms after seven years among the CHARLS participants and their subgroups who were free of depression at baseline and the relationship between depressive symptoms and baseline characteristics in participants without depressive symptoms after 7 years follow‐up. Among 5677 middle‐aged and elderly patients who were followed up, 2398 (42.2%) developed depressive symptoms after 7 years. The incidence of depressive symptoms was statistically significantly different among subgroups. For example, the rate was higher in female (50.1%) than male (34.1%), participants with lower household annual income or lower level of education, those with more difficulties in daily activity, those with three or more noncommunicable diseases (22.5%) compared to those with no diseases (13.8%), participants who had childhood deprivation (44.4%) compared to those with no deprivation (37.3%), and those who had poor hearing function (46.0%) compared to respondents with good hearing function (38.6%) (Table 1).
TABLE 1.
Seven‐year incidence of depressive symptoms among study participants free of disease at baseline and the association between sociodemographic and incidence
| Variables | N | Depressive symptoms n (%) | p‐value (χ2 test) |
|---|---|---|---|
| Total | 5677 | 2398 (42.2) | |
| Household income (Yuan) | <0.001 | ||
| ≤3000 | 1006 | 516 (51.3) | |
| 3000–10,000 | 926 | 463 (50.0) | |
| 10,000–24,000 | 1159 | 498 (43.0) | |
| 24,000–36,000 | 771 | 282 (36.6) | |
| >36,000 | 1815 | 639 (35.2) | |
| Education | <0.001 | ||
| Illiterate | 1301 | 757 (58.2) | |
| Primary school and below | 2312 | 1022 (44.2) | |
| Junior high school and above | 2064 | 619 (30.0) | |
| Age | <0.001 | ||
| <60 | 3622 | 1462 (40.4) | |
| 60–69 | 1575 | 695 (44.1) | |
| 70–79 | 439 | 213 (48.5) | |
| >80 | 41 | 28 (68.3) | |
| Gender | <0.001 | ||
| Female | 2879 | 1438 (50.1) | |
| Male | 2807 | 960 (34.1) | |
| Smoking | <0.001 | ||
| Current smoking | 1804 | 669 (37.1) | |
| Former smoking | 451 | 159 (35.3) | |
| Never smoking | 3422 | 1570 (45.9) | |
| Drinking | <0.001 | ||
| Current drinking | 1966 | 685 (34.8) | |
| Former drinking | 403 | 189 (46.9) | |
| Never drinking | 3308 | 1524 (42.2) | |
| Number of NCDs | <0.001 | ||
| 0 | 1939 | 659 (34.0) | |
| 1–2 | 2718 | 1202 (44.2) | |
| ≥3 | 812 | 440 (54.2) | |
| Missing | 208 | 97 (46.6) | |
| Self‐assessment health | <0.001 | ||
| Excellent | 43 | 12 (27.9) | |
| Very good | 427 | 120 (28.1) | |
| Good | 850 | 266 (31.3) | |
| Moderate | 2079 | 865 (41.6) | |
| Bad | 634 | 384 (60.6) | |
| Missing | 1644 | 751 (45.7) | |
| ADL score | <0.001 | ||
| 0 | 5117 | 2064 (40.3) | |
| 1 | 332 | 181 (54.5) | |
| 2–6 | 172 | 128 (74.4) | |
| Missing | 56 | 25 (44.6) | |
| BMI | <0.001 | ||
| ≤19 | 531 | 270 (50.9) | |
| 20–24 | 2582 | 1097 (42.5) | |
| 25–28 | 1440 | 581 (40.4) | |
| ≥29 | 516 | 214 (41.5) | |
| Missing | 608 | 236 (38.8) | |
| Childhood deprivation | <0.001 | ||
| No | 1702 | 634 (37.3) | |
| Yes | 3975 | 1764 (44.4) | |
| Hearing impairment | <0.001 | ||
| Good | 2873 | 1109 (38.6) | |
| Poor | 2804 | 1289 (46.0) | |
| Telephone connectivity | <0.001 | ||
| No | 2780 | 1259 (45.3) | |
| Yes | 2897 | 1139 (39.3) |
Abbreviations: ADL, activity of daily living; BMI, body mass index; NCD, non‐communicable diseases.
Table 2 showed the results of cox proportional hazards regressions. Participants with higher SES had a significantly lower risk of developing depressive symptoms in unadjusted model or models gradually adjusting for covariates during the 7‐year follow up. After adjusting for all potential confounders (in model 4), compared to the level 1 household annual income, participants with level 4 and level 5 household annual income had an estimate of 16% (HR = 0.84, 95% CI, 0.71–0.99) and 20% (HR = 0.80, 95% CI, 0.70–0.92) reduction in risk for elevated depressive model, respectively. Participants with primary school and below education and junior high school and above education were independently associated with a 17% and 41% reduced risk for developing elevated depressive symptoms (HR = 0.83, 95% CI, 0.75–0.92; HR = 0.59, 95% CI 0.52–0.69). Social support was negatively associated with depressive symptoms in all the models. With one score increase of social support, the risk of elevated depressive symptoms reduced 2% (HR = 0.98, 95% CI, 0.95–1.00) in model 4. We further explored the individual relationship of each type of social support with the risk of depressive symptoms. After seven‐year follow up, every increase in community support reduced the likelihood of elevated depressive symptoms by 3% (HR = 0.97, 95% CI 0.95–1.00, Table S1).
TABLE 2.
Hazard ratio of elevated depressive symptoms (95% CI)
| Variables | Model 1 | Model 2 | Model 3 | Model 4 |
|---|---|---|---|---|
| Household income (≤3000) | ||||
| 3000–10,000 | 0.95(0.84–1.08) | 0.95(0.84–1.08) | 0.98(0.86–1.11) | 1.00(0.88–1.14) |
| 10,000–24,000 | 0.85(0.75–0.97)** | 0.87(0.76–0.99)* | 0.89(0.78–1.02) | 0.91(0.79–1.03) |
| 24,000–36,000 | 0.76(0.65–0.90)*** | 0.79(0.67–0.92)** | 0.81(0.69–0.96)** | 0.84(0.71–0.99)* |
| >36,000 | 0.71(0.62–0.81)*** | 0.74(0.65–0.85)*** | 0.76(0.67–0.87)*** | 0.80(0.70–0.92)*** |
| Education (illiterate) | ||||
| Primary school and below | 0.72(0.65–0.80)*** | 0.73(0.66–0.81)*** | 0.82(0.74–0.91)*** | 0.83(0.75–0.92)*** |
| Junior high school and above | 0.47(0.41–0.53)*** | 0.48(0.42–0.55)*** | 0.60(0.53–0.67)*** | 0.59(0.52–0.69)*** |
| Social support | ‐ | 0.97(0.94–0.98)* | 0.97(0.95–1.00)* | 0.98(0.96–1.00)* |
| Gender (female) | ||||
| Male | ‐ | ‐ | 0.73(0.63–0.84)*** | 0.70(0.61–0.81)*** |
| Smoking (current smoking) | ||||
| Former smoking | ‐ | ‐ | 0.80(0.66–0.98)* | 0.78(0.64–0.96)* |
| Never smoking | ‐ | ‐ | 0.98(0.86–1.11) | 0.99(0.86–1.12) |
| Drinking (current drinking) | ||||
| Former drinking | ‐ | ‐ | 1.12(0.94–1.33) | 1.12(0.94–1.33) |
| Never drinking | ‐ | ‐ | 1.10(0.96–1.25) | 1.08(0.95–1.24) |
| Age (<60) | ||||
| 60–69 | ‐ | ‐ | 0.94(0.85–1.04) | 0.92(0.83–1.02) |
| 70–79 | ‐ | ‐ | 0.99(0.83–1.17) | 1.04(0.88–1.23) |
| >80 | ‐ | ‐ | 1.33(0.90–1.95) | 1.46(0.99–2.14) |
| Number of NCDs (0) | ||||
| 1–2 | ‐ | ‐ | 1.30(1.15–1.46)*** | 1.29(1.15–1.45)*** |
| ≥3 | ‐ | ‐ | 1.61(1.38–1.86)*** | 1.59(1.36–1.85)*** |
| Missing | ‐ | ‐ | 1.18(0.93–1.49) | 1.16(0.92–1.46) |
| Self‐assessment health (excellent) | ||||
| Very good | ‐ | ‐ | 0.84(0.45–1.56) | 0.78(0.41–1.49) |
| Good | ‐ | ‐ | 0.93(0.51–1.70) | 0.85(0.45–1.60) |
| Moderate | ‐ | ‐ | 1.16(0.64–2.11) | 1.05(0.56–1.96) |
| Bad | ‐ | ‐ | 1.61(0.88–2.95) | 1.46(0.78––2.75) |
| Missing | ‐ | ‐ | 1.08(0.59–1.96) | 0.98(0.52–1.83) |
| ADL score (0) | ||||
| 1 | ‐ | ‐ | 1.11(0.95–1.31) | 1.09(0.93–1.29) |
| 2–6 | ‐ | ‐ | 1.59(1.32–1.90)*** | 1.57(1.31–1.88)*** |
| Missing | ‐ | ‐ | 1.23(0.70–2.16) | 1.26(0.72–2.19) |
| BMI (≤19) | ||||
| 20–24 | 0.89(0.78–1.03)* | 0.87(0.76–1.00) | ||
| 25–28 | ‐ | ‐ | 0.81(0.69–0.96)*** | 0.80(0.68–0.93)** |
| ≥29 | ‐ | ‐ | 0.74(0.60–0.90)** | 0.72(0.59–0.88)*** |
| Missing | ‐ | ‐ | 0.89(0.73–1.09) | 0.89(0.73–1.08) |
| Childhood deprivation (yes) | ||||
| No | ‐ | ‐ | ‐ | 0.78(0.70–0.87)*** |
| Hearing impairment (good) | ||||
| Poor | ‐ | ‐ | ‐ | 1.05(0.95–1.16) |
| Telephone (yes) | ||||
| No | ‐ | ‐ | ‐ | 1.21(1.10–1.33)*** |
Abbreviations: ADL, activity of daily living; BMI, body mass index; NCD, non‐communicable disease.
*p < 0.05; **p < 0.01; ***p < 0.001.
Figure 2 and Table 3 demonstrated findings of the mediation role of social support between SES and depressive symptoms. For Figure 2, path a showed the direct link between SES and social support, path b showed the link between social support and depressive symptoms, path c represented the link between SES and depressive symptoms, and c’ displayed the effect of SES on depressive symptoms including the mediating social support. Path c was the total effect of depressive symptoms responding primarily to social support, and when the social support was considered, the coefficient of total effect was reduced to c’ (direct effect). After controlling for age, gender, and other potential confounders, the results showed that social support partially mediated the association between SES and depressive symptoms. The mediating effect (indirect effect, ab = c–c’) of social support was 0.0028, which accounted for 10.0% of the total effect. We also compared the mediation effect between female and male participants. The results revealed that compared to male (7.74%), the mediation effect (11.55%) was higher for female (Table S2).
FIGURE 2.
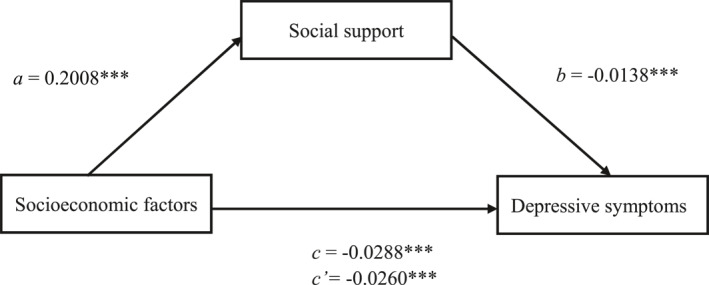
The mediating effects of social support on the relation between socioeconomic and depressive symptoms. Path a: The direct link between SES and social support. Path b: The link between social support and depressive symptoms. Path c: The link between SES and depressive symptoms. Path c’: The effect of SES on depressive symptoms including the mediating social support
TABLE 3.
Models of mediation effects of SES and depressive symptoms through social support
| β | SE | Z | P | 95% CI | |
|---|---|---|---|---|---|
| Total effect | −0.0286 | 0.0025 | −11.57 | <0.001 | (−0.0335, −0.0238) |
| Direct effect | −0.0256 | 0.0026 | −10.10 | <0.001 | (−0.0308, −0.0208) |
| Indirect effect | −0.0028 | 0.0007 | −4.24 | <0.001 | (−0.0041, −0.0015) |
Note: Adjusted for age, gender, non‐communicable diseases, smoking, drinking, self‐assessment health, body mass index, activity of daily living, childhood deprivation, telephone connection and hearing impairment.
Sensitivity analyses showed that after including the participants with missing income variable, similar results of model 1 to model 4 were found when the samples changed. In model 4, the participants in the level 4 and level 5 household annual income had an estimate 19% reduced risk of developing elevated depressive symptoms compared with the reference (95% CI, 0.70–0.93; 95% CI, 0.71–0.91), while the participants in the missing group had no significant difference with the reference (Table S3). Binary mediation analysis with bootstrap method showed that social support had significant mediation effect on the relationship between SES and depressive symptoms, and the indirect effect accounted for 10.22% of the total effect (Table S4).
4. DISCUSSION
This study analyzed a nationally representative sample of individuals over 45 years old from 28 provinces, 150 districts/counties, and 450 villages/neighborhood communities. The incidence of elevated depressive symptoms was 42.2% during 7‐year follow‐up of the individuals absent of depressive symptoms at baseline. This finding is consistent with previous studies, which indicated that depression in middle‐aged and elderly people had become a serious public health issue (Rong et al., 2020; Ruiz et al., 2019). To our knowledge, this is the first nationally representative study with relative long time follow up in China that investigated the prospective association between SES and depressive symptoms, as well as the mediation effect of social support on the relationship. Our study confirmed that higher SES had a significant protective effect on the depressive symptoms in individuals aged 45 years and older, and social support partially mediated the association. People with more social support could moderate the negative effect of depression caused by lower SES. Our findings highlighted the importance of increase social support for the middle‐aged and older people, particularly those with lower SES, with the proportion of older people expected to be over 25% in 2050.
The results from the cox proportional hazards regression analyses showed that the risk of developing elevated depressive symptoms for 7 years follow‐up was particularly higher in women than men, in individuals with lower household annual income and lower level of education. Similar to previous studies conducted in other countries (Johnson‐Lawrence et al., 2013; Lorant et al., 2003; Lotfaliany et al., 2019; Ng et al., 2014), these findings suggested important roles of socioeconomic factors in the etiology and pathogenetic mechanism of depression. High incomes enabled individuals to avoid risk factors and harmful exposure (Pescosolido et al., 2010). High education levels could increase the human capacity and personal capital (Montez et al., 2012), and reduce risky behaviors and unhealthy lifestyles, such as physical inactivity and drug abuse (Brunello et al., 2016; Margolis, 2013). Additionally, our results supported that the SES index constructed by the education level and income level illustrated that depressive symptoms and low SES were inextricably linked (Freeman et al., 2016). Higher SES promotes interpersonal connections and social networks to reduce the incidence of depressive symptoms (Zhang et al., 2019). People with lower SES had insufficient access to health care and even routine health care was of worse quality, which is likely to increase the burden of illness and depression (Ng et al., 2014).
This longitudinal study presented that social support was positively related to reduce the risk of developing elevated depressive symptoms, which was in accordance with the previous study (Del‐Pino‐Casado et al., 2017; Hu et al., 2018; Zhong et al., 2020). Studies pointed that older people living alone had significantly higher risk of depression (Lim & Kua, 2011). A dominant hypothesis linking social support and depressive symptoms focuses on the level, frequency, and duration of stressful experiences and the extent to which they are buffered by social supports in the form of emotional, informational, or instrumental resources provided by or shared with others (Allen et al., 2014). Support from the family, community and society, provides more access to information, resources and knowledge to the older people, making them easier to deal with the daily activity stress. Similar to other studies, we found that SES was significantly positive with social support, indicating people with lower SES may not receiving the same stress reducing benefits from social support compared to the individuals with higher SES (Riley & Eckenrode, 1986).
The mediation analyses revealed that the social support had a mediating role on SES and depressive symptoms for the older adults. The mediation effect accounted for about 10% of the total effect, which may partially shed light on the new perspective on the mechanisms through which the SES affects the depressive symptoms. People with low‐SES are more likely to be subjected to stressors and negative life events, and they frequently lack social support due to the considerable socioeconomic disparities in social support (Schafer & Vargas, 2016), which in turn contributes to higher risk of depression. A better understanding of the mediating role of the social support, will allow SES mechanisms to be shaped to either addressing the social support and/or depressive symptoms. Previous studies from other countries found the mediating role of social support in the association between SES and physical health after a twelve‐year follow up among the older women (Matthews et al., 2008), and social support had a non‐linear modifying effect on the relationship between SES and depression for the older people (Ng et al., 2014). However, what we should remember is that social support would not substantially account for the variation in depressive symptoms across the different SES groups (Huurre et al., 2007). Other social causation factors that refer to social relationships that impact on adult mental health, such as labor force participation, emotional support or health selection process arguing that mental health disorders are more likely to drift into low SES may play an important role in the relationship between SES and depressive symptoms (Power et al., 2002), which should be further explored in the future studies. In addition, the subgroup mediation effect analyses showed that gender difference existed in relation to the social support (Shumaker & Hill, 1991), and the mediation effect of social support on older women is higher than older men.
In summary, increasing the social support through a variety of activities could effectively alleviate the social and economic burden of depression in older adults. Depression is the result of complex combination of biological, psychological and social causes, as well as external events (Silva et al., 2016). Joint efforts from the family, community and the government are required to reduce the risk of depression, especially for the lower SES older adults. Family support had been confirmed more important than support from friends (Chou & Chi, 2003), and lowering the likelihood of living alone and boosting interaction with their children/grandchildren for the older adults are all effective measures to enhance the family support. Improving community support, such as building the older people association, and fostering community involvement could help to reduce the depressive symptoms (Hu et al., 2018). Government should emphasis more on the equity in social security and welfare, close the inequalities among people with different levels of SES, and focus on the older people with lower SES to better alleviate the harms caused by depression.
The strengths of our study included the prospective design, the nationally representative, the long follow‐up time, and the inclusion of the mediation effect of SES and depressive symptoms. However, there were some limitations in this study. First, most data including depressive symptoms are based on self‐reported information with no diagnostic verification. Second, the observational nature of our study limited our ability to confirm a causal relationship between SES, social support and depressive symptoms. Third, our study only involved the participants from China, thus the findings may not fully generalize to other low‐and middle‐income countries. Fourth, there were missing participants due to missing information of depressive symptoms and other variables, and for large scale household survey, selection issue was always one of the challenges researchers have to deal with. Our study was conducted based on the whole CHARLS sample, which had been proven that the non‐response appeared to be unrelated to demographic or socioeconomic position. Fifth, due to data limitations, the construction of community and public support indices was based on availability rather than connection, and there was no variable in our data to create family support based on living in a multigenerational family. More scientific and rigorous studies are needed to address these limitations in the future.
5. CONCLUSION
Socioeconomic factors have a significant association with the risk of developing depression symptoms among middle‐aged and elderly people, and the relationship was partially mediated by social support. Social support could be an effective intervention to alleviate the negative effects of lower SES on mental health. Multiple levels of policies or activities should accurately target low‐SES populations, and prompt intervention to enhance social support for this group should be used to reduce the impact of depression on individuals, family and the society as a whole.
CONFLICT OF INTEREST
The authors have no possible conflicts of interest to declare.
AUTHOR CONTRIBUTIONS
Shuduo Zhou and Zhi‐Jie Zheng drafting the manuscript, study design, data analysis and interpretation. Liqun Gao, Fangjing Liu, Wenya Tian, Yinzi Jin: critical revision of article for important intellectual content. Zhi‐Jie Zheng: study concept and design, data analysis and critical revision of article for important intellectual content. All authors gave final approval of the version to be published.
Supporting information
Supporting Information S1
ACKNOWLEDGMENTS
The authors thank the China Health and Retirement Longitudinal Study team for providing data and simple training in using the database. This research is financially supported by Peking University Health Science Center. Grant/Award Number: BMU2018YJ001. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Zhou, S. , Gao, L. , Liu, F. , Tian, W. , Jin, Y. , & Zheng, Z.‐J. (2021). Socioeconomic status and depressive symptoms in older people with the mediation role of social support: A population‐based longitudinal study. International Journal of Methods in Psychiatric Research, 30(4), e1894. 10.1002/mpr.1894
DATA AVAILABILITY STATEMENT
Data are available to the public: http://charls.pku.edu.cn.
REFERENCES
- Allen, J. , Balfour, R. , Bell, R. , & Marmot, M. (2014). Social determinants of mental health. International Review of Psychiatry, 26(4), 392–407. [DOI] [PubMed] [Google Scholar]
- Angkananard, T. , Anothaisintawee, T. , Ingsathit, A. , McEvoy, M. , Silapat, K. , Attia, J. , Sritara, P. , & Thakkinstian, A. (2019). Mediation effect of neutrophil lymphocyte ratio on cardiometabolic risk factors and cardiovascular events. Scientific Reports, 9(1), 2618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barth J., Schumacher M., & Herrmann‐Lingen C. (2004). Depression as a risk factor for mortality in patients with coronary heart disease: A meta‐analysis. Psychosomatic Medicine, 66(6), 802–813. [DOI] [PubMed] [Google Scholar]
- Boey, K. W. (1999). Cross‐validation of a short form of the CES‐D in Chinese elderly. International Journal of Geriatric Psychiatry, 14(8), 608–617. [DOI] [PubMed] [Google Scholar]
- Boss, G. R. , & Seegmiller, J. E. (1981). Age‐related physiological changes and their clinical significance. Western Journal of Medicine, 135(6), 434–440. [PMC free article] [PubMed] [Google Scholar]
- Brunello, G. , Fort, M. , Schneeweis, N. , & Winter‐Ebmer, R. (2016). The causal effect of education on health: What is the role of health behaviors? Health Economics, 25(3), 314–336. [DOI] [PubMed] [Google Scholar]
- Chen, H. , & Mui, A. C. (2014). Factorial validity of the center for epidemiologic studies depression scale short form in older population in China. International Psychogeriatrics, 26, 49–57. [DOI] [PubMed] [Google Scholar]
- Cheng, S. T. , & Chan, A. C. (2005). The center for epidemiologic studies depression scale in older Chinese: Thresholds for long and short forms. International Journal of Geriatric Psychiatry, 20(5), 465–470. [DOI] [PubMed] [Google Scholar]
- Chou, K. L. , & Chi, I. (2003). Reciprocal relationship between social support and depressive symptoms among Chinese elderly. Aging & Mental Health, 7(3), 224–231. [DOI] [PubMed] [Google Scholar]
- Del‐Pino‐Casado, R. , Palomino‐Moral, P. A. , Pastor‐Bravo, M. D. M. , & Frías‐Osuna, A. (2017). Determinants of depression in primary caregivers of disabled older relatives: A path analysis. BMC Geriatrics, 17(1), 274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fang, M. , Mirutse, G. , Guo, L. , & Ma, X. (2019). Role of socioeconomic status and housing conditions in geriatric depression in rural China: A cross‐sectional study. BMJ Open, 9(5), e024046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Faramarzi, M. , Hosseini, S. , Cumming, R. , Kheirkhah, F. , Parsaei, F. , Ghasemi, N. , & Bijani, A. (2015). A negative association between social support and depression in the elderly population of Amirkola City. British Journal of Medicine and Medical Research, 8(8), 707–716. [Google Scholar]
- Freeman, A. , Tyrovolas, S. , Koyanagi, A. , Chatterji, S. , Leonardi, M. , Ayuso‐Mateos, J. L. , Tobiasz‐Adamczyk, B. , Koskinen, S. , Rummel‐Kluge, C. , & Haro, J. M. (2016). The role of socio‐economic status in depression: Results from the COURAGE (aging survey in Europe). BMC Public Health, 16(1), 1098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gallo, L. C. , & Matthews, K. A. (2003). Understanding the association between socioeconomic status and physical health: Do negative emotions play a role? Psychological Bulletin, 129, 10–51. [DOI] [PubMed] [Google Scholar]
- Geckova, A. , van Dijk, J. P. , Stewart, R. , Groothoff, J. W. , & Post, D. (2003). Influence of social support on health among gender and socio‐economic groups of adolescents. The European Journal of Public Health, 13, 44–50. [DOI] [PubMed] [Google Scholar]
- Gunzler, D. , Chen, T. , Wu, P. , & Zhang, H. (2013). Introduction to mediation analysis with structural equation modeling. Shanghai Archives of Psychiatry, 25(6), 390–394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harrison, L. A. , Kats, A. , Williams, M. E. , & Aziz‐Zadeh, L. (2019). The importance of sensory processing in mental health: A proposed addition to the research domain criteria (RDoC) and suggestions for RDoC 2.0. Frontiers in Psychology, 10, 103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu, H. , Cao, Q. , Shi, Z. , Lin, W. , Jiang, H. , & Hou, Y. (2018). Social support and depressive symptom disparity between urban and rural older adults in China. Journal of Affective Disorders, 237, 104–111. [DOI] [PubMed] [Google Scholar]
- Hu, Y. , Li, P. , & Martikainen, P. (2019). Rural‐urban disparities in age trajectories of depression caseness in later life: The China Health and Retirement Longitudinal Study. PloS One, 14(4), e0215907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huurre, T. , Eerola, M. , Rahkonen, O. , & Aro, H. (2007). Does social support affect the relationship between socioeconomic status and depression? A longitudinal study from adolescence to adulthood. Journal of Affective Disorders, 100(1–3), 55–64. [DOI] [PubMed] [Google Scholar]
- Johnson‐Lawrence, V. , Griffith, D. M. , & Watkins, D. C. (2013). The effects of race, ethnicity, and mood/anxiety disorders on the chronic physical health conditions of men from a national sample. American Journal of Men's Health, 7(4 Suppl), 58S–67S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Katsarou, A. , Tyrovolas, S. , Psaltopoulou, T. , Zeimbekis, A. , Tsakountakis, N. , Bountziouka, V. , Gotsis, E. , Metallinos, G. , Polychronopoulos, E. , Lionis, C. , & Panagiotakos, D. (2010). Socio‐economic status, place of residence and dietary habits among the elderly: The Mediterranean Islands study. Public Health Nutrition, 13(10), 1614–1621. [DOI] [PubMed] [Google Scholar]
- Lei, X. , Sun, X. , Strauss, J. , Zhang, P. , & Zhao, Y. (2014). Depressive symptoms and SES among the mid‐aged and elderly in China: Evidence from the China Health and Retirement Longitudinal Study national baseline. Social Science & Medicine, 120, 224–232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li, H. , Zheng, D. , Li, Z. , Wu, Z. , Feng, W. , Cao, X. , Wang, J. , Gao, Q. , Li, X. , Wang, W. , Hall, B. J. , Xiang, Y.‐T. , & Guo, X. (2019). Association of depressive symptoms with incident cardiovascular diseases in middle‐aged and older Chinese adults. JAMA Network Open, 2(12), e1916591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li, L. W. , Liu, J. , Zhang, Z. , & Xu, H. (2015). Late‐life depression in rural China: Do village infrastructure and availability of community resources matter? International Journal of Geriatric Psychiatry, 30(7), 729–736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lim, L. L. , & Kua, E. H. (2011). Living alone, loneliness, and psychological well‐being of older persons in Singapore. Current Gerontology and Geriatrics Research, 2011, 673181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu, Q. , Cai, H. , Yang, L. H. , Xiang, Y.‐B. , Yang, G. , Li, H. , Gao, Y.‐T. , Zheng, W. , Susser, E. , & Shu, X.‐O. (2018). Depressive symptoms and their association with social determinants and chronic diseases in middle‐aged and elderly Chinese people. Scientific Reports, 8(1), 3841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu, Y. , Liu, G. , Wu, H. , Jian, W. , Wild, S. H. , & Gasevic, D. (2017). Sex differences in non‐communicable disease prevalence in China: A cross‐sectional analysis of the China health and retirement longitudinal study in 2011. BMJ Open, 7(12), e017450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lorant, V. , Deliege, D. , Eaton, W. , Robert, A. , Philippot, P. , & Ansseau, M. (2003). Socioeconomic inequalities in depression: A meta‐analysis. American Journal of Epidemiology, 157(2), 98–112. [DOI] [PubMed] [Google Scholar]
- Lotfaliany, M. , Hoare, E. , Jacka, F. N. , Kowal, P. , Berk, M. , & Mohebbi, M. (2019). Variation in the prevalence of depression and patterns of association, sociodemographic and lifestyle factors in community‐dwelling older adults in six low‐and middle‐income countries. Journal of Affective Disorders, 251, 218–226. [DOI] [PubMed] [Google Scholar]
- MacKinnon, D. (2008). Introduction to statistical mediation analysis. Lawrence Erlbaum Associates. [Google Scholar]
- Margolis, R. (2013). Educational differences in healthy behavior changes and adherence among middle‐aged Americans. Journal of Health and Social Behavior, 54(3), 353–368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mathers, C. D. , & Loncar, D. (2006). Projections of global mortality and burden of disease from 2002 to 2030. PLoS Medicine, 3(11), e442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Matthews, K. A. , Räikkönen, K. , Gallo, L. , & Kuller, L. H. (2008). Association between socioeconomic status and metabolic syndrome in women: Testing the reserve capacity model. Health Psychology, 27, 576–583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Matthews, S. , Stansfeld, S. , & Power, C. (1999). Social support at age 33: The influence of gender, employment status and social class. Social Science & Medicine, 49, 133–142. [DOI] [PubMed] [Google Scholar]
- Mcdougall, M. A. , Walsh, M. , Wattier, K. , Knigge, R. , Miller, L. , Stevermer, M. , & Fogas, B. S. (2016). The effect of social networking sites on the relationship between perceived social support and depression. Psychiatry Research, 246, 223–229. [DOI] [PubMed] [Google Scholar]
- Mickelson, K. D. , & Kubzansky, L. D. (2003). Social distribution of social support: The mediating role of life events. American Journal of Community Psychology, 32, 265–281. [DOI] [PubMed] [Google Scholar]
- Miech, R. A. , & Shanahan, M. J. (2000). Socioeconomic status and depression over the life course. Journal of Health and Social Behavior, 41, 162–176. [Google Scholar]
- Montez, J. K. , Hummer, R. A. , & Hayward, M. D. (2012). Educational attainment and adult mortality in the United States: A systematic analysis of functional form. Demography, 49(1), 315–336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ng, C. W. , Tan, W. S. , Gunapal, P. P. , Wong, L. Y. , & Heng, B. H. (2014). Association of socioeconomic status (SES) and social support with depressive symptoms among the elderly in Singapore. Annals Academy of Medicine Singapore, 43(12), 576–587. [PubMed] [Google Scholar]
- Osby, U. , Brandt, L. , Correia, N. , Ekbom, A. , & Sparén P. (2001). Excess mortality in bipolar and unipolar disorder in Sweden. Archives of General Psychiatry, 58, 844–850. [DOI] [PubMed] [Google Scholar]
- Pescosolido, B. A. , Martin, J. K. , McLeod, J. D. , & Rogers, A. (Eds.). (2010). Handbook of the sociology of health, illness, and healing: A blueprint for the 21st century. Springer Science & Business Media. [Google Scholar]
- Power, C. , Stansfeld, S. A. , Matthews, S. , Manor, O. , & Hope, S. (2002). Childhood and adulthood risk factors for socio‐economic differentials in psychological distress: Evidence from the 1958 British birth cohort. Social Science & Medicine, 55(11), 1989–2004. [DOI] [PubMed] [Google Scholar]
- Quashie, N. T. , Arpino, B. , Antczak, R. , & Mair, C. A. (2021). Childlessness and health among older adults: Variation across five outcomes and 20 countries. Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 76(2), 348–359. [DOI] [PubMed] [Google Scholar]
- Riley, D. , & Eckenrode, J. (1986). Social ties: Subgroup differences in costs and benefits. Journal of Personality and Social Psychology, 51(4), 770–778. [DOI] [PubMed] [Google Scholar]
- Rong, H. , Lai, X. , Jing, R. , Wang, X. , Fang, H. , & Mahmoudi, E. (2020). Association of sensory impairments with cognitive decline and depression among older adults in China. JAMA Network Open, 3(9), e2014186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruiz, M. , Hu, Y. , Martikainen, P. , & Bobak, M. (2019). Life course socioeconomic position and incidence of mid‐late life depression in China and England: A comparative analysis of CHARLS and ELSA. Journal of Epidemiology & Community Health, 73(9), 817–824. [DOI] [PubMed] [Google Scholar]
- Schafer, M. H. , & Vargas, N. (2016). The dynamics of social support inequality: Maintenance gaps by socioeconomic status and race? Social Forces, 94(4), 1795–1822. [Google Scholar]
- Shumaker, S. A. , & Hill, D. R. (1991). Gender differences in social support and physical health. Health Psychology, 10(2), 102–111. [DOI] [PubMed] [Google Scholar]
- Silva, M. , Loureiro, A. , & Cardoso, G. (2016). Social determinants of mental health: A review of the evidence. European Journal of Psychiatry, 30(4), 259–292. [Google Scholar]
- Sivertsen, H. , Bjørkløf, G. H. , Engedal, K. , Selbæk, G. , & Helvik, A.‐S. (2015). Depression and quality of life in older persons: A review. Dementia and Geriatric Cognitive Disorders, 40(5–6), 311–339. [DOI] [PubMed] [Google Scholar]
- Turner, R. J. , Wheaton, B. , & Lloyd, D. A. (1995). The epidemiology of social stress. American Sociological Review, 60, 104–125. [Google Scholar]
- UNFPA . (2020, May 15). UNFPA and Helpage international ageing. https://www.unfpa.org/ageing [Google Scholar]
- von Elm, E. , Altman, D. G. , Egger, M. , Pocock, S. J. , Gøtzsche, P. C. , & Vandenbroucke, J. P. (2007). The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Annals of Internal Medicine, 147(8), 573–577. [DOI] [PubMed] [Google Scholar]
- Wang, L. , Zhong, W. , Ji, X. , & Chen, J. (2016). Depression, caregiver burden and social support among caregivers of retinoblastoma patients in China. International Journal of Nursing Practice, 22(5), 478–485. [DOI] [PubMed] [Google Scholar]
- Wang, Z. , Yang, H. , Guo, Z. , Liu, B. , & Geng, S. (2019). Socio‐demographic characteristics and co‐occurrence of depressive symptoms with chronic diseases among older adults in China: The China longitudinal ageing social survey. BMC Psychiatry, 19(1), 1–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whiteford, H. A. , Ferrari, A. J. , Degenhardt, L. , Feigin, V. , & Vos, T. (2015). The global burden of mental, neurological and substance use disorders: An analysis from the global burden of disease study 2010. PloS One, 10(2), e0116820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization. (2017). Depression and other common mental disorders: Global health estimates. World Health Organization. [Google Scholar]
- Yang, L. , Jia, C. X. , & Qin, P. (2015). Reliability and validity of the Center for Epidemiologic Studies Depression Scale (CES‐D) among suicide attempters and comparison residents in rural China. BMC Psychiatry, 15, 76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang, J. , Hu, H. , Hennessy, D. , Zhao, S. , & Zhang, Y. (2019). Digital media and depressive symptoms among Chinese adolescents: A cross‐sectional study. Heliyon, 5(5), e01554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhao, Y. , Hu, Y. , Smith, J. P. , Strauss, J. , & Yang, G. (2014). Cohort profile: The China health and retirement longitudinal study (CHARLS). International Journal of Epidemiology, 43(1), 61–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhong, Y. , Wang, J. , & Nicholas, S. (2020). Social support and depressive symptoms among family caregivers of older people with disabilities in four provinces of urban China: The mediating role of caregiver burden. BMC Geriatrics, 20(1), 3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhou, S. , Song, S. , Jin, Y. , & Zheng, Z. J. (2020). Prospective association between social engagement and cognitive impairment among middle‐aged and older adults: Evidence from the China health and retirement longitudinal study. BMJ Open, 10(11), e040936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zurlo, K. A. , Hu, H. , & Huang, C. (2014). The effects of family, community, and public policy on depressive symptoms among elderly Chinese. Journal of Sociology and Social Work, 2(2), 1–23. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting Information S1
Data Availability Statement
Data are available to the public: http://charls.pku.edu.cn.