

Abstract
Objective:
To compare the clinical complications during treatment with either a removable mandibular acrylic splint (RMS) or with a cantilever (HC) Herbst appliance.
Methods:
Records from 159 Class II, division 1, consecutively treated patients with a Herbst appliance were examined. The sample was composed of 82 male and 77 female patients with a mean age of 11.8 years. The Herbst appliance was used for a mean of 12 months (standard deviation 2.15 months). Two main Herbst groups were analyzed: group RMS (n = 125) and group HC (n = 34). They were further subdivided according to the telescopic system used (Dentaurum type 1 or PMA) and fixation mode (splint with crowns or Grip Tite bands). Patients' clinical records were assessed to identify clinical complications.
Results:
The incidence of complications during treatment was 85.3% for the HC group and 88.0% for the RMS group, with no statistically significant difference (Mann-Whitney test, P > .05). The fixation mode (crown or band) also did not show a statistically significant difference (P > .05). Regarding the telescopic system used, the Dentaurum group had 2.9 times more susceptibility to complications than the PMA group, regardless of the Herbst type.
Conclusions:
On average, approximately 2.5 complications per patient were reported. Most patients had a maximum of three complications during Herbst treatment. Herbst appliance type (RMS or HC) and fixation mode (crowns or Grip Tite bands) did not influence the number of complications. The PMA (without screws) telescopic system seemed to be more reliable (regarding the number of complications) than Dentaurum type 1, regardless of the appliance design (RMS or HC).
Keywords: Herbst appliance, Angle Class II, Complications
INTRODUCTION
The Herbst appliance is the most frequently used functional appliance for the correction of Class II malocclusion.1 This fixed appliance permanently locates the lower jaw in a more anterior position. The forces generated by the telescopic component during Herbst treatment are believed to be responsible not only for the desired therapeutic effect but also for many complications associated with the device during the treatment period, such as lower splint breakage, band or crown fracture or debonding, screw loosening, rod distortion, pivot breakage, and soft tissue injuries.2
Many different Herbst appliance designs have been reported in the literature.3–7 Depending on the type of appliance that is used, different complications are more commonly reported. A few studies2,8–10 have compared complication rates between different Herbst appliance designs. To the best of our knowledge, no studies have been conducted to compare complications in different Herbst telescopic systems.
The aim of this study is to assess the number of complications occurring during treatment and to compare the incidence of clinical complications during treatment between lower cantilever (HC) and removable mandibular acrylic splint (RMS) Herbst designs while simultaneously considering different telescopic systems and fixation modes.
MATERIALS AND METHODS
The research protocol was approved by the Institutional Review Board of Positivo University.
The records of 159 Class II, division 1, malocclusion patients consecutively treated (between 1998 and 2010) with a Herbst appliance were examined. All these patients were treated by the same clinician in a private orthodontic office in Curitiba, Brazil. The sample comprised 82 male and 77 female patients with a mean age of 11 years, 8 months (standard deviation [SD] 2 years, 5 months; range, 8 to 16.7 years) when initial records were collected.
The sample was divided into two main groups:
Group RMS consisted of 125 Caucasian patients (65 male and 60 female) with a mean age of 11 years, 4 months (SD, 2 years, 3 months). These patients were treated with the Herbst appliance with stainless steel crowns (Ormco, Glendora, Calif) or Grip Tite bands (TP Orthodontics, La Porte, Ind) on the maxillary first molars and removable mandibular acrylic splint (Figure 1). A transpalatal arch connected the maxillary first molars.
Group HC consisted of 34 patients (17 male and 17 female) with a mean age of 11 years, 8 months (SD, 2 years, 5 months). These appliances were made in house and consisted of four stainless steel crowns (Ormco) on the first upper and lower molars. A transpalatal arch connected the maxillary molars. A lingual arch with occlusal stops on the lower first premolars connected the lower first molars. The cantilever was made with half-round 1.74 × 0.875-mm stainless steel wire (Figure 2). The lower axle was placed at the mesial end of the cantilever between the first and second premolars.
Figure 1.
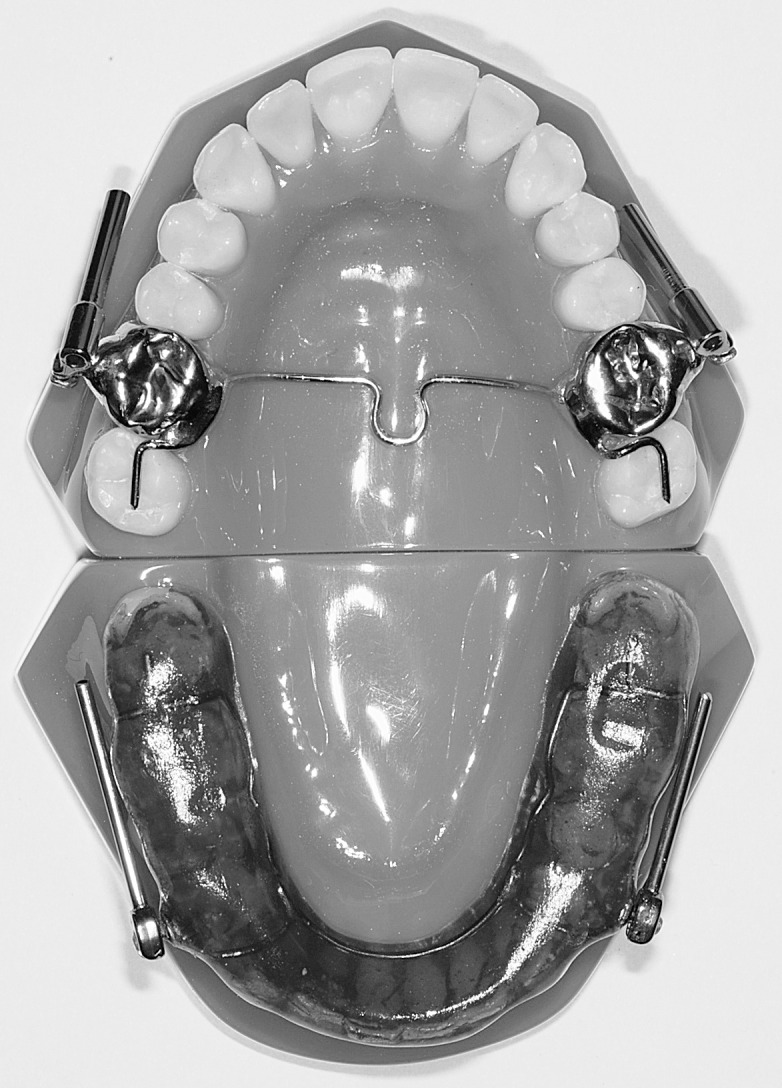
Herbst appliance with stainless steel crowns (Ormco) on the maxillary first molars and removable mandibular acrylic splint.
Figure 2.

Herbst appliance with four stainless steel crowns (Ormco) on the first upper and lower molars.
Both groups were then subdivided with respect to the telescopic system and fixation method used. Either a Dentaurum type 1 (Dentaurum, Ispringen, Germany) or a PMA (3M Unitek/Abzil, São José do Rio Preto, SP, Brazil) telescopic system was used (Figures 3 and 4). With regard to fixation mode, either a splint with stainless steel crowns or Grip Tite bands (TP Orthodontics) were used. The distribution of the sample according to this classification is shown in Figure 5.
Figure 3.

PMA telescopic System (3M Unitek/Abzil).
Figure 4.

Dentaurum type 1 telescopic system (Dentaurum).
Figure 5.

Distribution of groups according to the type, telescopic system, and fixation mode of the Herbst appliance.
For all patients, the Herbst appliance was activated initially to an edge-to-edge incisor relationship and was used for a mean of 12 months (SD 2.15 months; range, 10 to 18 months). No dropouts occurred during the first treatment phase (Herbst). Sixteen dropouts occurred during the fixed appliance phase. A few patients removed the Herbst before reaching 12 months owing to success of the correction, and others wore the appliance for longer than 12 months because of complications that delayed treatment. The steel crowns and bands were cemented with Fuji Ortho LC (GC America Inc, Chicago, Ill). In all patients, an overcorrected Class I molar relationship was achieved before the Herbst appliance was removed.
Instructions regarding appliance care were essentially the same for both groups. Patients were to avoid eating hard or sticky foods, and those who used the splint were to remove it only for tooth brushing.
Data of any clinical complications that occurred during treatment with the Herbst appliance were collected from the patients' clinical records (Table 1).
Table 1.
Clinical Complications During the Use of Different Herbst Appliances

All statistical analyses were conducted using IBM SPSS version 20.0, with P values < .05 considered significant. Quantitative outcome variables were reported as means, medians, SDs, and minimal and maximum values. Qualitative variables were reported as frequencies and percentages. Normality of data distribution was not satisfied for each group. Therefore, nonparametric statistical tests were used.
For the variables incidence and complication type, treatment groups were compared using Fisher's exact test or the chi-square test. To compare the total number of complications during treatment considering Herbst appliance design, telescopic systems used, and fixation mode used, a Mann-Whitney U-test was applied. With “no or at least one complication during treatment” considered a dichotomous variable and “type of appliance,” “telescopic system,” and “fixation mode” as factors, a multivariate analysis was performed with an adjusted logistic regression model and using the Wald test.
RESULTS
The total number of complications found in the patients' clinical records was 80 for the HC group (34 patients) and 316 for the RMS group (125 patients). Thirteen types of complications occurred: lesion in palate caused by transpalatal arch, lesion in cheek caused by long rod, screw loosening, crown debonding, rod distortion, crown fracture, mucosal injury caused by lingual arch, lesion in cheek caused by cantilever screw, rod loosening, lower splint breakage, poor use of splint (lack of use), pivot breakage, and transpalatal arch breakage. The incidence of patients exhibiting complications according to the type of appliance, telescopic system, and fixation mode is shown in Table 2.
Table 2.
Incidence of Complications (Number and Percentage) During Herbst Appliance Treatment According to Type of Appliance, Telescopic System, and Fixation Mode

Table 3 depicts the type, number (frequency), and percentage of complications in the HC and RMS groups. Evaluation of the total number of complications during Herbst appliance treatment is shown in Table 4. There was no statistically significant difference in the total number of complications according to appliance type, telescopic system, and fixation mode used when each factor was considered individually (all P > .05; Mann-Whitney U-test).
Table 3.
Type and Number of Instances of Complications for the HC and RMS Herbst Appliancesa

Table 4.
Comparisons of Total Number of Complications During Herbst Appliance Treatment According to the Types of Appliance, Telescopic System, and Fixation Mode

Table 5 describes the simultaneous effects of the three appliance design variables (appliance type, telescopic system, fixation mode used) through the multivariate analysis. The only statistically significant difference was found for the telescopic system used (P = .037; Wald test). The Dentaurum type 1 telescopic system had 2.9 times more susceptibility to complications than the PMA system, regardless of the type of appliance and/or fixation mode.
Table 5.
Number of Complications (%), Odds Ratios (ORs), and Confidence Intervals (CIs) of the Multivariate Analysis According to Type of Appliance, Telescopic System, and Fixation Mode

When comparing patients in the HC group who used the PMA telescopic system with those who used the Dentaurum system, it was found that the mean number of complications in the Dentaurum group was higher (3.2) than the mean in the PMA group (1.8) (P = .0024; Mann-Whitney U-test). When comparing patients in the RMS group who used the PMA telescopic system with those who used Dentaurum, no significant difference was found in the average total number of complications during treatment (2.7 for PMA and 2.5 for Dentaurum, P = .893; Mann-Whitney U-test). When comparing patients in RMS group who used bands with those who used crowns, no significant difference was found for the average number of complications (2.5 for crowns and 2.7 for bands, P = .702; Mann-Whitney U-test).
Table 6 groups the number of complications into intervals of zero or one, two to three, and more than three, per appliance type. No differences were found (P = .794; chi-square test).
Table 6.
Distribution (in %) of Patients Exhibiting 0–1, 2–3, or >3 Complications During Treatment with the Herbst Appliance, Evaluated by Chi-Square Test*

DISCUSSION
Many Herbst appliance designs are available today. The amount of available information from manufacturers for the orthodontist makes the choice of design a difficult task. All companies claim that their system has many advantages over the other systems.
One of the most important considerations when selecting an orthodontic appliance is the frequency of complications and the potential financial and time-related implications for both for the orthodontist and the patient. As stated earlier, many different Herbst appliance designs have been reported in the literature.3–7 Only a handful of studies2,8–10 have specifically compared the complication rates between different Herbst appliance designs; none have evaluated the actual financial cost of these complications. Although these studies2,8–10 reported Herbst-related complications, no studies have yet compared complications in different Herbst telescopic systems.
When we assessed the incidence of complications, it was observed that in about 15% of the HC group and 12% of the RMS group, no complications occurred. In other words, the frequency of complications is worrisome, with percentages around 85% of all treated cases; the average frequency of complications is around 2.5 per patient during treatment.
In a study comparing the Cantilever Bite Jumper (CBJ, Ormco) with RMS, Moro et al.2 found that 33% of patients treated with CBJ and 14% of patients treated with RMS had no complications. In their study, Hägg et al.8 found that 14% treated with a metallic splint and 21% treated with bands had no complications. Finally, Sanden et al.9 found that 33% of patients who used the Herbst with bands and 40% of patients who used a metallic splint had no complications during treatment. Although there is some variability in the reported frequency of complications, it can be summarized that, in terms of the incidence of complications, the different designs of Herbst appliances did not show great variation. Simultaneously, it can be stated that it is relatively usual that most patients with a Herbst appliance will experience some kind of complication during treatment.
In terms of the total number of complications per patient during Herbst treatment, we observed an average of 2.4 per patient with HC and an average of 2.5 per patient with RMS (no statistically significant difference). This result is in contrast to the findings of Moro et al.,2 who reported an average of 1.1 complications per patient with CBJ and an average of 2.5 complications per patient with RMS, a statistically significant difference. Hägg et al.8 found an average of 3.7 complications per patient with the Herbst appliance with metallic splint and an average of 2.9 complications per patient with Herbst with bands, which was suggestive of no difference. Finally, Sanden et al.9 observed an average of 2.8 complications per patient treated with Herbst with bands and an average of 2.1 complications per patient treated with the Herbst with metallic splint. These data showed that the average number of complications in this study was not different than the average reported by other studies that evaluated complications with Herbst appliances, except for the study of Moro et al.2 using the CBJ. This may indicate that the CBJ is very sturdy.
When evaluating individual occurrences of the most common complications in both groups, it was observed that, in the HC group, on 16 occasions (35.3%) screw loosening occurred, and rod distortion occurred 15 times (29.4%). In the RMS group, on 90 occasions (43.2%) screw loosening occurred, and breakage of the acrylic was seen 57 times (34.4%) (Table 3). In the study of Moro et al.,2 the CBJ group showed 6 occurrences of displacement of the crown and screw loosening, while in the splint group, 24 instances of screw loosening were seen. To explain this higher incidence, it may be speculated that the repeated removal and reinsertion of the splint (after meals to facilitate oral hygiene) may end up forcing the telescopic system and facilitating screw loosening. To avoid loosening of the screws, some authors11,12 have recommended the use of a glue (Ceka Bond, Preat Corporation, Santa Ynez, Calif) before fixing the screw. However, this was not used in the sample reported in this study or by Moro et al.2 One might assume that appliance reactivations could influence the study results; however, these were rare, because most appliances could be advanced only one step at a time into an edge-to-edge incisor relationship. The splint group did not require unscrewing of the telescopic system to place the spacers (shims). In the cantilever group, only 13 patients used the Dentaurum system with screws.
Another very frequent occurrence previously found was fracture of the lower splint on 13 occasions. This happened even though the devices were made with a reinforcing wire for lingual mandibular anterior teeth and the acrylic was thicker in the anterior splint.2
Schiöth et al.,10 when comparing complications with the use of a total metal splint (canines to molars) or a reduced metal splint (canines to second premolars), divided their sample into four categories according to the frequency of complications: low frequency (1–3 complications), moderate frequency (4–6 complications), high frequency (7–10 complications), and very high frequency (more than 10 complications). Most of the patients had a low frequency of complications, while only around 10% of patients in both groups had a high frequency of complications. Sanden et al.9 found that 55% of patients experienced between 1 and 3 complications, 29% had 4 to 6, 13% suffered 7 to 10, and 3% experienced more than 10 instances of complications. Moro et al.2 divided patients into three groups—none or one, two or three, or more than three complications—during treatment with the Herbst appliance. In the CBJ group, no individual patient experienced more than three complications, which showed a relatively better clinical performance of the device.2 In the splint group, 33% of patients had more than three complications during treatment, and the maximum number of six was observed in two patients.2 In this study, 35.2% of patients in the HC group and 32.8% in the RMS group had no or one complication. More than three complications were seen in 29.4% of HC patients and in 25.6% of the RMS group; however, the differences were not statistically significant. When comparing the results of this study with other findings reported in the literature, it can be concluded that most patients experience a maximum of three complications during Herbst treatment. This is disturbing, as this generates additional appointments for the patients, with associated discomfort, loss of work hours and time, and additional financial cost to the orthodontic office and/or patient's family.
The variable “having at least one complication during treatment” was considered as the response variable and the factors “appliance,” “system,” and “fixing” were used as explanatory variables in an adjusted logistic regression model, controlling for the age of patient. The results indicated that, regardless of the patient's age, the type of device, and the type of attachment, the Dentaurum system significantly increased the probability of the patient having at least one complication during treatment. The odds ratio indicated that a patient with the Dentaurum system was 2.9 times more likely to have at least one complication than a patient with the PMA system. This difference was probably caused by the increased chance of loosening the screws that hold the telescopic system.
Despite the clinical perception that the reinforced band would be weaker than the stainless steel crowns, no significant difference was found when patients who used the Herbst appliance with reinforced bands were compared with those who used the appliances with stainless steel crowns.
A Herbst appliance with a cantilever, from a clinical viewpoint, would seem to be more resistant than a Herbst appliance with a lower removable splint, as its perceived disadvantages include a tendency of the lower cantilever to sink, causing molar inclination; the possibility of rod distortion; and the tendency of the lower pivot to hurt the patient's cheek during the first week of use. On the other hand, the advantages of the Herbst appliance with lower removable splint are its affordability, the ability to remove it to brush teeth (facilitating hygiene), easier fit for patients, and a shorter learning curve for professionals. The disadvantages, observed clinically with the Herbst appliance with splint, are that the lower acrylic splint shows decreased resistance, there is a tendency to open the bite in the posterior regions because of the relative intrusion on the posterior teeth by the acrylic, and some patients tend not to cooperate.
In the office from which the samples are obtained, the decision to use Herbst with cantilever done in an in-office laboratory was based on the assumption that this would decrease its price versus the CBJ from Ormco, which is fabricated at a commercial laboratory. However, the results of these studies seem to indicate that the CBJ manufactured by Ormco is stronger than the HC manufactured in the laboratory of this specific private office. This information should not be extrapolated to other offices, as the skill of the technician and/or the clinician can vary significantly in different locations.
CONCLUSIONS
The type of Herbst appliance (RMS or HC) and the fixation mode (crowns or Grip Tite bands) did not influence the frequency of complications during Herbst treatment.
The PMA (without screws) telescopic system seems to be more reliable (regarding the number of complications) than the Dentaurum type 1 system for Herbst treatment, regardless of the appliance design (RMS or HC).
Approximately 2.5 complications per patient were reported. Most patients have a maximum of three complications during Herbst treatment with the evaluated designs.
REFERENCES
- 1.Keim RG, Gottlieb EL, Nelson AH, Vogels DS. 2002 JCO study of orthodontic diagnosis and treatment procedures: part 1, results and trends. J Clin Orthod. 2008;42:625–640. [PubMed] [Google Scholar]
- 2.Moro A, Janson G, Moresca R, Freitas MR de, Henriques JFC. Comparative study of complications during Herbst treatment with Cantilever Bite Jumper and removable mandibular acrylic splint. Dental Press J Orthod. 2011;16:e1–e10. [Google Scholar]
- 3.Pancherz H. Treatment of Class II malocclusion by jumping the bite with the Herbst appliance: a cephalometric investigation. Am J Orthod. 1979;76:423–442. doi: 10.1016/0002-9416(79)90227-6. [DOI] [PubMed] [Google Scholar]
- 4.Wieslander L. Intensive treatment of severe Class II malocclusions with a headgear-Herbst appliance in the early mixed dentition. Am J Orthod. 1984;86:1–13. doi: 10.1016/0002-9416(84)90271-9. [DOI] [PubMed] [Google Scholar]
- 5.Valant JR, Sinclair PM. Treatment effects of the Hersbt appliance. Am J Orthod Dentofacial Orthop. 1989;95:138–147. doi: 10.1016/0889-5406(89)90392-2. [DOI] [PubMed] [Google Scholar]
- 6.McNamara JA, Jr, Howe R, Dischinger T. A comparison of the Herbst and Fränkel appliances in the treatment of Class II malocclusion. Am J Orthod Dentofacial Orthop. 1990;98:134–144. doi: 10.1016/0889-5406(90)70007-Y. [DOI] [PubMed] [Google Scholar]
- 7.Moro A, Janson G, Freitas MR, Henriques JFC, Petrelli NE, Lauris JP. Class II correction with the Cantilever Bite Jumper. A variant of the Herbst. Angle Orthod. 2009;79:221–229. doi: 10.2319/121807-591.1. [DOI] [PubMed] [Google Scholar]
- 8.Hägg U, Tse ELK, Rabie ABM, Robinson W. A comparison of splinted and banded Herbst appliances: treatment changes and complications. Aust Orthod J. 2002;18:76–81. [PubMed] [Google Scholar]
- 9.Sanden E, Pancherz H, Hansen K. Complications during Herbst appliance treatment. J Clin Orthod. 2004;38:130–133. [PubMed] [Google Scholar]
- 10.Schiöth T, Bremen JV, Pancherz H, Ruf S. Complications during Herbst appliance treatment with reduced mandibular cast splints. J Orofac Orthop. 2007;68:321–327. doi: 10.1007/s00056-007-0703-4. [DOI] [PubMed] [Google Scholar]
- 11.Noble PSA. Clinical Management of Crown/Banded Bite Jumping Herbst Appliances 4th ed. Sturtevant: Allesee Orthodontic Appliances; 1999. [Google Scholar]
- 12.Rogers MB. Troubleshooting the Herbst appliance. J Clin Orthod. 2002;36:268–274. [PubMed] [Google Scholar]