

Abstract
Objective:
The objective of this study was to determine the availability and national distribution of HIV testing and counseling at substance use treatment facilities in the United States.
Methods:
Analysis of the 2018 National Survey of Substance Abuse Treatment Services assessed HIV testing and counseling availability in US substance use treatment facilities (excluding territories). Facilities were subcategorized by availability of mental health services and medication for opioid use disorders, and subsequently compared using logistic models. Descriptive statistics were calculated to characterize the availability of HIV testing and counseling by state, background HIV incidence, and facility characteristics.
Results:
Among US Substance Use Treatment Facilities (N=14,691), 29% offered HIV testing, 53% offered HIV counseling, 23% offered both, and 41% offered neither. State proportions of facilities offering HIV testing and counseling ranged from 9.0%–62.8% and 19.2%–83.3%, respectively. Only three states reported HIV testing being offered by ≥50% of facilities. Sites offering medication for opioid use disorder (48.0% vs. 16.0%, respectively) or mental health services (31.2% vs. 24.1%, respectively) were significantly more likely to offer HIV testing than other sites.
Conclusion:
Only 3 in 10 substance use treatment facilities offered HIV testing in 2018. This is a missed opportunity for early identification of HIV among people receiving treatment for substance use disorders.
Introduction
To improve early identification, treatment, and prevention of HIV, the Centers for Disease Control and Prevention (CDC) revised their HIV testing recommendations in 2006 to include routine HIV testing for all patients between ages 13–64 years, marking a shift away from risk-based testing (1). In 2013, the United States Preventive Services Task Force (USPSTF) also recommended routine HIV testing for patients aged 15–64 years (2). This recommendation was important, as USPSTF guidelines have implications for reimbursement. Unfortunately, these recommendations have not been consistently implemented across health care settings. Physicians often cite insufficient time, stigma, consent burden, competing priorities, and reimbursement concerns as barriers to HIV testing (3).
Substance use treatment facilities are uniquely positioned to improve early identification, treatment, and prevention of HIV (4), as they serve a high-risk population. Drug and alcohol use are broadly associated with increased HIV risk behaviors, including higher risk sexual and injection drug behaviors (5).
These facilities may play an especially important role in diagnosing HIV among the 25% of people with serious mental illness who have comorbid substance use disorders (6), nearly 30% of whom seek substance use treatment services (6). People with serious mental illness are up to ten times as likely to have HIV as the general US population (7), and people living with HIV and serious mental illness are more likely to experience increased HIV-related morbidity and mortality from decreased receipt of antiretroviral treatment and lower rates of viral suppression (8–10). Despite this high prevalence and poorer HIV treatment outcomes, HIV testing among this population remains quite low (11).
Before the 2006 CDC guidelines, fewer than 30% of US substance use treatment facilities offered HIV testing and counseling (12). The primary objective of this study was to estimate current HIV testing and counseling availability in US-based substance use treatment facilities and characterize state-to-state variation. The second objective was to assess HIV testing availability at facilities serving subpopulations at particularly high risk for HIV: those providing medication for opioid use disorder or mental health services.
Methods
Data Sources:
The National Survey of Substance Abuse Treatment Services (NSSATS) is an annual Substance Abuse and Mental Health Services Administration (SAMHSA) nationwide survey of drug and alcohol treatment facilities. The 2018 survey was sent to 16,365 eligible facilities across the US, including the District of Columbia and territories, with a response rate of 92% (170 respondents were deemed to represent facilities that were out-of-scope, and thus were excluded). The present study includes facilities that responded to the survey and were located in all 50 states and the District of Columbia (n=14,691), excluding those in territories. Background HIV incidence data for each state the year prior (2017) was obtained from the Centers for Disease Control’s 2018 HIV Surveillance Report (13).
Outcome Measures:
The primary outcome measure was availability of HIV testing. A secondary outcome measure was availability of HIV counseling as reported by the facility in response to the query ““Does this facility provide any form of HIV/AIDS education, counseling, or support?” We also examined these variables in combination, constructing measures for provision of both HIV testing and counseling as well as for provision of neither HIV testing nor counseling.
Facility Characteristics:
Facility characteristics included type of insurance reimbursement accepted and operation type (non-profit, for-profit, or government funded). To define sites most likely to serve especially high-risk populations (people who inject drugs and/or have serious mental illness), we identified whether a facility offered medication for opioid use disorder or mental health services. A facility was deemed to offer medication for opioid use disorder if they answered “Yes” to offering any one of the following medication services: 1) “Maintenance services with methadone or buprenorphine,” 2) “Maintenance services with medically-supervised withdrawal (or taper) after a period of stabilization,” 3) “Detoxification from opioids of abuse with methadone or buprenorphine,” or 4) “Relapse prevention with naltrexone.” (14). Facilities were also asked to indicate ancillary services offered at their facility location. Facilities were categorized as offering mental health services if they answered “Yes” to offering mental health services.
Data Analysis:
We used descriptive statistics to characterize the availability of HIV testing and counseling by state, 2017 background HIV incidence, and facility characteristics. We included all US states and the District of Columbia, but not US territories. We mapped the proportion of substance use treatment facilities offering HIV testing by state, then used linear regression to estimate the association of 2017 HIV statewide incidence with the percentage of sites offering HIV testing in each state (13). To estimate the strength of associations between offering medication for opioid use disorder and mental health services, we fit four separate logistic models predicting whether facilities offered HIV testing (irrespective of whether or not they offered counseling), HIV counseling (irrespective of whether or not they offered testing), both, or neither. Each of the four models included the two covariates of interest – whether facilities offered medication for opioid use disorder and whether they offered mental health services – and adjusted for other facility characteristics and state (as a proxy for the impact of statewide HIV incidence). To aid in interpretation, marginal effects with 95% confidence intervals were estimated to obtain adjusted differences in the predicted prevalence of each outcome associated with a facility offering medication for opioid use disorder and mental health services. Finally, we used chi-square tests to evaluate differences in facility characteristics between facilities that did and did not offer mental health services. All analyses were performed using Stata version 16.2 (15). This research was determined not to meet the definition of human subjects research by the [INSTITUTION’S] Committee on Human Research, and thus IRB approval was waived in December 2018.
Description of sample:
14,691 US-based substance use treatment facilities were included in the 2018 N-SSATS survey, including facilities in all 50 US states and the District of Columbia. Forty-one percent of facilities offered medication for opioid use disorder, and 68% offered mental health services. Facilities accepted a variety of insurance reimbursement sources: private insurance (71.6%), Medicaid (65.9%), Medicare (35.9%), and cash or self-payment (90.1%); 2.6% provided services for free. Facilities included those operated by private non-profit organizations (51.5%), private for-profit organizations (37.8%), or local, state, federal, or tribal governments (10.6%). 2017 CDC data shows newly diagnosed HIV cases nationally to be at about 12 per 100,000 people, with wide variation across states (range 1.7–45.3 per 100,000) (13).
Results
Among facilities (N=14,691), 29.0% offered HIV testing, 53.0% offered HIV counseling, 23.4% offered both HIV testing and counseling; and 41.4% offered neither. We found significant state-to-state variation in the proportion of facilities offering HIV testing (range 9.0% to 62.8%) and HIV counseling (range 19.2% to 83.3%) (Figure 1, eTable 1 provides state specific detail).
Figure 1:
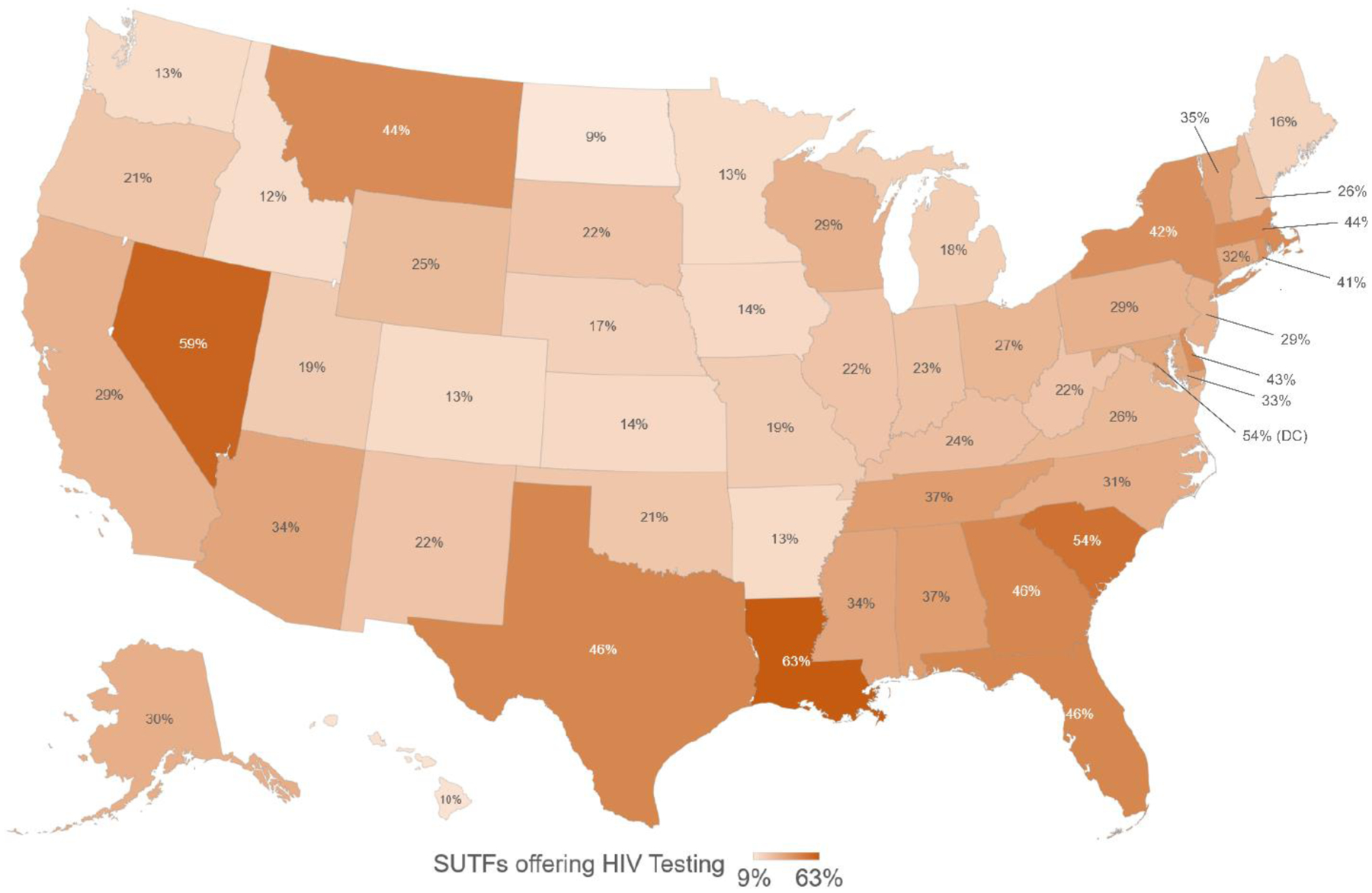
HIV Testing offered in US Substance Use Treatment Facilities (SUTFs) in 2018
Among facilities that provided medication for opioid use disorder, 48.0% offered HIV testing, 64.2% offered HIV counseling, 38.4% offered both HIV testing and counseling, and 26.3% offered neither. Rates of HIV testing availability were significantly higher in facilities offering medication for opioid use disorder (48.0% vs. 16.0% in facilities not offering medication for opioid use disorder), with an adjusted estimate of the difference in prevalence of 30.8% (95% CI: 29.3–32.4, p<.001) (Table 1). HIV counseling was significantly higher in facilities offering medication for opioid use disorder (64.2% vs. 45.4%), with an adjusted estimate of the difference in prevalence of 18.6% (95% CI: 17.0–20.2, p<.001) (Table 1).
Table 1:
HIV testing services offered at substance use treatment facilities, by Medication for Opioid Use Disorder (MOUD) services availability in 2018
| All Facilities N=14,691 | Offering MOUD N=5,963 (41%) | Not offering MOUD N= 8,728 (59%) | Adjusted Differences in Prevalence* | p-value | |||||
|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | % | 95% CI | ||
| HIV Testing | 4,258 | 29.0 | 2,862 | 48.0 | 1,396 | 16.0 | 30.8 | 29.3, 32.4 | <0.001 |
| HIV Counseling | 7,785 | 53.0 | 3,826 | 64.2 | 3,959 | 45.4 | 18.6 | 17.0, 20.2 | <0.001 |
| HIV Testing and Counseling | 3,441 | 23.4 | 2,292 | 38.4 | 1,149 | 13.2 | 24.6 | 23.2, 26.1 | <0.001 |
| Neither HIV Testing nor Counseling | 6,089 | 41.4 | 1,567 | 26.3 | 4,522 | 51.8 | −24.9 | −26.5, −23.4 | <0.001 |
Model adjusted for facility characteristics (insurance reimbursement options and operating agency)
Among facilities providing mental health services, 31.2% offered HIV testing, 54.3% offered HIV counseling, 25.7% offered both, and 40.2% offered neither. HIV testing rates were significantly higher in facilities offering mental health services (31.2% vs. 24.1% in facilities not offering mental health services), with an adjusted estimate of the difference in the prevalence of 3.4% (95% CI: 1.9–5.0, p<.001) (Table 2). HIV counseling was significantly higher in facilities offering mental health services compared to facilities not offering mental health services (54.3% vs. 50.2%), with an adjusted estimate of the difference in prevalence of 4.2% (95% CI: 2.4–5.9, p<.001) (Table 2).
Table 2:
HIV testing services offered at substance use treatment facilities, by mental health services availability in 2018
| All Facilities N=14,691 | Offering Mental Health Services N=10,014 (68%) | Not Offering Mental Health Services N=4,677 (32%) | Adjusted Differences in Prevalence* | p-value | |||||
|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | % | 95% CI | ||
| HIV Testing | 4,258 | 29.0 | 3,129 | 31.2 | 1,129 | 24.1 | 3.4% | 1.9, 5.0 | <0.001 |
| HIV Counseling | 7,785 | 53.0 | 5,435 | 54.3 | 2,350 | 50.2 | 4.2% | 2.4, 5.9 | <0.001 |
| HIV Testing and Counseling | 3,441 | 23.4 | 2,571 | 25.7 | 870 | 18.6 | 4.7% | 3.3, 6.1 | <0.001 |
| Neither HIV Testing nor Counseling | 6,089 | 41.4 | 4,021 | 40.2 | 2,068 | 44.2 | −2.9% | −4.6, −1.2 | <0.001 |
Model adjusted for facility characteristics (insurance reimbursement options and operating agency)
Additional analyses showed that in the 29% of facilities that offer both mental health services and medication for opioid use disorder, adjusted prevalence rates were even higher for HIV testing (47.3%; CI 45.8–48.7%) and HIV counseling (64.7%; 95% CI 63.3–66.1%), which is significantly higher than among facilities offering only mental health services (p<.001) but not statistically different when compared to those facilities offering only medication for opioid use disorder.
When compared to private non-profit facilities, private for-profit facilities were less likely to offer HIV testing (OR 0.66 95%CI 0.53–0.83, p<.001) while government facilities were more likely to offer HIV testing (OR 2.10, 95%CI 1.45–3.03, p<.001). Payment type accepted (e.g., no payment, cash, private insurance, Medicaid, Medicare) was not associated with HIV testing. Higher background state-level HIV incidence was related to an increased proportion of facilities offering HIV testing (R2=0.48; Figure 3).
Figure 3:
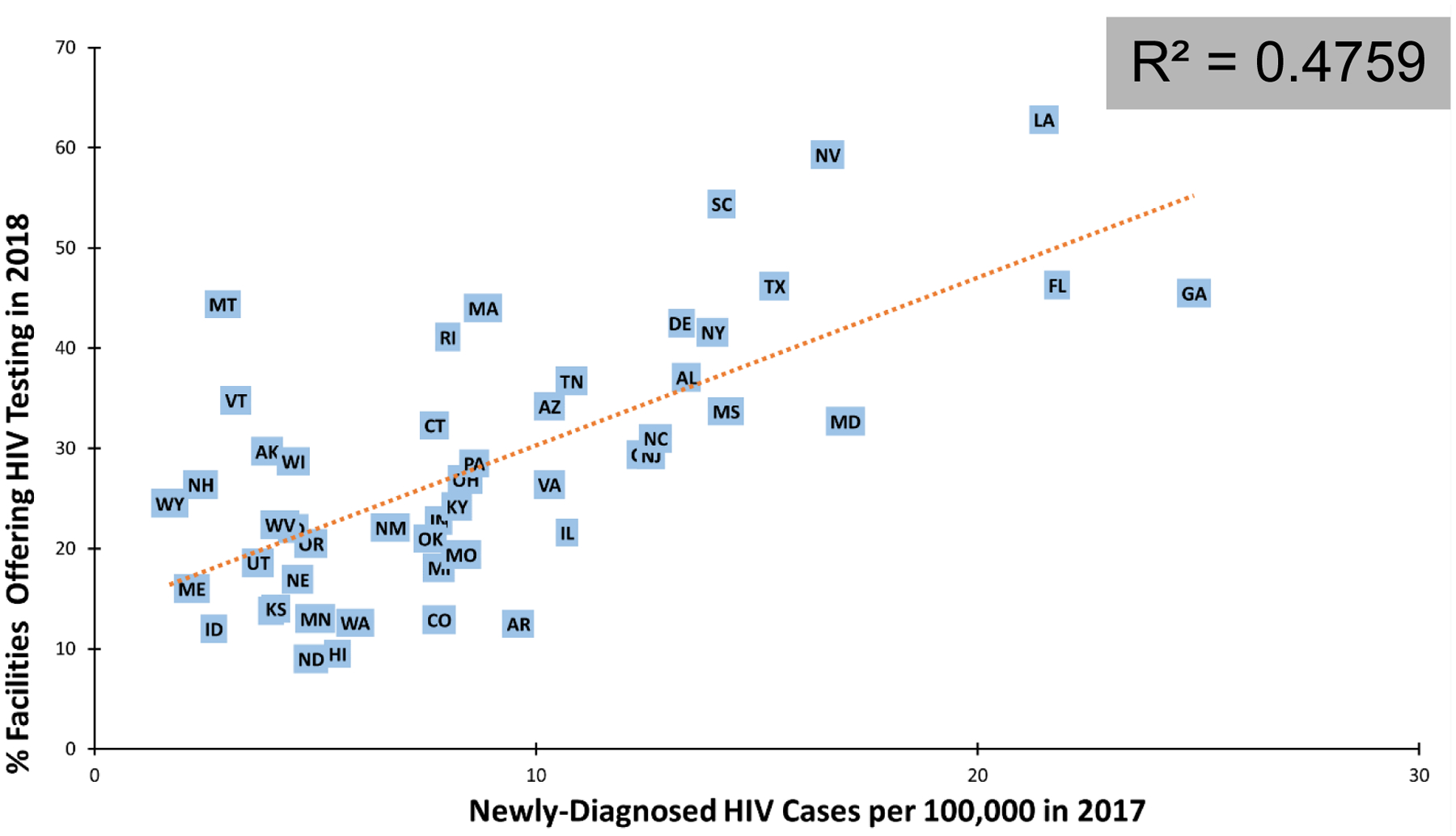
State HIV Incidence versus State HIV Testing in US Substance Use Treatment Facilities*
*Source: state data on facilities offering HIV testing in 2018 obtained from 2018 NSSATS survey; state data on newly diagnosed HIV cases in 2017 obtained from the CDC’s 2018 HIV Surveillance Report.
Note: Washington, DC was an outlier and was excluded from this analysis.
Discussion
Among US facilities reporting to N-SSATS, 29% offered HIV testing, consistent with prior reports in these settings (16). We found little change from prior estimates of HIV testing in these settings between 1995 and 2005 (27% to 29%) (12) despite increasing HIV incidence, updated 2006 CDC guidelines, new policies that incentivize or require reimbursement, and a decline in the rate of uninsured adults (12). This low rate of HIV testing is a missed opportunity for early HIV diagnosis, treatment, and prevention, particularly at a time when the nation is grappling with the impact of the opioid epidemic and investing in the “Ending the HIV Epidemic” initiative, which features testing as a key strategy (17). Given the CDC and USPSTF routine HIV testing recommendations, and the higher-risk population served, universal HIV testing in substance use treatment facilities could help identify individuals who are unaware of their HIV status, link those who are newly diagnosed to care, re-engage those previously diagnosed but out of care, and initiate HIV prevention interventions for those who test negative (1).
Among facilities offering medication for opioid use disorder, fewer than half offered HIV testing. While this is significantly higher than in facilities not offering medication for opioid use disorder (16%), sites offering medication for opioid use disorder are more likely to treat people who inject drugs. While our data show some improvement in these settings when compared to prior smaller studies in similar settings in 2011 (16), the results are nevertheless concerning since people with opioid use disorder—even those on medication for opioid use disorder—are more likely to engage in HIV-related risk behaviors, including sexual risk as well as high risk injection drug use (18). Notably, the CDC, the National HIV/AIDS Strategy, NIDA and SAMHSA all encourage routing HIV testing in opioid treatment programs or integration of HIV and substance use disorder services (19).
HIV testing availability was higher in facilities offering mental health services when compared to those who do not (31% vs. 24%). These modestly higher rates of testing availability could reflect the influence of organizational characteristics, where facilities offering behavioral health care may just offer more services in general, or may reflect need-based policies responding to the perceived presence of populations at higher risk for HIV. Given the low prevalence of HIV testing among people with serious mental illness served in community mental health settings (11), improving testing in substance use treatment settings could help fill this critical testing gap.
Finally, while we found a positive association between state-level diagnosed HIV incidence and rates of HIV testing within state substance use treatment facilities, adherence to universal HIV testing recommendations was low even in states with high HIV burden. For example, fewer than half of all facilities in New York and California offered HIV testing (Figure 1, eTable 1). In fact, only three states (Louisiana, Nevada, and South Carolina) and DC had 50% or more facilities offering HIV testing. Considering how widespread low rates of HIV testing in substance use treatment facilities were across the U.S., leadership at the federal as well as the state level may be needed to increase testing (3).
While it is important to document how HIV testing practices fall short of guidelines, barriers to adoption should be further investigated systematically and intervention strategies tested. One possible barrier to HIV testing is that many substance use treatment facilities are rooted in a 12-step philosophy, where providers may be more reluctant to adopt a medical model of care that would include routine HIV testing (20, 21).
We also found that government-run facilities were more likely than other facilities to offer HIV testing. Given that many of the non-government substance use treatment facilities accept federal funding, federal agencies could consider making funding contingent on the capacity to offer HIV testing or offering incentives to facilities that reach testing targets.
Another approach to increase testing rates of this population involves promoting or encouraging sites to offer rapid, on-site HIV testing with immediate results at substance use treatment facilities. Multiple randomized clinical trials in substance use treatment facilities have shown that offering this testing service more than triples the proportion of clients who receive HIV testing results (22, 23). Of note, the addition of counseling to rapid HIV testing did not reduce HIV risk behaviors or increase receipt of test results (23).
It is important to consider the results of this study in a larger context. Most people in the US who have a substance use disorder, with or without other comorbid mental illnesses, are not in treatment (24–26). While there are a range of reasons for this, one important barrier is the lack of access to services. Examining the system of substance use services that are currently in place in the US does not address this much larger problem of people out of care.
As we explore policy solutions aimed at expanding services to treat substance use disorders, our study supports the value of integrated services. Substance use programs that either offered medication for opioid use disorder or mental health services or both had higher rates of HIV testing and counseling, suggesting programs with a broader range of the services are also more likely to address the common medical comorbidities seen in this population, of which HIV infection is one prominent example.
As the nation grapples with the opioid epidemic in particular, new opportunities will arise that aid us in the goal of expanding access to comprehensive substance use services. One example is ongoing efforts to address the underuse of buprenorphine. In January 2021, the US Department of Health and Human Service published practice guidelines that allow physicians to prescribe buprenorphine without undergoing additional training and a waiver process (27). Expanding the scope of eligible providers could remove barriers to treatment by facilitating access and normalizing substance use treatment in a range of health care settings, but broad implementation efforts will likely be critical to move the needle. In addition to this change, the Centers for Medicare and Medicaid Services also issued guidance that all state Medicaid programs are required to cover treatment for opioid use disorders, including medication (28). While positive results of these changes may be anticipated, their success needs to be investigated empirically. As the range of settings providing treatment for people with opioid use disorders expands as a result of such policy changes and initiatives, it will also be important to extend access to HIV testing to this broader range of providers, even as efforts continue to expand provision of HIV testing in the licensed substance use disorder facilities that are included in the N-SSATS sample. These settings include, for example, federally qualified health centers, which play a significant role both in care of people with substance use disorder and for those with mental health disorders.
Strengths of this study include the size of the dataset and geographic diversity. One limitation is that N-SSATS is self-report data by clinic directors/supervisors, and thus may be missing, incomplete, or subject to social desirability bias. The N-SSATS database includes only the programs that seek to be listed in the SAMHSA services locator tool, and therefore likely over-represents publicly funded sites and under-represents programs that are primarily funded through patient self-pay or commercial health insurance plans. Additionally, N-SSATS surveys do not have client-level data, exclude facilities serving incarcerated individuals and do not define the extent or content of “HIV/AIDS counseling.” Finally, though it would have been preferrable to measure sites where the primary focus was providing mental health services, the response data for the pertinent survey question is not publicly available in the downloadable NSSATS dataset. We may have seen different results if the analysis was limited to facilities that focused on providing mental health services.
In summary, only about three in ten US substance use treatment facilities offer HIV testing, and fewer than half of facilities that treat people with medication for opioid use disorder offer HIV testing. State and federal-level policymakers have opportunities to use evidence-based approaches to increase HIV testing in these facilities, monitor adoption rates, and use financial incentives, as well as their regulatory and licensing authority, to increase testing and improve HIV-related health outcomes. Further, as the nation seeks to end the HIV epidemic through a national initiative, (29, 30) engaging substance use treatment facilities could represent one means of connecting a key risk population to needed HIV prevention and treatment services.
Supplementary Material
Figure 2:
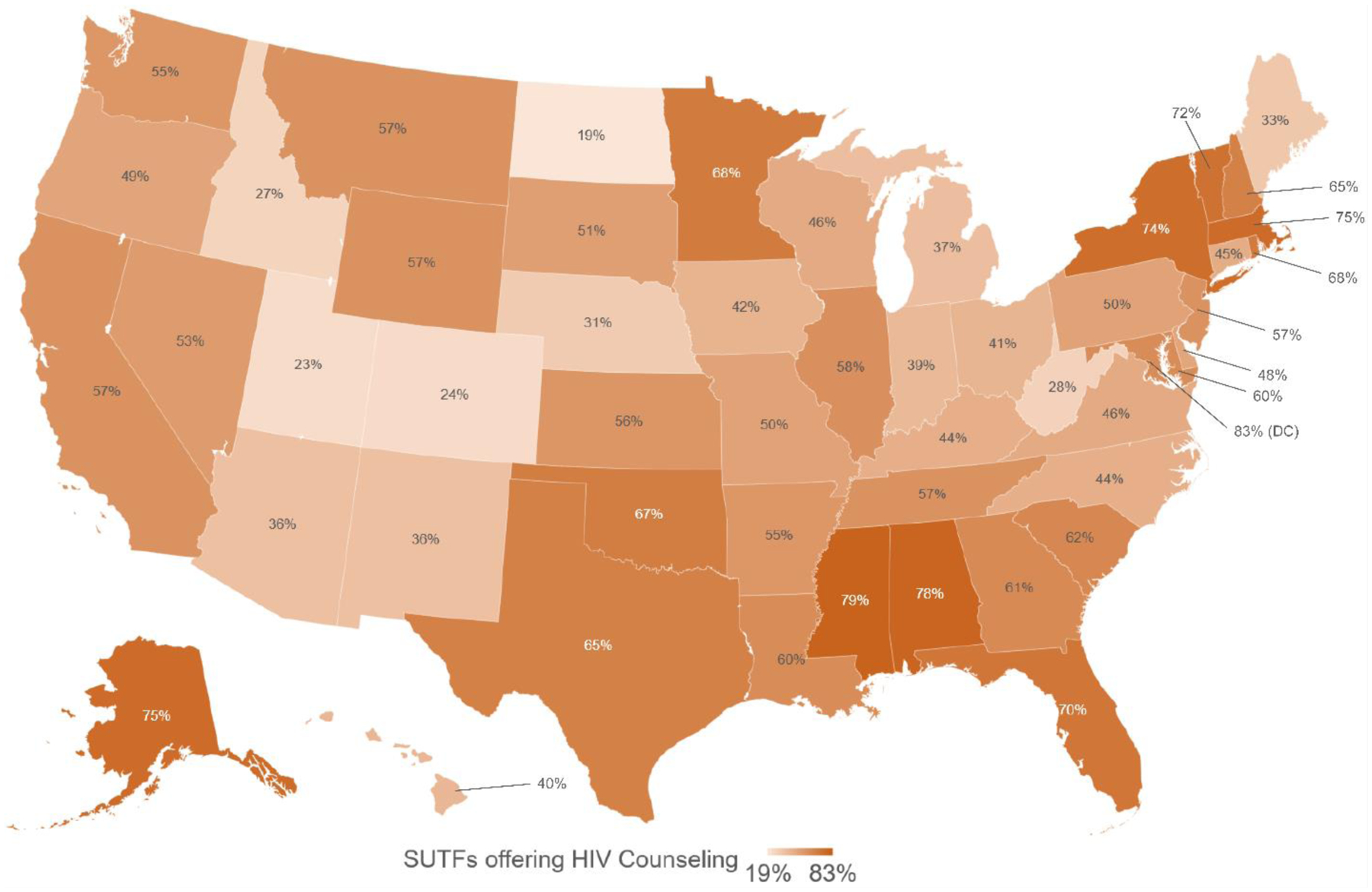
HIV Counseling offered in US Substance Use Treatment Facilities (SUTFs) in 2018
Highlights:
Substance use treatment facilities are uniquely poised to improve early identification, treatment, and prevention of HIV.
These facilities could play an important role in diagnosing HIV among the 25% of people with serious mental illness who have comorbid substance use disorders.
Only 3 in 10 substance use treatment facilities offered HIV testing in 2018.
Disclosures and Acknowledgements:
All authors, excluding Authors B, H, and I, were supported by NIMH grant R01MH112420. Outside of this work, Author C receives support from the NIMH, NIDA, NICHD, and the California HIV/AIDS Research Program. Authors F and G receive support from HRSA. Author H is funded by the Elton John AIDS Foundation. Author I is supported by NIH/NIMH grant R25MH060482. Author J is supported by NIDA R01 DA047347, AHRQ R18-HS023258, and NCATS UL1TR003017. Author K is supported by several grants including the Doris Duke Charitable Fund Foundation, the California Health Care Foundation, and the California Office of Statewide Health Planning and Development. The remaining authors have no disclosures. The authors would like to thank Andrea Elser, BA (L) for her assistance with generating initial figures in this manuscript.
Nicholas S. Riano, MAS (A)
Hannah M. Borowsky, BA (B)
Emily A. Arnold, PhD (C)
Mark Olfson, MD, MPH (D)
James T. Walkup, PhD (E)
Eric Vittinghoff, PhD (F)
Francine Cournos, MD (G)
Lindsey Dawson, MA (H)
Alexander R. Bazazi, MD, PhD (I)
Stephen Crystal, PhD (J)
Christina Mangurian, MD, MAS (K)
Footnotes
Previous Presentation: This project was presented at the 175th Annual American Psychiatric Association Annual Meeting in San Francisco, California, on May 20, 2019.
REFERENCES
- 1.Centers for Disease Control: Revised Recommendations for HIV Testing of Adults, Adolescents, and Pregnant Women in Health-Care Settings, 2006. MMWR Recommendations and Reports 55:1–17, 2006 [PubMed] [Google Scholar]
- 2.Moyer VA, U. S. Preventive Services Task Force: Screening for HIV: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med 159:51–60, 2013 [DOI] [PubMed] [Google Scholar]
- 3.Burke RC, Sepkowitz KA, Bernstein KT, et al. : Why don’t physicians test for HIV? A review of the US literature. Aids 21:1617–24, 2007 [DOI] [PubMed] [Google Scholar]
- 4.Simeone CA, Seal SM, Savage C: Implementing HIV testing in substance use treatment programs: a systematic review. Journal of the Association of Nurses in AIDS Care 28:199–215, 2017 [DOI] [PubMed] [Google Scholar]
- 5.Centers for Disease Control and Prevention: HIV and Substance Use in the United States, 2019
- 6.Jones CM, McCance-Katz EF: Co-occurring substance use and mental disorders among adults with opioid use disorder. Drug and alcohol dependence 197:78–82, 2019 [DOI] [PubMed] [Google Scholar]
- 7.Hughes E, Bassi S, Gilbody S, et al. : Prevalence of HIV, hepatitis B, and hepatitis C in people with severe mental illness: a systematic review and meta-analysis. The Lancet Psychiatry 3:40–8, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.McGinty EE, Baller J, Azrin ST, et al. : Quality of medical care for persons with serious mental illness: A comprehensive review. Schizophr Res 165:227–35, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Carrico AW, Bangsberg DR, Weiser SD, et al. : Psychiatric correlates of HAART utilization and viral load among HIV-positive impoverished persons. Aids Lond Engl 25:1113–8, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Weiser SD, Wolfe WR, Bangsberg DR: The HIV Epidemic Among Individuals with Mental Illness in the United States. Curr Infect Dis Rep 6:404–10, 2004 [DOI] [PubMed] [Google Scholar]
- 11.Mangurian C, Cournos F, Schillinger D, et al. : Low Rates of HIV Testing Among Adults With Severe Mental Illness Receiving Care in Community Mental Health Settings. Psychiatr Serv 68:443–8, 2017 [DOI] [PubMed] [Google Scholar]
- 12.Pollack HA, D’Aunno T: HIV testing and counseling in the nation’s outpatient substance abuse treatment system, 1995–2005. Journal of substance abuse treatment 38:307–16, 2010 [DOI] [PubMed] [Google Scholar]
- 13.Centers for Disease Control and Prevention: HIV Surveillance Report, 2018 (Updated); vol. 31., 2020 [Google Scholar]
- 14.Substance Abuse and Mental Health Services Administration: National Survey of Substance Abuse Treatment Services (N-SSATS), Data on Substance Abuse Treatment Facilities, 2017
- 15.StataCorp: Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC, 2019 [Google Scholar]
- 16.Frimpong JA, D’Aunno T, Helleringer S, et al. : Low rates of adoption and implementation of rapid HIV testing in substance use disorder treatment programs. Journal of substance abuse treatment 63:46–53, 2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.US Department of Health and Human Services: What is ‘Ending the HIV Epidemic: A Plan for America’?, 2020
- 18.McHugh RK, Weitzman M, Safren SA, et al. : Sexual HIV risk behaviors in a treatment-refractory opioid-dependent sample. Journal of psychoactive drugs 44:237–42, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Volkow ND, Montaner J: The urgency of providing comprehensive and integrated treatment for substance abusers with HIV. Health Affairs 30:1411–9, 2011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Nowinski J, Baker S: The twelve-step facilitation handbook: A systematic approach to early recovery from alcoholism and addiction: Jossey-Bass, 1992
- 21.Rothman J, Rudnick D, Slifer M, et al. : Co-located substance use treatment and HIV prevention and primary care services, New York State, 1990–2002: a model for effective service delivery to a high-risk population. J Urban Health 84:226–42, 2007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Frimpong JA, Shiu-Yee K, Tross S, et al. : Bundling Rapid Human Immunodeficiency Virus and Hepatitis C Virus Testing to Increase Receipt of Test Results: A Randomized Trial. Medical care 58:445–52, 2020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Metsch LR, Feaster DJ, Gooden L, et al. : Implementing rapid HIV testing with or without risk-reduction counseling in drug treatment centers: results of a randomized trial. Am J Public Health 102:1160–7, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Williams AR, Nunes EV, Bisaga A, et al. : Development of a Cascade of Care for responding to the opioid epidemic. Am J Drug Alcohol Abuse 45:1–10, 2019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hasin DS, Stinson FS, Ogburn E, et al. : Prevalence, correlates, disability, and comorbidity of DSM-IV alcohol abuse and dependence in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psychiatry 64:830–42, 2007 [DOI] [PubMed] [Google Scholar]
- 26.Priester MA, Browne T, Iachini A, et al. : Treatment Access Barriers and Disparities Among Individuals with Co-Occurring Mental Health and Substance Use Disorders: An Integrative Literature Review. J Subst Abuse Treat 61:47–59, 2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.US Department of Health and Human Services: HHS Expands Access to Treatment for Opioid Use Disorder, 2021
- 28.Costello A: RE: Mandatory Medicaid State Plan Coverage of MedicationAssisted Treatment, 2020
- 29.HIV.gov: Ending the HIV Epidemic: Overview, 2020
- 30.Dawson L, Kates J: The U.S. Ending the HIV Epidemic (EHE) Initiative: What You Need to Know: Kaiser Family Foundation, 2020
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.