

Abstract
Background and Objectives
To investigate the pathogenicity of 2 novel KDM5C variations, report the clinical and neuroimaging findings, and review the available literature.
Methods
Physical examinations, structural neuroimaging studies, and exome sequence analysis were performed. KDM5C constructs were used to study the effect of the variations in transfected cells.
Results
We identified 2 novel variations c.2233C>G and c.3392_3393delAG in the KDM5C gene harboring from 2 Chinese families with X-linked intellectual disability (ID). The affected male patients exhibited severe ID, short stature, and facial dysmorphism. The 1 with c.3392_3393delAG additionally had epilepsy and autistic spectrum disorder (ASD). Transiently transfected mutant KDM5C constructs both reduced protein expression and stability and decreased histone demethylase activities in cells. Reviewing the available literature, we found that the associated ASD tended to occur in patients with variations near the C-terminus of KDM5C.
Discussion
We report the clinical, molecular genetic, and pathologic features in patients with novel variations of KDM5C. The variability of the clinical phenotype in addition to an ID may associate with altered particular parts of KDM5C.
Intellectual disability (ID) is a disability of intellectual and adaptive functions, including reasoning, problem solving, planning, abstract thinking, judgment, academic learning, and personal independence/social responsibility developing1,2 It is an important medical issue and affects 1.5%–3% of the population worldwide.1,3 Underlying causes of ID were very diverse, including brain malformation, metabolic disorders, brain traumatic injury, vascular disorders, nerve system infection, genetic abnormalities, or even environmental factors.2,4 As the quality of clinical care is improved, the genetic contribution to ID becomes even more significant.5 Studies of numerous large cohorts of patients with ID showed a significant excess of males with male to female ratio: about 1.4 for moderate to severe ID (IQ < 50) and 1.9 for mild form (IQ 50–70).6 These indicate the male predominance in patients with ID and that X-linked gene defects are considered to be the informant causes of ID.
It had been estimated that 28.5% of patients with moderate to severe ID and 50% of patients with mild ID are X-linked ID (XLID).6 Clinical observations and linkage studies in families revealed that XLID is a highly heterogeneous condition and is subdivided into syndromic and nonsyndromic forms. The most common form of syndromic XLID is the fragile X syndrome, which is associated with a cytogenetic marker in the distal region of the long arm of the X chromosome involving the FMR1 gene.6 In addition to fragile X syndrome, there are more than 140 syndromic forms of XLID described, and in almost half of them, causative genetic defects have been identified.7
Among these causative genes of XLID, KDM5C is one of the most frequently mutated genes in XLID and estimated to be associated with approximately 0.7%–2.8% of all XLID cases.8,9 The KDM5C (MIM #300534) gene is located at Xp11.22 and encodes a ubiquitous 1560-aa protein that catalyzes the removal of methyl groups from dimethylated and trimethylated histone H3 lysine 4 (H3K4).10 H3K4me2/3, the substrate of KDM5C, is generally associated with promoters of transcriptionally active or poised genes and plays important roles in gene transcription.11 Previous reports suggest a central transcriptional repressive role for KDM5C in chromatin dynamics and epigenetic regulation during cell growth, differentiation, and development, and alterations in chromatin landscape may contribute to disease.12,13
KDM5C-associated XLID is also called Claes-Jensen syndrome. The clinical manifestations included severe ID, epileptic seizure, slowly progressive spastic paraplegia, short stature, microcephaly, maxillary hypoplasia, and small feet.14,15 The truncation or other types of variations of KDM5C have been found in patients with Claes-Jensen syndrome. The majority of missense variations functionally tested to date result in reduced demethylation activity of KDM5C.12,16 Here, we present 2 unrelated families with patients with XLID, harboring 2 novel KDMC variations, p.Q745E and p.E1131Afs.17 Phenotypes, clinical manifestations, and neurologic developmental courses of them were provided. In addition, the pathogenicity of these 2 novel variations was confirmed by in vitro functional assays.
Methods
Patients
From our previously reported cohort of 61 patients with ID, we identified 2 unrelated families with patients with XLID, harboring 2 novel KDMC variations, p.Q745E, and p.E1131Afs.17 The previous cohort included patients with ID with unexplained etiology. ID was defined by a performance score at least 2 SDs below the mean for an appropriate test, including the Bayley Scales of Infant Development (BSID-III) or Wechsler Preschool and Primary Scale of Intelligence (WPPSI-IV).17 All medical records and laboratory results, especially MR neuroimages and metabolic disorder surveys, were reviewed.17 Patients with ID with any possible known etiology were excluded.17
Standard Protocol Approvals, Registrations, and Patient Consents
Written informed consent was obtained from the parents of each patient. Experiments were conducted after obtaining approval from the ethics committee at National Cheng Kung University Hospital.
Targeted Panel Gene—Whole-Exome Sequencing
Genomic DNA isolated from blood was qualified by the Qubit Fluorometer (Thermo Fisher). The SeqCap EZ MedExome Target Enrichment Kit (Roche Sequencing) was used for the gDNA library preparation and exome enrichment following the manufacturer's protocol. We subjected the enriched fragmental DNAs to sequencing by using the nextseq500 high-output sequencing system (Illumina) to produce 2 × 150 bp paired-end sequencing raw data.17 Paired sequence reads were aligned to the human reference genome (hg 19) using Burrows-Wheeler Aligner (BWA version 0.7.8), and then, variants were called using SAMtools, which were provided by Partek Flow (Partek Inc.). Rare variants were filtered according to the related records from genomic sequences databases including 1000 Genomes Project, ExAC, dbSNP, and gnomAD, and the allele frequency of rare variant also was checked with the information from Taiwan Biobank to pick up meaningful variant. To isolate the variant that may directly affect the function of a particular protein, stepwise filtering was used to remove common single nucleotide variations (formerly single nucleotide polymorphisms), 3′ and 5′ untranslated region (UTR) variants, non–splice-related intronic variants, and synonymous variants located at the nonconserved position or had less likely splicing impact. The functional variant was further subjected for genotype to phenotype analysis and manually reviewed by checking with ClinVar and OMIM database.17 The potential pathogenic variants that passed the above filtering steps were subsequently validated by Sanger sequencing to confirm the calling without bias.17
Validation of Variations by Sanger Sequencing
Candidate pathogenic variants were validated by Sanger sequencing. For PCR amplification of KDM5C, the primers were listed in eTable 1 (links.lww.com/NXG/A499). PCR was performed in a total volume of 20 μL containing 10 μL AmpliTaq Gold Fast PCR Master Mix (Applied Biosystems, Foster City, CA), 0.2 μL of each primer with a concentration of 10 pmol/μL, and 4 μL genomic DNA in a concentration of 10 ng/μL.18 The PCR amplicons were sequenced using the BigDye Terminator v1.1 Cycle Sequencing Kit (Applied Biosystems by Life Technologies Corporation). Sequencing was performed using the 3500 Genetic Analyzer (Applied Biosystems by Life Technologies Corporation).18
Computational Modeling
The deduced full-length and mutant proteins were subjected for 3D structure prediction by using the SWISS-MODEL server (swissmodel.expasy.org) according to the suggested procedures. The predicted model of protein structure was visualized, and the substituted residue was labeled by YASARA (yasara.org). The protein contained domains were analyzed by the NCBI Conserved Domains Database (ncbi.nlm.nih.gov/cdd).
Functional Assays
KDM5C cDNA Constructs
The wild-type (WT) human KDM5C cDNA in pcDNA3.1+/C-(K)DYK vector was purchased from GenScript Technologies, Inc. (NJ). To generate the Q745E and p.E1131Afs mutants, we used a mutagenesis kit (QuikChange II Site-Directed Mutagenesis Kit; Stratagene, La Jolla, CA) following the manufacturer's protocol. Plasmids were purified with a plasmid DNA kit (Qiagen Plasmid Mini Kit; Qiagen, Venlo, Limburg, and PureLink HiPure Plasmid Midiprep Kit; Life Technologies Corp., Carlsbad, CA).19 All plasmid construct sequences were confirmed by direct sequencing.
Cell Culture
Human embryonic kidney cells (HEK293) were obtained from ATCC. Cells were maintained in Dulbecco's Modified Eagle Medium (DMEM; Invitrogen, Carlsbad, CA) with 10% fetal bovine serum (FBS) and 100 units/mL of penicillin-streptomycin (Invitrogen) in a humidified 5% (vol/vol) CO2 atmosphere.
Transient Transfection
The targeting construct was transiently transfected into cells using Lipofectamine 2000 reagent (Invitrogen) according to the manufacturer's instructions. In brief, cells (3 x 106) were seeded overnight. The mixture of plasmid DNA (1 μg) and 2 μg of Lipofectamine 2000 diluted in Opti-MEM was added to cells, and cells were cultured for 48 hours before experiments.
Western Blotting
Briefly, the protein samples (50 μg/lane) are separated by sodium dodecyl sulfate–polyacrylamide gel electrophoresis and then subjected to electrotransfer onto the polyvinylidene difluoride membrane. The membrane was subsequently incubated with primary antibodies (anti-KDM5C [Proteintech 14426-1-AP] and anti-H3K4me3 [Cell Signaling 9727]) at 4°C for overnight. Thereafter, the membranes were incubated with an HRP-conjugated secondary immunoglobulin G antibody for 2 hours at room temperature. Protein bands of interest in the membrane were visualized using the Super Signal Western Dura substrate. Following stripping, membranes were incubated with anti-actin antibody (Sigma-Aldrich A5441) or anti-GAPDH antibody (Abcam ab181602) for protein semiquantification.
Protein Stability
HEK293 cells transfected with WT or mutant clones of KDM5C were incubated with cycloheximide (Sigma, 20 mg/mL) for 0 (DMSO vehicle only), 1, 2, 4, 8, and 24 hours, lysed, and subjected to Western blotting.11
Quantitative RT-PCR
Total RNA was isolated using the FavorPrep Tissue Total RNA Mini Kit (Favorgen) according to the manufacturer's instructions. Polyadenylated RNA was purified from at least 50 µg of total RNA using PolyA + Track mRNA Isolation System III from Promega (#Z5300), according to the manufacturer's instructions. First-strand cDNA was synthesized from total RNA using a GoScript Reverse Transcription System (Promega) and T100 Thermal Cycler (Bio-Rad) according to the manufacturer's manual. Transcript abundance was determined by quantitative PCR using a StepOnePlus Real-Time PCR (Applied Biosystems) and primers specific for each transcript (eTable 1, links.lww.com/NXG/A499). Expression levels were normalized to the GAPDH housekeeping gene.
Immunofluorescence for In Situ Demethylation Assay
Cells transfected with WT and mutant clones of KDM5C grown on glass coverslips were fixed with 2% formaldehyde for 10 minutes and then with 100% ice-cold methanol for 10 minutes. Cells were permeabilized with 0.1% NP-40 in PBS, blocked with 20% FBS in PBS for 1 hour, and then incubated with the appropriate primary antibodies including anti-H3K4me3 (Genetex GTX50897), anti-KDM5C (Proteintech 14426-1-AP), and anti-Flag (Sigma-Aldrich F3165) overnight at 4°C.11 After washing, cells were incubated with Alexa 594–conjugated donkey anti-rabbit or Alexa 488-conjugated goat anti-mouse secondary antibodies (Molecular Probes) for 30 minutes at room temperature.11 Coverslips were then mounted with Vectashield containing DAPI (Vector Laboratories) for nuclear localization. Images were acquired by laser confocal microscopy (Olympus).
Statistics
A commercial program (SPSS version 20.0; SPSS Institute, Chicago, IL) was used for the statistical analysis. Data were presented as mean ± SD (SD). In case of multiple comparisons, the 1-way ANOVA plus Scheffe post hoc test was applied.
Data Availability
The data that support the findings of this study are always available from the corresponding author.
Results
Clinical Features of the Patients
These 2 Taiwanese families both have 2 affected male siblings, respectively. The proband in the 1st family, a 12-year-old boy is the first child born to healthy nonconsanguineous parents. His perinatal history was unremarkable. The patient started walking at age 23 months and riding a tricycle at age 4.5 years. He started babbling at age 12–14 months and spoke his first words after age 3 years; yet he could not reliably use sentences. The formal intelligence test revealed severe ID. The brain MRI at age 11 years was normal (Figure 1). His sibling was diagnosed with severe ID later. These boys had some dysmorphic features including short stature (less than 3rd percentile), microcephaly (48 cm at age 5 years, 3rd percentile), facial dysmorphism (prognathism of the mandible, slight maxillary hypoplasia, flat philtrum, strabismus, and diastema) (Figure 1). Besides being severely ID, these 2 patients did not have seizures.
Figure 1. Clinical Features and Neuroimages.

Frontal and lateral views of the older sibling at age 9 years (A and B) and the younger sibling at age 6 years and 4 months (C and D) in the 1st family. Brain MRI of the older sibling of the 1st family at age 10 years (E and F: T2-weighted images) and of the younger sibling of the 2nd family at age 13 years (G: T1-weighted image; H: FLAIR image). There were small white matter lesions (arrow) in the patient with p.E1131Afs variation of the 2nd family.
In the 2nd family, there were also 2 affected boys of healthy nonconsanguineous parents. The perinatal histories of them were also unremarkable. Both had a similar clinical course presenting with severe developmental delay, precocious puberty, and epilepsy. They both started walking at around age 24 months and still had poor daily coping skills like using spoons. They spoke a few meaningful words after age 3 years; yet they could not reliably use sentences. The formal intelligence test revealed severe ID in both patients. Focal seizures and generalized tonic-clonic seizures occurred in both patients since early childhood. The EEG revealed slow background and active epileptiform discharges at each side of frontotemporal areas. Over the years, a variety of anticonvulsants were tried to control seizures including valproic acid, oxcarbazepine, lamotrigine, levetiracetam, and topiramate, but epilepsy became intractable to anticonvulsants thereafter. The proband is the younger sibling, who was also diagnosed with autistic spectrum disorder at age 3 years, and his MRI at age 14 years showed small nodular T2 hyperintensity lesions over bilateral periventricular white matter (Figure 1). Besides, they both had short stature and facial dysmorphism (prognathism of the mandible, flat philtrum, and diastema) as well. These 4 affected boys now are at the Special Education School in their hometown.
Identification of Novel Variants in KDM5C by Whole-Exome Sequencing
We identified sequence variants in KDM5C by whole-exome sequencing in 3 patients of these 2 families. Overall, we detected 2 unique variants including c.2233C>G (p.Q745E) in 2 siblings of the 1st family and c.3392_3393delAG (p.E1131Afs) in 1 sibling of the 2nd family (Figure 2A, B). The p.Q745E occurs at highly conserved residues and was predicted to be deleterious and was absent in population‐based databases (gnomAD and Taiwan Biobank) (Figure 2C). The other variant (p.E1131Afs) had a small indel resulting in a truncated protein (Figure 2C) and is predicted to be deleterious as well. It has not been documented in gnomAD and Taiwan Biobank either. In accordance with the ACMG criteria, these variants were all classified as pathogenic.
Figure 2. Variations.

The pedigree of the 1st family (A) and 2nd family (B) and sequence chromatograms of parts of the KDM5C gene. The c.2233C>G nucleotide change of the 1st family is indicated with a circle (p.Q745E), and the c.3392_3393delAG nucleotide change of the 2nd family is indicated with an arrow (p.E1131Afs). (C) Schematic of functional domains on human KDM5C proteins encoded by our 2 reported variations. (D) Molecular modeling of the variant. Model generation is based on template structure PDB: 5fwj.1.A by using SWISS-MODEL server. p.Q745E found in affected individuals shown in red. Zinc finger domain is in blue, and zinc ions are shown as a yellow ball. The surface model of the zinc finger domain is presented as light gray. Because of the lack of a suitable 3D structure, the modeling of p.E1131Afs is not available now. JmN = jumonji-N domain; ARID = AT-rich interacting domain; PHD = plant homeodomain box domain; JmjC = jumonji-C catalytic domain; ZF = zinc finger domain; PLU-1 = PLU-1–like domain.
Further segregation analysis by Sanger sequencing was conducted in the 1st family and showed that the p.Q745E was inherited from their mother. Because both mothers have a normal intellectual phenotype and social adjustment ability, the inheritance pattern of p.Q745E should be an X-linked recessive type. For some family issues, the parents in the 2nd family refused the segregation analysis to validate the inheritance pattern.
Functional Complementation
RNA Expression, Protein Expression, and Protein Stability
The effects of the genetic variations on the RNA expression level of KDM5C in HEK293 cells transfected with WT and mutant clones were detected using qRT-PCR, which showed that KDM5C mRNA levels did not reduce in p.Q745E and p.E1131Afs mutants of KDM5C compared with that in KDM5C WT (Figure 3A). However, the protein levels of KDM5C p.Q745E and p.E1131Afs were significantly reduced compared with those of KDM5C WT (Figure 3B). The reduction of KDM5C (a demethylase enzyme) protein levels correlated with the increases of its substrate H3K4me3 (Figure 3B). To investigate whether the stability of KDM5C protein was affected by p.Q745E and p.E1131Afs, we treated cells with cycloheximide, an inhibitor of protein synthesis for 0–24 hours. As shown in Figure 3C, the increased degradation of p.Q745E and p.E1131Afs KDM5C was reflected by a reduction of their half-life from more than 24 hours (WT) to near 21 hours (p.Q745E) and 1.8 hours (p.E1131Afs). The data suggested that protein stability is largely affected by both variations.
Figure 3. Impacts of the p.Q745E and p.E1131Afs Variations on Expression of KDM5C.

(A) Representative gel image of semiquantitative (above) and quantitative RT-PCR analysis (below) of KDM5C mRNA expression in HEK293 cells transfected with control plasmid, WT KDM5C, and mutants of KDM5C. The expression levels were normalized with that of housekeeping gene GAPDH of the control (HEK293) cells. (N = 3) (B) Whole cell lysates from HEK293 cells transfected with control plasmid, WT KDM5C, and mutants were analyzed for the expression of KDM5C and H3K4me3 protein. (N = 4) (C) Cycloheximide (CHX) chase analysis was performed. Immunoblotting was in the left panel, and graphs in the right panel represented the percentage of remaining KDM5C. The level of WT KDM5C decreased to 78%, whereas the level of p.Q745E and p.E1131Afs KDM5C decreased to 47% and 11% at 24 hours after the CHX treatment. The half-life of WT KDM5C was more than 24 hours, and the half-life of p.Q745E and p.E1131Afs KDM5C was near 21 hours and 1.8 hours, respectively. Dotted line indicates 50% of initial normalized KDM5C protein level. (N = 3) Data are expressed as mean ± SD. *p < 0.05; **p < 0.01. CHX = cycloheximide; H3K4 = H3 lysine 4; WT = wild type
Enzymatic Activity
A majority of disease-associated KDM5C variations exhibit a decrease in histone demethylase activity, suggesting a loss-of-function pathogenic mechanism.17,20 The demethylation activities were assessed ex vivo in cells (Figure 4). A significant decrease of H3K4me3 signals was observed in cells with ectopic expression of KDM5C WT. In contrast, signals of H3K4me3 were preserved in cells with ectopic expression of p.Q745E or p.E1131Afs KDM5C, indicating that the demethylation activity of KDM5C was nearly abrogated by these 2 variations.
Figure 4. In Situ Assay on Demethylation Activity of KDM5C.
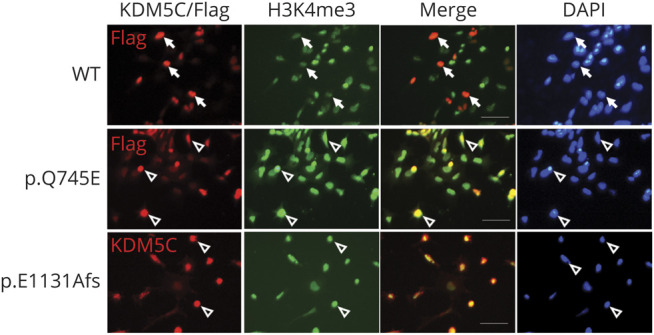
Representative immunofluorescence images of KDM5C and H3K4me3 in cells transfected with WT and variations of KDM5C (N = 4). Cells transfected with WT KDM5C showed reduced H3K4me3 signals, implicating demethylase activity of KDM5C (arrow). Cells transfected with p.Q745E or p.E1131Afs variation retained high H3K4me3 signals implicating the reduction of demethylase activity of KDM5C (open arrowhead). Nuclei were stained with DAPI. Scale bar = 50 μm. H3K4 = H3 lysine 4
Discussion
KDM5C encodes a ubiquitous protein, which contains several highly conserved domains including the catalytic JmjC domain, the ARID DNA binding domain, the zinc finger domain, and the JmjN domain for protein stability and 2 plant homeodomains (PHDs) for chromatin association.21 KDM5C medicates the demethylation of trimethylated and dimethylated lysines on H3K4 (H3K4me3 and H3K4me2, respectively) and possesses functions as a transcriptional corepressor and an enhancer modulator.12,16,22 This chromatin-modifying enzyme is mainly expressed in brain and exerts tight dose- and time-dependent control over neuronal development through silencing germline genes, fine-tune the neuronal epigenome, and preclude spurious transcription.23 Thus, KDM5C dysfunction plays a role in the etiology of ID and other neurologic disorders. It was reported that germinal loss of KDM5C in mice causes dendritic and spine anomalies and recapitulates cognitive, adaptive, and social abnormalities seen in patients with KDM5C variations, including increased aggression, decreased anxiety, and social behavior and defects in learning and memory.24 Furthermore, RNA interference–mediated silencing of the KDM5C gene resulted in the derepression of genes including SCN2A, encoding sodium channel; CACNA1B and CACNA1H, encoding calcium channels; and SCL4A3, SLC18A1, and SLC6A12, encoding monoamine transporters.12,25 All these KDM5C target genes have been previously implicated in neurologic disorders such as epilepsy, autism, or schizophrenia.12
In this study, we present 2 Taiwanese families with XLID caused by novel variations c.2233C>G (p.Q745E) and c.3392_3393delAG (p.E1131Afs) in the KDM5C gene, and both were confirmed to be pathogenic. The first variation (c.2233C>G; p.Q745E) is a missense variation located in the coding region of the zinc finger domain. This highly conserved domain contains potential zinc ligand-binding residues and may have a DNA-binding function.12 Previous studied showed that variations in the zinc finger caused different degrees of decreased histone demethylase activities and the associated neurodevelopmental disability relied on the residual enzyme activities.19,26 The p.Q745E variation of KDM5C identified in our study decreased KDM5C protein levels and reduced protein stabilities compared with cell expression with that of the WT KDM5C. The in situ demethylation assay showed that KDM5C with this p.Q745E variation cannot efficiently reduce levels of its substrate H3K4me3, suggesting loss of its histone demethylase activities. The second variation (c.3392_3393delAG; p.E1131Afs) is a frameshift variation located in the C-terminus of the KDM5C. Although most of the functional domains were preserved in this truncated KDM5C caused by p.E1131Afs, the level and stability of the truncated KDM5C were tremendously attenuated compared with WT KDM5C and KDM5C with p.Q745E variation.
To date, 57 pathogenic variations on the KDM5C gene have been described in the English literature.9,14,15,18,25-36 We summarized their loci and clinical manifestations in Figure 5. Of interest, the missense and splice site variations commonly occur in functional domains, and the nonsense and frameshift variations are frequently in nonfunctional regions. The phenotype varies within and between families; it is probably due to the functional severity of the variations, the existence of possible compensatory mechanisms by alternative histone demethylases, and other epigenetic and environmental modifying factors.25 Patients with variations in the zinc finger domain including our patient with p.Q745E variation usually have severe ID, short stature, and some facial dysmorphism. However, none with variations involving the zinc finger domain have the manifestation of seizures when compared with variations involving in other domains (Figure 5). Moreover, we found that autistic spectrum disorder is not a common manifestation in these patients with KDM5C variations, but it only occurs in patients with variations near the C-terminus, like our reported patient with the p.E1131Afs variation. This evidence indicates that involvements of particular functional domains of KDM5C on the epigenetic regulations may have distinguished impacts on the CNS development.
Figure 5. Distribution of Variations and Associated Phenotypes.

Distribution of variations was shown on the KDM5C protein. Each column in the heatmap represents a patient ranked by the position of the variant carried by the patient, and each row represents a clinical phenotype from patient surveys in the literature (references 9,14,15,26–36).
KDM5C is one of the most frequently mutated genes found in XLID.8,9 It should be taken into consideration when patients with ID in the families with at least 2 affected male siblings and may accompany with short stature and/or seizures. Further studies identify that novel disease-causing mechanisms associated with variations within a particular domain of KDM5C will help understand the role of KDM5C in the CNS development.
Acknowledgment
The authors express their gratitude to the patients, their caretakers, and the clinical and laboratory staff from National Cheng Kung University Hospital.
Glossary
- ASD
autistic spectrum disorder
- BSID
Bayley Scales of Infant Development
- BWA
Burrows-Wheeler Aligner
- FBS
fetal bovine serum
- H3K4
H3 lysine 4
- ID
intellectual disability
- HEK
human embryonic kidney
- PHD
plant homeodomain
- UTR
untranslated region
- WPPSI
Wechsler Preschool and Primary Scale of Intelligence
- WT
wild type
- XLID
X-linked intellectual disability
Appendix. Authors

Contributor Information
Po-Ming Wu, Email: bradsteve41@gmail.com.
Wen-Hao Yu, Email: fieldof19@yahoo.com.tw.
Chi-Wu Chiang, Email: chiangcw@mail.ncku.edu.tw.
Chen-Yu Wu, Email: wusteven994@gmail.com.
Jia-Shing Chen, Email: cjshing77@gmail.com.
Study Funding
This study was supported by grants from National Cheng Kung University Hospital (NCKUH-10802015) and Ministry of Science and Technology (MOST 106-2314-B-006-075 and 108-2314-B-006 -066) of Taiwan.funding
Disclosure
The authors report no disclosures. Go to Neurology.org/NN for full disclosures.
References
- 1.de Ligt J, Willemsen MH, van Bon BW, et al. Diagnostic exome sequencing in persons with severe intellectual disability. N Engl J Med. 2012;367(20):1921-1929. [DOI] [PubMed] [Google Scholar]
- 2.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed: American Psychiatric Association; 2013. [Google Scholar]
- 3.Leonard H, Wen X. The epidemiology of mental retardation: challenges and opportunities in the new millennium. Ment Retard Dev Disabil Res Rev. 2002;8(3):117-134;. [DOI] [PubMed] [Google Scholar]
- 4.Kuo HT, Muo CH, Chang YT, Lin CK. Change in prevalence status for children with developmental delay in Taiwan: a nationwide population-based retrospective study. Neuropsychiatr Dis Treat. 2015;11:1541-1547; doi: 10.2147/NDT.S84088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ropers HH. Genetics of early onset cognitive impairment. Annu Rev Genomics Hum Genet. 2010;11:161–187. [DOI] [PubMed] [Google Scholar]
- 6.Ropers HH, Hamel BC. X-linked mental retardation. Nat Rev Genet. 2005;6(1):46-57. [DOI] [PubMed] [Google Scholar]
- 7.Vissers LE, Gilissen C, Veltman JA. Genetic studies in intellectual disability and related disorders. Nat Rev Genet. 2016;17(1):9-18. [DOI] [PubMed] [Google Scholar]
- 8.de Brouwer AP, Yntema HG, Kleefstra T, et al. Mutation frequencies of X-linked mental retardation genes in families from the EuroMRX consortium. Hum Mutat. 2007;28(2):207-208. [DOI] [PubMed] [Google Scholar]
- 9.Vallianatos CN, Farrehi C, Friez MJ, Burmeister M, Keegan CE, Iwase S. Altered gene-regulatory function of KDM5C by a novel mutation associated with autism and intellectual disability. Front Mol Neurosci. 2018;11:104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Merath K, Ronchetti A, Sidjanin DJ. Functional analysis of HSF4 mutations found in patients with autosomal recessive congenital cataracts. Invest Ophthalmol Vis Sci. 2013;54(10):6646-6654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Brookes E, Laurent B, Õunap K, et al. Mutations in the intellectual disability gene KDM5C reduce protein stability and demethylase activity. Hum Mol Genet. 2015;24(10):2861-2872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Tahiliani M, Mei P, Fang R, et al. The histone H3K4 demethylase SMCX links REST target genes to X-linked mental retardation. Nature. 2007;447(7144):601-605. [DOI] [PubMed] [Google Scholar]
- 13.Kouzarides T. Chromatin modifications and their function. Cell. 2007;128(4):693-705. [DOI] [PubMed] [Google Scholar]
- 14.Abidi FE, Holloway L, Moore CA, et al. Mutations in JARID1C are associated with X-linked mental retardation, short stature and hyperreflexia. J Med Genet. 2008;45(12):787-793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Jensen LR, Amende M, Gurok U, et al. Mutations in the JARID1C gene, which is involved in transcriptional regulation and chromatin remodeling, cause X-linked mental retardation. Am J Hum Genet. 2005;76(2):227-236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Iwase S, Lan F, Bayliss P, et al. The X-linked mental retardation gene SMCX/JARID1C defines a family of histone H3 lysine 4 demethylases. Cell. 2007;128(6):1077-1088. [DOI] [PubMed] [Google Scholar]
- 17.Chen JS, Yu WH, Tsai MC, Hung PL, Tu YF. Comorbidities associated with genetic abnormalities in children with intellectual disability. Sci Rep. 2021;11:6563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Laidoudi Y, Davoust B, Varloud M, Niang EHA, Fenollar F, Mediannikov O. Development of a multiplex qPCR-based approach for the diagnosis of Dirofilaria immitis, D. repens and Acanthocheilonema reconditum Parasit Vectors. 2020;13(1):319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Merath K, Ronchetti A, Sidjanin DJ. Functional analysis of HSF4 mutations found in patients with autosomal recessive congenital cataracts. Invest Ophthalmol Vis Sci. 2013;54(10):6646-6654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Rujirabanjerd S, Nelson J, Tarpey PS, et al. Identification and characterization of two novel JARID1C mutations: suggestion of an emerging genotype-phenotype correlation. Eur J Hum Genet. 2010;18(3):330-335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Gonçalves TF, Gonçalves AP, Fintelman Rodrigues N, dos Santos JM, Pimentel MM, Santos-Rebouças CB. KDM5C mutational screening among males with intellectual disability suggestive of X-Linked inheritance and review of the literature. Eur J Med Genet. 2014;57(4):138-144. [DOI] [PubMed] [Google Scholar]
- 22.Collins BE, Greer CB, Coleman BC, Sweatt JD. Histone H3 lysine K4 methylation and its role in learning and memory. Epigenetics Chromatin. 2019;12(1):7; [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Scandaglia M, Lopez-Atalaya JP, Medrano-Fernandez A, et al. Loss of Kdm5c causes spurious transcription and prevents the fine-tuning of activity-regulated enhancers in neurons. Cell Rep. 2017;21(1):47-59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Iwase S, Brookes E, Agarwal S, et al. A mouse model of X-linked intellectual disability associated with impaired removal of histone methylation. Cel Rep. 2016;14(5):1000-1009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Santos-Reboucas CB, Fintelman-Rodrigues N, Jensen LR, et al. A novel nonsense mutation in KDM5C/JARID1C gene causing intellectual disability, short stature and speech delay. Neurosci Lett. 2011;498(1):67-71. [DOI] [PubMed] [Google Scholar]
- 26.Ounap K, Puusepp-Benazzouz H, Peters M, et al. A novel c.2T > C mutation of the KDM5C/JARID1C gene in one large family with X-linked intellectual disability. Eur J Med Genet. 2012;55(3):178-184. [DOI] [PubMed] [Google Scholar]
- 27.Tzschach A, Lenzner S, Moser B, et al. Novel JARID1C/SMCX mutations in patients with X-linked mental retardation. Hum Mutat 2006;27(4):389. [DOI] [PubMed] [Google Scholar]
- 28.Adegbola A, Gao H, Sommer S, Browning M. A novel mutation in JARID1C/SMCX in a patient with autism spectrum disorder (ASD). Am J Med Genet A. 2008;146A:505–511. [DOI] [PubMed] [Google Scholar]
- 29.Guerra JVS, Oliveira-Santos J, Oliveira DF, et al. DNA methylation fingerprint of monozygotic twins and their singleton sibling with intellectual disability carrying a novel KDM5C mutation. Eur J Med Genet. 2020;63(3):103737. [DOI] [PubMed] [Google Scholar]
- 30.Fujita A, Waga C, Hachiya Y, et al. Different X-linked KDM5C mutations in affected male siblings: is maternal reversion error involved? Clin Genet. 2016;90(3):276-281. [DOI] [PubMed] [Google Scholar]
- 31.Ding N, Zhang P, Mao Y, et al. [Clinical features and gene variant of a pedigree affected with X-linked recessive mental retardation Claes-Jensen type]. Zhonghua Yi Xue Yi Chuan Xue Za Zhi. 2020;37(12):1352-1355. [DOI] [PubMed] [Google Scholar]
- 32.Kawano-Matsuda F, Maeda T, Kaname T, Yanagi K, Ihara K. X-linked mental retardation and severe short stature with a novel mutation of the KDM5C gene. Clin Pediatr Endocrinol. 2021;30(1):61-64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Carmignac V, Nambot S, Lehalle D, et al. Further delineation of the female phenotype with KDM5C disease causing variants: 19 new individuals and review of the literature. Clin Genet. 2020;98(1):43-55. [DOI] [PubMed] [Google Scholar]
- 34.Redin C, Gérard B, Lauer J, et al. Efficient strategy for the molecular diagnosis of intellectual disability using targeted high-throughput sequencing. J Med Genet. 2014;51(11):724-736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Santos C, Rodriguez-Revenga L, Madrigal I, Badenas C, Pineda M, Milà M. A novel mutation in JARID1C gene associated with mental retardation. Eur J Hum Genet. 2006;14(5):583-586. [DOI] [PubMed] [Google Scholar]
- 36.Grafodatskaya D, Chung BH, Butcher DT, et al. Multilocus loss of DNA methylation in individuals with mutations in the histone H3 lysine 4 demethylase KDM5C. BMC Med Genomics. 2013;6:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are always available from the corresponding author.