

Abstract
Lateral neck ectopic thyroid tissue remains a rare entity that can be affected by any lesion involving the gland. The origin of lateral neck ectopic thyroid carcinomas still debated between a metastatic disease secondary to thyroid primary tumor and primary malignancy on the ectopic tissue. Anyway, it should indicate an exploration of the gland.
We report the case of a 36 years old female with one year history of hyperthyroidism who was admitted for multinodular grade II goiter with a firm mass in the left level II of the lateral neck. The thyroid scintigraphy demonstrated multiple functioning nodules corresponding to toxic multinodular goiter; in addition to two cold hypofunctional nodules. The cervical ultrasound showed a voluminous multinodular goiter classified as EU TIRADS 5. The surgical procedure exposed a multinodular mass, lateral to the internal jugular vein, with the appearance and structure of the thyroid gland and no connection to it. The thyroid gland was exposed next through a collar incision. Each mass was dissected and removed individually. The histopathology examination of the thyroid gland found papillary carcinoma extracapsular extension. The pathology results of the other mass reported multiple colloid nodules with cystic component, papillary in appearance, with the same cancer proliferation, compatible with ectopic thyroid tissue with papillary carcinoma. No lymph node tissue was found. The patient was sent for complementary RAItherapy.
We report a rare case of lateral neck ectopic thyroid papillary carcinoma that supplements and supports the lacking literature data concerning the management of this rare entity.
Keywords: Lateral neck ectopic thyroid tissue, Thyroid gland, Papillary carcinoma
Highlights
-
•
Lateral neck ectopic thyroid tissue is a rare entity that can possibly be affected by any lesion involving the gland.
-
•
Metastasis from thyroid primary carcinoma are difficult to distinguish from primary malignancy of the ectopic tissues.
-
•
The discovery of papillary carcinoma on ectopic thyroid tissue should indicate an exploration of the gland.
1. Introduction
Most ectopic thyroid tissues are located in the midline area corresponding to the embryological descending path of the gland. Lateral neck ectopic thyroid tissue remains a rare entity that can be affected by any lesion involving the gland [1], [2], [3].
Lateral neck ectopic thyroid carcinomas secondary to metastatic diseases from thyroid primary carcinoma are hardly distinguished from true primary malignancy of the ectopic tissues [4]. Thus, the discovery of papillary carcinoma on ectopic thyroid tissue should indicate an exploration of the gland [5].
We report a rare case of lateral neck ectopic thyroid papillary carcinoma with misleading clinical presentation of a lymphadenopathy, that supplements and supports the lacking literature data concerning the diagnosis and management of this rare entity.
2. Presentation of the case
We report the case of a 36 years old female, with one year history of hyperthyroidism under Carbimazole 5 mg/day. The clinical examination found mobile multinodular grade II goiter with a firm mass in the left level II of the lateral neck.
The thyroid scintigraphy demonstrated multiple functioning nodules corresponding to toxic multinodular goiter; in addition to two cold hypofunctional nodules one in the isthmus and the other on the superior part of the left lobe. The cervical ultrasound showed a voluminous multinodular goiter classified as EU TIRADS 5 according to its most suspicious nodule, associated to infracentimetric lymph nodes. The TSH value was normal (0,56 mU/l) as well as T3 (3,5 ng/l) and T4 (9,8 ng/l).
The surgery was performed under general anaesthesia and aimed to remove the lateral mass first for an extemporaneous examination which would indicate lymph node dissection if malignant. The procedure started by left superior horizontal U-shaped incision regarding the lateral mass. The surgical dissection exposed a multinodular mass, lateral to the internal jugular vein, with the appearance and structure of the thyroid gland and no connection to it (Fig. 1).
Fig. 1.

Left cervical mass with the structure and appearance of the thyroid gland.
The following surgical time consisted on exposing the thyroid gland through a collar incision. After the muscular dissection, the recurrent laryngeal nerves and parathyroids were preserved in both sides. This surgical step allowed the exposure of two independent masses corresponding to the thyroid gland and a mass with the same structure and appearance presenting as ectopic thyroid tissue (Fig. 2).
Fig. 2.
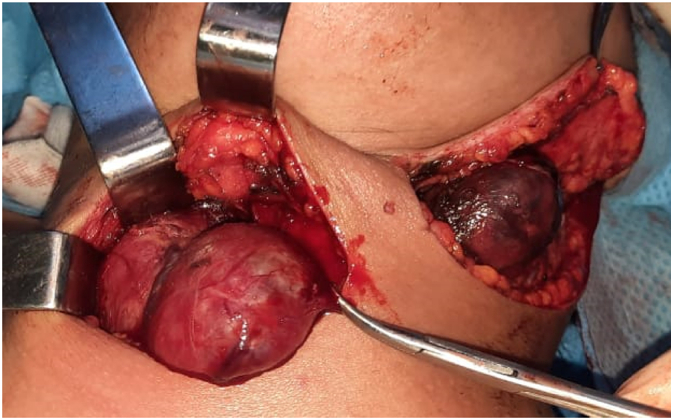
The exposure of two independent masses, the thyroid gland and lateral ectopic thyroid tissue.
Each mass was dissected and removed individually (Fig. 3). The cavities were closed on Redon drains. The postoperative follow up was uneventful.
Fig. 3.
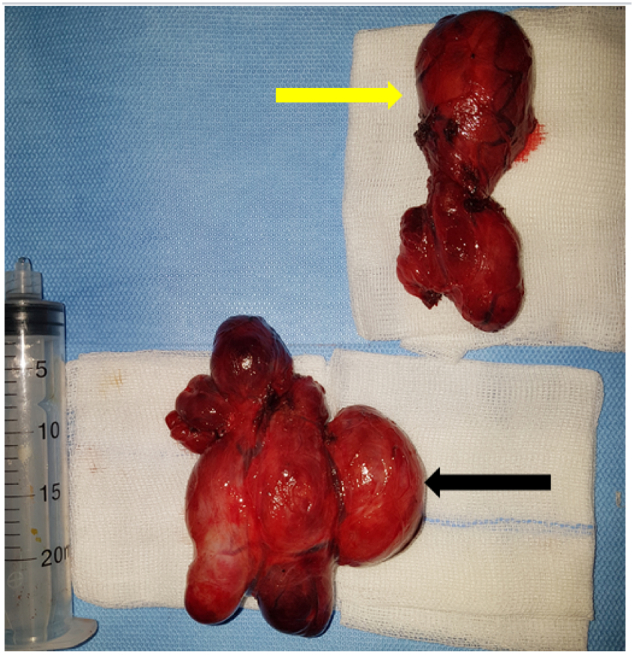
The two thyroid masses removed individually: the thyroid gland (black arrow) and lateral ectopic thyroid tissue (yellow arrow). (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
The histopathology examination of the thyroid gland found papillary carcinoma with extracapsular extension. The pathology results of the second mass reported multiple colloid nodules with cystic component, papillary in appearance, with the same cancer proliferation, compatible with ectopic thyroid tissue with papillary carcinoma. No lymph node tissue was found. The patient was sent for complementary RAItherapy.
This case has been reported in line with the SCARE 2020 criteria [6].
3. Discussion
The thyroid gland has two embryological origins. It originates medially from a diverticulum located in the median ventral wall of the pharynx by an endodermal thickening between the 1st and 2nd pharyngeal pouches around the 4th week of development forming most of the thyroid parenchyma. The neural crest cells from the 4th and 5th lateral pharyngeal pouches contribute in the formation of parafollicular C cells. In the 3 following weeks, the primitive thyroid tissue descends from the foramen caecum, anterior to the hyoid bone and laryngeal cartilages, to reach its final pretracheal location, and then the diverticulum pathway retracts forming the thyroglossal duct which involutes later [1], [2], [7].
Abnormal descent of the thyroid gland leads to an ectopic thyroid mostly located in the midline area of its descending path described as lingual (90%), sublingual, thyroglossal or intralatyngotracheal. The occurrence of ectopic thyroid tissue in a non-midline site is extremely rare and can be found as lateral neck lymphatic nodules, on the pericardium, or on the cervical oesophagus and can be mistaken for neoplastic disease [1], [2], [5]. This ectopic entity may represent the only functional thyroid tissue in the body [4].
Since they share the same structure, any lesion which affects the main thyroid gland may also involve the ectopic thyroid remnants, including cysts, nodular goiter and carcinomas [3]. Indeed, primary thyroid carcinomas arising from ectopic thyroid tissue are uncommon, mostly reported in the thyroglossal cysts, lateral aberrant thyroid tissue, lingual and mediastinal thyroid and struma ovarii. The main histological types are papillary, mixed papillary and follicular carcinomas or Hurthle cell tumours [8].
The lateral cervical location of ectopic thyroid tissue (1–3%) was considered first as an embryological variation since it originated from lateral thyroid remains deposited outside the gland as it descended from the base of the tongue to the triangular cervical muscles. Presently, multiple authors relate its origin to a metastatic deposit of well-differentiated thyroid carcinoma. The absence of lymph node tissue in the pathology study could be explained by the total replacement of the lymphoid tissue by the thyroid carcinoma [2]. However, the ectopic tissue can, in rare cases, include a primary thyroid carcinoma [1], [4].
As a result, precise incidence and prevalence data of lateral neck ectopic thyroid carcinomas are lacking, secondary to the difficulty of identifying metastatic diseases related to a thyroid primary carcinoma from the true primary malignancy of these ectopic tissue [4].
The discovery of papillary carcinoma on ectopic thyroid tissue raises the possibility of an occult primary in the thyroid gland and should indicate an exploration of the gland or even removal of at least the ipsilateral lobe [5], [9].
In the case of primary carcinoma of ectopic thyroid tissue, regarding the lack of data, there are no evidence-based guidelines on the optimal treatment [4]. Simion et al. proposed total thyroidectomy with ipsilateral modified neck dissection followed by radioactive iodine therapy [10]. Agosto-Vargas et al. reported a case treated with total thyroidectomy followed by radiation therapy [4].
4. Conclusion
Lateral neck ectopic thyroid carcinomas remain a rare entity. They present difficulty to distinguish metastatic diseases related to a thyroid primary carcinoma from true primary malignancy of the ectopic tissues. Thus, the discovery of papillary carcinoma on ectopic thyroid tissue raises the possibility of an occult primary in the thyroid gland and should indicate an exploration of the gland, by imaging techniques first.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Sources of funding
None.
Ethical approval
Ethical approval has been exempted by our institution.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contribution
El Bouhmadi Khadija: Corresponding author and writing the paper
Oukessou Youssef: Study concept
Sami Rouadi: study concept
Abada Reda: study concept
Roubal Mohamed: correction of the paper
Mahtar Mohamed: correction of the paper
Research registration
N/A.
Guarantor
El Bouhmadi Khadija.
Declaration of competing interest
None.
References
- 1.Policeni Bruno A., Smoker Wendy R.K., Reede Deborah L. Anatomy and embryology of the thyroid and parathyroid glands. Semin. Ultrasound CT MR. 2012;33(2):104–114. doi: 10.1053/j.sult.2011.12.005. ISSN 0887-2171. [DOI] [PubMed] [Google Scholar]
- 2.Sánchez Fuentes M.N., Miguelena Bobadilla J.M., Casamayor Franco M.C., Barranco Domínguez J.I., Dobón Rascón M.Á. Tumor laterocervical de cuello: tiroides ectópico vs. metástasis de carcinoma tiroideo diferenciado. Cir. Esp. 2015;93:e115–e117. doi: 10.1016/j.ciresp.2013.10.007. [DOI] [PubMed] [Google Scholar]
- 3.Smithers D.W. Carcinoma associated with thyroglossal duct anomalies. Monogr. Neoplast. Dis. Var. Sites. 1970;6:155–161. PMID: 4950331. [PubMed] [Google Scholar]
- 4.Agosto-Vargas Yanerys., Gutiérrez Madeleine, Martínez José Hernán, Mangual-Garcia Michelle, Palermo Coromoto, Vélez-Maymi Sharon, Hernández-Vázquez Luis, Miranda-Rodríguez Samayra, González-Bossolo Alex, Solá-Sánchez Ernesto, Hernández-Negrón Marianne. Papillary thyroid carcinoma: ectopic malignancy versus metastatic disease. Case Rep. Endocrinol. 2017;2017 doi: 10.1155/2017/9707031. 3 pages. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Feisal T.K., Prepageran N., Shahrizal T., Zulkiflee A.B. Unusual parapharyngeal lesion: aberrant thyroid gland. Singap. Med. J. 2008 May;49(5):e137–e138. PMID: 18465039. [PubMed] [Google Scholar]
- 6.Agha R.A., Franchi T., Sohrabi C., Mathew G., for the SCARE Group The SCARE 2020 guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int. J. Surg. 2020;84:226–230. doi: 10.1016/j.ijsu.2020.10.034. [DOI] [PubMed] [Google Scholar]
- 7.Hebbar K.A., K S, Deshmane V.L., Kumar V., Arjunan R. Papillary carcinoma in median aberrant thyroid (ectopic) - case report. J. Clin. Diagn. Res. 2014;8(6) doi: 10.7860/JCDR/2014/7626.4463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Shah B.C., Ravichand C.S., Juluri S., Agarwal A., Pramesh C.S., Mistry R.C. Ectopic thyroid cancer. Ann. Thorac. Cardiovasc. Surg. 2007 Apr;13(2):122–124. PMID: 17505421. [PubMed] [Google Scholar]
- 9.Clay R.C., Blackman S.S. Lateral aberrant thyroid: metastasis to the lymph nodes from primary carcinoma of the thyroid gland. Arch. Surg. 1944;48(3):223–228. doi: 10.1001/archsurg.1944.01230010231007. [DOI] [Google Scholar]
- 10.Simion N.I., Muntean V. Cervical lymphadenopathy: metastasis of papillary carcinoma or ectopic thyroid tissue? BMJ Case Rep. 2012;2012 doi: 10.1136/bcr.01.2012.5603. [DOI] [PMC free article] [PubMed] [Google Scholar]