

Abstract
Aim
This study aimed to assess the nurses' knowledge, concerns, perceived impact and preparedness toward the COVID‐19 pandemic.
Background
As COVID‐19 is a new disease, its spread and emergence cause fear, anxiety and confusion among the general population. Nurses are in close contact with infected persons, and their knowledge plays an important role in preventing the transmission chain.
Methods
In this cross‐sectional study, 207 nurses were selected using convenience sampling from 29 March to 19 April 2020. The study used a questionnaire assessing the nurses' baseline characteristics, their source of information, knowledge, concerns, the perceived impact and their preparedness for the COVID‐19 pandemic.
Results
Around half of the surveyed nurses (51.2%) reported that the Ministry of Health's and World Health Organization's websites and official pages were their main sources of information. The majority of nurses (81.6%) knew the nature of the virus, 83.6% agreed that their job puts them at risk of infection with COVID‐19 and 72% felt personally prepared for the pandemic.
Conclusion
The majority of nurses had an acceptable level of knowledge regarding COVID‐19. However, psychological interventions are needed to be addressed in the planning stage before any pandemic.
Keywords: concerns, COVID‐19, knowledge, nursing, perceived impact, preparedness
Summary statement
What is already known about this topic?
It is well established that COVID‐19 is a highly infectious disease with a fatality rate of about 6.48% in Egypt.
Studies about nursing and COVID‐19 are relatively few.
There is a lack of data regarding the nurses' knowledge, concerns, perceived impact and preparedness toward COVID‐19.
What does this paper add?
Nurses prefer gaining their knowledge regarding COVID‐19 from the Ministry of Health's and the World Health Organization's websites and official pages rather than the social media websites.
Nurses have an acceptable level of knowledge regarding COVID‐19. The majority of surveyed nurses knew the nature of the virus along with its signs and symptoms.
The majority of surveyed nurses feel that their job puts them at the risk of infection with COVID‐19, and they are quite afraid of being infected.
The implications of this paper:
Psychological interventions are needed in the planning stage before any pandemic to enhance the protection of nurses and health care workers and to reduce the psychological impact.
Sustainable awareness programmes are required for health care workers, keeping them up to date with the most recent information regarding prevention and management methods from the World Health Organization's guidelines and other instructional materials.
Hospitals can hold meetings and organize regular psychological support groups to allow nurses to manage their fears and acquire stress reduction strategies.
1. INTRODUCTION
Since December 2019, the novel coronavirus disease (COVID‐19) has spread from Wuhan city to different areas in China and around the world (Wang et al., 2020). On 11 March 2020, the World Health Organization (WHO) announced the COVID‐19 outbreak as a pandemic (Shi et al., 2020). On 21 April 2020, the confirmed number of patients changed into 2 555 760 with around 75 254 new cases globally (Karasneh et al., 2020). On 14 February, Egypt reported its first COVID‐19 case. Accordingly, Egypt scaled up measures of prevention, with a fractional lockdown starting on 25 March 2020. On 31 March, Egypt reported 710 more COVID‐19 cases and confirmed 46 related deaths with a fatality rate of 6.48% (Hassany et al., 2020).
The high risk of infection, generic and non‐specific traits of COVID‐19 and vigorous progression of the virus make COVID‐19 a very important subject in the medical world. The incubation period for COVID‐19 lasts between 1 and 14 days (Saba & Elsheikh, 2020). In terms of symptoms, the main signs and symptoms of the virus are dry cough, myalgia, fever, breathing difficulties, fatigue and pneumonia. Besides, there might be some complications including shock, secondary infection, acute respiratory distress syndrome, acute renal injury, arrhythmia and acute cardiac injury, and it might lead to death in the most severe cases (Huang et al., 2020; Lei et al., 2020).
A wide range of healthcare workers are involved in caring for cases of this highly infectious virus. However, the literature suggests that misunderstandings and lack of awareness about the virus as well as the poor infection control practices among the health care providers result in delaying diagnoses and increase the risk of infection (Omrani & Shalhoub, 2015; Saqlain et al., 2020). As nurses are in close contact with COVID‐19 cases, they are likely an essential piece of the infection transmission chain. Therefore, developing their knowledge, as well as increasing the preventive and protective measures toward COVID‐19, might help them in preventing the transmission chain (Nemati et al., 2020). Besides, as COVID19 is a novel virus, so its spread and emergence cause anxiety, confusion and dread among the general population. Dread and fear lead to feelings of disdain and stigma. Trauma could be the result of being isolated; being in direct contact with the infected cases; looking after them, for instance, or being in high‐risk positions. Consequently, the mental health of the medical and nursing staff might be impacted (Kang et al., 2020; Roy et al., 2020).
Prior research has investigated the health care workers' knowledge and attitudes during an epidemic (Angelillo et al., 2001; Askarian et al., 2007; Daugherty et al., 2009; Sarani et al., 2015). In 2009, a study, investigating the knowledge and attitudes of the medical staff concerning the H1N1 influenza pandemic, found that the willingness of health care workers to look after patients infected with H1N1 reported by only 82.3% of clinicians (Ma et al., 2011). Also, other research has reported that health care workers had inadequate knowledge and attitude toward the Severe Acute Respiratory Syndrome and Middle East Respiratory Syndrome (Alsahafi & Cheng, 2016; Althomairy et al., 2018). Moreover, based on the previous responses to the unexpected spread of severe acute respiratory syndrome, health care workers showed psychological distress gradually. With the early outbreak of the epidemic, anxiety, dread and fear decreased and then appeared immediately, but trauma symptoms, psychophysiological symptoms and depression appeared later on and lasted for a long time, causing profound outcomes (Wu et al., 2009).
Epidemics and pandemics are a periodic phenomenon. People in the community face various challenges during such periods. Inadequate knowledge often leads to an unconcerned attitude, which may adversely influence the preparedness to face these challenges (Roy et al., 2020). To best of our knowledge, this is the first study that has thoroughly assessed the nurses' knowledge, concerns, perceived impact and preparedness toward COVID‐19 pandemic in Egypt.
Nurses are under enormous pressure when working with patients with COVID‐19. However, at the same time, the fact that the information about the virus was newly discovered at that time required the information obtained to be transferred to the application area quickly. This situation has led to the nurses' concerns and fears about how to cope with the virus. For this reason, understanding the knowledge and concerns they have in the epidemic situation is important for managing the pandemic and predicting the outcomes of COVID‐19 in Egypt. Additionally, understanding these issues will help support nurses by informing leaders and decision‐makers about these issues and providing recommendations and implications.
2. METHODS
2.1. Aim
The study aimed to assess the nurses' knowledge, concerns, perceived impact and preparedness toward the COVID‐19 pandemic.
2.2. Study design
This study was conducted using the cross‐sectional design based on a self‐administered questionnaire. It followed the guidelines for reporting Observational Studies: Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement.
2.3. Participants
The participants in the present study were a convenience sample of 207 nurses working in Mansoura University Hospitals before receiving the Personal Protective Equipment (PPE) Training at the Faculty of Nursing at Mansoura University in Egypt. Post hoc power analysis was done online (https://www.sphanalytics.com/statistical-power-calculator-using-average-values/) with sample mean 27.65 and SD = 2.26, precision of 5% and sample size of 207; then the study power is 100%. This reflects adequacy of the sample size.
2.4. Data collection tools
A self‐administered questionnaire consisted of four sections was used. The first section assessed baseline characteristics included sex, age, residence, marital status, having children or not, family members, level of education, experience, caring for COVID‐19 patients or not and one item regarding the source of information about COVID‐19.
The second section assessed the nurses' knowledge. This section comprised of 15 items which were mainly adapted from the interim guidance and information for health care workers, published by the Centers for Disease Control and Prevention (2020), the WHO course materials on emerging respiratory viruses including COVID‐19 (WHO, 2020a) and the WHO Question and Answer about COVID‐19 (WHO, 2020b). The nurses were asked about what they know regarding the nature of the disease (one item), manifestations (four items), risk group (one item), transmission (four items), the incubation period (one item), management (three items) and precautions/preventions (one item). Participants could have chosen one of three responses: yes, no or I don't know. Responses were made on a 3‐point Likert scale: incorrect (0), I don't know (1) and correct (2). The score of knowledge ranged from 0 to 30. Higher scores indicated more acceptable knowledge levels.
The third and the fourth sections were adapted from a previous study by Al Ghobain et al. (2017) towards the Middle East Respiratory Syndrome Coronavirus. The third section assessed nurses' concerns which comprised nine items assessing work‐related concerns (four items) and non‐work‐related concerns (five items). Responses are made on a 3‐point Likert scale: disagree (0), neutral (1) and agree (2). The score of concerns section ranged from 0 to 18. A higher score indicated higher concerns expressed by surveyed nurses. The fourth section included 10 items about the perceived impact of COVID‐19 on nurses (5 items) and their preparedness for COVID‐19 pandemic (5 items) before the time of data collection. Responses were made on a 3‐point Likert scale: disagree (0), neutral (1) and agree (2). Both scores of perceived impact and preparedness ranged from 0 to 10. A higher score indicated higher perceived impact and preparedness expressed by surveyed nurses.
2.4.1. Questionnaire translation, validity and reliability
First, the questionnaire was translated into Arabic language following the forward and back translation procedure, being customized to be suitable for the Egyptian culture. Second, the study questionnaire was sent to the nursing and medical professionals to give their feedback regarding its importance, relativity and simplicity. Third, researchers carried out a pilot study on a small sample of nurses (n = 30), and after getting into discussions with them, they recommended that the questionnaire should be shorter, simpler, clearer and more comprehendible. The pilot study component of the research helped the researchers to improve the reliability and to achieve a degree of the face and content validity, by clarifying measurement fit and specifying content in different constructs (Neuman, 2014). The pilot study data were not used for the final analysis. The reliability coefficient was calculated by using SPSS v.22, and the value of Cronbach's alpha was found to be 0.8 for knowledge sections, 0.79 for the concerns section and 0.76 for the perceived impact and preparedness section.
2.5. Procedure and data collection process
This study was first conducted on 29 March 2020 and lasted for 3 weeks to 19 April 2020. The Faculty of Nursing in Mansoura University organized a PPE Training for nurses, working in Mansoura University Hospitals, to prepare them to deal with the COVID‐19 pandemic. The nurses who signed up to attend the training were divided into groups; the number of each group members ranged from 10 to 20 nurses. However, the principle of social distancing was strictly applied and followed. The training programme for each group lasted for 1 day. Groups changed every day. Nurses who approved of taking part in the study asked to fill out a self‐administered questionnaire before starting the training. The average completion time of the survey was 10 min.
2.6. Ethics statement
The permission to conduct the study was obtained from the Faculty of Nursing at Mansoura University. After explaining to them in detail what kind of study was it, the nurses were asked if they would like to participate, and they were told that it was a voluntary task. So they were free to accept to participate or to decline participation altogether. They were assured that all data would be treated in a confidential way and publications would include aggregate data only. Their verbal consent was given.
2.7. Data analysis
The data were analysed with SPSS version 22. All of the categorical data were summarized as percentages and frequencies. The normality of data was first tested with a one‐sample Kolmogorov–Smirnov test. Continuous variables were presented as Median and range for non‐parametric data. Spearman correlation test was used to correlate continuous to non‐ parametric data. Results were considered significant when the probability of error was less than 5% (P < 0.05), non‐significant when the probability of error was more than 5% (P > 0.05) and highly significant when the probability of error was less than 0.1% (P < 0.001). The smaller the P value obtained, the more significant were the results.
3. RESULTS
Nurses' baseline characteristics are presented in Table 1. A total number of 207 nurses participated in this study. The majority of participants were female nurses (77.8%), around 50% aged between 25 and 30 years old; 84.5% were living in rural areas; the majority were married (81.2%); around two fifths held bachelor degrees in nursing (39%) and 43.5% had a work experience of 1 to less than 5 years. Most of the nurses (96.1%) did not have direct contact with patients infected with COVID‐19.
TABLE 1.
Baseline characteristics of participants (N = 207)
| Baseline characteristics | N (%) | |
|---|---|---|
| Sex | Male | 46 (22.2) |
| Female | 161 (77.8) | |
| Age in years | Up to 25 | 45 (21.7) |
| 25: < 30 | 100 (48.3) | |
| 30: 35 | 32 (15.5) | |
| More than 35 | 30 (14.5) | |
| Residence | Urban | 32 (15.5) |
| Rural | 175 (84.5) | |
| Marital status | Unmarried (divorced and single) | 39 (18.8) |
| Married | 168 (81.2) | |
| Have children | Yes | 169 (81.6) |
| No | 38 (18.4) | |
| Family members | 2 | 10 (4.8) |
| 3 | 89 (43) | |
| 4 | 66 (31.9) | |
| More than 4 | 42 (20.3) | |
| Levels of education |
Nursing diplomat (intermediate education) |
62 (30) |
|
Nursing technical institute (upper‐intermediate education) |
50 (24.2) | |
|
Bachelor's degree in nursing (high education) |
81 (39) | |
|
Master's degree in nursing (post‐graduate) |
14 (6.8) | |
| Experience (years) | Up to 1 | 20 (9.7) |
| 1: <5 | 90 (43.5) | |
| 5: 10 | 31 (15) | |
| More than 10 | 66 (31.8) | |
| Provided care for a COVID‐19 patient | Yes | 8 (3.9) |
| No | 199 (96.1) | |
Figure 1 illustrates the sources of information utilized by nurses to look for information regarding COVID‐19. Around half of the surveyed nurses (51.2%) reported that the Ministry of Health's and World Health Organization's websites and official pages were their main sources of information followed by social media networks (25.1%), friends and colleagues (12.6%) and online courses (11.1%).
FIGURE 1.
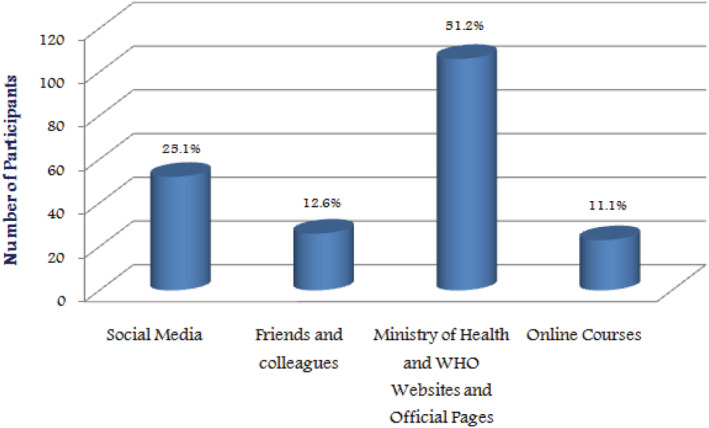
Information sources reported by participants (N = 207)
Table 2 shows frequencies of correct answers of items assessing basic knowledge regarding COVID‐19. The majority of nurses (81.6%) knew the nature of the virus. The vast majority of them (91.3%) answered correctly that cough, fever and difficulty breathing were the most common manifestations of COVID‐19. Most of the nurses (96.1%) knew that the elderly and people with chronic diseases were more likely to be infected, and more than three quarters (78.7%) knew that COVID‐19 can be transmitted in all regions, including hot and humid regions. All of the nurses (100%) knew that people could be infected by infection from other people who are infected with the virus, and 88.4% knew that the COVID‐19 incubation period ranges from 1 to 14 days, and most often, it lasts for 5 days. Around half of the nurses (48.8%) answered correctly that most people recover from COVID‐19 without the need for special treatment. Almost most of the nurses (97.1%) knew the most effective ways to protect themselves and others from the emerging COVID‐19.
TABLE 2.
Knowledge of participants about COVID‐19 (N = 207)
| Statements | N (%) correct answers |
|---|---|
| 1. Coronaviruses are groups of widespread viruses known to cause infectious diseases ranging from the common cold to more severe diseases, such as Severe Acute Respiratory Syndrome and Middle East Respiratory Syndrome. | 169 (81.6) |
| 2. Common signs of COVID‐19 infection include respiratory symptoms, fever, cough, difficulty breathing, nasal congestion, dyspnea, sore throat, myalgia or diarrhoea | 189 (91.3) |
| 3. In the most severe cases, infection with COVID‐19 may cause pneumonia, severe acute respiratory syndrome, kidney failure and even death. | 171 (82.6) |
| 4. Usually, the symptoms of infection with COVID‐19 are mild and are beginning gradually. | 161 (77.8) |
| 5. Some cases become infected without feeling ill and without exhibiting manifestations. | 175 (84.5) |
| 6. People with old age or with chronic illnesses such as diabetes mellitus, hypertension and cardiac diseases are more likely to be infected with COVID‐19. | 199 (96.1) |
| 7. COVID‐19 can be transmitted in all regions, including hot and humid regions. | 163 (78.7) |
| 8. People can be infected with COVID‐19 by infection from other people who are already infected. | 207 (100) |
| 9. Transmission of COVID‐19 between people can be through small droplets scattered from the mouth or nose when the infected case sneezes or coughs. | 206 (99.5) |
| 10. When these droplets fall on the surfaces or objects surrounding the infected case, then other people can become infected with COVID‐19 when they come into contact with these surfaces or objects and then touch their mouth, nose or eyes. | 206 (99.5) |
| 11. The incubation period of COVID‐19 ranges from 1 to 14 days and usually lasts 5 days. | 183 (88.4) |
| 12. Most people recover from COVID‐19 without the need for special treatment. | 101 (48.8) |
| 13. Antibiotics should not be used as a means of preventing or treating the emerging COVID‐19. | 169 (81.6) |
| 14. To this day, there is neither a specific antiviral drug nor a vaccine to treat or prevent COVID‐19. | 189 (91.3) |
| 15. The most effective methods for protection are persisting in cleaning hands, covering the mouth when coughing by tissue or bending the elbow and staying at least 1 m (3 feet) away from a person who sneezes or coughs. | 201 (97.1) |
| Median = 28 range = 8 min‐max = 22–30 | |
Results in Table 3 summarize work and non‐work‐related concerns as experienced by nurses. The majority of nurses (83.6%) agreed that they were at risk of being infected with COVID‐19 because of their work. Around two fifths of them (41.5%) were afraid of being infected. On the other hand, only 2.9% of nurses felt that they should not care for patients with COVID‐19. Also, only 2.9% of them showed their willingness to leave their job and search for another. The majority felt that their job would expose their families (82.6%) and work colleagues (80.2%) to the risk of infection. Around two thirds reported that they felt that because of their work position, their parents (68.1%) and close friends (66.2%) were at high risk of COVID‐19 infection.
TABLE 3.
Work and non‐work‐related concerns of participants regarding COVID‐19 (N = 207)
| Statements | Disagree N (%) | Neutral N (%) | Agree N (%) |
|---|---|---|---|
| I. Work‐related concerns | |||
| 1. My job would put me at great risk of exposure | 20 (9.7) | 14 (6.8) | 173 (83.6) |
| 2. I am afraid of being infected with COVID‐19 | 28 (13.5) | 93 (44.9) | 86 (41.5) |
| 3. I should not be caring for COVID‐19 patients | 189 (91.3) | 12 (5.8) | 6 (2.9) |
| 4. I might change my job because of the risk | 195 (94.2) | 6 (2.9) | 6 (2.9) |
| II. Non‐work‐related concerns | |||
| 1. Family | 17 (8.2) | 19 (9.2) | 171 (82.6) |
| 2. Parents | 34 (16.4) | 32 (15.5) | 141 (68.1) |
| 3. Close friends | 17 (8.2) | 53 (25.6) | 137 (66.2) |
| 4. Work colleagues | 20 (9.7) | 21 (10.1) | 166 (80.2) |
| 5. Persons close to me would be worried about my health | 18 (8.7) | 26 (12.6) | 163 (87.7) |
| Total concerns | |||
| Median = 12 range = 15 min‐max = 3–18 | |||
Table 4 demonstrates the perceived impact of COVID‐19 and readiness for a pandemic. Around two thirds of nurses (67.6%) reported that they would be afraid of telling their families about the risk of their exposure to patients and infection, whereas only 15% agreed that because of their work, people would avoid dealing with them. More than half of nurses would have an increase in workload (58.5%). Regarding preparedness for COVID‐19, the majority of nurses attended infection control training (81.2%), agreed that their workplaces had sufficient infection control staff (85%) and agreed that their hospitals were well prepared to handle a COVID‐19 pandemic. Around three quarters of nurses (72%) felt personally prepared for COVID‐19.
TABLE 4.
Frequencies and percentages of responses to perceived impact on personal life, workload, and preparedness for COVID‐19 by participants (N = 207)
| Perceived impact and preparedness | Disagree N (%) | Neutral N (%) | Agree N (%) |
|---|---|---|---|
| Perceived impact | |||
| 1. Fear of telling my family about the risk I am exposed to. | 53 (25.6) | 14 (6.8) | 140 (67.6) |
| 2. Because of my job, persons would avoid me. | 98 (47.3) | 78 (37.7) | 31 (15) |
| 3. There would be inadequate staff in my hospital to control the increased emergencies. | 95 (45.9) | 65 (31.4) | 47 (22.7) |
| 4. Stress would be increasing at work. | 62 (30) | 27 (13) | 118 (57) |
| 5. Workload would be increasing. | 48 (23.2) | 38 (18.4) | 121 (58.5) |
| Median = 6 range = 10 min‐max = 0–10 | |||
| Preparedness | |||
| 6. I have received an infection control training | 39 (18.8) | 0 (0) | 168 (81.2) |
| 7. At the hospital where I work, there is sufficient infection control staff. | 14 (6.8) | 17 (8.2) | 176 (85) |
| 8. My workplace has a preparedness plan to deal with COVID‐19 pandemic. | 6 (2.9) | 23 (11.1) | 178 (86) |
| 9. I attended the PPE training. | 4 (1.9) | 12 (5.8) | 191(92.3) |
| 10. I am personally prepared for COVID‐19 | 10 (4.8) | 48 (23.2) | 149 (72) |
| Median = 9 range = 9 min‐max = 1–10 | |||
Spearman correlation test in Table 5 shows a statistically significant positive linear correlation between knowledge and concerns, perceived impact and preparedness scores as follows (r = 0.168, P = .016), (r = 0.389, P ≤ 0.001) and (r = 0.478, P ≤ 0.001), respectively.
TABLE 5.
Correlation between scores of Nurses' knowledge, concerns, perceived impact and preparedness for COVID‐19
| Variable | Correlation coefficient (r) | P value |
|---|---|---|
| Knowledge – concerns | 0.168 | 0.016 * |
| Knowledge – perceived impact | 0.389 | ≤0.001 * |
| Knowledge – preparedness | 0.478 | ≤0.001 * |
| Concerns ‐ perceived impact | 0.334 | ≤0.001 * |
| Concerns ‐ preparedness | −0.124 | 0.075 |
Note: (r) Spearman correlation.
Statistically significant at P < 0.05.
4. DISCUSSION
The present study findings revealed that nurses preferred gaining knowledge about COVID‐19 from the Ministry of Health's and the WHO's websites and official pages rather than the social media networks which might spread fake news and misinformation. There is a positive point to be highlighted here that nurses access official websites and pages for all the health‐related issues and pieces of information such as expected manifestations and the most appropriate methods in preventing transmission.
These findings are inconsistent with a study that reported that 87.68% of health care providers stated that their main source of information was the social media networks while only 23.19% seek information from seminars and workshops (Saqlain et al., 2020). Besides, Giao et al. (2020) reported social media as the main source of information regarding COVID‐19 used by 91.1% of health care workers followed by the Ministry of Health website used by 82.6%. Similarly, a study carried out on 453 health care providers found that more than 60% of respondents utilized social media networks to obtain knowledge about COVID‐19 (Bhagavathula et al., 2020). The difference between the results of these studies may be due to the fact that previous studies were carried out earlier than the current study during the pandemic period. Besides, it is quite noticeable that the nature of the COVID‐19 pandemic has made it vital for nurses to increase their knowledge corresponding to the importance of the situation and to make efforts to follow the guidelines, recommendations and reports published by both the Ministry of Health and the WHO.
The results in the current study demonstrated that nurses had an acceptable level of knowledge regarding COVID‐19. The majority of nurses knew the nature of the virus and its signs and symptoms such as cough, fever and dyspnea. Most of the nurses knew that the elderly and people with chronic diseases are more likely to be infected. All of the nurses knew that people could be infected from other people who are infected with the virus, and 88.4% knew that the COVID‐19 incubation period is between 1 day and 2 weeks and usually lasts for 5 days. Around half of the nurses answered correctly that most people recover from COVID‐19 without the need for special treatment. Almost of the nurses knew the best effective methods of protection for themselves and others from the emerging COVID‐19.
These findings are in line with a study assessing knowledge regarding COVID‐19 among health care professionals in Henan, China. Nurses compromised 46.5% of the study population. Results showed that 89% of health care workers had adequate knowledge about COVID‐19 (Zhang et al., 2020). Other studies, such as Giao et al. (2020), Saqlain et al. (2020) and Shi et al. (2020), demonstrated that 88.4%, 93.2% and 89.51% of health care workers, respectively, had adequate levels of knowledge about COVID‐19.
Moreover, another study concluded that the median knowledge score regarding COVID‐19 outbreak and guidelines of infection control was four out of five. The participants answered correctly as the following: 76.9% aware that COVID‐19 is single‐stranded RNA, 90.4% knew that respiratory droplets are the main source of transmission, 86.5% knew that cough and fever are the most common manifestations and only 40.4% knew that the period of 5 days is the most accurate estimation of the incubation period (Alhaj et al., 2020). Another study conducted on nurses revealed that more than 50% of the nurses had sufficient knowledge about COVID‐19 (Nemati et al., 2020). On the other hand, another study found that health care providers had insufficient knowledge regarding COVID‐19 manifestations, transmission, prevention and treatment (Bhagavathula et al., 2020).
Results of the present study indicated that the majority of nurses felt that their job puts them at the risk of being infected with COVID‐19 and they were afraid of being infected. Another interesting finding is most of the nurses were willing to provide care for COVID‐19 patients. This result reflects that the surveyed nurses have a professional obligation and high standards of ethical values towards their patients and their jobs. The surveyed nurses experienced concern for their own families, parents, work colleagues and close friends. The probable reasons for these concerns might be the rapid spread of the highly infectious virus, the difficulty in controlling the pandemic and the fear of being infected. A pilot study carried out in Saudi Arabia, in which the majority of subjects were nurses, found that the well‐being of families and colleagues and the fear for personal safety were the main sentiments that had been focused on by the health care workers (Khalid et al., 2016).
The current findings are in line with the findings of another study reported that about 85% of the participants had a fear of being infected at their work (Zhang et al., 2020). Also, a previous study conducted on 85 nurses revealed that nurses displayed a feeling of anxiety toward themselves and their families (Nemati et al., 2020). Moreover, in China, Huang and Zhao (2020) in a study carried out during the COVID‐19 pandemic found that the surveyed health care professionals experienced elevated levels of anxiety compared to others. Moreover, another study indicated that 77.17% of health care workers were willing to look after psychotic patients experiencing COVID‐19 (Shi et al., 2020). Besides, one more study result reported that health care workers had a significant concern about dealing with infected patients and in turn pass the virus to their families, especially their parents (Giao et al., 2020). Conversely, rates of absenteeism among health care workers reached 36% because of the influenza pandemic as reported in an Australian study (Martinese et al., 2009).
The current study results showed that 67.6% of nurses have fears about telling their family about the risk they are exposed to and more than half reported increasing workload and stress. Perhaps the nurses' concealment of their interaction with patients infected with the virus is due to their fear of others avoiding them as a kind of stigma afflicts them. It is also possible that the nurses' feelings may play a role. It is possible that they do not prefer to worry their families about them as a result of dealing with infected patients. Moreover, nurses expressed fear of the virus and evaluated it as a factor that creates stress and increases workload. They are also afraid of transmitting the virus to their loved ones or colleagues. Besides, the increasing numbers of sick patients and the importance of the nursing care provided to them in light of adherence to all precautionary measures might also play an important in increasing workload and stress.
Other positive findings of the present study were that the majority of nurses received training regarding infection control. Also, they agreed that their workplaces have sufficient infection control staff and agreed that their hospitals are well prepared to handle a COVID‐19 outbreak. Also, around three quarters of nurses felt personally prepared for COVID‐19. Perhaps the reason for this is the nurses' feeling of responsibility towards their vital role in facing the virus, and it is possible that their concern about the virus led to the nurses' pursuit and their workplaces to hold more training to face the pandemic. The evidence for that explanation is that 81.2% of nurses attended infection‐control training sessions, 86% of them saw that their workplaces had a pandemic preparedness plan and 92.2% attended PPE training. Previous studies conducted on medical staff in Chinese psychiatric hospitals revealed that 64.63% of participants attended training sessions regarding how to deal with COVID‐19 (Shi et al., 2020). Besides, Alhaj et al. (2020) reported in their study that less than 50% of the health care workers and more than two thirds expressed preparedness for looking after COVID‐19 patients.
4.1. Strengths and limitations
The findings provide needed information about the knowledge, concerns, perceived impact and preparedness of nurses toward the COVID‐19 pandemic. There is a dearth of research on COVID‐19 and nursing. The present study highlighted a less explored area where scarce literature is available.
The study used the WHO guidelines and recommendations regarding COVID‐19 to design a validated questionnaire. The designed questionnaire was pilot tested and not did not have any open‐ended questions to reduce bias with regard to information given. This is a cross‐sectional study conducted on nurses who attended the PPE Training sessions in the Faculty of Nursing at Mansoura University in Egypt. The present study data are self‐reported and partly based on the participants' honesty and recalling ability or good memory; thus, they might be subject to recall bias. As the COVID‐19 is a novel disease, the standardized and validated instruments are still unavailable. The questionnaire was developed in a form of true/false questions. The probability of guessing the correct answer is high approximately 50%, and nurses can just check an answer without any comprehension of the question.
5. CONCLUSION
In conclusion, this study provides evidence about the adequacy of knowledge of the surveyed nurses about COVID‐19 during the pandemic. Also, nurses felt prepared for the COVID‐19 pandemic—both personally and professionally. This study raises some important concerns about the psychological impact of COVID‐19 pandemic on nurses due to the fear of infections. There is a clear need for psychological interventions to be addressed in the planning stage before any pandemic so as for enhancing the protection of nurses and health care workers and to reduce the psychological impact.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest.
FUNDING INFORMATION
The financial support for this study was provided by the authors themselves.
AUTHORSHIP STATEMENT
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing or revision of the manuscript. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication before its appearance in the International Journal of Nursing Practice. AHE had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study design: AHE, MA, and YE. Questionnaire development: AHEl, YEl, and ASA. Data collection: AHE and ASA. Pilot study: ASA. Statistical and data analysis: AHEl, MA, MZ. Manuscript drafting: AHE, MA, ASA, and YE. Manuscript revision: All authors have read, reviewed and approved the final manuscript before submission.
ACKNOWLEDGEMENTS
The authors would like to thank all nurses for their voluntary participation in the study and for being at the forefront in the daily battle against infectious diseases.
El‐Monshed, A. H. , Amr, M. , Ali, A. S. , Elmasry, Y. M. , & Zoromba, M. (2021). Nurses' knowledge, concerns, perceived impact and preparedness toward COVID‐19 pandemic: A cross‐sectional survey. International Journal of Nursing Practice, 27(6), e13017. 10.1111/ijn.13017
REFERENCES
- Al Ghobain, M. , Aldrees, T. , Alenezi, A. , Alqaryan, S. , Aldabeeb, D. , Alotaibi, N. , Aldhabib, A. , Alghalibi, S. , & Alharethy, S. (2017). Perception and attitude of emergency room resident physicians toward Middle East respiratory syndrome outbreak. Emergency Medicine International, 2017, 1–4. 10.1155/2017/6978256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alhaj, A. K. , Al‐Saadi, T. , Mohammad, F. , & Alabri, S. (2020). Neurosurgery residents perspective on the COVID‐19: Knowledge, readiness, and impact of this pandemic. World Neurosurgery, 139, e848–e858. 10.1016/j.wneu.2020.05.087 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alsahafi, A. J. , & Cheng, A. C. (2016). Knowledge, attitudes and behaviours of healthcare workers in the kingdom of Saudi Arabia to MERS coronavirus and other emerging infectious diseases. International Journal of Environmental Research and Public Health, 13(12), 1214. 10.3390/ijerph13121214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Althomairy, S. , Baseer, M. , Assery, M. , & Alsaffan, A. (2018). Knowledge and attitude of dental health professionals about middle east respiratory syndrome in Saudi Arabia. Journal of International Society of Preventive and Community Dentistry, 8(2), 137–144. 10.4103/jispcd.jispcd_9_18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Angelillo, I. F. , Viggiani, N. M. A. , Greco, R. M. , & Rito, D. (2001). HACCP and food hygiene in hospitals knowledge, attitudes, and practices of food‐services staff in Calabria, Italy. Infection Control and Hospital Epidemiology, 22(6), 363–369. 10.1086/501914 [DOI] [PubMed] [Google Scholar]
- Askarian, M. , McLaws, M. L. , & Meylan, M. (2007). Knowledge, attitude, and practices related to standard precautions of surgeons and physicians in university‐affiliated hospitals of shiraz, Iran. International Journal of Infectious Diseases, 11(3), 213–219. 10.1016/j.ijid.2006.01.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bhagavathula, A. S. , Aldhaleei, W. A. , Rahmani, J. , Mahabadi, M. A. , & Bandari, D. K. (2020). Knowledge and perceptions of COVID‐19 among health care workers: Cross‐sectional study. JMIR Public Health and Surveillance, 6(2), e19160. 10.2196/19160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention . (2020). Information for healthcare professionals about coronavirus (COVID‐19)|CDC. Retrieved March 3, 2020, from https://www.cdc.gov/coronavirus/2019-ncov/hcp/index.html
- Daugherty, E. L. , Perl, T. M. , Rubinson, L. , Bilderback, A. , & Rand, C. S. (2009). Survey study of the knowledge, attitudes, and expected behaviors of critical care clinicians regarding an influenza pandemic. Infection Control and Hospital Epidemiology, 30(12), 1143–1149. 10.1086/648085 [DOI] [PubMed] [Google Scholar]
- Giao, H. , Han, N. T. , Van Khanh, T. , Ngan, V. K. , Van Tam, V. , & Le An, P. (2020). Knowledge and attitude toward COVID‐19 among healthcare workers at district 2 hospital, Ho Chi Minh City. Asian Pacific Journal of Tropical Medicine, 13(March), 6–11. 10.4103/1995-7645.280396 [DOI] [Google Scholar]
- Hassany, M. , Abdel‐Razek, W. , Asem, N. , AbdAllah, M. , & Zaid, H. (2020). Estimation of COVID‐19 burden in Egypt. In The lancet infectious diseases (Vol. 20) (pp. 896–897). Lancet Publishing Group. 10.1016/S1473-3099(20)30319-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huang, C. , Wang, Y. , Li, X. , Ren, L. , Zhao, J. , Hu, Y. , Zhang, L. , Fan, G. , Xu, J. , Gu, X. , Cheng, Z. , Yu, T. , Xia, J. , Wei, Y. , Wu, W. , Xie, X. , Yin, W. , Li, H. , Liu, M. , … Cao, B. (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet, 395(10223), 497–506. 10.1016/S0140-6736(20)30183-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huang, Y. , & Zhao, N. (2020). Generalized anxiety disorder, depressive symptoms and sleep quality during COVID‐19 outbreak in China: A web‐based cross‐sectional survey. Psychiatry Research, 288, 112954. 10.1016/j.psychres.2020.112954 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kang, L. , Ma, S. , Chen, M. , Yang, J. , Wang, Y. , Li, R. , Yao, L. , Bai, H. , Cai, Z. , Xiang Yang, B. , Hu, S. , Zhang, K. , Wang, G. , Ma, C. , & Liu, Z. (2020). Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: A cross‐sectional study. Brain, Behavior, and Immunity, 87, 11–17. 10.1016/j.bbi.2020.03.028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karasneh, R. , Al‐Azzam, S. , Muflih, S. , Soudah, O. , Hawamdeh, S. , & Khader, Y. (2020). Media's effect on shaping knowledge, awareness risk perceptions and communication practices of pandemic COVID‐19 among pharmacists. Research in Social & Administrative Pharmacy, 17, 1897–1902. 10.1016/j.sapharm.2020.04.027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khalid, I. , Khalid, T. J. , Qabajah, M. R. , Barnard, A. G. , & Qushmaq, I. A. (2016). Healthcare workers emotions, perceived stressors and coping strategies during a MERS‐CoV outbreak. Clinical Medicine & Research, 14(1), 7–14. 10.3121/cmr.2016.1303 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lei, S. , Jiang, F. , Su, W. , Chen, C. , Chen, J. , Mei, W. , Zhan, L. Y. , Jia, Y. , Zhang, L. , Liu, D. , Xia, Z. Y. , & Xia, Z. (2020). Clinical characteristics and outcomes of patients undergoing surgeries during the incubation period of COVID‐19 infection. EClinicalMedicine, 21, 100331. 10.1016/j.eclinm.2020.100331 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ma, X. , He, Z. , Wang, Y. , Jiang, L. , Xu, Y. , Qian, C. , … Du, B. (2011). Knowledge and attitudes of healthcare workers in Chinese intensive care units regarding 2009 H1N1 influenza pandemic. BMC Infectious Diseases, 11, 1–7. 10.1186/1471-2334-11-24 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martinese, F. , Keijzers, G. , Grant, S. , & Lind, J. (2009). How would Australian hospital staff react to an avian influenza admission, or an influenza pandemic? EMA ‐ Emergency Medicine Australasia, 21(1), 12–24. 10.1111/j.1742-6723.2008.01143.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nemati, M. , Ebrahimi, B. , & Nemati, F. (2020). Assessment of Iranian Nurses' knowledge and anxiety toward COVID‐19 during the current outbreak in Iran. Archives of Clinical Infectious Diseases, 15(COVID‐19). 10.5812/archcid.102848 [DOI] [Google Scholar]
- Neuman, W. L. (2014). Social research methods: Qualitative and quantitative approaches (7th ed.). Harlow: Pearson Education Limited. [Google Scholar]
- Omrani, A. S. , & Shalhoub, S. (2015). Middle East respiratory syndrome coronavirus (MERS‐CoV): What lessons can we learn? In Journal of hospital infection (Vol. 91, Issue 3) (pp. 188–196). W.B. Saunders Ltd. 10.1016/j.jhin.2015.08.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roy, D. , Tripathy, S. , Kar, S. K. , Sharma, N. , Verma, S. K. , & Kaushal, V. (2020). Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID‐19 pandemic. Asian Journal of Psychiatry, 51, 102083. 10.1016/j.ajp.2020.102083 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saba, A. I. , & Elsheikh, A. H. (2020). Forecasting the prevalence of COVID‐19 outbreak in Egypt using nonlinear autoregressive artificial neural networks. Process Safety and Environmental Protection, 141, 1–8. 10.1016/j.psep.2020.05.029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saqlain, M. , Munir, M. M. , Rehman, S. U. , Gulzar, A. , Naz, S. , Ahmed, Z. , Tahir, A. H. , & Mashhood, M. (2020). Knowledge, attitude, practice and perceived barriers among healthcare professionals regarding COVID‐19: A cross‐sectional survey from Pakistan. The Journal of Hospital Infection, 105, 419–423. 10.1016/j.jhin.2020.05.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sarani, H. , Balouchi, A. , Masinaeinezhad, N. , & Ebrahimitabas, E. (2015). Knowledge, attitude and practice of nurses about standard precautions for hospital‐acquired infection in teaching hospitals affiliated to Zabol University of Medical Sciences (2014). Global Journal of Health Science, 8(3), 193–198. 10.5539/gjhs.v8n3p193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shi, Y. , Wang, J. , Yang, Y. , Wang, Z. , Wang, G. , Hashimoto, K. , Zhang, K. , & Liu, H. (2020). Knowledge and attitudes of medical staff in Chinese psychiatric hospitals regarding COVID‐19. Brain, Behavior, & Immunity ‐ Health, 4, 100064. 10.1016/j.bbih.2020.100064 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang, H. , Wang, Z. , Dong, Y. , Chang, R. , Xu, C. , Yu, X. , Zhang, S. , Tsamlag, L. , Shang, M. , Huang, J. , Wang, Y. , Xu, G. , Shen, T. , Zhang, X. , & Cai, Y. (2020). Phase‐adjusted estimation of the number of coronavirus disease 2019 cases in Wuhan, China. Cell Discovery, 6(1), 10. 10.1038/s41421-020-0148-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization|WHO . (2020a). Emerging respiratory viruses, including COVID‐19: methods for detection, prevention, response and control. Retrieved March 2, 2020, from https://openwho.org/courses/introduction-to-ncov [DOI] [PMC free article] [PubMed]
- World Health Organization|WHO . (2020b). Questions & answers on coronaviruses (COVID‐19). Retrieved March 3, 2020, from https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/q-a-coronaviruses
- Wu, P. , Fang, Y. , Guan, Z. , Fan, B. , Kong, J. , Yao, Z. , Liu, X. , Fuller, C. J. , Susser, E. , Lu, J. , & Hoven, C. W. (2009). The psychological impact of the SARS epidemic on hospital employees in China: exposure, risk perception, and altruistic acceptance of risk. Canadian Journal of Psychiatry, 54(5), 302–311. 10.1177/070674370905400504 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang, W. , Zhao, Y. , Zhang, F. , Wang, Q. , Li, T. , Liu, Z. , Wang, J. , Qin, Y. , Zhang, X. , Yan, X. , Zeng, X. , & Zhang, S. (2020). The use of anti‐inflammatory drugs in the treatment of people with severe coronavirus disease 2019 (COVID‐19): The experience of clinical immunologists from China. In Clinical Immunology (Vol. 214) (108393). Academic Press Inc. 10.1016/j.clim.2020.108393 [DOI] [PMC free article] [PubMed] [Google Scholar]