

Abstract
Objectives
This study aimed at revealing the caregiving challenges of the caregivers of people with dementia (PwD) during the COVID‐19 pandemic when daycare service was stopped as an infection control measure, and discussed ways to help PwD and their family caregivers to maintain their well‐being in the era of the pandemic.
Methods
Between April and May 2020, a cross‐sectional survey was conducted in 152 family caregivers of PwD who were clients of daycare service prior to the pandemic. The survey examined caregivers' stress and challenges faced during daycare service cessation, their perceived needs for continuation of daycare service, and observed changes in functional status of PwD. Regression analyses were performed to explore the associated factors of caregiving stress and preference for continuation of daycare service.
Results
Family caregivers of PwD experienced greater caregiving stress after cessation of daycare service. Infection was their main challenge in caregiving, and their physical and emotional health was adversely affected by the longer time commitment with PwD under the stay‐home policy. Older age of caregivers, greater emotional and communication problems of PwD, and more time spent with PwD were associated with greater caregiving stress. More than one‐third of the participants preferred the continuation of daycare service during the pandemic.
Conclusions
Policy makers should consider the well‐being of PwD and their caregivers when planning infection control measures. Daycare service with enhanced infection controlled measures should remain available to PwD during the COVID‐19 pandemic.
Keywords: caregiving stress, COVID‐19, daycare, dementia, functional decline
Key points
Family caregivers of PwD experienced greater caregiving stress during the COVID‐19 pandemic due to anxiety of infection and longer time commitment with PwD.
The cognitive function and mobility of PwD deteriorated after daycare service cessation because of the lack of cognitive, social, and physical activities with the stay‐home policy.
More than a third of family caregivers thought that continuation of daycare service during the COVID‐19 pandemic was important because it provided useful respite for the caregivers and a safer place for PwD to go to.
Online intervention could be an alternative form of social stimulation for PwD and may reduce caregiving stress.
1. INTRODUCTION
The coronavirus disease 2019 (COVID‐19) is caused by severe acute respiratory syndrome coronavirus 2, the first case was identified in Wuhan, People's Republic of China, in late December 2019. 1 As of 27 July 2021, there are more than 194 million confirmed cases and over four million confirmed deaths. 2 The outbreak of COVID‐19 leads to further challenge to people with dementia (PwD) and their caregivers in the sense that the infection control measures including cessation of daycare services, social distancing, and restricted caregiver visits in residential facilities deprive PwD of routine cognitive and social activities which is crucial to maintaining their cognitive and psychological health; in addition, social distancing and cessation of daycare service increases caregiving burden because the caregivers lack support from families, friends, and professional on their caregiving tasks. 3 , 4
People with dementia are associated to a higher risk of death when infected with COVID‐19, 5 , 6 , 7 the caregivers encounter the dilemma between keeping the PwD at home to reduce the risk of infection and letting their beloved ones go out for necessary rehabilitation. The uncertainty about the development of the pandemic and the worry about what measures are to the best interest of the care recipients creates distress to caregivers. 8 , 9 , 10 The practitioners of elderly service need to understand the unique challenges and worries encountered by the caregivers, so that appropriate measures can be implemented to facilitate the caregivers to carry out their caregiving tasks in the trying time of COVID‐19 pandemic.
In this study, we tried to investigate the difficulties and challenges encountered by the caregivers of PwD during the COVID‐19 pandemic. We hypothesized that the caregivers of PwD experienced greater caregiving stress, and the PwD had deteriorated functional condition during the COVID‐19 pandemic without the support of daycare service.
2. METHODS
2.1. Study design and participants
This study was conducted in a one time‐point cross‐sectional survey design through telephone interview by a trained researcher or through online self‐completion by the participants. The target participants of this study were caregivers of PwD. The inclusion criteria were: caregivers of people with any form of dementia using the daycare service in Hong Kong, the diagnosis of dementia was identified by the professional staff of the participating daycare centres, and the care recipients have suspended the daycare service during the COVID‐19 the pandemic. The exclusion criteria were: the caregivers who were not able to comment the observed deterioration of the care recipients, and visual or hearing problem that hinder interview or online self‐completion. The study was conducted between April and May 2020. The study was approved by the Survey and Behavioral Research Ethics Committee of the Chinese University of Hong Kong (Ref No.: SBRE‐19‐585).
In order to provide more information on the observed deterioration of PwD during daycare service cessation, the findings of the service evaluation of two of the participating centres (Jockey Club Centre for Positive Ageing and Jockey Club CADENZA Hub) were presented here as supplementary findings (Study 2). The two centres measured cognitive, mobility, and psychological parameters of service users with dementia and their caregivers (Supplementary Table 1) after the service users with dementia resumed daycare service so as to understand their updated condition. The data of PwD were collected by social workers, occupational therapists, and physiotherapists through face‐to‐face assessment, the data of caregivers were collected through telephone interview by a trained researcher or through caregiver self‐completion (hardcopy mail‐delivered assessment or online assessment constructed by Google Form). The data collection took place from February 2020 to January 2021. The data were compared with those within 12 months prior to daycare service cessation to understand the changes due to daycare cessation. Informed consent was obtained from the family caregivers of the PwD. Study 2 was approved by the Survey and Behavioral Research Ethics Committee of the Chinese University of Hong Kong (Ref No.: SBRE‐19‐680) and was registered in the Chinese Clinical Trial Registry (Ref.: ChiCTR2000033517). The two studies conformed to the Declaration of Helsinki – Ethical principles for medical research involving human subjects.
2.2. Procedures
Recruitment was done in 11 daycare centres providing daycare services to PwD with convenience and maximum sampling design. The social workers or nurses of the participating centres identified the service users with dementia from their admission records, then telephoned the caregivers whose care recipients had suspended daycare service during the period of data collection. After obtaining consent in oral manner, the contacts of the participants were passed to a trained researcher to conduct the telephone interview. The participants who preferred to self‐complete the survey were given an online questionnaire constructed using Google Forms for self‐completion. Informed consent (oral format by the researcher for telephone survey, or written format for online self‐completion) was obtained before data collection.
2.3. Outcomes
The survey questionnaire was constructed by the research team of Jockey Club Centre for Positive Ageing (JCCPA) based on literature review and pilot interviews with some caregivers, and was reviewed by two geriatricians and a social worker. The survey investigated the following areas: (1) caregiving difficulties during the COVID‐19 the pandemic: 16 prompted caregiving difficulties with yes/no responses plus an open‐ended, unprompted “others” option; (2) caregiving stress during daycare service cessation compared with time before cessation: five‐point Likert scale from “much greater stress” to “much less stress”; (3) observed care recipient condition during daycare service cessation: 5‐point Likert scale from “much worse” to “much better” in five domains: cognition, mobility, physical health, mood, and activities of daily living (taking reference of Lawton IADL Scale); (4) observed care recipient accidents or injuries during daycare service cessation: whether the care recipients had fall/home accident/hospital admission due to physical, mood, or behavioral problem/wandering during daycare cessation (yes/no), compared with time before service cessation for those having had such incidents during service cessation; (5) whether the caregivers thought that the daycare service should continue during the pandemic (yes/no), prompted reasons of their preference (yes/no), plus open‐ended, unprompted “others” option; (6) living condition during daycare service cessation: participants' work‐from‐home arrangement/whether they spent more time with the care recipients (more/same/less), whether the care recipients went out more or less (more/same/less). Demographic variables included the caregivers' relationship with care recipients, living condition of care recipients during the pandemic, days of service cessation, age (participant and care recipient), gender (participant and care recipient), and care recipients' stage of dementia reported by the participants.
2.4. Statistical analysis
The participant characteristics and survey responses were presented in descriptive data. This study had two primary outcomes: caregiving stress, and preference of daycare service during the pandemic. Regression analyses were conducted to examine the associated factors of these two outcomes. The independent variables were drawn based on existing literature and our available data, as listed in Tables 1 and 2. Univariate regression was conducted on the independent variables, and variables with p < 0.1 were included in the multivariate regression. Ordinal regression was conducted for the caregiving stress outcome, and binary logistic regression was conducted for the daycare service preference outcome. The data analysis was performed by SPSS version 26 (IBM Corp. Released 2019. IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp.), statistical significance was tested at p < 0.05. As for Study 2, the change of functional, psychological and caregiver burden variables before and after daycare service cessation was examined by paired samples t test.
TABLE 1.
Univariate and multivariate ordinal regression analysis on caregiving stress
| Univariate regression result | Multivariate regression result | |||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Age | ||||
| CG | 1.05 (1.02–1.08) | <0.001 a | 1.04 (1.00–1.07) | 0.036* |
| CR | 1.01 (0.97–1.04) | 0.701 | – | – |
| Gender | ||||
| CG (male) | 0.76 (0.35–1.68) | 0.501 | – | – |
| CR (male) | 1.57 (0.84–2.93) | 0.161 | – | – |
| CG relationship with CR (reference: others) | ||||
| Spouse | 1.34 (0.26–6.94) | 0.724 | – | – |
| Child/Child‐in‐law | 0.33 (0.07–1.59) | 0.167 | – | – |
| CG worked at home during pandemic | 1.24 (0.51–3.00) | 0.630 | – | – |
| CG spent more time with CR during pandemic | 3.76 (1.93–7.32) | <0.001 a | 4.02 (1.67–9.66) | 0.002* |
| CR went out more during pandemic | 2.07 (0.44–9.78) | 0.360 | – | – |
| Observed CR deterioration | ||||
| Cognition (worse) | 5.33 (2.63–10.82) | <0.001 a | 2.19 (0.90–5.34) | 0.084 |
| Mobility (worse) | 3.22 (1.64–6.32) | 0.001 a | 1.12 (0.47–2.64) | 0.799 |
| Physical health (worse) | 3.99 (2.07–7.69) | <0.001 | 1.60 (0.70–3.68) | 0.264 |
| Emotion (worse) | 7.45 (3.70–15.01) | <0.001 | 5.61 (2.48–12.67) | <0.001* |
| Communication (worse) | 4.44 (2.31–8.50) | <0.001 a | 2.33 (1.01–5.41) | 0.048* |
| Transportation (worse) | 0.96 (0.43–2.13) | 0.919 | – | – |
| Shopping (worse) | 0.95 (0.35–2.55) | 0.911 | – | – |
| CR living status during pandemic | ||||
| Lived with CG | 1.44 (0.75–2.75) | 0.268 | – | – |
| Lived with spouse | 1.43 (0.78–2.61) | 0.246 | – | – |
| Lived with child/child‐in‐laws | 0.43 (0.22−0.81) | 0.009 a | 0.24 (0.10−0.54) | 0.001* |
| Lived with other relatives | 0.57 (0.26–1.23) | 0.151 | – | – |
| Lived with maid | 0.54 (0.29–1.00) | 0.052 a | 0.58 (0.28–1.21) | 0.146 |
| Lived alone | 0.15 (0.01–1.52) | 0.108 | – | – |
| Observed CR dementia stage (reference: late) | ||||
| Early | 0.95 (0.33–2.72) | 0.920 | – | – |
| Moderate | 0.89 (0.39–2.01) | 0.775 | – | – |
Abbreviations: CG, Participant; CI, Confidence level; CR, Care recipient; OR, Odds ratio.
Variables with p < 0.1 in univariate regression were included in the multivariate regression: participant age; time spent with care recipient during the pandemic; observed care recipient deterioration of cognitive functioning, mobility, physical health, emotion, and communication; and whether the care recipient lived with child and maid; these variables also had good univariate model fit (test of parallel lines p > 0.05). The final model met the proportional odds assumption (χ 2 = 9.379, df = 18, p = 0.950).
*p < 0.05.
TABLE 2.
Univariate and multivariate logistic regression analysis on preference of daycare service
| Univariate regression result | Multivariate regression result | |||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Age | ||||
| CG | 1.00 (0.97–1.03) | 0.982 | – | – |
| CR | 0.97 (0.93–1.00) | 0.062 a | 0.96 (0.93–1.00) | 0.051 |
| Gender | ||||
| CG (male) | 0.92 (0.38–2.23) | 0.855 | – | – |
| CR (male) | 0.76 (0.37–1.53) | 0.441 | – | – |
| CG relationship with CR (reference: others) | ||||
| Spouse | 0.67 (0.12–3.73) | 0.644 | – | – |
| Child/Child‐in‐law | 0.51 (0.10–2.68) | 0.430 | – | – |
| CG worked at home during pandemic | 0.75 (0.28–2.01) | 0.568 | – | – |
| CG spent more time with CR during pandemic | 1.38 (0.67–2.81) | 0.381 | – | – |
| CR went out more during pandemic | 9.60 (1.09–84.42) | 0.041 a | 12.28 (1.28–117.92) | 0.030* |
| Observed CR deterioration | ||||
| Cognition (worse) | 3.15 (1.38–7.18) | 0.006 a | 3.53 (1.48–8.45) | 0.005* |
| Mobility (worse) | 2.66 (1.19–5.91) | 0.017 a | n.s. | n.s. |
| Physical health (worse) | 1.69 (0.86–3.34) | 0.129 | – | – |
| Emotion (worse) | 2.28 (1.14–4.54) | 0.019 a | n.s. | n.s. |
| Communication (worse) | 2.58 (1.31–5.08) | 0.006 a | n.s. | n.s. |
| Transportation (worse) | 2.19 (0.92–5.22) | 0.076 a | n.s. | n.s. |
| Shopping (worse) | 2.19 (0.75–6.41) | 0.153 | – | – |
| CR living status during pandemic | ||||
| Lived with CG | 0.83 (0.41–1.70) | 0.619 | – | – |
| Lived with spouse | 1.10 (0.57–2.15) | 0.773 | – | – |
| Lived with child/child‐in‐laws | 1.26 (0.62–2.56) | 0.519 | – | – |
| Lived with other relatives | 1.41 (0.61–3.26) | 0.417 | – | – |
| Lived with maid | 1.17 (0.59–2.29) | 0.656 | – | – |
| Lived alone | 0.88 (0.08–9.93) | 0.917 | – | – |
| Observed CR dementia stage (reference: late) | ||||
| Early | 0.67 (0.21–2.16) | 0.499 | – | – |
| Moderate | 0.73 (0.30–1.79) | 0.487 | – | – |
Abbreviations: CG, Participant; CR, Care recipient; OR, Odds ratio; CI, Confidence level; n.s., not significant in multivariate regression.
Variables with p < 0.1 in univariate regression were included in the multivariate regression (logistic regression – forward likelihood ratio): care recipient age; care recipient going out frequency, observed care recipient deterioration of cognitive functioning, mobility, emotion, communication, and taking transportation.
*p < 0.05.
3. RESULTS
In total, N = 275 caregivers were invited, among them n = 116 refused to participate in this study, n = 7 dropped out during interview, n = 152 participants successfully completed the survey and were included in the analysis. Among the successful interview, 65% was conducted through phone interview and 35% self‐completion by the participants (Figure 1). The average time lapse between the date of service suspension and the caregiver survey was 104 ± 11.4 days.
FIGURE 1.
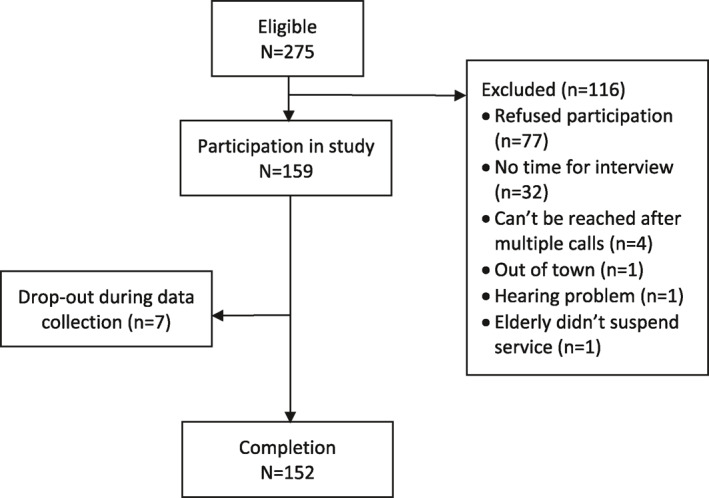
Study flowchart
3.1. Participant characteristics
The participants were mainly female (83%), average age being 58 ± 11.1 years. The care recipients were mainly female (65%), average age being 82 ± 9.3 years, and more in middle stage of dementia (45%). The majority of the participants were children or children‐in‐laws (70%) and spouse (26%) of the care recipients. Seventy percent of the participants lived with PwD during outbreak. Sixty six percent of the participants spent more time with PwD during daycare service cessation, while 84% care recipients went out less during daycare service cessation (Table 3).
TABLE 3.
Participant and care recipient characteristics
| N (%)/Mean (SD) | |
|---|---|
| Participant (caregivers) | |
| Gender | |
| Male | 26 (17.1) |
| Female | 126 (82.9) |
| Age | 57.6 (11.1) |
| Work from home arrangement during cessation of daycare service | |
| All working days | 9 (5.9) |
| Over half of working days | 11 (7.2) |
| Less than half of working days | 10 (6.6) |
| No such arrangement | 40 (26.3) |
| Not applicable since not working | 82 (53.9) |
| Time spent with care recipient during service cessation | |
| More | 101 (66.4) |
| Same | 35 (23.0) |
| Less | 16 (10.5) |
| Relationship with care recipient | |
| Spouse | 40 (26.3) |
| Children/children‐in‐law | 106 (69.7) |
| Grandchildren | 1 (0.7) |
| Siblings | 1 (0.7) |
| Relatives | 3 (2.0) |
| Friend | 1 (0.7) |
| Living with care recipient during service cessation (response of “yes”) | 106 (69.7) |
| Care recipient (people with dementia) | |
| Gender | |
| Male | 53 (34.9) |
| Female | 99 (65.1) |
| Age | 82.0 (9.3) |
| Informant stage of dementia | |
| Early | 21 (13.8) |
| Moderate | 68 (44.7) |
| Late | 28 (18.4) |
| Not sure | 35 (23.0) |
| Frequency care recipient went out during service cessation | |
| More | 6 (3.9) |
| Same | 18 (11.8) |
| Less | 128 (84.2) |
| Living condition during service cessation a | |
| Alone (response of “yes”) | 3 (2.0) |
| Spouse (response of “yes”) | 64 (42.1) |
| Children/children‐in‐law (response of “yes”) | 100 (65.8) |
| Grandchildren (response of “yes”) | 25 (16.4) |
| Siblings (response of “yes”) | 1 (0.7) |
| Relatives (response of “yes”) | 3 (2.0) |
| Domestic helpers (response of “yes”) | 60 (39.5) |
| Length of daycare cessation for the service recipients at time of survey | 104 ± 11.4 days |
| Duration of daycare service usage at time of survey (n = 36) b | 3 ± 2.7 days |
| Frequency of daycare service attendance prior to daycare cessation (n = 36) b | 3 ± 0.9 days |
Multiple choices as care recipients may co‐reside with one or more types of persons.
Based on n = 36 whose relevant information were able to be retrieved from the admission records for this study.
3.2. Impact of daycare service cessation on family caregivers
Seventy six percent of the participants had greater caring stress compared with time before daycare service cessation. Over 70% participants said that they were afraid that they themselves would get infected and then infect the care recipients (73%) or the care recipients would get infected (72%). Over half of the participants said that they spent more time accompanying or taking care of the care recipients who stayed at home for longer time, they could not leave the care recipients alone and had less time to do their own things (55%), needed to adjust their mood (53%), and got more physically tired (50%) (Table 4).
TABLE 4.
Caregiving stress and challenges during daycare service cessation
| Caregiving stress during compared with time before service cessation | N (%) of “Yes” |
|---|---|
| Much greater | 48 (31.6) |
| A bit greater | 68 (44.7) |
| Same | 35 (23.0) |
| A bit less | 1 (0.7) |
| Caregiving difficulties | |
| Prompted responses – Wellbeing of participants | |
| Worried that I or other family members would get infected and then infect the care recipient | 111 (73.0) |
| Worried that care recipient would get infected | 110 (72.4) |
| Need to adjust my emotion because I need to accompany/contact care recipient | 81 (53.3) |
| More physically tired because I need to accompany care recipient | 76 (50.0) |
| My emotion is disturbed because care recipient's emotion is disturbed by the pandemic | 47 (30.9) |
| My emotion is disturbed by the pandemic and care recipient's emotion is then disturbed | 38 (25.0) |
| Argument with care recipient because he/she wants to go out but I don't want him/her to | 36 (23.7) |
| Argument with care recipient because he/she doesn't want to go out but I want him/her to maintain social life | 16 (10.5) |
| Prompted responses – Arrangement of daily life | |
| Less time for my own living because I need to accompany care recipient | 83 (54.6) |
| Need to accompany care recipient because I dare not leave him/her alone | 83 (54.6) |
| Less time for myself to take rest | 67 (44.1) |
| Can't sleep well because I need to take care of care recipient at night | 64 (42.1) |
| More difficult for care recipient to go out because of transport disruption due to the pandemic | 54 (35.5) |
| Less time to take care of other family members because I need to accompany care recipient | 27 (17.8) |
| Need to adjust my work because of caregiving | 22 (14.5) |
| More difficult to accompany care recipient because of transport disruption due to the pandemic | 13 (8.6) |
| Unprompted “others" responses – Wellbeing of participants | |
| Worried that care recipient's physical functioning will deteriorate because of lack of daycare service | 6 (3.9) |
| Argument with care recipient because he/she doesn't want to go physical exercise or training but I want him/her to | 5 (3.3) |
| Worried that care recipient's cognitive functioning will deteriorate because of lack of daycare service | 4 (2.6) |
| Unprompted “others” responses – Arrangement of daily life | |
| Difficult to arrange training similar to what offered by daycare service at home | 13 (8.6) |
| More difficult on daily live caregiving | 7 (4.6) |
| Care recipient can't comprehend infection control measures | 6 (3.9) |
| Lack community resources to help caregiving | 2 (1.3) |
| Don't know how to handle the challenging behaviors of care recipients | 2 (1.3) |
The results of the univariate and multivariate ordinal regression analysis on associated factors of caregiving stress were presented in Table 1. The results of the multivariate ordinal regression showed that the odds of increased caregiving stress were significantly greater for older participants (OR = 1.04, 95% CI: 1.00–1.07, p = 0.036), for participants who observed greater emotional (OR = 5.61, 95% CI: 2.48–12.67, p < 0.001) and communication problems (OR = 2.33, 95% CI: 1.01–5.41, p = 0.048) of PwD during the COVID‐19 the pandemic, and for participants having spent more time with PwD during the COVID‐19 the pandemic (OR = 4.02, 95% CI: 1.67–9.66, p = 0.002), while the odds were significantly lower if the care recipients lived with their children or children‐in‐law during the pandemic (OR = 0.24, 95% CI: 0.10−0.54, p = 0.001).
3.3. Preference of daycare service during the pandemic
Thirty six percent of the participants (n = 55) preferred daycare service remaining available during the pandemic, because they were worried that the mobility (84%), cognition (76%), and mood (66%) of the care recipients would deteriorate without daycare service. They also emphasized that daycare service was a main source of respite for them (76%). On the other hand, participants who preferred cessation of daycare service mainly feared that PwD might get infected in daycare centres (88%) or when going outdoors (71%) (Table 5).
TABLE 5.
Reasons of preference of daycare service maintenance/cessation during the COVID‐19 pandemic
| N (%) of “Yes” | |
|---|---|
| Reasons of preference to daycare service remaining available | |
| Prompted responses | |
| Care recipient's mobility will deteriorate without daycare service | 46 (83.6) |
| Care recipient's cognitive functioning will deteriorate without daycare service | 42 (76.4) |
| Daycare service serves a respite for me | 42 (76.4) |
| Care recipient's emotion will deteriorate without daycare service | 36 (65.5) |
| Unpromoted “others” responses | |
| Daycare service spares me time to do my own things | 9 (16.4) |
| Care recipient is difficult to maintain daily routine without daycare services | 5 (9.1) |
| Care recipient is difficult to maintain social life without daycare services | 4 (7.3) |
| Daycare service can alleviate caregiving stress | 3 (5.5) |
| Difficult to take care of care recipient by my own | 1 (1.8) |
| Daycare centre is safer than home because it already has good infection control | 1 (1.8) |
| Reasons of preference to daycare service cessation | |
| Prompted responses | |
| Care recipient may get infected in daycare centre | 85 (87.6) |
| Care recipient may get infected when going out | 69 (71.1) |
| Unprompted “others” responses | |
| Staff may get infected in daycare centre | 5 (5.2) |
| Centre does not have enough manpower to provide good care during the pandemic | 1 (1.0) |
| Infection control measures increase staff burden | 1 (1.0) |
Note: Percentages were based on n = 55 having preferred daycare service to maintain and n = 97 having preferred cessation of daycare service.
The results of the univariate and multivariate logistic regression analysis on associated factors of daycare service preference were presented in Table 2. The results of the multivariate logistic regression showed that the odds of preferring daycare service to remain available during the pandemic were significantly greater if the care recipients went outdoors more frequently during the pandemic (OR = 12.28, 95% CI: 1.28–117.92, p = 0.030) and if the participants observed deterioration in cognitive function of PwD (OR = 3.53, 95% CI: 1.48–8.45, p = 0.005).
3.4. Impact of daycare service cessation on people with dementia
Seventy percent of the participants observed that PwD deteriorated in mobility and cognitive function during daycare service cessation, while 55% participants observed that PwD had greater problem with mood (Figure 2); this was in accord with the observed findings in two participating centres (Study 2), in which the paired sample t‐test analysis showed a significant decline in cognitive function (Montreal Cognitive Assessment, t(34) = 2.405, p = 0.022) and mobility (Elderly Mobility Scale, t(44) = 2.341, p = 0.024) after daycare service cessation (Supplementary Table 1). Among PwD in this study being reported to have home accidents and fall during daycare service cessation, 50% and 48% respectively did not have such incidents when they had usual daycare service.
FIGURE 2.
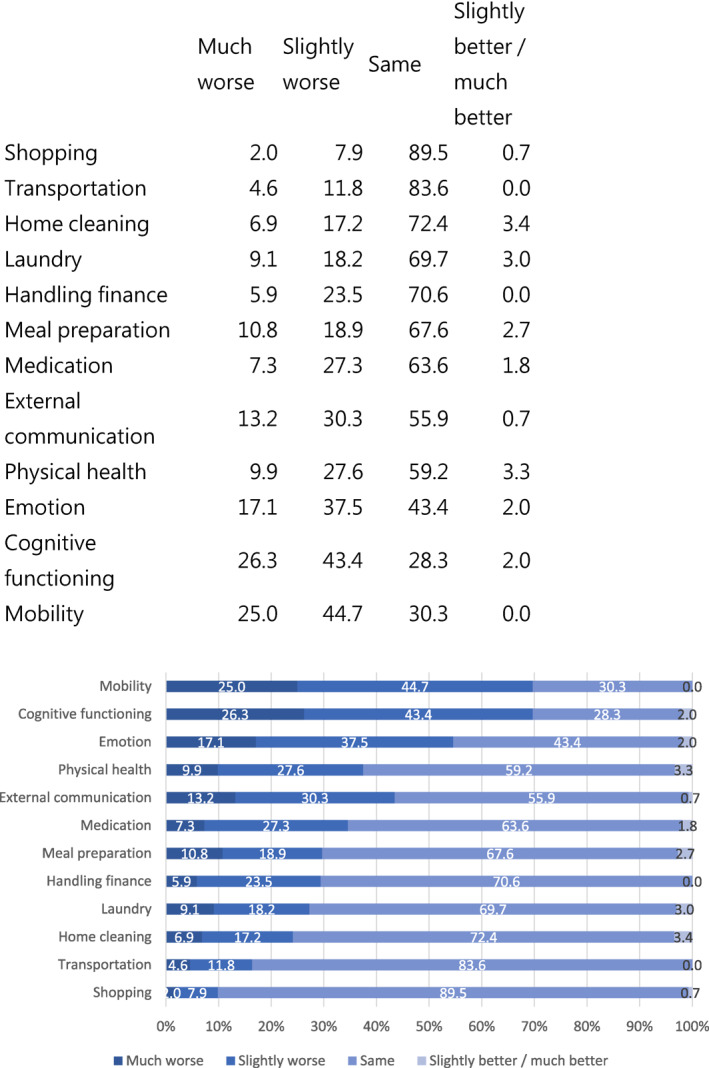
Change of functioning of people with dementia during daycare service cessation
4. DISCUSSION
This study provided important information about how cessation of daycare service, as a social distancing measure, affected PwD and their caregivers. Our findings showed that the majority of caregivers of PwD encountered a greater caregiving stress when daycare service was not available, they became alert to the care recipients and had sleep problem, these findings were consistent with a survey conducted to US caregivers of PwD. 11 Our caregiver participants had less time for their own lives due to the increased time accompanying the care recipients; this would not only increase caregiving stress but also adversely affect the caregiver's health, 12 and such maladaptive caregiving pattern would further worsen when care recipients stay home longer without daycare service.
In this study, we found that older caregivers were more vulnerable to caregiving stress during the pandemic. Our study findings showed that in general, the greatest caregiving challenge of family caregivers of PwD was infection control. Infection control was deemed particularly difficult among older caregivers because they were less able in securing infection control necessities such as queuing for purchasing masks or hand sanitizers. In addition, age was also a risk factor of infection and mortality due to COVID‐19 which made them more stressed about any potential risk of infection themselves. 13 , 14 On the other hand, caregiving stress was less when the care recipients lived with their children or children‐in‐law. We speculated that caregiving stress might be relieved when the children caregivers could keep a closer watch on PwD when they lived together.
The COVID‐19 pandemic caused tremendous change of lives of people in the world; city‐wide lockdowns, restricted outdoor activities, cessation of care facilities and cessation of non‐emergency medical services, to name a few, caused adverse effect to the physical and mental health of PwD by disrupting their daily routine. This study revealed that PwD went out less during the COVID‐19 pandemic, stayed longer time at home (presumably without proper physical exercise) and lacked social engagement, resulting in deterioration in cognitive, mobility, and communication function. In addition, PwD might not be able to comprehend the rationale for restricted outdoor activities. Such disruption of daily routine and activities might make them more emotionally disturbed, thereby increasing caregiver stress, especially that the caregivers needed to spend more time with PwD after the cessation of daycare service.
Moreover, out of anxiety or emotional uneasiness, some PwD might want to go out despite the objection from the family caregivers who were understandably worried about the infection risk. This might explain our study findings that when PwD tended to go out, the caregivers tended to prefer continuation of daycare service. Daycare centres were felt to be a safer place for PwD to be as stringent infection control measures under professional monitoring could be more assured there.
The challenges encountered by the caregivers differed in different waves of COVID‐19 outbreak. The challenges during the first wave were mainly related to the tangible needs; at the beginning of the COVID‐19 outbreak, mask and hand sanitizers were in short supply globally, people needed to queue for long time and pay a lot more for purchasing protective materials. As time went by, when materialistic supply became more stable, the caregivers' stress became more related to the lack of support services during the COVID‐19 pandemic because of strict social distancing policies. When the pandemic went on without foreseeable end, the caregivers felt stressed about the increase in behavioral problems of PwD and the challenges of imposing infection control measures on PwD. There have been guidelines developed on how to take care of PwD during COVID‐19 pandemic. 15 , 16 Unfortunately there were no such guidelines were publicized in Hong Kong. The limitation of knowledge and the lack of confidence in executing infection control most probably had contributed to greater caregivers' stress observed in this study.
Public education and professional advice is therefore essential to relieve some of the caregiving stress. Local guideline that is situation‐ and cultural‐specific 17 should be developed to advise family caregivers on the management of distressed behavior of PwD during the pandemic. 18 Concrete skills in dementia care with empowerment and training materials for meaningful engagement are available. 19 , 20 , 21 , 22 In addition, case managers at the daycare centres should provide continual support to family caregivers during the pandemic. 23 , 24 , 25 , 26 According to the Jockey Club Centre for Positive Ageing (JCCPA), one of the participating centres of this study, weekly telephone calls or video phone calls by case managers to the caregivers provided emotional support and helped reduce dementia caregiving stress by providing timely advice on behavior management at home.
Cluster infection in elderly service setting (daycare centres, residential facilities, etc.) has been observed throughout the COVID‐19 pandemic. While daycare activities may pose additional infection risk, we should balance this with the tangible needs for daycare in some PwD and their caregivers. Our study revealed that there was a significant minority of caregivers looking for daycare service despite the fear of COVID‐19 infection. To them, daycare service was vital to maintain the functional capabilities of the care recipients as well as an important channel for them to take respite. The risk of infection in daycare setting could be largely contained by infection control measures such as mask wearing, hand hygiene, restriction in group sizes, and avoidance of activities that would spread droplets such as singing. 27
Our study showed that many caregivers refrained the care recipients from going to daycare centres out of fear of infection, in spite of greater caregiving stress and observed deterioration of the care recipients. For them, alternative intervention such as online group or individual cognitive stimulation intervention should be developed. 28 JCCPA has conducted a pilot to turn face‐to‐face cognitive intervention online for people with mild cognitive impairment and people in the early stage of dementia, the pilot result showed that the attendance rate was over 90%, indicating a positive acceptance of online mode of intervention among people with cognitive impairment. Without a foreseeable end to this pandemic, there is a need to regularize online interventions for PwD. This will involve more funding from government or charities for both hardware (equipment, Internet connection) and software (development of evidence‐based intervention protocol, staff training). In addition, we should also be aware of the need of some caregivers in technical support, because of limited computer and internet literacy.
This study is subject to the following limitations. Firstly, the study was done by convenience sampling, most of our participants were not working people, so the results might not be generalized to the whole population of family caregivers of PwD such as the caregivers who were working, especially those having to work outside their homes during the pandemic. Secondly, we used telephone interview and online self‐completion as the data collection method to reduce the risk of infection. The change of functional status of PwD were therefore mostly based on observation of the caregivers, though we supplemented our research findings with the data collected in two participating centres (Study 2).
5. CONCLUSION
COVID‐19 has had great and adverse impact on dementia care worldwide. The restricted daily life and activities imposed by social distancing policies, and the threat of high mortality with COVID‐19 infection in older people has led to great stress to PwD and their caregivers. Family caregiver stress was compounded by much restricted social services during the pandemic. Daycare service cessation, in particular, has led to functional decline and mood problems in PwD and greater caregiver stress. Daycare service with appropriate infection control measures should therefore remain open to those PwD and family caregivers who needed it, and case managers should continue to support family caregivers who opt for the PwD to stay at home. Local guidelines for dementia care under COVID‐19 should be developed and publicized to guide caregivers in managing infection control measures and challenging behavior of PwD. There is also a need to develop online interventions as alternative means to deliver social stimulation for PwD and caregiver support.
CONFLICT OF INTEREST
The authors declare no conflict of interest for this study.
AUTHOR CONTRIBUTION
Bel Wong, Timothy Kwok, and Florence Ho conceived the study. Timothy Kwok, Florence Ho, and Jean Woo reviewed and approved the final version of questionnaire. Bel Wong and Tobi Cheng worked on the organization and statistical analysis of the study. All authors contributed to the interpretation of the results, the writing of this article, and approved the final version for submission.
Supporting information
Supplementary Table 1
ACKNOWLEDGEMENTS
The authors would like to thank the following organizations (in total 11 daycare centres among these organizations) for helping subject recruitment: Elderly Community Support & Care Services of Yan Chai Hospital Social Services Department, Jockey Club Centre for Positive Ageing, Jockey Club CADENZA Hub, The Evangelical Lutheran Church of HK, and The Neighbourhood Advice‐Action Council. The authors would also like to thank all the participants for their trust and contribution in this study.
Wong BP‐s, Kwok TC‐y, Chui KC‐m, Cheng TS‐t, Ho FK‐y, Woo J. The impact of dementia daycare service cessation due to COVID‐19 pandemic. Int J Geriatr Psychiatry. 2021;1‐11. doi: 10.1002/gps.5621
DATA AVAILABILITY STATEMENT
The datasets used in the study are available from the corresponding author on reasonable request. The data are not publicly available due to privacy or ethical restrictions.
REFERENCES
- 1. World Health Organization . Timeline: WHO's COVID‐19 Response; 2021. https://www.who.int/emergencies/diseases/novel‐coronavirus‐2019/interactive‐timeline [Google Scholar]
- 2. World Health Organization . Coronavirus Disease (COVID‐19) Pandemic; 2021. https://www.who.int/emergencies/diseases/novel‐coronavirus‐2019 [PubMed] [Google Scholar]
- 3. Tretteteig S, Vatne S, Rokstad AMM. The influence of day care centres for people with dementia on family caregivers: an integrative review of the literature. Aging Ment Health. 2016;20(5):450‐462. [DOI] [PubMed] [Google Scholar]
- 4. Zarit SH, Kim K, Femia EE, Almeida DM, Savla J, Molenaar PC. Effects of adult day care on daily stress of caregivers: a within‐person approach. J Gerontol Ser B: Psychol Sci Soc Sci. 2011;66(5):538‐546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Azarpazhooh MR, Amiri A, Morovatdar N, et al. Correlations between COVID‐19 and burden of dementia: an ecological study and review of literature. J Neurol Sci. 2020;416:117013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Matias‐Guiu JA, Pytel V, Matías‐Guiu J. Death rate due to COVID‐19 in Alzheimer’s disease and frontotemporal dementia. J Alzheimer's Dis. 2020(Preprint):1‐5. [DOI] [PubMed] [Google Scholar]
- 7. Zuin M, Guasti P, Roncon L, Cervellati C, Zuliani G. Dementia and the risk of death in elderly patients with COVID‐19 infection: systematic review and meta‐analysis. Int J Geriatr Psychiatry. 2020;36(5), 697‐703. [Google Scholar]
- 8. Canevelli M, Valletta M, Blasi MT, et al. Facing dementia during the COVID‐19 outbreak. J Am Geriatr Soc. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Cohen G, Russo MJ, Campos JA, Allegri RF. Living with dementia: increased level of caregiver stress in times of COVID‐19. Int Psychogeriatr. 2020;32(11):1377‐1381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Mok VC, Pendlebury S, Wong A, et al. Tackling challenges in care of Alzheimer's disease and other dementias amid the COVID‐19 pandemic, now and in the future. Alzheimer's Dementia. 2020;16(11):1571‐1581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. UsAgainstAlzheimer's. UsAgainstAlzheimer’s Survey #7 on COVID‐19 and Alzheimer’s Community Summary of Findings October 2020; 2020. [Google Scholar]
- 12. Hughes TB, Black BS, Albert M, et al. Correlates of objective and subjective measures of caregiver burden among dementia caregivers: influence of unmet patient and caregiver dementia‐related care needs. Int Psychogeriatr. 2014;26(11):1875‐1883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Nikolich‐Zugich J, Knox KS, Rios CT, Natt B, Bhattacharya D, Fain MJ. SARS‐CoV‐2 and COVID‐19 in older adults: what we may expect regarding pathogenesis, immune responses, and outcomes. GeroScience. 2020;42(2):505‐514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID‐19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323(13):1239‐1242. [DOI] [PubMed] [Google Scholar]
- 15. Taiwan Alzheimer’s Disease Association . The Reference Handbook of Dementia Care Responding to COVID‐19; 2020. https://drive.google.com/file/d/1_P3IJxzN9IhrDwXsLq_9NzjPEWzBjj7g/view [Google Scholar]
- 16. Alzheimer's Association . Coronavirus (COVID‐19): Tips for Dementia Caregivers; 2021. https://www.alz.org/help‐support/caregiving/coronavirus‐(covid‐19)‐tips‐for‐dementia‐care [Google Scholar]
- 17. Borges‐Machado F, Barros D, Ribeiro Ó, Carvalho J. The effects of COVID‐19 home confinement in dementia care: physical and cognitive decline, severe neuropsychiatric symptoms and increased caregiving burden. Am J Alzheimer's Dis Other Dementias. 2020;35:1533317520976720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Alzheimer’s Disease International . Advice and Support during COVID‐19: General Advice and Resources from Alzheimer Associations; 2020. https://www.alzint.org/resource/advice‐and‐support‐during‐covid‐19‐general‐advice‐and‐resources‐from‐alzheimer‐associations/ [Google Scholar]
- 19. Keng A, Brown EE, Rostas A, et al. Effectively caring for individuals with behavioral and psychological symptoms of dementia during the COVID‐19 pandemic. Front Psychiatry. 2020;11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Alzheimer’s Society . Coronavirus Support for People Affected by Dementia; 2020. https://www.alzheimers.org.uk/get‐support/coronavirus [Google Scholar]
- 21. Dementia UK. Giving the Covid‐19 Vaccine to Someone Living with Dementia; 2020. https://www.dementiauk.org/giving‐covid‐19‐vaccine‐to‐someone‐with‐dementia/ [Google Scholar]
- 22. Soares WB, Silvestre IT, Lima AMdO, de Almondes KM. The influence of telemedicine care on the management of behavioral and psychological symptoms in dementia (BPSD) risk factors induced or exacerbated during the COVID‐19 pandemic. Front Psychiatry. 2020;11:965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Aledeh M, Adam PH. Caring for dementia caregivers in times of the COVID‐19 crisis: a systematic review. Am J Nurs Res. 2020;8(5):552‐561. [Google Scholar]
- 24. Alzheimer’s Association . COVID‐19, Alzheimer’s and Dementia: What You Need to Know; 2020. https://www.alz.org/alzheimers‐dementia/coronavirus‐covid‐19 [Google Scholar]
- 25. Alzheimer’s Scotland . Coronavirus Updates; 2020. https://www.alzscot.org/coronavirus‐updates [Google Scholar]
- 26. Dementia Australia . A Coronavirus (COVID‐19) Update from Dementia Australia; 2020. https://www.dementia.org.au/an‐update‐from‐dementia‐australia [Google Scholar]
- 27. Korea Disease Control And Prevention Agency . The Updates on COVID‐19 in Korea as of 17 June; 2020. http://www.kdca.go.kr/board/board.es?mid=&bid=0030&act=view&list_no=367536&tag=&nPage=5 [Google Scholar]
- 28. Dai R, Spector A, Wong G. e‐Mental health care for people living with dementia: a lesson on digital equality from COVID‐19. Alzheimer's Dementia Diagn Assess Dis Monit. 2020;12(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Table 1
Data Availability Statement
The datasets used in the study are available from the corresponding author on reasonable request. The data are not publicly available due to privacy or ethical restrictions.