

Abstract
The Taussig‐Bing anomaly is a rare cyanotic congenital heart defect treated surgically in the early infancy. The preferred repair procedure is an arterial switch operation combined with ventricular septal defect closure. Despite promising long‐term functional outcomes and survival benefits, neo‐aortic dysfunction and arrhythmias might be relevant complications.
Keywords: arrhythmia, congenital disease, neo‐aortic regurgitation, sudden cardiac arrest, Taussing‐Bing anomaly
The Taussig‐Bing anomaly is a rare cyanotic congenital heart defect treated surgically in the early infancy. Despite promising long‐term functional outcomes and survival benefits, neo‐aortic dysfunction and arrhythmias might be relevant complications needing intervention. The most important to prevent serious complications are regular routine follow‐ups.

1. BACKGROUND
The Taussig‐Bing anomaly (TBA) is a rare cyanotic congenital heart defect and is the third most common variant of double outlet right ventricle (DORV). 1 , 2 The anomaly was first described in 1949 by collaborators Helen B. Taussig and Richard J. Bing. 1 It is characterized by the presence of non‐restrictive subpulmonic ventricular septal defect (VSD) and side‐by‐side great vessels that arise entirely from the right ventricle (DORV, double outlet right ventricle). Unlike transposition of the great arteries (TGA) with VSD, this anomaly is characterized by the presence of a bilateral conus and the absence of pulmonary‐mitral fibrous continuity. 3 , 4 Left‐to‐right shunting across the VSD causes increase pulmonary blood flow, early onset of pulmonary vascular disease, pulmonary hypertension, and heart failure. 3 , 4 The repair in the early infancy period is recommended. 5 Currently, the preferred repair procedure of the Taussig‐Bing defect is an arterial switch operation (ASO; an anatomic correction) combined with VSD closure. 6 The arterial switch operation by Jatene 7 involves surgically switching the vessels and switching the coronary arteries to put them on the pulmonary artery instead of the aorta where they were previously located. LeCompte et al. introduced a new surgical technique that includes extensive resection of the outlet septum and direct reimplantation of the pulmonary trunk on the superior margin of the right ventricular infundibulotomy. This procedure restores the correct continuity between the right ventricle and the pulmonary artery, without use of an extracardiac tube. 8 Despite promising long‐term functional outcomes and survival benefits after correction procedures, neo‐aortic regurgitation (AR) and neo‐aortic root dilatation might be relevant complications. 9 , 10 Therefore, the lifelong monitoring of patients with corrected Taussig‐Bing heart is necessary. We describe the patient with Taussig‐Bing anomaly who underwent the correction procedures in early childhood.
2. CASE PRESENTATION
The 18‐year‐old male patient with Taussig‐Bing anomaly after pulmonary artery binding and closure of patent ductus arteriosus when 1 year old and after the Jatene's switch procedure with modified LeCompte procedure at the age of 2 years was admitted to our Department in November 2018. He has been transferred from ICU 3 weeks after an episode of sudden cardiac arrest in the mechanism of ventricular fibrillation.
In physical examination, the patient was awake, the heart rate (HR) was 68 bpm with blood pressure (BP) 120/80 mmHg and while breathing room air his oxygen saturation was 98% with no visible or palpable lower limb edema. During auscultation, the normal vesicular sound was heard as well as loud a systolic‐diastolic murmur over the heart. The patient before admission was treated in Anesthesiology and Intensive Care Unit with metoprolol 150 mg/day, nadroparinum 0.6 ml/day, carbamazepinum 600 mg/day, trimetiazidinum 70 mg/day, and lorazepamum 1 mg/day. Laboratory analysis revealed features of normocytic anemia (hemoglobin—HGB 11.5 g/dl; hematocrit—HCT 32.6%; and mean corpuscular volume—MCV 84.5 fl), increased plasma level of lactate dehydrogenase (LDH)—375 U/L, alanine aminotransferase (ALT)—71 U/L, and aspartate aminotransferase (AST)—76 U/L, of N‐terminal probrain natriuretic peptide (NT‐proBNP)—278 pg/ml and of d‐dimer—2144 ng/ml. Troponine T, C‐reactive protein, creatinine, serum electrolytes, glucose, and urea were within normal range.
An electrocardiogram showed sinus rhythm, left axis deviation, left anterior fascicular block, right bundle branch block, and signs of left ventricular hypertrophy (Figure 1).
FIGURE 1.
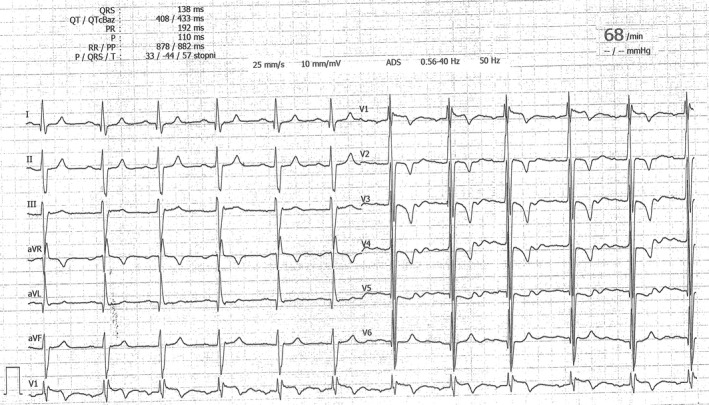
An electrocardiogram. Sinus rhythm, left axis deviation, left anterior fascicular block, right bundle branch block and signs of left ventricular hypertrophy
Echocardiographic examination using an Vivid E95 system (GE Healthcare) with a 1.4–5.2 MHz matrix transducer and tissue Doppler imaging (TDI) software revealed preserved systolic function of both ventricles left ventricle ejection fraction, LVEF > 60%; tricuspid annular plane systolic excursion, TAPSE 25 mm; right ventricular peak systolic velocity in TDI, RV S' 13 cm/s) without contractility disturbances.
The enlarged and hypertrophic left ventricle consists of the primary cavity connecting by VSD (size 39 mm) with a fragment of the right ventricle separated from the rest of the right ventricle by the Gore‐Tex patch acting as a ventricular septum—without any leakage features (Figure 2A). We noticed also an enlarged left atrium (Left Atrial Volume Index, LAVI 87 ml/m2) and severe mitral valve regurgitation (Effective Regurgitant Orifice, ERO 70; type I according Carpentier), connected with straddling. The patch attached to the trabecula of the right ventricle (Figure 2B,C). We also observed increased diameter of neo‐aortic bulb (50 mm) and severe neo‐aortic regurgitation (AV max: 1.85 m/s; ERO: 70; vena contracta, VC 8mm; and pressure half‐time, PHT 327 ms; Figure 2D–F). In the past medical history of our patient, the last follow‐up was preformed 3 years later in Pediatrics Cardiology Department. At that time, neo‐aortic and mitral valve regurgitations were moderate.
FIGURE 2.
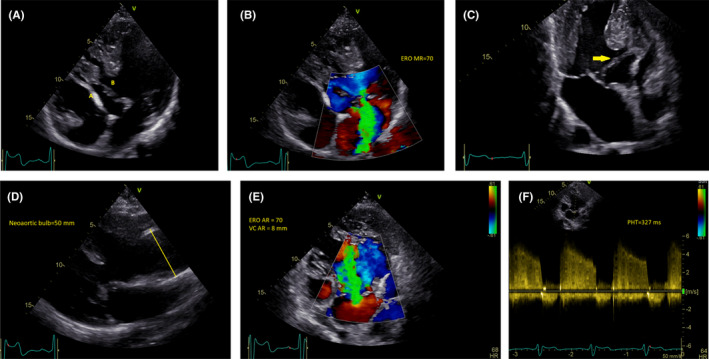
A, Apical 4‐chamber view. A. A patch with Gore‐Tex acting as a ventricular septum. B. Ventricular Septum Defect (VSD). B, Apical 4‐chamber view. Severe mitral valve regurgitation. Effective Regurgitant Orifice (ERO). C, Apical 4‐chamber view. Severe mitral valve regurgitation. Straddling a patch attached to trabecula the right ventricle. D, Parasternal long axis view. Dilatation of neo‐aortic bulb. E, Apical 4‐chamber view. Severe neo‐aortic valve regurgitation. Effective regurgitant orifice (ERO); vena contracta (VC). F, Apical 4‐chamber view. Severe neo‐aortic valve regurgitation. Pressure half‐time (PHT)
Two months later, the subcutaneous implantable cardioverter defibrillator (ICD) Boston Scientific Emblem with the subcutaneous defibrillation electrode was implanted.
In follow‐up after next 2 months, patient did not report any disturbing symptoms at rest and during normal activity. During cardiopulmonary exercise testing, he managed 12 min 29 s on a cycle ergometer, achieving a respiratory exchange ratio (RER) of 1.10 (Figure 3A). Peak oxygen consumption (peak VO2) was 27 ml/min/kg at a load 7.9 METs (62% predicted; Figure 3B) with an anaerobic threshold of 17 ml/min/kg (Figure 3C). The study was stopped because of fatigue, assessed expiratory exchange ratio, and the episode of nonsustained ventricular tachycardia (nsVT; Figure 3D).
FIGURE 3.

A, Respiratory exchange ratio (RER) against time. B, Peak oxygen consumption (VO2peak) against time. C, Cardiopulmonary exercise test results. D, Electrocardiogram during cardiopulmonary exercise testing. Nonsustained ventricular tachycardia (nsVT)
In Angio‐CT of coronary vessels performed during control hospitalization, there were no pathological changes. After the decision of the Heart Team, the patient was qualified for surgical treatment of valve defects: the Bentall procedure and mitral valve replacement. 11
3. DISCUSSION
Patients with corrected complex, congenital heart defects reach adulthood through advanced surgical and medical care. However, adult patients with corrected Taussig‐Bing anomaly are out of any guidelines and need an individual approach. 12 , 13 Despite TBA after ASO 10 , 14 , 15 and LeCompte procedure 16 , 17 have very good late survival with acceptable functional ability, during further follow‐up late complications are observed. One of the most common complications are connected with the neo‐aortic dysfunction. 13 , 18 , 19 The neo‐aortic dysfunction includes neo‐aortic root dilatation and neo‐aortic valve regurgitation and may require reoperation with neo‐aortic root replacement. 13 , 18 , 19 Risk factors that are related to the development of neo‐aortic dysfunction after ASO in TBA are older age at the time of ASO (1 year or older), presence of VSD, and previous pulmonary artery band (PAB). 18 , 19
Life‐threatening arrhythmias like ventricular tachycardia and ventricular fibrillation occur more often after physiology Mustard and Senning correction than anatomic correction. 20 However, the presented patient underwent cardiac arrest in the mechanism of ventricular fibrillation. Looking for other risk factors of ventricular arrhythmia in complex congenital heart disease is necessary. Coronary artery dysfunction, ventricular hypertrophy and dysfunction, the electrical activity of the patch area may be potential risk factors. 21
The lifelong, repeatable diagnostics should be provided only in specialistic GUCH centers. The carefully scheduled monitoring of patients with corrected Taussig‐Bing heart may reveal risk factors of life‐threatening complications and allow planned optimal prevention (like ICDs implantation). 20 , 22 , 23 The routine follow‐ups in our stable adult patients with congenital heart diseases are performed every 6 months in ambulatory clinic and once a year as a hospital stay.
4. SUMMARY AND CONCLUSIONS
Corrective procedures of the Taussig‐Bing anomaly in the early infancy period are essential to prevent heart failure development and for survival benefits. The late complications such as neo‐aortic root dilatation or neo‐aortic valve dysfunction and arrhythmias require attentive observation.
The monitoring during proper follow‐ups schedule is obligatory. Correctly performed echocardiographic study may reveal vessel roots dilatations or valves and chambers dysfunctions, which allow planning potential surgical intervention.
CONFLICT OF INTEREST
None declared.
AUTHOR CONTRIBUTIONS
ABD prepared a first draft of manuscript and take part in management of the patient. AB performed an analysis of literature in this field and improved a draft. MR performed first echocardiographic assessment. FP and JL involved in taking medical care about patient. MB and MM supervised patient care. All authors revised and accepted a manuscript.
ETHICAL APPROVAL
The study is in compliance with the Declaration of Helsinki.
CONSENT
The authors have confirmed during submission that patient consent has been signed and collected in accordance with the journal's patient consent policy.
ACKNOWLEDGEMENT
None.
Bielecka‐Dabrowa A, Bikiewicz A, Rybak M, et al. Patient after correction Taussig‐Bing anomaly with severe neo‐aortic regurgitation after sudden cardiac arrest. Clin Case Rep. 2021;9:e05085. 10.1002/ccr3.5085
Funding information
The study was financed from the statutory funds of the Polish Mother's Memorial Hospital Research Institute in Łódź.
DATA AVAILABILITY STATEMENT
Individual participant data that was presented in this article after deidentification will be available for researchers who provide a methodologically sound proposal. Proposals may be submitted after 9 months and up to 36 months following article publication.
REFERENCES
- 1. Taussig HB, Bing RJ. Complete transposition of the aorta and a levoposition of the pulmonary artery; clinical, physiological, and pathological findings. Am Heart J. 1949;37(4):551‐559. [DOI] [PubMed] [Google Scholar]
- 2. Walters HL III, Mavroudis C, Tchervenkov CI, Jacobs JP, Lacour‐Gayet F, Jacobs ML. Congenital heart surgery nomenclature and database project: double outlet right ventricle. Ann Thorac Surg. 2000;69:S249‐S263. [DOI] [PubMed] [Google Scholar]
- 3. Konstantinov IE. Taussig‐Bing anomaly: from original description to the current era. Tex Heart Inst J. 2009;36:580‐585. [PMC free article] [PubMed] [Google Scholar]
- 4. Van Praagh R. What is the Taussig‐Bing malformation? Circ. 1968;38(3):445‐449. [DOI] [PubMed] [Google Scholar]
- 5. Brawn WJ, Mee RBB. Early results for anatomic correction of transposition of the great arteries and for double outlet right ventricle with subpulmonary ventricular septal defect. J Thorac Cardiovasc Surg. 1988;95:230‐238. [PubMed] [Google Scholar]
- 6. Griselli M, McGuirk SP, Ko C‐S, Clarke AJB, Barron JD, Brawn WJ. Arterial switch operation in patients with Taussig‐Bing anomaly — influence of staged repair and coronary anatomy on outcome. Eur J Cardiothorac Surg. 2007;31(2):229‐235. [DOI] [PubMed] [Google Scholar]
- 7. Jatene AD, Fontes VF, Paulista PP, et al. Anatomic correction of transposition of the great vessels. J Thorac Cardiovasc Surg. 1976;72:364‐370. [PubMed] [Google Scholar]
- 8. Lecompte Y, Neveux JY, Leca F, et al. Reconstruction of the pulmonary outflow tract without prosthetic conduit. J Thorac Cardiovasc Surg. 1982;84(5):727‐733. [PubMed] [Google Scholar]
- 9. Soszyn N, Fricke TA, Wheaton GR, et al. Outcomes of the arterial switch operation in patients with Taussig‐Bing anomalny. Ann Thorac Surg. 2011;92:673‐679. [DOI] [PubMed] [Google Scholar]
- 10. Schwarz F, Blaschczok HC, Sinzobahamvya N. The Taussig‐Bing anomaly: long‐term results. Eur J Cardiothorac Surg. 2013;44(5):821‐827. [DOI] [PubMed] [Google Scholar]
- 11. Bielecka‐Dabrowa AM, Rybak M, Pawliczak F, Lewek J, Banach M, Maciejewski M. P253 Patient after correction of Taussig‐Bing anomaly with severe neoaortic regurgitation and after sudden cardiac arrest. Eur Heart J Cardiovasc Imaging. 2020;21:319.114. [Google Scholar]
- 12. Stout KK, Daniels CJ, Aboulhosn JA, et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease: executive summary: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. J Am Coll Cardiol. 2019;973(12):1494‐1563. [DOI] [PubMed] [Google Scholar]
- 13. Baumgartner H, De Backer J , Babu‐Narayan SV, et al. 2020 ESC guidelines for the management of adult congenital heart disease. The task force for the management of adult congenital heart disease of the European society of cardiology (ESC). Endorsed by: association for European paediatric and congenital cardiology (AEPC), international society for adult congenital heart disease (ISACHD). European Heart J. 2021;42(6):563‐645. [DOI] [PubMed] [Google Scholar]
- 14. Vergnat M, Baruteau AE, Houyel L, et al. Late outcomes after arterial switch operation for Taussig‐Bing anomaly. J Thorac Cardiovasc Surg. 2015;149:1124‐1130. [DOI] [PubMed] [Google Scholar]
- 15. Hayes DA, Jones S, Quaegebeur JM, et al. Primary arterial switch operation as a strategy for total correction of Taussig Bing anomaly: a 21‐year experience. Circ J. 2013;128:194‐198. [DOI] [PubMed] [Google Scholar]
- 16. Wetter J, Belli E, Sinzobahamvya N, Blaschzok HC, Brecher AM, Urban AE. Transposition of the great arteries associated with ventricular septal defect: surgical results and long‐term outcome. Eur J Cardiothorac Surg. 2001;20:816‐823. [DOI] [PubMed] [Google Scholar]
- 17. Masuda M, Kado H, Shiokawa Y, et al. Clinical results of arterial switch operation for double‐outlet right ventricle with subpulmonary VSD. Eur J Cardiothorac Surg. 1999;15(3):283‐288. [DOI] [PubMed] [Google Scholar]
- 18. Schwartz ML, Gauvreau K, del Nido P, Mayer JE, Colan SD. Long‐term predictors of aortic root dilation and aortic regurgitation after arterial switch operation. Circ. 2004;110:128‐132. [DOI] [PubMed] [Google Scholar]
- 19. McMahon C, Ravekes W, O’Brian SE, et al. Risk factors for neo‐aortic root enlargement and aortic regurgitation following arterial switch operation. Pediatr Cardiol. 2004;25:329‐335. [DOI] [PubMed] [Google Scholar]
- 20. Sodhi SS, Cedars AM. Primary prevention of sudden cardiac death in adults with transposition of the great arteries: a review of implantable cardioverter‐defibrillator placement. Tex Heart Inst J. 2015;42(4):309‐318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Gatlin S, Kalynych A, Sallee D, Campbell R. Detection of a coronary artery anomaly after a sudden cardiac arrest in a 17 Year‐old with D‐transposition of the great arteries status post arterial switch operation: a case report. Congenit Heart Dis. 2011;6(4):384‐388. [DOI] [PubMed] [Google Scholar]
- 22. Slater TA, Cupido B, Parry H, et al. Implantable cardioverter‐defibrillator therapy to reduce sudden cardiac death in adults with congenital heart disease: a registry study. J Cardiovasc Electrophysiol. 2020;31(8):2086‐2092. [DOI] [PubMed] [Google Scholar]
- 23. Moore BM, Cao J, Cordina RL, McGuire MA, Celermajer DS. Defibrillators in adult congenital heart disease: long‐term risk of appropriate shocks, inappropriate shocks, and complications. Pacing Clin Electrophysiol. 2020;43(7):746‐753. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Individual participant data that was presented in this article after deidentification will be available for researchers who provide a methodologically sound proposal. Proposals may be submitted after 9 months and up to 36 months following article publication.