

Abstract
In the 1930s United States, urban neighborhoods were graded on their desirability for investment (often based on race), a process known as “redlining.” This study examined how historical redlining relates to current disparities in an important health determinant: tobacco retailer density. Analyses were conducted for thirteen Ohio cities using negative binomial models that accounted for retailer spatial dependence and controlled for present-day sociodemographic characteristics. Findings indicated that as grades increased from “Best” to “Still Desirable” to “Definitely Declining” and “Hazardous,” retailer density increased monotonically. These results highlight the persisting impacts of redlining and how disparities, once intentionally created, can be perpetuated over time.
Introduction
The process of “redlining” began in the United States during the late 1930s when the Home Owners’ Loan Corporation (HOLC) was established and tasked with creating “residential security maps” to assist in the determination of which neighborhoods would receive mortgage loans.1 Examiners ultimately visited over 150 cities in the United States to determine their desirability.1 Neighborhoods within these cities were assigned gradings of “Best”, “Still Desirable”, “Definitely Declining” or “Hazardous” and outlined on maps in green, blue, yellow or red ink, respectively.1 The HOLC reported that the grading determinations were made based on the age and condition of housing, transportation access, and the economic class and employment status of residents as well as their ethnic and racial composition.1 While the grading determinations appear to be based on many measures, the HOLC kept records of the density of African American residents in each neighborhood and the majority of African American neighborhoods were described as “Hazardous.”2
The HOLC’s residential security maps were shared and adopted widely by the Federal Housing Administration and many private lenders, resulting in the institutionalization of mortgage loan segregation.2 These rankings systematically segregated African American, Hispanic, other minority, and low-income populations. In addition, the implementation of this policy and the resulting disinvestment and denial of services to low-income, high-minority neighborhoods exacerbated the discrimination that already existed in the United States.
The Association between Redlining and Current Health Inequalities
Growing recognition of the social determinants of health, including structural racism, has led to research on the associations between redlining and elements of the built environment and contemporary health outcomes. Such work demonstrates how neighborhoods that were historically redlined are often present-day “food deserts” with little accessibility to supermarkets; this leaves many residents reliant on less healthy alternatives, such as convenience stores, for their food supplies.3,4 Residents who live in redlined neighborhoods also have less access to other resources beneficial to health including pharmacies and areas conducive to physical activity.5,6 Conversely, redlined neighborhoods have been found to have a higher concentration of deleterious resources such as alcohol outlets.7 One study dubbed the positive association between redlining and liquor store concentration “liquorlining”.8 Differences in the levels of racial segregation,1 homeownership rates, home values, credit scores,9 foreclosures,10 and violence rates11 have additionally been found across redlining boundaries. Contemporary negative health outcomes found to be associated with redlining include higher rates of asthma,12 breast cancer, infant mortality, diabetes,13 and poorer cancer survival.14,15 These associations show the broad, persistent effects that redlining has had on elements of the built environment, resource accessibility, and overall health outcomes of neighborhoods.
The Potential for an Association between Redlining and Tobacco Retailer Density
Many studies have examined contemporary tobacco marketing, retailer density, and access to tobacco products as they compare to the contemporary racial composition of a neighborhood. Such studies have found that tobacco retailer density tends to be higher in areas characterized by high-minority and/or low-income populations.16-19 Even when controlling for income level and socioeconomic status, tobacco retailer density remains higher in predominantly African American areas than predominantly White areas.20 Some researchers have speculated that these current disparities in tobacco retailer density may have their roots in redlining.21 However, evidence of an association between redlining designations and contemporary tobacco retailer disparities is lacking.
Nevertheless, disparities in tobacco retailer density are a concern because of their association with disparities in tobacco use.22,23 For example, higher tobacco retailer density is associated with more exposure to point-of-sale tobacco marketing,16,24 higher youth smoking frequency,25 and lower rates of tobacco cessation among adults.26 Higher rates of tobacco use, in turn, relate to higher incidence of tobacco-related morbidity and mortality, such as cancers, cardiovascular diseases, and respiratory diseases.27 Importantly, there are meaningful disparities in many of these tobacco-related health outcomes. 28-30
Need for this Study
Although present-day disparities in neighborhood demographics and tobacco retailer density partially tell the story of redlining, current racial composition and income levels are not exact representations of the past redlining status of a neighborhood. Analyzing historical redlining status against contemporary tobacco retailer density better represents the lasting effects of the policy. By identifying such connections, we can better understand how disparities in tobacco retailer density have been perpetuated over time through the lasting consequences of disinvestment and neighborhood reputation. Therefore, this study aimed to examine how the four categories of historical redlining relate to current disparities in tobacco retailer density. To distinguish the impact of historical vs. contemporary sociodemographic distributions, analyses controlled for present-day sociodemographic characteristics (e.g., neighborhood poverty). Analyses were conducted for most of the densely populated areas of Ohio, which is a large and diverse state with fourteen cities that were redlined by the HOLC (thirteen of which were available for the present analyses, as described below).
Methods
Software
All calculations for the geospatial statistical analysis were calculated using the R software package, using the maptools, MASS, rgeos, sp and spam R libraries.31
Tobacco Retailers
At the time of data collection, Ohio’s tobacco licensing law required cigarette retailers to purchase a retail cigarette dealer’s license from their County Auditor’s office; a license for selling other types of tobacco products was not required. Names and addresses of all retailers with active cigarette licenses (gas stations, convenience stores, grocery stores, tobacco shops, etc.) were obtained from each of Ohio’s 88 county auditor offices in the fall of 2017. For other types of tobacco retailers that do not require a cigarette license—namely, hookah cafés and vape shops—we used the methods described by Kates et al.32 for searching internet directories (e.g., Yelp, Yellowpages.com). Details on our internet directory searches, as well as our process for cleaning and checking all tobacco retailer data for accuracy via groundtruthing, are provided elsewhere.18 Our final list indicated there were 11,392 tobacco retailers in the state of Ohio (11,065 cigarette licenses and 327 vape/hookah stores). In the thirteen Ohio cities analyzed in this paper, there were 5,548 tobacco retailers (5,379 cigarette licenses and 169 vape/hookah stores). As described in detail elsewhere18 these retailers were then geocoded based on their street address.
Contemporary Sociodemographic Measures
We obtained census tract-level information about race/ethnicity, poverty, age, and population size from the 2016 American Community Survey 5-year estimates. All cut-offs distinguishing “high” and “low” groups were selected a priori and are consistent with our previous work.18,33 Census tracts were coded as having a high prevalence of African Americans [Hispanics] if 15% or more of the population was African American [Hispanic]; all other tracts were coded as having a low prevalence of African Americans [Hispanics]. Tracts were coded as having a high prevalence of young people if 25% or more of the population was under age 18; all other tracts were coded as having a low prevalence of young people. Finally, tracts were coded as having a high prevalence of poverty if more than 15.4% of the population was below the poverty level (15.4% is the state average for Ohio); all other tracts were coded as having a low prevalence of poverty.
Defining Redlined Areas
Fourteen cities in Ohio were redlined from 1936-1940: Akron, Canton, Cincinnati, Cleveland, Columbus, Dayton, Hamilton, Lima, Lorain, Portsmouth, Springfield, Toledo, Warren, and Youngstown. Shapefiles of the original redlining maps for thirteen cities were obtained from University of Richmond’s Mapping Inequality Project.34 The shapefile for Cincinnati’s redlining map was not available and thus this city is not part of this analysis. TIGER shapefiles for the census tracts for the State of Ohio came from the U.S. Census Bureau.35
Merging Historical and Contemporary Maps
Census tract borders shift over time, or tracts can be added or removed entirely, in order to keep the population in each census tract relatively constant.36 Consequently, areas in the 1930s and 2016 maps did not match. To address this issue, we created smaller subregions of each 1930 HOLC graded area that overlapped with part of a single 2016 census tract. These subregions served as our geographic unit of analysis. Each subregion was assigned its respective HOLC grade: Green (A) indicated “Best,” blue (B) indicated “Still Desirable,” yellow (C) indicated “Definitely Declining,” and red (D) indicated “Hazardous.” There were also areas in each county that were not given HOLC grades in the 1930s; we denoted these subregions as type E. Figure 1 demonstrates an example of one of our final county maps (maps for other counties, and grayscale county maps, are available in the Supplement).
Figure 1:

Subregions with the HOLC grade for Cleveland in Cuyahoga County; A: “Best” (green), B: “Still Desirable” (blue), C: “Declining” (yellow), and D: “Hazardous” (red). Subregions not graded by HOLC in 1940 are denoted E (gray).
We next reapportioned, by area, the number of tobacco retailers and the total population in each 2016 census tract to the subregions that contained the tract. Thus, each subregion contained its own retailer count, population, and HOLC grade. All other sociodemographic factors were assigned to each subregion. There were 4383 subregions across the thirteen counties/cities. After removing subregions that contained five or fewer people (a process that eliminated three tobacco retailers and less than 0.15% of the total population from the study), 3,846 subregions remained for analyses.
Spatial Statistical Analysis
After accounting for possible changes by city/county by removing the average log retailer density for each area, we explored relationships between tobacco retailer density, sociodemographic factors, and HOLC grade using descriptive statistics and figures. We then used negative binomial regression models relating the retailer density to sociodemographic factors, while accounting for possible overdispersion in the retailer counts (overdispersion refers to extra-Poisson variability arising from possible clustering effects or unexplained covariates). As the distribution of retailer counts is spatially dependent across census tracts,18 we expected the counts to also be spatially dependent across subregions. To test this assumption, we used Moran’s I statistic (e.g., Waller and Gotway)37 to test for residual spatial dependence. Since a standard negative binomial model would assume independence among the retailer counts, we used a generalized estimating equation (GEE) approach to account for spatial dependence over subregions. Specifically, our spatial model assumes a conditional dependence between subregions that share a border. See the supplement of Adibe et al.18 for further details of the spatial modeling approach. In examining differences among the retailer density by HOLC grade, we adjust for multiple comparisons using the Tukey method to produce simultaneous confidence intervals (CIs).38
Progression of Statistical Models
After determining our spatial statistical approach, we used analysis of deviance and the Akaike information criterion (AIC) to assess the outcomes of three sets of models. In the first, we related tobacco retailer density to sociodemographic factors (subregions with a high and low prevalence of African Americans, Hispanics, Poverty, and a Population aged under 18). We investigated possible interactions between these factors and also included a fixed effect for each of the thirteen different cities/counties. In the second, we included an effect for city/county and the HOLC grade (A, B, C, D, or E). The third model then contained all effects: city/county and sociodemographic factors from the first model, and the HOLC grade from the second model.
Results
Descriptive and Exploratory Summaries
In the 3,846 subregions in the thirteen urban counties/cities, there were 5,548 present-day tobacco retailers across a total contemporary population of over 5.8 million – a density of 0.95 retailers per thousand people.
Table 1 summarizes the distributions of various sociodemographic factors and HOLC grades across the cities. The prevalence of African Americans, Hispanics, and Poverty varied greatly by city. The distribution of HOLC grades also varied greatly over all the subregions. Most subregions (38.4%) were not historically graded (E). Of those subregions that were graded, most were grade C: “Definitely Declining” (28.0% of subregions; 730.1 thousand people), followed by B: “Still Desirable” (15.6% of subregions; 414.0 thousand people), then D: “Hazardous” (11.7% of subregions; 217.2 thousand people), and finally A: “Best” (6.3% of subregions; 171.3 thousand people). Looking at the spatial distribution of the HOLC grades for each city (see Figure 1 for example for Cleveland/Cuyahoga County), as expected, we saw spatial clustering among the grades. In particular C: “Definitely Declining” and D: “Hazardous” tended to cluster together over all the thirteen cities. In larger cities such as Akron, Cleveland, Columbus, and Dayton, there was also clustering of the A: “Best” and B: “Still Desirable” grades.
Table 1:
Summary statistics of the tobacco retailers by sociodemographic factors and HOLC grade.
| City/County | N of Subregion |
High Prevalence of | HOLC Grade | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| African Amer. % |
Hispanic % |
Poverty % |
Age < 18 % |
A % |
B % |
C % |
D % |
E % |
||
| Akron/Summit | 405 | 38.3 | 0 | 51.1 | 25.7 | 9.4 | 16.5 | 31.4 | 11.4 | 31.4 |
| Canton/Stark | 155 | 27.7 | 0 | 56.1 | 40.0 | 3.2 | 17.4 | 13.5 | 10.3 | 55.5 |
| Cleveland/Cuyahoga | 1207 | 49.9 | 12.6 | 57.9 | 27.4 | 7.9 | 16.4 | 31.6 | 14.2 | 30.0 |
| Columbus/Franklin | 579 | 38.9 | 4.3 | 60.3 | 39.7 | 4.5 | 16.8 | 23.3 | 8.5 | 47.0 |
| Dayton/Montgomery | 328 | 35.7 | 5.5 | 67.7 | 38.4 | 7.0 | 14.3 | 20.7 | 12.5 | 45.4 |
| Hamilton/Butler | 123 | 7.3 | 8.9 | 51.2 | 50.4 | 1.6 | 8.9 | 17.1 | 7.3 | 65.0 |
| Lima/Allen | 103 | 43.7 | 0 | 67.0 | 51.5 | 3.9 | 17.5 | 35.0 | 12.6 | 31.1 |
| Lorain/Lorain | 116 | 7.8 | 50.9 | 59.5 | 44.0 | 0 | 6.0 | 20.7 | 10.3 | 62.9 |
| Portsmouth/Scioto | 63 | 0 | 0 | 85.7 | 12.7 | 4.8 | 11.1 | 33.3 | 19.0 | 31.7 |
| Springfield/Clark | 122 | 21.3 | 0.8 | 76.2 | 42.6 | 7.4 | 16.4 | 27.9 | 13.1 | 35.2 |
| Toledo/Lucas | 336 | 41.1 | 11.0 | 73.5 | 37.2 | 6.8 | 17.6 | 34.2 | 6.5 | 34.8 |
| Warren/Trumbull | 95 | 16.8 | 0 | 65.3 | 30.5 | 4.2 | 12.6 | 20.0 | 5.3 | 57.9 |
| Youngstown/Mahoning | 214 | 50.0 | 9.8 | 69.6 | 26.2 | 5.6 | 14.5 | 34.1 | 17.8 | 28.0 |
| Total | 3846 | 38.8 | 8.4 | 61.6 | 33.5 | 6.3 | 15.6 | 28.0 | 11.7 | 38.4 |
Data are for subregions that contain more than five people. Values in bold indicate cities/counties that have percentages that are exactly zero.
The HOLC grades are A: “Best”, B: “Still Desirable”, C: “Declining”, and D: “Hazardous”. Subregions not graded by the HOLC are denoted E.
Figure 2 displays summaries of the per capita log retailer density by subregion in the population (we added a value of 0.1 to retailer counts before taking logs to guard against taking a log of zero). Figure 2(a) demonstrates that there are city-by-city differences in retailer density, and that the retailer rate tends to be highest in Portsmouth/Scioto County. In Figure 2(b), we account for the average effect of city, and investigate the residual relationship with the sociodemographic factors and the HOLC grade. This indicates the retailer rate is higher for subregions with a higher prevalence of African Americans, Hispanics and Poverty, replicating the findings of Adibe et al.18 in these thirteen cities. In terms of the HOLC grade, the retailer density tends to increase as we move from A: “Best” subregions to D: “Hazardous,” indicating that before accounting for other factors in our model, there is evidence of an effect of redlining. The subregions that were not graded by the HOLC (Grade E) in the 1930s have a retailer density more similar to the subregions graded A and B.
Figure 2:
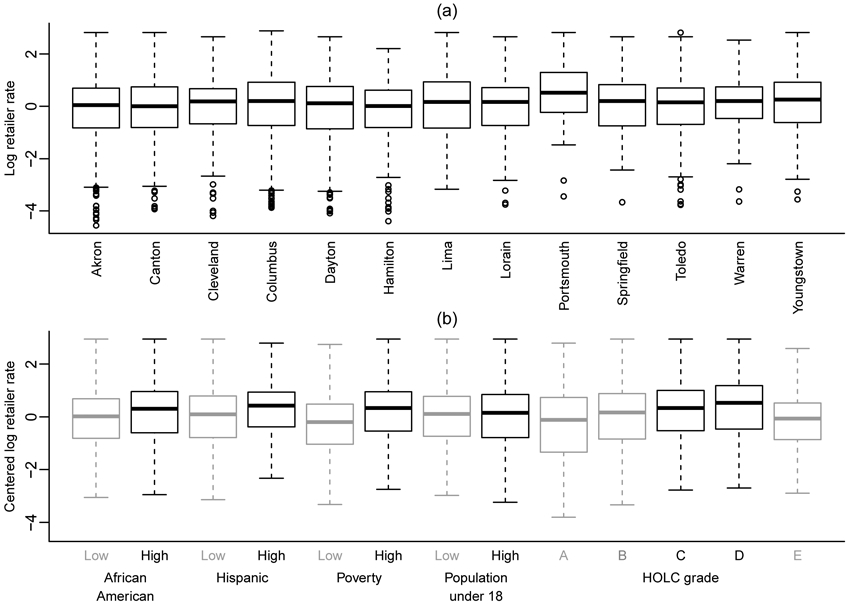
Boxplots of the observed log rate of tobacco retailers, per 1000 people, by city for various sociodemographic characteristics, both (a) by city (b) and by sociodemographic characteristics and HOLC grade, centering to remove the average effect for each city (b).
Model Comparisons and Results
Table 2 displays summaries of the three sets of negative binomial models examining associations between predictive factors and tobacco retailer counts. All three models had significant residual spatial dependence with p-values close to zero. Moran’s I statistic was 0.11, 0.13, and 0.09 respectively across the three models, indicating that, as expected, the negative binomial models that included more factors had less spatial dependence.
Table 2:
A summary of three statistical models (relative risk, RR and 95% pointwise CIs, lower and upper) that explain possible associations between tobacco retailer counts in each subregion using different sets of factors.
| Model 1 Sociodemographic |
Model 2: HOLC grade |
Model 3: Sociodemographic + HOLC grade |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| Factor | RR | Lower | Upper | RR | Lower | Upper | RR | Lower | Upper |
| Akron vs Columbus | 1.04 | 0.87 | 1.25 | 0.95 | 0.78 | 1.16 | 1.05 | 0.88 | 1.25 |
| Canton vs Columbus | 1.17 | 0.93 | 1.48 | 1.08 | 0.84 | 1.39 | 1.17 | 0.94 | 1.45 |
| Cleveland vs Columbus | 1.10 | 0.96 | 1.27 | 1.08 | 0.92 | 1.25 | 1.09 | 0.96 | 1.25 |
| Dayton vs Columbus | 1.08 | 0.89 | 1.30 | 1.08 | 0.88 | 1.33 | 1.08 | 0.90 | 1.29 |
| Hamilton vs Columbus | 1.17 | 0.91 | 1.50 | 1.08 | 0.82 | 1.41 | 1.15 | 0.91 | 1.46 |
| Lima vs Columbus | 1.29 | 0.92 | 1.81 | 1.18 | 0.82 | 1.70 | 1.27 | 0.93 | 1.75 |
| Lorain vs Columbus | 1.22 | 0.93 | 1.59 | 1.20 | 0.90 | 1.60 | 1.20 | 0.93 | 1.54 |
| Portsmouth vs Columbus | 1.18 | 0.76 | 1.83 | 1.33 | 0.83 | 2.11 | 1.16 | 0.77 | 1.75 |
| Springfield vs Columbus | 1.21 | 0.88 | 1.67 | 1.18 | 0.83 | 1.66 | 1.20 | 0.89 | 1.63 |
| Toledo vs Columbus | 1.10 | 0.91 | 1.32 | 1.14 | 0.93 | 1.39 | 1.11 | 0.93 | 1.32 |
| Warren vs Columbus | 1.41 | 1.07 | 1.86 | 1.45 | 1.07 | 1.96 | 1.40 | 1.08 | 1.82 |
| Youngstown vs Columbus | 1.04 | 0.81 | 1.34 | 1.00 | 0.76 | 1.32 | 1.02 | 0.81 | 1.30 |
| African American | 1.12 | 1.02 | 1.24 | 1.12 | 1.02 | 1.22 | |||
| Hispanic | 1.25 | 1.08 | 1.44 | 1.21 | 1.06 | 1.39 | |||
| Poverty | 1.65 | 1.50 | 1.80 | 1.60 | 1.47 | 1.75 | |||
| Aged Below 18 | 0.83 | 0.77 | 0.90 | 0.83 | 0.77 | 0.89 | |||
| HOLC grade B vs A | 1.68 | 1.31 | 2.15 | 1.37 | 1.07 | 1.75 | |||
| HOLC grade C vs A | 2.35 | 1.83 | 3.01 | 1.81 | 1.42 | 2.31 | |||
| HOLC grade D vs A | 2.79 | 2.11 | 3.68 | 1.98 | 1.52 | 2.60 | |||
| HOLC grade E vs A | 1.80 | 1.41 | 2.29 | 1.68 | 1.33 | 2.13 | |||
The CIs account for possible spatial dependence among the subregions. Values in bold indicate relative risks that are significantly different from one.
Model 1 includes terms for City, African American, Hispanic, Poverty and Age Below 18; Model 2 includes City and HOLC grade; and Model 3 includes City, African American, Hispanic, Poverty, Age Below 18, and HOLC grade.
We did consider versions of Model 1 that included higher order interactions between sociodemographic factors. While some models with interactions did have a smaller AIC compared to models that only contained main effects (the smallest AIC for all the models with interactions was 9121 versus 9168 for the main effects model), once we accounted for spatial dependence among the retailer counts, there were no practical differences among the associations between the retailer density and a combination of sociodemographic factors.
Although at times somewhat attenuated, all factors found to be significant in Models 1 and 2 were also significant in Model 3, the full model that tested the impact of all effects (city/county, sociodemographic factors, and the HOLC). Therefore, Model 3 findings will primarily be discussed.
Model 3 indicated that, after accounting for spatial dependence, only Warren had a significantly different tobacco retailer density from Columbus (the city that we chose to be the reference). In contrast, all associations between the retailer density and sociodemographic factors were statistically significant. Subregions with a high (vs. low) prevalence of African Americans had 1.12 times higher retailer density, and subregions with a high (vs. low) prevalence of Hispanics had 1.21 times higher retailer density. Similarly, subregions with high (vs. low) Poverty had 1.60 times higher retailer density. Subregions with a high (vs. low) prevalence of people aged over 18 have smaller retailer density (0.83 times).
Models examining the predictive impact of HOLC grade used A: “Best” as the reference group (as this hides many comparisons of interest in understanding the relationship between tobacco retailer density and HOLC grade, Figure 3 display all possible pairwise comparisons of relative risk). Model 3 indicated there was a statistically significant effect of redlining upon the tobacco density in these thirteen cities, even after accounting for differences among cities and present-day sociodemographic factors. As the HOLC grade increased from A: “Best” to C: “Definitely Declining,” the density of retailers increases monotonically. Subsequent analyses indicated there was no difference between the C: “Definitely Declining” and D: “Hazardous” subregions; further, there was no difference between the E (non-graded) subregions and grade C or D subregions.
Figure 3:
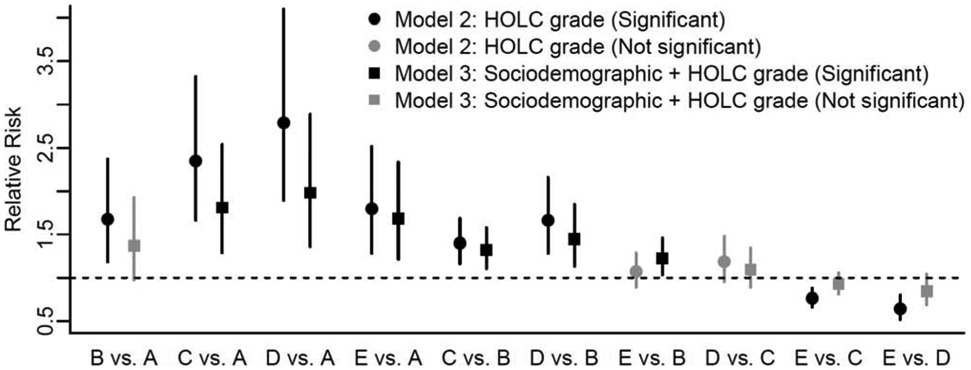
Relative risk comparisons of the density of tobacco retailers in each subregion, among all pairs of HOLC grades.
The circles denote the relative risks for a model that only contains a possible city effect and HOLC grade effect (Model 2) and the squares denote the relative risk for a model that also contains sociodemographic factors (Model 3). Note that Model 1 did not assess HOLC grades and cannot therefore be included.
Black font indicates statistically-significant differences between pairs; gray font indicates no difference. Unlike Table 2, significance tests adjust for multiple comparisons. The vertical lines denote simultaneous 95% CIs for the relative risk, accounting for spatial dependence across the subregions. The HOLC grades are A: “Best”, B: “Still Desirable”, C: “Declining”, and D: “Hazardous”. Subregions not graded by the HOLC are denoted E.
Discussion
This study demonstrated how historical redlining designations relate to present-day disparities in tobacco retailer density in thirteen cities in Ohio. Specifically, more than eighty years after the HOLC drew its lines for investment/disinvestment, areas of cities originally graded as “Best” had lower tobacco retail density compared to those graded “Still Desirable,” which, in turn, had lower density than those graded “Definitely Declining” or “Hazardous.” The effect remained in analyses that accounted for present-day sociodemographics, suggesting a lasting effect of redlining in these cities. This finding adds quantitative evidence to qualitative and anecdotal claims made in a previous publication about the relation between redlining and tobacco retailer density.21 This finding also aligns with other research indicating an association between redlining and elements of the built environment, such as less access to healthy food and more access to alcohol outlets.3,4,7,8
To our knowledge, this study is the first to examine the lasting association between historic redlining policy and current tobacco retailer density. Whereas most existing literature about disparities in tobacco retailer density focuses on inequities seen across areas with differing current sociodemographic factors such as racial composition and income level, this study provides insight into the processes that led to the current distribution of tobacco retailers. Importantly, our analyses also used a spatial modeling approach to sufficiently adjust for spatial dependence in retailer density. The fact that, even with these rigorous methods and accounting for present-day sociodemographics, we observed an association between historical redlining and subsequent retailer density suggests there was a causal relationship. The sequence of events also argues against assumptions that tobacco retailers are denser in low-income and minority neighborhoods simply to meet the demands of their clientele.
Limitations and Future Directions
This study examined only thirteen of the fourteen cities in Ohio that were redlined because Cincinnati’s redlining map was unavailable from the National Archives34 (likely either misplaced or destroyed). Some Ohio cities examined also lacked subregions with a high prevalence of Hispanics or had zero counts for certain HOLC grades. As analyses were limited to Ohio, further research is needed to confirm whether findings generalize to other U.S. cities. While the HOLC created residential security maps in a systematic way and used consistent criteria to assign areas A, B, C, or D grades, the implementation of these maps by the Federal Housing Administration, banks, and other organizations varied greatly by region. The model utilized in this study can be replicated to examine tobacco retailer density across the U.S. The model can also be adapted to investigate the association between historic redlining, current sociodemographic factors, and other public health issues.
Implications
A full understanding of present-day disparities requires an appreciation for the historical machinations that led to them. This study highlights the far-reaching and persisting impacts of historical redlining, in terms of the lasting consequences of disinvestment and neighborhood reputation. While the original redlining policy was focused on mortgage lending, the resulting disinvestment in areas graded “Definitely Declining” or “Hazardous” created inequalities across all sectors. Neighborhoods considered less desirable were avoided by key health-promoting retailers, and left to be targeted by predatory markets, such as tobacco retailers. Given the established deleterious impact of living in an areas with high tobacco retailer density,16,22-26 the lasting consequences for health disparities are serious.
This information can be used for programs aimed at raising awareness of redlining and other historical examples of structural racism. While existing education about redlining may mention increased access to generally deleterious resources in previously redlined areas, this paper brings to light a specific association between redlining and tobacco retailer density that can be incorporated into education moving forward.
It is important to note that historical redlining cannot serve as a proxy for present-day geographically-based disparities, especially as many underserved populations have spread beyond historically redlined borders.39 Therefore, although it’s imperative to understand the historical roots of disparities, public health should focus on where present-day disparities lie when directing its efforts. For example, given that underage sales are more likely in low-income and racial/ethnic minority neighborhoods,40-44 strong enforcement of the minimum legal sales age is needed in disadvantaged neighborhoods. Another promising approach that directly addresses disparities in tobacco retailer density is tobacco licensing law policies. These policies can be implemented to reduce or restrict some aspect of the tobacco retailer landscape (e.g., restricting tobacco sales within 1000 feet of a school). Research indicates that, when paired appropriately with their community, licensing laws have the potential for equitable impacts—reducing density the most in vulnerable neighborhoods.44 Public health practitioners and policy makers should advocate for and implement these and other policies to dismantle structural racism and promote more equitable conditions. Since the creation of redlining maps and the disinvestment of redlined neighborhoods were intentional, actions taken to dismantle the lasting impacts of redlining must also be intentional.
Supplementary Material
Highlights.
In the 1930s U.S., the Home Owners’ Loan Corporation (HOLC) was esablished
HOLC graded urban neighborhoods on their desibarilty for investment
African American and low-income neighborhoods received poor grades (“redlining”)
Today, disparities in tobacco retailer density impact initiation and cessation
We examined how historical redlining relates to current disparities in density
Analyses showed worse HOLC grades related to greater tobacco retailer density
These results highlight the persisting impacts of redlining-based disparities
Acknowledgements:
This work was supported by the National Cancer Institute under grant R21CA212308.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Mitchell B, Franco J. HOLC “redlining” maps: The persistent structure of segregation and economic inequality » NCRC. NCRC. Published March 20, 2018. Accessed May 7, 2020. https://ncrc.org/holc/ [Google Scholar]
- 2.Nier C Perpetuation of Segregation: Toward a New Historical and Legal Interpretation of Redlining under the Fair Housing Act, 32 J. Marshall L. Rev. 617 (1999). John Marshall Law Rev. 1999;32(3):51. [Google Scholar]
- 3.New York Law School Racial Justice Project. Unshared Bounty: How Structural Racism Contributes to the Creation and Persistence of Food Deserts. (with American Civil Liberties Union). 2012. Racial Justic Project. Book 3. [Google Scholar]
- 4.Zhang M, Debarchana G. Spatial Supermarket Redlining and Neighborhood Vulnerability: A Case Study of Hartford, Connecticut. Trans GIS TG. 2016;20(1):79–100. doi: 10.1111/tgis.12142 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kwate NOA, Loh JM, White K, Saldana N. Retail Redlining in New York City: Racialized Access to Day-to-Day Retail Resources. J Urban Health Bull N Y Acad Med. 2013;90(4):632–652. doi: 10.1007/s11524-012-9725-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hannon L, Sawyer P, Allman RM. Housing, the Neighborhood Environment, and Physical Activity among Older African Americans. J Health Disparities Res Pract. 2012;5(3):27–41. [PMC free article] [PubMed] [Google Scholar]
- 7.Trangenstein PJ, Gray C, Rossheim ME, Sadler R, Jernigan DH. Alcohol Outlet Clusters and Population Disparities. J Urban Health Bull N Y Acad Med. 2020;97(1):123–136. doi: 10.1007/s11524-019-00372-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Maxwell A, Immergluck D. Liquorlining: Liquor Store Concentration and Community Development in Lower-Income Cook County Neighborhoods. Published online January 1997. Accessed May 7, 2020. https://woodstockinst.org/wp-content/uploads/2013/05/liquorlining.pdf [Google Scholar]
- 9.Aaronson D, Hartley D, Mazumder B. The Effects of the 1930s HOLC “Redlining” Maps (REVISED February 2019) - Federal Reserve Bank of Chicago. Accessed May 7, 2020. https://www.chicagofed.org/publications/working-papers/2017/wp2017-12 [Google Scholar]
- 10.McClure E, Feinstein L, Cordoba E, et al. The legacy of redlining in the effect of foreclosures on Detroit residents’ self-rated health. Health Place. 2019;55:9–19. doi: 10.1016/j.healthplace.2018.10.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Jacoby SF, Dong B, Beard JH, Wiebe DJ, Morrison CN. The enduring impact of historical and structural racism on urban violence in Philadelphia. Soc Sci Med 1982. 2018;199:87–95. doi: 10.1016/j.socscimed.2017.05.038 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Nardone A, Casey JA, Morello-Frosch R, Mujahid M, Balmes JR, Thakur N. Associations between historical residential redlining and current age-adjusted rates of emergency department visits due to asthma across eight cities in California: an ecological study. Lancet Planet Health. 2020;4(1):e24–e31. doi: 10.1016/S2542-5196(19)30241-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Reece J, Martin M, Bates J, Golden A, Mailman K, Nimps R. History Matters: Understanding the Role of Policy, Race and Real Estate in Today’s Geography of Health Equity and Opportunity in Cuyahoga County. Kirwan Institute for the Study of Race & Ethnicity & The City & Regional Planning Program at the Knowlton School of Architecture The Ohio State University; 2015:32. http://kirwaninstitute.osu.edu/wp-content/uploads/2015/02/history-of-race-real-estate.pdf [Google Scholar]
- 14.Beyer KMM, Zhou Y, Matthews K, Bemanian A, Laud PW, Nattinger AB. New spatially continuous indices of redlining and racial bias in mortgage lending: links to survival after breast cancer diagnosis and implications for health disparities research. Health Place. 2016;40:34–43. doi: 10.1016/j.healthplace.2016.04.014 [DOI] [PubMed] [Google Scholar]
- 15.Zhou Y, Bemanian A, Beyer KMM. Housing Discrimination, Residential Racial Segregation, and Colorectal Cancer Survival in Southeastern Wisconsin. Cancer Epidemiol Biomark Prev Publ Am Assoc Cancer Res Cosponsored Am Soc Prev Oncol. 2017;26(4):561–568. doi: 10.1158/1055-9965.EPI-16-0929 [DOI] [PubMed] [Google Scholar]
- 16.Loomis BR, Kim AE, Goetz JL, Juster HR. Density of tobacco retailers and its association with sociodemographic characteristics of communities across New York. Public Health. 2013;127(4):333–338. doi: 10.1016/j.puhe.2013.01.013 [DOI] [PubMed] [Google Scholar]
- 17.Fakunle DO, Milam AJ, Furr-Holden CDM, Butler J, Thorpe RJ, LaVeist TA. The Inequitable Distribution of Tobacco Outlet Density: The Role of Income in Two Black Mid-Atlantic Geopolitical Areas. Public Health. 2016;136:35–40. doi: 10.1016/j.puhe.2016.02.032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Adibe C, Craigmile PF, Onnen N, Schwartz E, Roberts ME. The Relationship between Tobacco Retailer Density and Neighborhood Demographics in Ohio. Ohio J Public Health. 2019;2(1):7. [PMC free article] [PubMed] [Google Scholar]
- 19.Bay M, Fabian A. Race and Retail: Consumption Across the Color Line. Rutgers University Press; 2015. [Google Scholar]
- 20.Fakunle DO, Curriero FC, Leaf PJ, Furr-Holden DM, Thorpe RJ. Black, white, or green? The effects of racial composition and socioeconomic status on neighborhood-level tobacco outlet density. Ethn Health. 2019:1–16. doi: 10.1080/13557858.2019.1620178 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lee JGL, Sun DL, Schleicher NM, Ribisl KM, Luke DA, Henriksen L. Inequalities in tobacco outlet density by race, ethnicity, and socioeconomic status, 2012, USA: Results from the ASPiRE Study. J Epidemiol Community Health. 2017;71(5):487–492. doi: 10.1136/jech-2016-208475 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Pearce J, Hiscock R, Moon G, Barnett R. The neighbourhood effects of geographical access to tobacco retailers on individual smoking behaviour. J Epidemiol Community Health. 2009;63(1):69–77. doi: 10.1136/jech.2007.070656 [DOI] [PubMed] [Google Scholar]
- 23.Peterson NA, Lowe JB, Reid RJ. Tobacco outlet density, cigarette smoking prevalence, and demographics at the county level of analysis. Subst Use Misuse. 2005;40(11):1627–1635. doi: 10.1080/10826080500222685 [DOI] [PubMed] [Google Scholar]
- 24.Lee JGL, Henriksen L, Rose SW, Moreland-Russell S, Ribisl KM. A Systematic Review of Neighborhood Disparities in Point-of-Sale Tobacco Marketing. Am J Public Health. 2015;105(9):e8–18. doi: 10.2105/AJPH.2015.302777 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Lipperman-Kreda S, Mair C, Grube JW, Friend KB, Jackson P, Watson D. Density and proximity of tobacco outlets to homes and schools: relations with youth cigarette smoking. Prev Sci Off J Soc Prev Res. 2014;15(5):738–744. doi: 10.1007/s11121-013-0442-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Cantrell J, Anesetti-Rothermel A, Pearson JL, Xiao H, Vallone D, Kirchner TR. The impact of the tobacco retail outlet environment on adult cessation and differences by neighborhood poverty. Addict Abingdon Engl. 2015;110(1):152–161. doi: 10.1111/add.12718 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.United States Surgeon General. The Health Consequences of Smoking -- 50 Years of progress: A Report of the Surgeon General: (510072014-001). Published online 2014. doi: 10.1037/e510072014-001 [DOI] [Google Scholar]
- 28.Webb Hooper M Editorial: Preventing Tobacco-Related Cancer Disparities: A Focus on Racial/Ethnic Minority Populations. Ethn Dis. 28(3):129–132. doi: 10.18865/ed.28.3.129 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Simmons VN, Pineiro B, Hooper MW, Gray JE, Brandon TH. Tobacco-Related Health Disparities Across the Cancer Care Continuum. Cancer Control J Moffitt Cancer Cent. 2016;23(4):434–441. doi: 10.1177/107327481602300415 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Margerison-Zilko C, Cubbin C. Socioeconomic disparities in tobacco-related health outcomes across racial/ethnic groups in the United States: National Health Interview Survey 2010. Nicotine Tob Res Off J Soc Res Nicotine Tob. 2013;15(6):1161–1165. doi: 10.1093/ntr/nts256 [DOI] [PubMed] [Google Scholar]
- 31.R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. 2020. https://www.R-project.org/ [Google Scholar]
- 32.Kates FR, Salloum RG, Thrasher JF, Islam F, Fleischer NL, Maziak W. Geographic Proximity of Waterpipe Smoking Establishments to Colleges in the U.S. Am J Prev Med. 2016;50(1):e9–e14. doi: 10.1016/j.amepre.2015.07.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Craigmile PF, Onnen N, Schwartz E, Glassser A, Roberts ME. Evaluating how licensing-law strategies will impact disparities in tobacco retailer density: a simulation in Ohio. Tob Control. Published online August 21, 2020. doi: 10.1136/tobaccocontrol-2020-055622 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Nelson R, Winling L, Marciano R, Connolly N. Mapping Inequality. Richmond University. Accessed May 7, 2020. https://dsl.richmond.edu/panorama/redlining/ [Google Scholar]
- 35.TIGER/Line® Shapefiles. Accessed August 24, 2020. https://www.census.gov/cgi-bin/geo/shapefiles/index.php
- 36.Weessies K LibGuides: Finding Census Tract Data: About Census Tracts. Michigan State University Libraries. Accessed May 7, 2020. //libguides.lib.msu.edu/c.php?g=96120&p=625755 [Google Scholar]
- 37.Waller LA, Gotway CA. Applied Spatial Statistics for Public Health Data. Wiley; 2004. [Google Scholar]
- 38.Dean AM, Voss D, Draguljic D. Design and Analysis of Experiments. 2nd ed. Springer; 2017. [Google Scholar]
- 39.Harshbarger AMP and D. America’s formerly redlined neighborhoods have changed, and so must solutions to rectify them. Brookings. Published October 14, 2019. Accessed August 24, 2020. https://www.brookings.edu/research/americas-formerly-redlines-areas-changed-so-must-solutions/ [Google Scholar]
- 40.Asumda F, Jordan L. Minority youth access to tobacco: A neighborhood analysis of underage tobacco sales. Health Place. 2009;15(1):140–147. doi: 10.1016/j.healthplace.2008.03.006 [DOI] [PubMed] [Google Scholar]
- 41.Dai H, Hao J. The effects of tobacco control policies on retailer sales to minors in the USA, 2015. Tob Control. Published online February 20, 2017:tobaccocontrol-2016-053408. doi: 10.1136/tobaccocontrol-2016-053408 [DOI] [PubMed] [Google Scholar]
- 42.Lee JGL, Landrine H, Torres E, Gregory KR. Inequities in tobacco retailer sales to minors by neighbourhood racial/ethnic composition, poverty and segregation, USA, 2015. Tob Control. Published online September 8, 2016:tobaccocontrol-2016-053188. doi: 10.1136/tobaccocontrol-2016-053188 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Lipperman-Kreda S, Grube JW, Friend KB. Contextual and community factors associated with youth access to cigarettes through commercial sources. Tob Control. 2014;23(1):39–44. doi: 10.1136/tobaccocontrol-2012-050473 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Landrine H, Corral I, Klonoff EA, et al. Ethnic Disparities in Youth Access to Tobacco: California Statewide Results, 1999-2003. Health Promot Pract. 2010;11(1):132–139. doi: 10.1177/1524839908317230 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.