

Abstract
Cognitive–behavioural models of health anxiety propose a positive association between information seeking and health anxiety; however, it is unclear the extent to which cognitive mechanisms may mediate this relationship. Catastrophic cognitions are one type of cognition that may mediate this relationship, and the COVID‐19 pandemic has presented an opportunity to examine these relationships within the context of a global health catastrophe. The current study investigated both cross‐sectional (N = 797) and longitudinal (n = 395) relationships between information seeking, health anxiety and catastrophizing during the pandemic. Data were collected using Amazon Mechanical Turk during April and May 2020. Information seeking and health anxiety were positively associated both cross‐sectionally and longitudinally (rs = .25–.29). Catastrophic cognitions significantly mediated the relationship between information seeking and health anxiety both cross‐sectionally and longitudinally. Developing effective methods of reducing information seeking and catastrophizing may serve to reduce health anxiety during global health crises such as the current pandemic.
Keywords: catastrophizing, cognition, COVID‐19, health anxiety, information seeking
Key Practitioner Message.
Health anxiety is an issue of concern during the COVID‐19 pandemic.
Assessing and reducing levels of information seeking and catastrophic cognitions during treatment may be helpful to reduce health anxiety.
Approaches such as cognitive–behavioural therapy may be particularly effective to reduce information seeking and catastrophic cognitions.
1. INTRODUCTION
Health anxiety is characterized by either the appraisal of benign bodily sensations as indicating the presence of a serious illness or being overly worried about contracting an illness (Asmundson & Fergus, 2019). Cognitive models highlight the importance of cognitive and behavioural factors in both the development and maintenance of health anxiety (Abramowitz et al., 2002; Salkovskis & Warwick, 2001; Taylor & Asmundson, 2004). Catastrophic cognitions, focusing on ‘worst‐case scenario’ predictions, are one cognitive factor that has been associated with health anxiety (Marcus et al., 2007). Behavioural responses to health anxiety can be varied, and one common response is reassurance seeking to reduce health‐related fears (Abramowitz et al., 2002). Information seeking is an example of a reassurance behaviour. Specifically, information regarding the feared illness is sought to reassure oneself that the likelihood of having contracted the illness is low. Paradoxically, information seeking places more attention on the feared illness and can actually serve to maintain health anxiety (McMullan et al., 2019; Salkovskis & Warwick, 1986, 2001).
Information seeking involves either intentionally pursuing information (e.g., searching for information on the internet) or inactively acquiring information (e.g., seeing news while using social media; Kelly et al., 2014). Health‐related information seeking has been found to be very prevalent, with people being more likely to engage in information seeking in response to uncertainty of information presented in the media (Guillaume & Bath, 2004). Over a 1‐year period, close to three quarters of US adults sought out health‐related information (Fox & Duggan, 2013). Information seeking is beneficial when done to exercise autonomy (Brashers et al., 2002). For example, information seeking can be an important component of shared decision making between patient and clinician (Moumjid et al., 2007) and can help encourage greater communication between patients and their healthcare providers (Hong, 2008). Greater information seeking is also associated with an increase in preventative health behaviours such as hand washing during the current pandemic (Liu, 2020). However, greater health‐related information seeking is also associated with negative outcomes. Specifically, individuals who engage in health‐related information seeking are more likely to diagnose themselves with an illness (Larner, 2006) and may be less likely to adhere to treatment protocols (Weaver et al., 2009). A recent meta‐analysis of 20 studies found that greater information seeking was associated with higher levels of health anxiety with moderate effect sizes (McMullan et al., 2019). Further, during periods of high risk, greater information seeking is also associated with higher levels of anxiety (Turner et al., 2006).
The association between information seeking and health anxiety is well documented, such that information seeking is more common in those with higher levels of health anxiety (Baumgartner & Hartmann, 2011; Lee & Hawkins, 2016; Muse et al., 2012). Greater levels of online health information seeking, as well as greater participation in the posting of health‐related information on online forums, is associated with greater self‐reported health anxiety (Baumgartner & Hartmann, 2011). Furthermore, individuals with higher levels of health anxiety tend to seek out health‐related information to alleviate their anxiety (Asmundson & Taylor, 2020). While seeking out information as an act of reassurance seeking may temporarily alleviate one's anxiety, overall, seeking out health‐related information actually serves to increase one's anxiety long‐term due to negative reinforcement of the information‐seeking behaviours (Starcevic & Berle, 2013). Specifically, those who seek out health‐related information are more likely to worry if they have higher levels of health anxiety, than those who have lower levels of health anxiety (Baumgartner & Hartmann, 2011). During the current pandemic, this relationship between information seeking and health anxiety has been supported. A recent study found that trait health anxiety moderates the relationship between current COVID‐19 anxiety and excessive health‐related internet search behaviour, such that a greater level of trait health anxiety is associated with a stronger link between excessive health‐related internet search behaviour and COVID‐19 anxiety (Jungmann & Witthöft, 2020). However, conversely, health‐related worries were also found to predict health information seeking (Lee & Hawkins, 2016), suggesting that the relationship between health anxiety and information seeking may be bidirectional.
Despite the established positive association between information seeking and health anxiety, there has been little examination of factors that mediate this relationship (Go & You, 2018). Catastrophic cognitions are ‘worst‐case scenario’ predictions of highly dangerous or threatening outcomes (Gautreau et al., 2015; Marcus et al., 2008). For example, individuals who catastrophize about bodily sensations may jump to the conclusion that benign bodily sensations may be indicative of serious underlying medical diseases. These cognitions may be one potential mediator of the relationship between information seeking and health anxiety. Cognitive models of health anxiety emphasize the role of catastrophic cognitions in the development and maintenance of health anxiety, as well as the extant relationship between information seeking and health anxiety (Warwick & Salkovskis, 1990). Warwick and Salkovskis' (1990) model of health anxiety attributes the development of health anxiety to the dysfunctional beliefs that individuals have about the prevalence and transmission of disease. These beliefs can be triggered by events, such as encountering information about the disease (Baumgartner & Hartmann, 2011). For example, an individual may watch a news report about a new illness circulating in their community, learn about the bodily symptoms associated with this illness and start to mistakenly perceive that these symptoms are present in themselves, which can in turn lead to greater levels of anxiety and distress. Thus, seeking information about the illness resulted in greater levels of health anxiety. In this example, if the same individual were to start making negative predictions about their health, based on an evaluation of their perceived symptoms, this would be an example of a catastrophic cognition. Therefore, revisiting the initial examples, individuals who watch a news report about a new illness circulating in the community (i.e. participating in information seeking) may then be more likely to start to mistakenly perceive that they are experiencing the symptoms of the illness and make negative predictions about their own health (i.e., experiencing catastrophic cognitions), which will result in them likely experiencing greater levels of anxiety about their health. Indeed, catastrophic cognitions can take the form of overly negative predictions about the effects of a disease at both the individual and societal levels, which have been shown to be associated with greater levels of health anxiety (Weck et al., 2012). Catastrophic cognitions have also been linked with information‐seeking behaviour, as those who engage in more information seeking are associated with having greater levels of pain catastrophizing (Verhoeven et al., 2012). Given the established associations between information seeking, catastrophizing and health anxiety, and the role of catastrophic cognitions in maintaining health anxiety, it is possible that catastrophic cognitions mediate the relationship between information seeking and health anxiety; however, this has never been examined. Uncovering mechanisms associated with developing and maintaining health anxiety will be critical to developing targeted treatments.
The COVID‐19 pandemic has created a global context that is ideal for examining these interrelationships. Global crises, such as the current pandemic, are associated with an increased propensity to seek information about the crisis (Dillard et al., 2020; Silver & Matthews, 2017). Following announcements of the first COVID‐19 cases in the United States, internet searches of terms such as ‘coronavirus symptoms’ and ‘hand sanitizer’ increased from 35% to 52% (Bento et al., 2020). Similarly, health anxiety has increased during the pandemic (Özdin & Bayrak Özdin, 2020), while psychological well‐being has decreased (Vindegaard & Benros, 2020). Some countries have even reported that the number of individuals reporting high levels of anxiety has doubled (16% to 38%) since the onset of the pandemic (Dozois & Mental Health Research Canada, 2020). Furthermore, catastrophic cognitions about COVID‐19 have also been found to contribute to various psychiatric symptoms associated with disorders such as depression, agoraphobia and panic disorder (Rosebrock et al., 2021). Overall, individuals feeling stressed about the potential of being infected with COVID‐19, as well as feeling stressed as a result of global social isolation orders, has resulted in numerous negative emotional outcomes (e.g., depression and anxiety), which has bolstered the need for psychosocial interventions to help target these needs (Pfefferbaum & North, 2020). Thus, identifying factors that are associated with these negative emotional outcomes is the first step towards developing streamlined interventions to help target these negative states and promote greater psychological well‐being during the current pandemic.
The present study had two aims: (1) to examine the relationship between information seeking and health anxiety during the COVID‐19 pandemic and (2) to evaluate whether catastrophic cognitions mediate the relationship between information seeking and health anxiety. To our knowledge, this is the first study examining the relationship between information seeking, health anxiety and catastrophizing during the COVID‐19 pandemic and is the first study to examine whether catastrophic cognitions mediate the relationship between information seeking and health anxiety.
2. METHODS
2.1. Participants and procedure
Participants were recruited through Amazon Mechanical Turk (MTurk) as part of a larger study on mental health and quality of life during the COVID‐19 pandemic (Leibovitz et al., 2021; Shamblaw et al., 2021). MTurk has been validated for use in psychological research (Clifford et al., 2015), with evidence indicating that data collected on MTurk is more representative of community‐based demographics than other sampling techniques (Cheung et al., 2017). Participants in this study could access the survey if they had a Canadian‐ or US‐based internet protocol (IP) address and a 99% approval rating from other requesters for prior MTurk tasks, indicating accurate completion of tasks. We recruited 1000 participants for the baseline survey. In our survey, we also embedded an effort measure, specifically comprising of nonsensical questions, as an attention check. Participants were required to respond to at least three out of four effort questions correctly, in order to be eligible for the final sample. Based on past research, we expected to exclude 20% to 25% of responses due to failure of effort items, which would result in an analysable baseline sample of 750 to 800 participants. Of this sample, a 50% attrition rate was expected for the follow‐up survey based on previous MTurk studies. This would result in a final longitudinal sample of approximately 400 participants, which is sufficient to detect small to moderate mediation effects (Fritz & MacKinnon, 2007). This recruitment approach ensured that all analyses in the current study would be adequately powered. The baseline survey (T1) was accessed between 21 and 25 April 2020 and participants completed the follow‐up survey (T2) approximately 1 month later between 21 and 27 May 2020. Participants were compensated with $2 (USD) for each survey, and participants that passed the effort questions on both surveys were provided with a bonus $2 (USD). This research was approved by the University of Toronto Research Ethics Board. All participants provided written informed consent.
2.2. Materials
2.2.1. Information seeking
Information seeking was assessed with the following items: (1) ‘Number of times per day intentionally checking COVID‐19‐related news’ and (2) ‘Number of times per day you see/hear news related to COVID‐19 without seeking it out (e.g., seeing posts on social media)?’. Both items were rated on a 5‐point scale: ‘0’ (none), ‘1’ (1–2 times per day), ‘2’ (3–5 times per day), ‘3’ (6–10 times per day), ‘4’ (11–20 times per day) and ‘5’ (21+ times per day). Higher scores indicate more information seeking.
2.2.2. HAQ (Lucock & Morley, 1996)
The Health Anxiety Questionnaire (HAQ) is a 21‐item self‐report measure that assesses health anxiety across four domains: health worry and preoccupation, fear of illness and death, reassurance‐seeking behaviour and interference with life. Items are rated on a 4‐point scale ranging from ‘0’ (not at all or rarely) to ‘3’ (most of the time) with higher scores indicating greater health anxiety. A total score is created by summing all items. In the current study, internal consistency was α = .941 for the total scale at baseline. At follow‐up, internal consistency was α = .945 for the total scale at baseline.
2.2.3. Catastrophic cognitions
Catastrophic cognitions were assessed with the following items: (1) ‘What do you think is the likelihood of contracting COVID‐19 during the current outbreak?’; (2) ‘What do you think is the likelihood of a family member or friend contracting COVID‐19?’; (3) ‘What do you think is the likelihood of surviving COVID‐19 if infected?’; (4) ‘What do you think is the likelihood of a family member or friend surviving COVID‐19 if infected?’; (5) ‘How long do you think the COVID‐19 pandemic will continue for?’; (6) ‘How long do you think it will take the economy to recover after the COVID‐19 pandemic is over?’ and (7) ‘What is the likelihood that society will ever return to normal?’. Items 1 through 4 and Item 7 were rated on a 10‐point scale: ‘0’ (0% to 9%), ‘1’ (10% to 19%), ‘2’ (20% to 29%), ‘4’ (40% to 49%), ‘5’ (50% to 59%), ‘6’ (60% to 69%), ‘7’ (70% to 79%), ‘8’ (80% to 89%) and ‘9’ (90% to 100%). Scores for all these items were transformed to a 10‐point scale from 1 to 10 for the purpose of the analyses. Items 3 and 4 were reverse coded. For Question 5, items were rated on a 6‐point scale: ‘0’ (less than 1 month), ‘1’ (1–3 months), ‘2’ (4–6 months), ‘3’ (6 months to 1 year), ‘4’ (1–2 years) and ‘5’ (2+ years). For Question 6, items were rated on a 5‐point scale: ‘0’ (less than 1 year), ‘1’ (1–3 years), ‘2’ (3–5 years), ‘3’ (6–10 years) and ‘4’ (10+ years). A total score was calculated as the mean of all items with higher scores indicating more catastrophizing.
2.2.4. Effort items
Four embedded effort questions adapted from Huang et al. (2015) were included to assess response validity: (1) I have never used a computer (valid responses: disagree, somewhat disagree); (2) I eat cement occasionally (valid responses: never, almost never); (3) Select the answer ‘very dissatisfied’ (valid responses: very dissatisfied, dissatisfied) and (4) Select the answer ‘I never feel this way’ (valid responses: I never feel this way, I rarely feel this way). Participants were required to correctly respond to at least three of the effort questions to be included in the final sample.
2.3. Data analyses
All analyses were conducted using IBM SPSS Statistics Version 26. Descriptive statistics were calculated for all demographic (i.e., age, gender and race/ethnicity) and primary study variables (i.e., information seeking, catastrophic cognitions, health anxiety and indirect experience with COVID‐19) at baseline. To examine Aim 1, a cross‐lagged panel analysis was conducted to examine the longitudinal relationship between information seeking and health anxiety. To examine Aim 2, cross‐sectional and longitudinal mediation analyses were conducted using PROCESS version 3.5 (Hayes, 2012). For the cross‐sectional mediation analysis, catastrophic cognitions were examined as a mediator of the relationship between information seeking and health anxiety at baseline (T1). For the longitudinal analysis, catastrophic cognitions at follow‐up (T2) were examined as a mediator of the relationship between information seeking at baseline (T1) and health anxiety at follow‐up (T2). The significance of the indirect path was evaluated by estimating the lower and upper level confidence interval limits of the 95% bias‐corrected bootstrap intervals using 5000 bootstrap iterations.
3. RESULTS
3.1. Participants
Demographic characteristics are presented in Table 1. Descriptive statistics for catastrophic cognitions, information seeking and health anxiety are presented in Table 2.
TABLE 1.
Demographic characteristics of the sample
| Baseline (N = 797) | Longitudinal (n = 395) | |
|---|---|---|
| Age, M years (SD) | 32.2 (11.5) | 33.7 (12.6) |
| Country of residence, n (%) | ||
| USA | 755 (94.7) | 366 (92.7) |
| Canada | 42 (5.3) | 29 (7.3) |
| Gender, n (%) | ||
| Male | 357 (44.8) | 173 (43.8) |
| Female | 435 (54.6) | 220 (55.7) |
| Non‐binary | 3 (0.4) | 2 (0.5) |
| Two‐spirit | 2 (0.3) | 0 (0.0) |
| Ethnicity, n (%) | ||
| White | 538 (67.5) | 274 (69.4) |
| Black | 66 (8.3) | 28 (7.1) |
| Multiracial | 52 (6.5) | 26 (6.6) |
| Latin American | 49 (6.1) | 21 (5.3) |
| South Asian | 36 (4.5) | 20 (5.1) |
| Chinese | 22 (2.8) | 11 (2.8) |
| Southeast Asian | 11 (1.4) | 7 (1.8) |
| Filipino | 8 (1.0) | 3 (0.8) |
| Korean | 4 (0.5) | 1 (0.3) |
| West Asian | 3 (0.4) | 1 (0.3) |
| Indigenous | 2 (0.3) | 1 (0.3) |
| Arab | 2 (0.3) | 1 (0.3) |
| Japanese | 2 (0.3) | 1 (0.3) |
| Other | 2 (0.3) | 0 (0.0) |
TABLE 2.
Descriptive statistics of information seeking, catastrophic cognitions and health anxiety
| Item/scale | Baseline (N = 797) | Follow‐up (n = 395) | ||||
|---|---|---|---|---|---|---|
| M | SD | Range | M | SD | Range | |
| Information‐seeking total score | 1.96 | 0.94 | 5.00 | 1.59 | 0.85 | 5.00 |
| Catastrophic cognitions total score | 3.51 | 1.20 | 7.48 | 3.63 | 1.29 | 8.57 |
| Health Anxiety Questionnaire | 15.41 | 11.71 | 61.00 | 13.58 | 11.17 | 56.00 |
Participants who completed the follow‐up survey were significantly older (M = 33.72, SD = 12.63) compared to participants who did not complete the follow‐up survey (noncompleters; M = 30.80, SD = 10.09, t(795) = 3.60, p < .001). A greater proportion of the noncompleter sample was American (96.7%) compared to completers (92.6%), χ 2(1) = 6.97, p = .01, and noncompleters (M = 3.61, SD = 1.16) were also found to have significantly higher catastrophizing scores than completers (M = 3.41, SD = 1.24). There were no other significant differences between completers and noncompleters on health anxiety, information seeking, gender (female vs. male) or ethnicity (White vs. non‐White), ps > .057.
3.2. Aim 1: Relationship between information seeking and health anxiety
The cross‐lagged panel analysis is displayed in Figure 1. All correlations were significant (p < .001). Information seeking and health anxiety were significantly related at baseline (r = .29) and follow‐up (r = .27). The autocorrelations for both information seeking (r = .53) and health anxiety (r = .75) were high. The temporal effects of information seeking on health anxiety were similar in both directions such that information seeking at baseline was associated with health anxiety at follow‐up (r = .27) and that health anxiety at baseline was associated with information seeking at follow‐up (r = .25).
FIGURE 1.
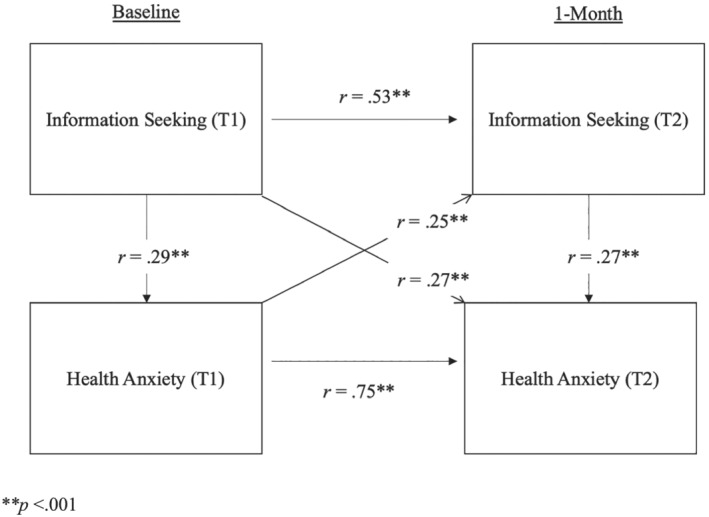
Cross‐lagged panel displaying correlations between information seeking and health anxiety and both baseline and follow‐up
3.3. Aim 2: Mediating role of catastrophizing
At baseline, information seeking was significantly associated with catastrophic cognitions (Path a: 0.17, 95% CI [0.10, 0.24]), and catastrophic cognitions were significantly associated with health anxiety (Path b: 0.29, 95% CI [0.22, 0.35]). The relationship between information seeking and health anxiety (Path c: 0.29, p < .001) was significantly mediated by catastrophic cognitions (Indirect Effect ab: β = 0.05, 95% CI [0.03, 0.08]; Figure 2). When catastrophic cognitions were included in the model, the relationship between information seeking and health anxiety remained significant (Path c′: 0.24, 95% CI [0.17, 0.30]), indicating partial mediation.
FIGURE 2.
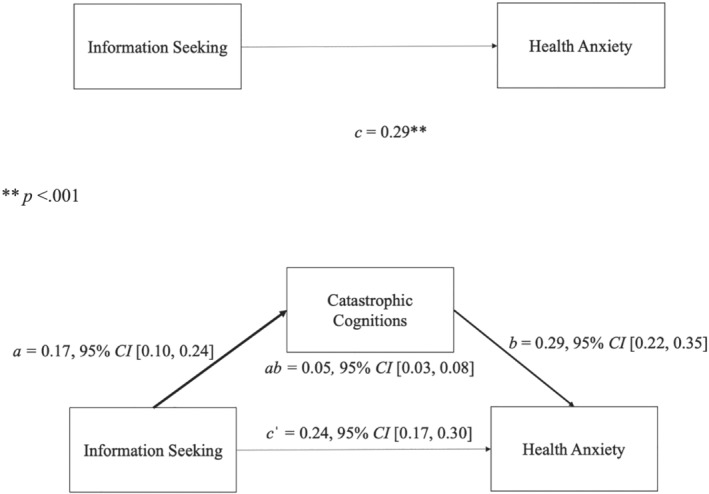
Cross‐sectional relationship between information seeking and health anxiety as mediated by catastrophic cognitions
Longitudinally, information seeking at baseline was significantly associated with catastrophic cognitions at follow‐up (Path a: 0.19, 95% CI [0.09, 0.28]), and catastrophic cognitions at follow‐up were significantly associated with health anxiety at follow‐up (Path b: 0.34, 95% CI [0.25, 0.43]). The relationship between information seeking at baseline and health anxiety at follow‐up (Path c: 0.27, p < .001) was also mediated by catastrophic cognitions (Indirect Effect ab: 0.06, 95% CI [0.02, 0.11]; Figure 3). When catastrophic cognitions were included in the model, the relationship between information seeking and health anxiety remained significant (Path c′: 0.21, 95% CI [0.12, 0.30]), indicating partial mediation.
FIGURE 3.
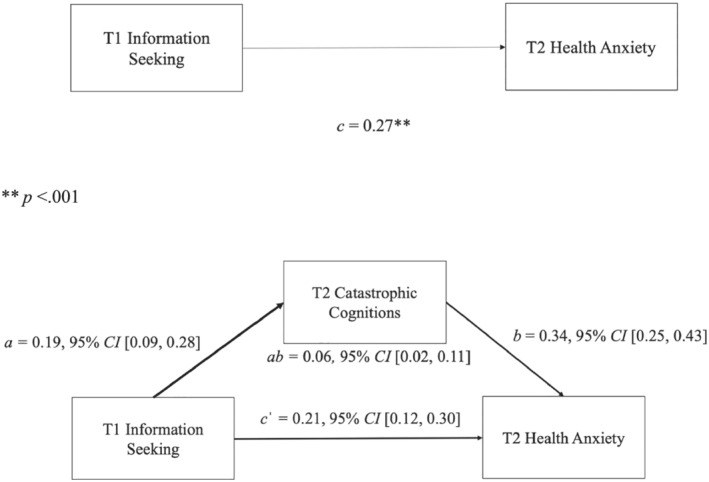
Relationship between information seeking at baseline and health anxiety at follow‐up as mediated by catastrophic cognitions at follow‐up
At baseline, active information was significantly associated with catastrophic cognitions (Path a: 0.20, 95% CI [0.13, 0.27]), and catastrophic cognitions were significantly associated with health anxiety (Path b: 0.28, 95% CI [0.22, 0.35]). The relationship between active information seeking and health anxiety (Path c: 0.26, p < .001) was significantly mediated by catastrophic cognitions (Indirect Effect ab: β = 0.06, 95% CI [0.03, 0.08]; Figure 4). When catastrophic cognitions were included in the model, the relationship between active information seeking and health anxiety remained significant (Path c′: 0.24, 95% CI [0.18, 0.31]), indicating partial mediation.
FIGURE 4.
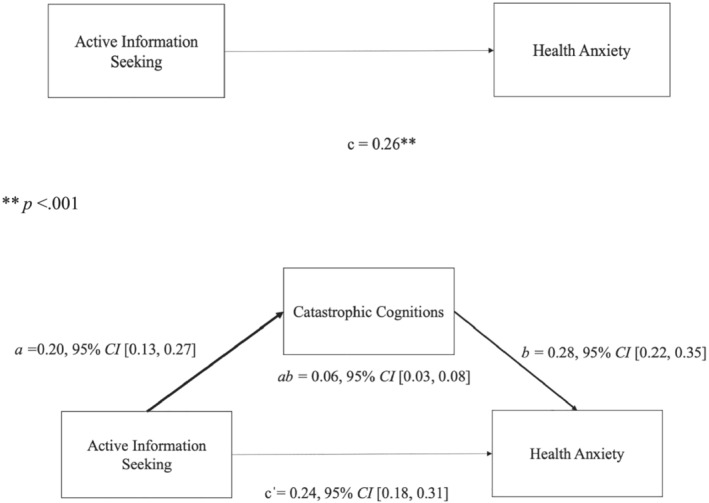
Relationship between active information seeking and health anxiety as mediated by catastrophic cognitions
At baseline, passive information was also significantly associated with catastrophic cognitions (Path a: 0.10, 95% CI [0.03, 0.16]), and catastrophic cognitions were significantly associated with health anxiety (Path b: 0.31, 95% CI [0.25, 0.38]). The relationship between passive information seeking and health anxiety (Path c: 0.09, p = .009) was significantly mediated by catastrophic cognitions (Indirect Effect ab: β = 0.03, 95% CI [0.01, 0.05]; Figure 5). When catastrophic cognitions were included in the model, the relationship between passive information seeking and health anxiety remained significant (Path c′: 0.16, 95% CI [0.09, 0.23]), indicating partial mediation.
FIGURE 5.
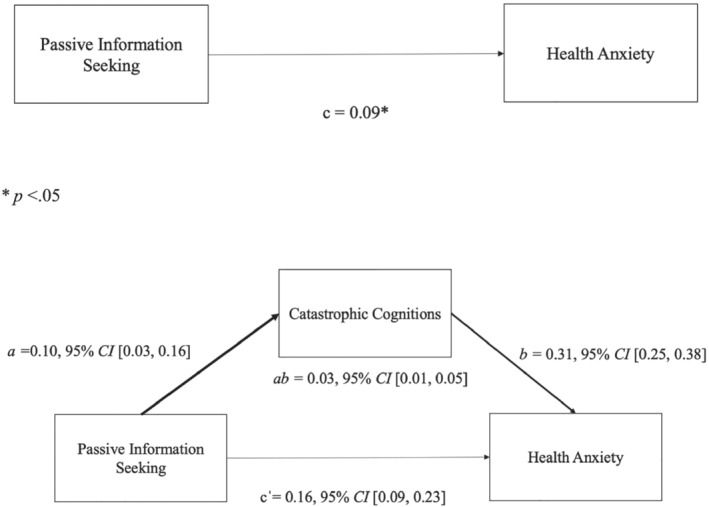
Relationship between passive information seeking and health anxiety as mediated by catastrophic cognitions
Longitudinally, active information seeking was significantly associated with catastrophic cognitions (Path a: 0.21, 95% CI [0.11, 0.30]), and catastrophic cognitions at follow‐up were significantly associated with health anxiety at follow‐up (Path b: 0.35, 95% CI [0.25, 0.44]). The relationship between active information seeking at baseline and health anxiety at follow‐up (Path c: 0.16, p = .002) was also mediated by catastrophic cognitions (Indirect Effect ab: 0.07, 95% CI [0.03, 0.12]; Figure 6). When catastrophic cognitions were included in the model, the relationship between active information seeking and health anxiety remained significant (Path c′: 0.16, 95% CI [0.06, 0.25]), indicating partial mediation.
FIGURE 6.
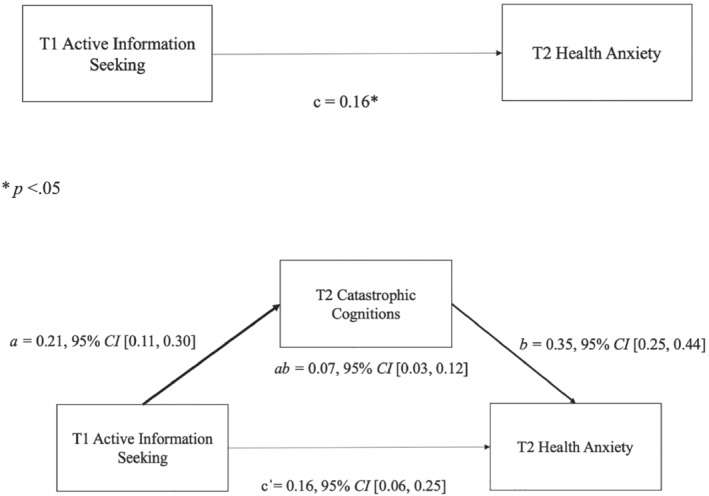
Relationship between active information seeking at baseline and health anxiety at follow‐up as mediated by catastrophic cognitions at follow‐up
Longitudinally, passive information seeking was also significantly associated with catastrophic cognitions (Path a: 0.12, 95% CI [0.20, 0.21]), and catastrophic cognitions were significantly associated with health anxiety at follow‐up (Path b: 0.36, 95% CI [0.27, 0.45]). The relationship between passive information seeking at baseline and health anxiety at follow‐up (Path c: 0.17, p = .001) was also mediated by catastrophic cognitions (Indirect Effect ab: 0.04, 95% CI [0.02, 0.90]; Figure 7). When catastrophic were included in this model, the relationship between passive information seeking and health anxiety remained significant (Path c′: 0.18, 95% CI [0.10, 0.27]), indicating partial mediation.
FIGURE 7.
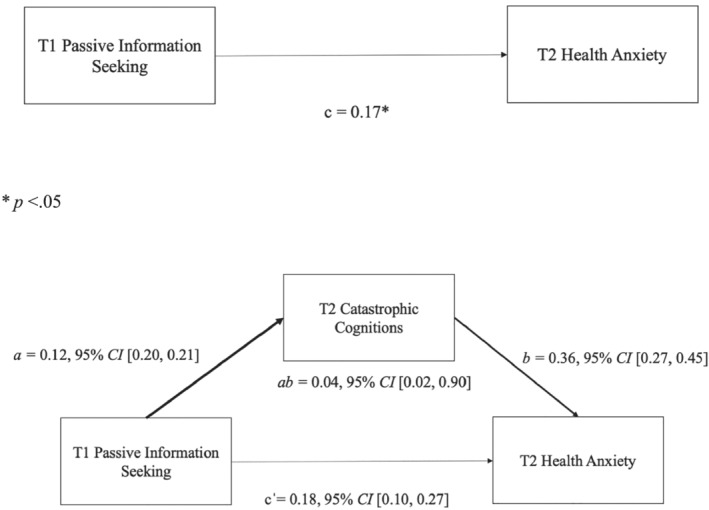
Relationship between passive information seeking at baseline and health anxiety at follow‐up as mediated by catastrophic cognitions at follow‐up
4. DISCUSSION
The current study examined the relationship between information seeking and health anxiety during the COVID‐19 pandemic and whether catastrophic cognitions mediated this relationship. Both passive and active types of information seeking and health anxiety were associated both cross‐sectionally and longitudinally with little evidence for a directional relationship over time. Catastrophic cognitions partially mediated the relationship between passive and active types of information seeking and health anxiety such that greater information seeking was associated with more catastrophic cognitions, which was associated with more health anxiety.
Information seeking is consistently found to be associated with health anxiety (Lagoe & Atkin, 2015; McMullan et al., 2019; te Poel et al., 2016), with cognitive theories indicating that information seeking contributes to both the development and maintenance of health anxiety (Salkovskis & Warwick, 1986; Taylor & Asmundson, 2004). The present results provide further support for this relationship within the context of the COVID‐19 pandemic; however, there was no evidence found for a directional relationship between information seeking and health anxiety over time. Baseline information seeking predicted follow‐up health anxiety to a similar level that baseline health anxiety predicted follow‐up information seeking. At the time of the current study, health anxiety may have already developed to such an extent that it was already in the maintenance phase with a reciprocal relationship in place. Thus, greater information seeking may have been maintaining greater health anxiety and greater health anxiety may have been maintaining greater information seeking. Although data collection occurred early in the pandemic, it may have needed to occur even earlier, at the first news of COVID‐19, to detect any temporal relationships between information seeking and health anxiety.
In addition to the relationship between information seeking and health anxiety, catastrophic cognitions were also found to significantly mediate the relationship between information seeking and health anxiety. Although the relationship between catastrophic cognitions and both information seeking (Gibler et al., 2019; Verhoeven et al., 2012) and health anxiety (Norris & Marcus, 2014; Marcus, 1999; Weck et al., 2012) is well documented (Gautreau et al., 2015; Gibler et al., 2019; Marcus et al., 2008), this is the first study to examine the mediating role of catastrophic cognitions. The mechanism underlying the positive association between information seeking and health anxiety appears to at least be partially a result of a catastrophic cognitive process in which information‐seeking results increase the likelihood that people become fixated on the ‘worst‐case scenario’. Partial mediation was observed in the current study, which may indicate that the information seeking has a direct effect on health anxiety, but it could also suggest that other cognitive factors may be important to consider as mediators in this process.
For example, two factors that may be implicated in the relationship between information seeking and health anxiety are anxiety sensitivity and an attentional bias towards threat. Anxiety sensitivity, referring to the tendency to fear sensations associated with anxious arousal, is a prominent factor associated with anxiety disorders (Abramowitz & Braddock, 2008; Asmundson et al., 2010) and has been identified as a possible vulnerability factor for health anxiety. It may also be considered as a possible mediator of the relationship between information seeking and health anxiety, as it is associated with health anxiety, even after controlling for factors such as depression and negative affect (Olatunji & Wolitzky‐Taylor, 2009). In addition to anxiety sensitivity, the cognitive–behavioural model of health anxiety (Salkovskis & Warwick, 1986) has also implicated certain attentional processes in the development of health anxiety. Specifically, those with higher levels of health anxiety may have an attentional bias towards illness threat which may cause them to selectively attend to information that conforms to the notion of having an illness and ignore other evidence which may disconfirm this (Owens et al., 2004). Thus, it is possible that both anxiety sensitivity and an attentional bias towards threat may act as mediators between information seeking and health anxiety. For example, the relationship between information seeking and health anxiety may be due to the fact that there are certain people who are overly attuned towards the notion of developing an illness, and so when seeking out information generally, they may misinterpret the information negatively in relation to themselves and become more anxious about their health.
The current results suggest several points of intervention to improve health anxiety. Given the positive association between information seeking and health anxiety, assessing and reducing levels of information seeking may be helpful to reduce health anxiety. Reductions in information seeking during internet‐delivered cognitive–behavioural therapy were found to significantly mediate the relationship between treatment and improvements in health anxiety (Newby & McElroy, 2020), suggesting that reducing information seeking is an important mechanism in treatment. During the COVID‐19 pandemic, there is a vast amount of information about COVID‐19 that is often conflicting, and for people with high levels of health anxiety, it may be useful to limit exposure to this information. Catastrophic cognitions may also be useful to assess and treat for individuals with high levels of health anxiety. Cognitive–behavioural therapy is an effective treatment for health anxiety that can decrease both catastrophic cognitions and information seeking (Olatunji et al., 2014). Working to evaluate and reframe catastrophic cognitions through cognitive–behavioural techniques has shown to be useful in other conditions such as generalized anxiety disorder (Stefan et al., 2019) and fibromyalgia (Lazaridou et al., 2017; Nelson & Tucker, 2006) and may be helpful to apply in the context of health anxiety. Within the context of the COVID‐19 pandemic, positive reframing has been the most effective coping strategy to maintain mental health and quality of life (Shamblaw et al., 2021) providing further support for the efficacy of the cognitive–behavioural approaches.
Although information seeking may lead to increased catastrophic cognitions and health anxiety, it is worth considering whether a certain amount of information seeking is beneficial to promote health behaviours during the COVID‐19 pandemic, such as wearing a mask or being vaccinated. There may be a point at which health anxiety changes from supporting health behaviours to becoming unhelpful and associated with health anxiety. Future studies could examine the interrelationships between information seeking, health anxiety and health behaviours to determine at what level information seeking promotes health behaviours and at what level it becomes associated with health anxiety.
These findings should be interpreted with consideration of several limitations. First, the study was conducted on MTurk. While MTurk is advantageous for its ability to conduct rapid, remote research during the pandemic, the use of MTurk may limit the generalizability of the sample since participants must be proficient with using the MTurk platform. Additionally, MTurk samples have also been found to overrepresent certain types of psychopathology, such as social anxiety disorder and depression (Arditte et al., 2016), in addition to having greater levels of negative affect compared to the general population (McCredie & Morey, 2019). However, past research has also shown that MTurk samples are more representative of community‐based demographics than other sampling techniques (Cheung et al., 2017; Clifford et al., 2015). Second, all constructs were assessed using self‐report measures which may be subject to response biases. We also relied on retrospective recall, in particular, for our information seeking measure which has been demonstrated to be poorly correlated with more real‐time measures of affect and experiences, such as ecological momentary assessment (Shiffman et al., 2008). Future studies could benefit from using multimethod assessments including interview‐based measures, as well as real‐time measures such as ecological momentary assessment, to help overcome the limitations associated with self‐report. Third, the assessments of information seeking and catastrophizing were created specifically for this study based on the theoretical constructs being measured and the specific context of COVID‐19. However, these measures had not been previously validated. Additionally, our measure of information was very broad and did not take into account the quality of information individuals may be exposed to. For example, past research has shown that exposure to misinformation or conspiracy theory beliefs is associated with anxiety and depression during the COVID‐19 pandemic (De Coninck et al., 2021). It is possible that seeking our certain types of COVID‐19 information (e.g., conspiracy theories) may differentially influence health anxiety and catastrophic cognitions. Thus, future studies should endeavour to examine the quality and type of information individuals are seeking to further shed light on these relationships. Finally, this study measured anxiety in the general population, rather than using a sample of individuals with diagnosed illness anxiety disorder. It is possible that studies using clinical samples may produce different results.
5. CONCLUSIONS
Information seeking and health anxiety are associated both cross‐sectionally and longitudinally during the COVID‐19 pandemic. The relationship between information seeking and health anxiety was also partially mediated by catastrophic cognitions about the current pandemic, both cross‐sectionally and longitudinally. These results support targeting catastrophic cognitions about the current COVID‐19 pandemic specifically through cognitive–behavioural approaches to treating health anxiety and information seeking.
CONFLICT OF INTEREST
The authors declare no conflicts of interest.
Jagtap, S. , Shamblaw, A. L. , Rumas, R. , & Best, M. W. (2021). Information seeking and health anxiety during the COVID‐19 pandemic: The mediating role of catastrophic cognitions. Clinical Psychology & Psychotherapy, 28(6), 1379–1390. 10.1002/cpp.2684
DATA AVAILABILITY STATEMENT
Data for this study are available upon reasonable request from the authors and research ethics board approval for data sharing.
REFERENCES
- Abramowitz, J. S. , & Braddock, A. (2008). Psychological treatment of health anxiety and hypochondriasis: A biopsychosocial approach. Hogrefe Publishing. [Google Scholar]
- Abramowitz, J. S. , Schwartz, S. A. , & Whiteside, S. P. (2002). A contemporary conceptual model of hypochondriasis. Mayo Clinic Proceedings, 77(12), 1323–1330. 10.4065/77.12.1323 [DOI] [PubMed] [Google Scholar]
- Arditte, K. A. , Çek, D. , Shaw, A. M. , & Timpano, K. R. (2016). The importance of assessing clinical phenomena in Mechanical Turk research. Psychological Assessment, 28(6), 684–691. 10.1037/pas0000217 [DOI] [PubMed] [Google Scholar]
- Asmundson, G. J. G. , Abramowitz, J. S. , Richter, A. A. , & Whedon, M. (2010). Health anxiety: Current perspectives and future directions. Current Psychiatry Reports, 12(4), 306–312. 10.1007/s11920-010-0123-9 [DOI] [PubMed] [Google Scholar]
- Asmundson, G. J. G. , & Fergus, T. A. (2019). The concept of health anxiety. In Hedman‐Lagerlöf E. (Ed.), The clinician's guide to treating health anxiety: Diagnosis, mechanisms, and effective treatment (pp. 1–18). Elsevier Academic Press. 10.1016/B978-0-12-811806-1.00001-9 [DOI] [Google Scholar]
- Asmundson, G. J. G. , & Taylor, S. (2020). How health anxiety influences responses to viral outbreaks like COVID‐19: What all decision‐makers, health authorities, and health care professionals need to know. Journal of Anxiety Disorders, 71(January), 102211. 10.1016/j.janxdis.2020.102211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baumgartner, S. E. , & Hartmann, T. (2011). The role of health anxiety in online health information search. Cyberpsychology, Behavior and Social Networking, 14(10), 613–618. 10.1089/cyber.2010.0425 [DOI] [PubMed] [Google Scholar]
- Bento, A. I. , Nguyen, T. , Wing, C. , Lozano‐Rojas, F. , Ahn, Y. Y. , & Simon, K. (2020). Evidence from internet search data shows information‐seeking responses to news of local COVID‐19 cases. Proceedings of the National Academy of Sciences of the United States of America, 117(21), 11220–11222. 10.1073/pnas.2005335117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brashers, D. E. , Gobldsmith, D. J. , & Hsteh, E. (2002). Information seeking and avoiding in health contexts. Human Communication Research, 28(2), 258–271. 10.1093/hcr/28.2.258 [DOI] [Google Scholar]
- Cheung, J. H. , Burns, D. K. , Sinclair, R. R. , & Sliter, M. (2017). Amazon Mechanical Turk in organizational psychology: An evaluation and practical recommendations. Journal of Business and Psychology, 32(4), 347–361. 10.1007/s10869-016-9458-5 [DOI] [Google Scholar]
- Clifford, S. , Jewell, R. M. , & Waggoner, P. D. (2015). Are samples drawn from Mechanical Turk valid for research on political ideology? Research and Politics, 2(4), 205316801562207. 10.1177/2053168015622072 [DOI] [Google Scholar]
- De Coninck, D. , Frissen, T. , Matthijs, K. , d'Haenens, L. , Lits, G. , Champagne‐Poirier, O. , Carignan, M. E. , David, M. D. , Pignard‐Cheynel, N. , Salerno, S. , & Généreux, M. (2021). Beliefs in conspiracy theories and misinformation about COVID‐19: Comparative perspectives on the role of anxiety, depression and exposure to and trust in information sources. Frontiers in Psychology, 12, 646394. 10.3389/fpsyg.2021.646394 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dillard, J. P. , Li, R. , & Yang, C. (2020). Fear of Zika: Information seeking as cause and consequence. Health Communication, 36(13), 1785–1795. 10.1080/10410236.2020.1794554 [DOI] [PubMed] [Google Scholar]
- Dozois, D. J. A. , & Mental Health Research Canada . (2020). Anxiety and depression in Canada during the COVID‐19 pandemic: A national survey. Canadian Psychology/Psychologie Canadienne, 62, 136–142. 10.1037/cap0000251 [DOI] [Google Scholar]
- Fox, S. , & Duggan, M. (2013). Tracking for health. Pew Research Center's Internet & American Life Project. [Google Scholar]
- Fritz, M. S. , & MacKinnon, D. P. (2007). Required sample size to detect the mediated effect. Psychological Science, 18(3), 233–239. 10.1111/j.1467-9280.2007.01882.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gautreau, C. M. , Sherry, S. B. , Sherry, D. L. , Birnie, K. A. , Mackinnon, S. P. , & Stewart, S. H. (2015). Does catastrophizing of bodily sensations maintain health‐related anxiety? A 14‐day daily diary study with longitudinal follow‐up. Behavioural and Cognitive Psychotherapy, 43(4), 502–512. 10.1017/S1352465814000150 [DOI] [PubMed] [Google Scholar]
- Gibler, R. C. , Jastrowski Mano, K. E. , O'Bryan, E. M. , Beadel, J. R. , & McLeish, A. C. (2019). The role of pain catastrophizing in cyberchondria among emerging adults. Psychology, Health and Medicine, 24(10), 1267–1276. 10.1080/13548506.2019.1605087 [DOI] [PubMed] [Google Scholar]
- Go, E. , & You, K. H. (2018). Health‐related online information seeking and behavioral outcomes: Fatalism and self‐efficacy as mediators. Social Behavior and Personality, 46(5), 871–879. 10.2224/sbp.6501 [DOI] [Google Scholar]
- Guillaume, L. , & Bath, P. A. (2004). The impact of health scares on parents' information needs and preferred information sources: A case study of the MMR vaccine scare. Health Informatics Journal, 10(1), 5–22. 10.1177/1460458204040664 [DOI] [Google Scholar]
- Hayes, A. F. (2012). PROCESS: A versatile computational tool for observed variable mediation, moderation, and conditional process modeling [White paper]. Retrieved from http://www.afhayes.com/public/process2012.pdf
- Hong, T. (2008). Internet health information in the patient‐provider dialogue. Cyberpsychology & Behavior: The Impact of the Internet, Multimedia and Virtual Reality on Behavior and Society, 11(5), 587–589. 10.1089/cpb.2007.0172 [DOI] [PubMed] [Google Scholar]
- Huang, J. L. , Bowling, N. A. , Liu, M. , & Li, Y. (2015). Detecting insufficient effort responding with an infrequency scale: Evaluating validity and participant reactions. Journal of Business and Psychology, 30(2), 299–311. 10.1007/s10869-014-9357-6 [DOI] [Google Scholar]
- Jungmann, S. M. , & Witthöft, M. (2020). Health anxiety, cyberchondria, and coping in the current COVID‐19 pandemic: Which factors are related to coronavirus anxiety? Journal of Anxiety Disorders, 73(April), 102239. 10.1016/j.janxdis.2020.102239 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kelly, S. , Eldredge, S. A. , Dalton, E. D. , & Miller, L. E. (2014). Health‐information behavior: An initial validity portfolio for active and passive measures. Communication Research Reports, 31(2), 171–182. 10.1080/08824096.2014.907145 [DOI] [Google Scholar]
- Lagoe, C. , & Atkin, D. (2015). Health anxiety in the digital age: An exploration of psychological determinants of online health information seeking. Computers in Human Behavior, 52, 484–491. 10.1016/j.chb.2015.06.003 [DOI] [Google Scholar]
- Larner, A. J. (2006). Searching the Internet for medical information: Frequency over time and by age and gender in an outpatient population in the UK. Journal of Telemedicine and Telecare, 12(4), 186–188. 10.1258/135763306777488816 [DOI] [PubMed] [Google Scholar]
- Lazaridou, A. , Kim, J. , Cahalan, C. M. , Loggia, M. L. , Franceschelli, O. , Berna, C. , Schur, P. , Napadow, V. , & Edwards, R. R. (2017). Effects of cognitive‐behavioral therapy (CBT) on brain connectivity supporting catastrophizing in fibromyalgia. The Clinical Journal of Pain, 33(3), 215–221. 10.1097/AJP.0000000000000422 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, S. Y. , & Hawkins, R. P. (2016). Worry as an uncertainty‐associated emotion: Exploring the role of worry in health information seeking. Health Communication, 31(8), 926–933. 10.1080/10410236.2015.1018701 [DOI] [PubMed] [Google Scholar]
- Leibovitz, T. , Shamblaw, A. L. , Rumas, R. , & Best, M. W. (2021). COVID‐19 conspiracy beliefs: Relations with anxiety, quality of life, and schemas. Personality and Individual Differences, 175, 110704. 10.1016/j.paid.2021.110704 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu, P. L. (2020). COVID‐19 information seeking on digital media and preventive behaviors: The mediation role of worry. Cyberpsychology, Behavior and Social Networking, 23(10), 677–682. 10.1089/cyber.2020.0250 [DOI] [PubMed] [Google Scholar]
- Lucock, M. P. , & Morley, S. (1996). The Health Anxiety Questionnaire. British Journal of Health Psychology, 1(2), 137–150. 10.1111/j.2044-8287.1996.tb00498.x [DOI] [Google Scholar]
- Marcus, D. K. (1999). The cognitive‐behavioral model of hypochondriasis: Misinformation and triggers. Journal of Psychosomatic Research, 47(1), 79–91. 10.1016/s0022-3999(99)00008-2 [DOI] [PubMed] [Google Scholar]
- Marcus, D. K. , Gurley, J. R. , Marchi, M. M. , & Bauer, C. (2007). Cognitive and perceptual variables in hypochondriasis and health anxiety: A systematic review. Clinical Psychology Review, 27(2), 127–139. 10.1016/j.cpr.2006.09.003 [DOI] [PubMed] [Google Scholar]
- Marcus, D. K. , Hughes, K. T. , & Arnau, R. C. (2008). Health anxiety, rumination, and negative affect: A mediational analysis. Journal of Psychosomatic Research, 64(5), 495–501. 10.1016/j.jpsychores.2008.02.004 [DOI] [PubMed] [Google Scholar]
- McCredie, M. N. , & Morey, L. C. (2019). Who are the Turkers? A characterization of MTurk workers using the personality assessment inventory. Assessment, 26(5), 759–766. 10.1177/1073191118760709 [DOI] [PubMed] [Google Scholar]
- McMullan, R. D. , Berle, D. , Arnáez, S. , & Starcevic, V. (2019). The relationships between health anxiety, online health information seeking, and cyberchondria: Systematic review and meta‐analysis. Journal of Affective Disorders, 245(July 2018), 270–278. 10.1016/j.jad.2018.11.037 [DOI] [PubMed] [Google Scholar]
- Moumjid, N. , Gafni, A. , Brémond, A. , & Carrère, M. O. (2007). Shared decision making in the medical encounter: Are we all talking about the same thing? Medical Decision Making: An International Journal of the Society for Medical Decision Making, 27(5), 539–546. 10.1177/0272989X07306779 [DOI] [PubMed] [Google Scholar]
- Muse, K. , McManus, F. , Leung, C. , Meghreblian, B. , & Williams, J. M. G. (2012). Cyberchondriasis: Fact or fiction? A preliminary examination of the relationship between health anxiety and searching for health information on the Internet. Journal of Anxiety Disorders, 26(1), 189–196. 10.1016/j.janxdis.2011.11.005 [DOI] [PubMed] [Google Scholar]
- Nelson, P. J. , & Tucker, S. (2006). Developing an intervention to alter catastrophizing in persons with fibromyalgia. Orthopaedic Nursing, 25(3), 205–214. 10.1097/00006416-200605000-00011 [DOI] [PubMed] [Google Scholar]
- Newby, J. M. , & McElroy, E. (2020). The impact of internet‐delivered cognitive behavioural therapy for health anxiety on cyberchondria. Journal of Anxiety Disorders, 69(September 2019), 102150. 10.1016/j.janxdis.2019.102150 [DOI] [PubMed] [Google Scholar]
- Norris, A. , & Marcus, D. K. (2014). Cognition in health anxiety and hypochondriasis: Recent advances. Current Psychiatry Reviews, 10(1), 44–49. 10.2174/1573400509666131119004151 [DOI] [Google Scholar]
- Olatunji, B. O. , Kauffman, B. Y. , Meltzer, S. , Davis, M. L. , Smits, J. A. , & Powers, M. B. (2014). Cognitive‐behavioral therapy for hypochondriasis/health anxiety: A meta‐analysis of treatment outcome and moderators. Behaviour Research and Therapy, 58, 65–74. 10.1016/j.brat.2014.05.002 [DOI] [PubMed] [Google Scholar]
- Olatunji, B. O. , & Wolitzky‐Taylor, K. B. (2009). Anxiety sensitivity and the anxiety disorders: A meta‐analytic review and synthesis. Psychological Bulletin, 135(6), 974–999. 10.1037/a0017428 [DOI] [PubMed] [Google Scholar]
- Owens, K. M. B. , Asmundson, G. J. G. , Hadjistavropoulos, T. , & Owens, T. J. (2004). Attentional bias toward illness threat in individuals with elevated health anxiety. Cognitive Therapy and Research, 28(1), 57–66. 10.1023/B:COTR.0000016930.85884.29 [DOI] [Google Scholar]
- Özdin, S. , & Bayrak Özdin, Ş. (2020). Levels and predictors of anxiety, depression and health anxiety during COVID‐19 pandemic in Turkish society: The importance of gender. International Journal of Social Psychiatry, 66(5), 504–511. 10.1177/0020764020927051 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pfefferbaum, B. , & North, C. S. (2020). Mental health and the Covid‐19 pandemic. New England Journal of Medicine, 383(6), 510–512. 10.1056/NEJMp2008017 [DOI] [PubMed] [Google Scholar]
- Rosebrock, L. , Černis, E. , Lambe, S. , Waite, F. , Rek, S. , Petit, A. , Ehlers, A. , Clark, D. M. , & Freeman, D. (2021). Catastrophic cognitions about coronavirus: The Oxford psychological investigation of coronavirus questionnaire [TOPIC‐Q]. Psychological Medicine, 1–10. 10.1017/S0033291721000283n [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salkovskis, P. M. , & Warwick, H. M. (1986). Morbid preoccupations, health anxiety and reassurance: A cognitive‐behavioural approach to hypochondriasis. Behaviour Research and Therapy, 24(5), 597–602. 10.1016/0005-7967(86)90041-0 [DOI] [PubMed] [Google Scholar]
- Salkovskis, P. M. , & Warwick, H. M. C. (2001). Meaning, misinterpretations, and medicine: A cognitive‐behavioral approach to understanding health anxiety and hypochondriasis. In Starcevic V. & Lipsitt D. R. (Eds.), Hypochondriasis: Modern perspectives on an ancient malady (pp. 202–222). Oxford University Press. [Google Scholar]
- Shamblaw, A. L. , Rumas, R. L. , & Best, M. W. (2021). Coping during the COVID‐19 pandemic: Relations with mental health and quality of life. Canadian Psychology/Psychologie Canadienne, 62, 92–100. 10.1037/cap0000263 [DOI] [Google Scholar]
- Shiffman, S. , Stone, A. A. , & Hufford, M. R. (2008). Ecological momentary assessment. Annual Review of Clinical Psychology, 4, 1–32. 10.1146/annurev.clinpsy.3.022806.091415 [DOI] [PubMed] [Google Scholar]
- Silver, A. , & Matthews, L. (2017). The use of Facebook for information seeking, decision support, and self‐organization following a significant disaster. Information Communication and Society, 20(11), 1680–1697. 10.1080/1369118X.2016.1253762 [DOI] [Google Scholar]
- Starcevic, V. , & Berle, D. (2013). Cyberchondria: Towards a better understanding of excessive health‐related internet use. Expert Review of Neurotherapeutics, 13(2), 205–213. 10.1586/ern.12.162 [DOI] [PubMed] [Google Scholar]
- Stefan, S. , Cristea, I. A. , Szentagotai Tatar, A. , & David, D. (2019). Cognitive‐behavioral therapy (CBT) for generalized anxiety disorder: Contrasting various CBT approaches in a randomized clinical trial. Journal of Clinical Psychology, 75(7), 1188–1202. 10.1002/jclp.22779 [DOI] [PubMed] [Google Scholar]
- Taylor, S. , & Asmundson, G. J. (2004). Treating health anxiety: A cognitive‐behavioral approach. Guilford Press. [Google Scholar]
- te Poel, F. , Baumgartner, S. E. , Hartmann, T. , & Tanis, M. (2016). The curious case of cyberchondria: A longitudinal study on the reciprocal relationship between health anxiety and online health information seeking. Journal of Anxiety Disorders, 43, 32–40. 10.1016/j.janxdis.2016.07.009 [DOI] [PubMed] [Google Scholar]
- Turner, M. M. , Rimal, R. N. , Morrison, D. , & Kim, H. (2006). The role of anxiety in seeking and retaining risk information: Testing the risk perception attitude framework in two studies. Human Communication Research, 32(2), 130–156. 10.1111/j.1468-2958.2006.00006.x [DOI] [Google Scholar]
- Verhoeven, K. , Goubert, L. , Jaaniste, T. , Van Ryckeghem, D. M. , & Crombez, G. (2012). Pain catastrophizing influences the use and the effectiveness of distraction in schoolchildren. European Journal of Pain (London, England), 16(2), 256–267. 10.1016/j.ejpain.2011.06.015 [DOI] [PubMed] [Google Scholar]
- Vindegaard, N. , & Benros, M. E. (2020). COVID‐19 pandemic and mental health consequences: Systematic review of the current evidence. Brain, Behavior, and Immunity, 89, 531–542. 10.1016/j.bbi.2020.05.048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Warwick, H. M. C. , & Salkovskis, P. M. (1990). Hypochondriasis. Behaviour Research and Therapy, 28(2), 105–117. 10.1016/0005-7967(90)90023-C [DOI] [PubMed] [Google Scholar]
- Weaver, J. B. III , Thompson, N. J. , Weaver, S. S. , & Hopkins, G. L. (2009). Healthcare non‐adherence decisions and internet health information. Computers in Human Behavior, 25(6), 1373–1380. 10.1016/j.chb.2009.05.011 [DOI] [Google Scholar]
- Weck, F. , Neng, J. M. , Richtberg, S. , & Stangier, U. (2012). The restrictive concept of good health in patients with hypochondriasis. Journal of Anxiety Disorders, 26(8), 792–798. 10.1016/j.janxdis.2012.07.001 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data for this study are available upon reasonable request from the authors and research ethics board approval for data sharing.