

Abstract
There is a potential for a long‐lasting psychological and social impact from the COVID‐19 pandemic. Recently, the COVID‐19 Anxiety Syndrome Scale (C19‐ASS) has been developed, which measures individuals' coping mechanisms in relation to the fear or threat of COVID‐19. The C19‐ASS was developed and has been used so far only in Western samples. Further psychometric evaluation is needed in ethnically diverse samples. Therefore, the current study sought to test the psychometric properties in a large sample of Iranians (n = 1429; female = 52.1%; Mean age = 35.83, ±12.89) who completed a cross‐sectional survey. Exploratory factor analysis revealed that the Persian C19‐ASS has a two‐factor structure corresponding to the perseveration and avoidance subscales of the original scale. Confirmatory factor analyses also supported a two‐factor solution, which showed a firm model fit and high internal consistencies. Furthermore, it showed excellent divergent validity from generalized anxiety, indicating that it is concerned explicitly with COVID‐19, supported by correlational analyses and exploratory factor analysis. Test of incremental validity indicated the Persian C19‐ASS explained more variance in functional impairment and COVID‐19 anxiety than the gender, marital and educational status, generalized anxiety, neuroticism, openness, consciousness and having lost someone close due to COVID‐19. Also, based on a mediation test, it was found that C19‐ASS mediates the relationship between the Big Five personality traits (except openness and consciousness) and health anxiety, generalized anxiety, depression and COVID‐19 anxiety. Overall, the current findings provide further evidence for the construct of the COVID‐19 anxiety syndrome. The COVID‐19 anxiety syndrome is discussed in light of the S‐REF model that provides an explanatory framework for this pandemic‐related construct.
Keywords: avoidance, COVID‐19 Anxiety Syndrome Scale, factor structure, perseveration, reliability, validity
Key Practitioner Message.
Exploratory and confirmatory factor analyses confirmed perseveration and avoidance as two components of the COVID‐19 anxiety syndrome.
The C19‐ASS can predict COVID‐19 anxiety and functional impairment above and beyond gender, marital and educational status, generalized anxiety, neuroticism, openness, consciousness, and having experienced loss of someone close due to COVID‐19.
The COVID‐19 anxiety syndrome showed potential as a candidate construct for an underlying mechanism of COVID‐19‐related psychopathology.
1. INTRODUCTION
Coronavirus disease (COVID‐19), caused by the SARS‐CoV‐2 virus, was declared a pandemic by the World Health Organization (WHO) on 11 March 2020. By June 2021, there were 176 million reported cases of COVID‐19 infections by WHO (2021); this number is near three million in Iran (Ministry of Health and Medical Education of Iran, 2021).
From the beginning of the COVID‐19 outbreak, people have experienced elevated psychological distress in their everyday lives (e.g., Akbari, Seydavi, et al., 2021; Brailovskaia et al., 2021; Cao et al., 2020; Chen et al., 2021; Duong, 2021; Kontoangelos et al., 2020; Lee, 2020; Mansueto et al., 2021; Shevlin et al., 2020) including depression and anxiety (Huang & Zhao, 2020; Oh et al., 2021; Wierenga et al., in press), obsessive–compulsive symptoms (Abba‐Aji et al., 2020; Seçer & Ulaş, 2020; Wheaton et al., 2021), substance use (Akbari et al., 2020; Czeisler et al., 2020), post‐traumatic stress symptoms (Akbari, Hosseini, et al., 2021; Johnson et al., 2020; Liu et al., 2020), suicidal ideation (Czeisler et al., 2020), health anxiety (Akbari, Spada, et al., 2021; Özdin & Özdin, 2020), psychological distress (Wang et al., 2020; Wu et al., 2020), hopelessness (Hacimusalar et al., 2020), loneliness and fatigue (Hou et al., 2020; Mansueto et al., 2021), loss and grief (Wallace et al., 2020; Zhai & Du, 2020), sleep problems (Duong, 2021; Jahrami et al., 2021) and reduced life satisfaction (Duong, 2021).
1.1. COVID‐19 psychological distress measures
In a short space of time during the initial phase of the pandemic, different measures were developed by researchers for assessing fear, anxiety and stress related to COVID‐19. These early measures include the Fear of COVID‐19 Scale (FCV‐19S; Ahorsu et al., 2020), the Coronavirus Anxiety Scale (CAS; Lee, 2020), the COVID Stress Scales (CSS; Taylor et al., 2020), the Coronavirus Stress Scale (Arslan et al., 2020) and the Perceived Coronavirus Threat Questionnaire (PCTQ; Conway et al., 2020) (for a recent review, see Voitsidis et al., 2021). The common feature of these measures is the focus on the experience of specific psychological states linked to the COVID‐19 pandemic, be it anxiety, stress, a phobic response or perceived threat.
1.2. The COVID‐19 Anxiety Syndrome Scale
In early 2020, Nikčević and Spada (2020) developed a measure to specifically assess maladaptive cognitive‐behavioural coping in the form of avoidance, checking, worrying and threat monitoring in response to fear or threat of COVID‐19. The researchers labelled this constellation of coping responses the COVID‐19 anxiety syndrome and developed a measure to assess this construct: the COVID‐19 Anxiety Syndrome Scale (C‐19ASS), with two components of perseveration (checking, worrying and monitoring because of the fear or threat of COVID‐19), and avoidance (of public spaces, transport and contact with objects because of the fear or threat of COVID‐19).
This construct is conceptually consistent with the Self‐Regulatory Executive Function (S‐REF) model of psychopathology (Wells, 2011), which maintains that distress outcomes such as anxiety arise through maladaptive cognitive, behavioural and attentional forms of coping. These forms of coping, taken together, are termed the ‘cognitive‐attentional syndrome’ (CAS) and are constituted by an unwavering focus on threat, worry, rumination, checking, though suppression and avoidance. The activation of the CAS limits the possibility of readily existing distressing states and also contributes to the incubation of more threat‐related cognitive and affective triggers.
The C19‐ASS was developed using community samples of US residents, and in the original validation of the scale, it was shown that the C‐19ASS predicts COVID‐19 anxiety above and beyond risk status, perceived COVID‐19 threat and the Big Five personality traits. Furthermore, it also predicted work and social adjustment above and beyond risk status, age, perceived COVID‐19 threat and the Big Five personality traits. This brief measure with two factors has shown good psychometric properties, including reliability and concurrent validity.
Albery et al. (2021) have provided further evidence for the validation of the C‐19ASS in a UK community sample. They found that the COVID‐19 anxiety syndrome correlates with generalized anxiety and depression. Also, the perseveration dimension of the C‐19ASS can predict generalized anxiety and depression while controlling for age, gender, the Big Five personality traits (conscientiousness and openness), health anxiety and COVID‐19 anxiety. Furthermore, the researchers found associations between the total C‐19ASS and the avoidance and perseveration dimensions with an attentional bias towards COVID‐19‐related stimuli. Nikčević et al. (2021) also showed, in a sample of US residents, that the C19‐ASS predicts generalized anxiety and depression after controlling age, gender, employment status, risk status, the Big Five personality traits, health anxiety and COVID‐19 anxiety. The findings of Nikčević et al. (2021) established the critical importance of studying the Big Five personality traits in relation to depressive and anxiety symptomology during the pandemic. Although the exact mechanism by which personality traits are associated with the psychopathology remains unclear, the researchers observed that the C19‐ASS significantly mediated this path in a Western sample. Thus, additional research in understudied populations, such as Iranians, could provide a broader perspective on the role of C19‐ASS in the association between personality traits and depressive and anxiety symptomology during the COVID‐19 pandemic.
1.3. Aim of the current study
Developing robust measures designed to assess psychological distress during the COVID‐19 pandemic may expand the limited existing literature and our understanding of the psychological impact of COVID‐19, in particular in the long term. Given that there is no validation study for the C‐19ASS to date in non‐Western samples, the current study aimed to assess the psychometric properties of the C‐19ASS in a sample of the general Iranian community through a national survey.
In line with the parent study, we utilized exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) to determine the factor structure of this measure. Internal consistency, construct validity, concurrent validity and incremental validity were all evaluated. To extend the validation of the original scale by testing divergent validity, we examined whether C19‐ASS can be differentiated from generalized anxiety disorder (GAD). We further aimed to assess the association of the C‐19ASS with a series of demographic features and COVID‐19‐related background factors. Finally, using path analysis, we aimed to ascertain whether C19‐ASS could mediate the relationship between the Big Five personality traits and psychopathology (health anxiety, generalized anxiety, depression and COVID‐19 anxiety).
2. METHOD
2.1. Participants
The present research was an online study among the general population in Iran. The online survey was completed within 3 months (the end of the fourth and beginning of the fifth waves of the pandemic) by 1429 participants (mean age = 35.83 ± 12.89). Slightly more than half of the sample was female (52.1%; mean age = 34.72, ±12.88), and the rest were males (47.9%; mean age = 37.04, ±12.81).
All participants were in the age range of 18–65 years and had consented to participate in the study. The participants' demographic characteristics and other provided information are presented in Table 1, and, as seen, 50.2% were married, and slightly more than half of the samples (57.2%) were educated at college level. In terms of occupational status, 58.6% reported being employed. The majority of our sample (73.4%) did not consider themselves at high risk if they were to contract COVID‐19. The majority (87.2%) had not been diagnosed with a mental health disorder based on their self‐report. Also, about one third (23.2%) reported having lost someone close due to COVID‐19.
TABLE 1.
Demographic features and additional data of the sample (n = 1,429)
| N | % | ||
|---|---|---|---|
| Gender | Female | 745 | 52.1 |
| Male | 684 | 47.9 | |
| Marital status | Single | 717 | 50.2 |
| Married | 712 | 49.8 | |
| Educational level | Academic | 818 | 57.2 |
| Non‐academic | 611 | 42.8 | |
| Occupational status | Employed | 838 | 58.6 |
| Unemployed | 591 | 41.4 | |
| Mental status (been diagnosed with a mental health disorder) | Yes | 107 | 7.5 |
| No | 1,246 | 87.2 | |
| Prefer not to disclose | 76 | 5.3 | |
| Risk status | Yes | 380 | 26.6 |
| No | 1,049 | 73.4 | |
| Close death | Yes | 332 | 23.2 |
| No | 1,097 | 76.8 |
2.2. Measures
In the present study, the Persian forms of the following questionnaires were used.
2.2.1. Socio‐demographic and COVID‐19‐related variables
Participants were asked to provide a series of socio‐demographic details including age, gender, educational level (academic/non‐academic), marital status (single/married), employment status (employed/unemployed/other) and history of diagnosis of a mental health disorder (yes/no/does not wish to disclose). Moreover, participants were asked information relating to COVID‐19, including whether they considered themselves to be at high risk of having a more negative response to the infection and the reason (being of older age/ethnicity/pregnancy/health problem/disability/other) and whether they had lost someone close due to COVID‐19.
2.2.2. COVID‐19 Anxiety Syndrome Scale
This self‐report scale comprises nine items yielded on a two‐factor structure model, assessing features of the anxiety syndrome related to COVID‐19. Two factors of the C‐19ASS include (1) perseveration (six items), with items concerning checking (e.g., “I have checked myself for symptoms of coronavirus”), worrying (e.g., “I have imagined what could happen to my family members if they contracted coronavirus”) and threat monitoring (e.g., “I have been paying close attention to others displaying possible symptoms of coronavirus”), and (2) avoidance (three items) (e.g., “I have avoided touching things in public spaces because of the fear of contracting coronavirus”). Items are rated on a 5‐point Likert scale from 0 (Not at all) to 4 (Nearly every day over the last 2 weeks) with a total score ranging from 0 to 36. Higher scores indicate higher levels of COVID‐19 anxiety syndrome. Nikčević and Spada (2020) found the C‐19ASS to be a reliable and valid measure of the COVID‐19 anxiety syndrome.
2.2.3. Work and Social Adjustment Scale
An adjusted version for COVID‐19 was used in the present study. This self‐report scale comprises five items assessing the functional impairment of a particular problem, with the following preamble: “Thinking about the COVID‐19 pandemic and the way it may have impacted your mental health, please look at each statement below and rate the extent to which the following items apply to you.” Responses were recorded on a 9‐point Likert scale from 0 (not at all) to 8 (very severely), the WSAS scores range from 0 to 40, where higher scores indicate higher social and functional impairment levels. Mundt et al. (2002) reported good internal consistency (Cronbach's alphas = 0.70–0.94), test–retest reliability and convergent validity for the original scale. The Persian version of the WSAS has also shown good psychometric properties (Mohammadi, 2011).
2.2.4. Coronavirus Anxiety Scale
This self‐report scale comprises five items, assessing thoughts and physiological symptoms related to COVID‐19 during the last 2 weeks. Items are rated on a 5‐point Likert scale from 0 (not at all) to 4 (nearly every day over the last 2 weeks). The CAS presents a total score with a range of 0–20, and higher scores indicate higher levels of COVID‐19‐related anxiety; the CAS is a reliable and valid scale (Lee, 2020). The Persian version of the CAS has also shown good reliability, convergent validity and divergent validity (Mohammadpour et al., 2020).
2.2.5. Patient Health Questionnaire 9
Based on DSM‐IV criteria, this self‐report scale comprises nine items, assessing, screening and monitoring depression severity during the past 2 weeks. Items are rated on a 4‐point Likert scale from 0 (not at all) to 3 (nearly every day), with a total score with a range of 0–27. Higher scores indicate higher levels of depression. Scores ranges 15–19 are considered moderately severe, and 20–27 are considered severe depression. Kroenke et al. (2001) found the Patient Health Questionnaire 9 (PHQ‐9) as a reliable and valid measure of depression severity. The Persian version of the PHQ‐9 has also shown good psychometric properties (including internal consistency, test–retest reliability, construct, convergent, discriminant and criterion validity) in validation studies (Dadfar et al., 2018; Farrahi et al., 2021; Rafiey et al., 2018).
2.2.6. Generalized anxiety disorder 7
This widely used self‐report scale comprises seven items, assessing and screening GAD and its severity during the past 2 weeks based on DSM‐IV criteria. Items are rated on a 4‐point Likert scale from 0 (not at all) to 3 (nearly every day), with a total score ranging of 0–21. Higher scores indicate higher levels of generalized anxiety. Scores ranges 10–14 are considered moderate, and 15–21 are considered severe generalized anxiety levels. Spitzer et al. (2001) reported good reliability, criterion, construct, factorial, and procedural validity for this scale. The Persian version of the GAD‐7 (Spitzer et al., 2006) has also shown good psychometric properties (including internal consistency, test–retest reliability and convergent validity) in validation studies (Nainian et al., 2011; Omani‐Samani et al., 2018).
2.2.7. Whiteley index
This self‐report scale comprises seven items, screening somatization and hypochondriasis. Items answered on a dichotomous scale (0 = no, 1 = yes). The Whiteley index 7 (WI‐7) (Fink et al., 1999) presents a total score with a range of 0–7. High scores indicate higher levels of worrying about illness. Fink et al. (2001) found the WI‐7 as a reliable and valid measure. There is no validation study for Persian WI‐7 yet, so we had conducted a pilot study. First, the English WI‐7 was translated into Persian by two Persian speaker authors and a bilingual psychologist. After this, the equivalence of the two versions was evaluated. In the next step, the preliminary version was provided to a group of volunteers. Notably, we have inserted a Likert scale for each item to ensure the understandability and fluency of the translation. Eighty‐eight participants completed this version (female = 67%; mean age = 22.83, ±6.63 years) from the general population. This process resulted in some edits. Finally, the final Persian WI‐7 was obtained. The pilot study indicated a Cronbach's alpha of 0.72.
2.2.8. Big Five Inventory‐10
This self‐report scale comprises five two‐item dimensions, assessing the Big Five personality traits, including neuroticism, extroversion, agreeableness, openness and conscientiousness. Ten items are rated on a 5‐point Likert scale from 1 (disagree strongly) to 5 (agree strongly). The Big Five Inventory‐10 (BFI‐10) presents a score with a range of 2–10 for each dimension. Higher scores indicate greater levels of each five traits. Rammstedt and John (2007) reported significant levels of reliability and validity for the original scale. The Persian version of the BFI‐10 has also shown acceptable reliability and validity (Kakabaraee et al., 2011; Mohammad Zadeh & Najafi, 2010).
2.3. Procedure
In the first instance, for the validation of the C‐19ASS, permission was obtained from the developers. Two Iranian authors translated the original version. Next, a back translation process was done by another Iranian author who was fluent in English. Comparison between two English forms showed no inconsistencies between the two versions. Four clinical psychologists who were Persian speakers were requested to evaluate the content validity of the translated version. They confirmed the comprehensibility and fluency of C‐19ASS items. Following this process, the preliminary evaluation of the first Persian version was conducted through a pilot study. In this pilot study, 81 participants (female = 59.4%; mean age = 29.4, ±4.23) from the general population completed this scale and rated the understandability of each item in an attached Likert scale. The pilot study did not result in any changes in items and showed an excellent Cronbach's alpha score (0.93). Eventually, the final Persian C‐19ASS was obtained.
The current study was conducted during the COVID‐19 pandemic outbreak in Iran. First, all selected questionnaires and demographic features, and other information required for the present study were provided in an integrated online package. The study was promoted on various social networks. After signing the electronic consent form, the volunteers were directed to the front page of the study. Participants had the right to discontinue participation at any time. This study was conducted under the 1989 Helsinki Declaration. No incentives were given.
2.4. Data analysis
Data were analysed using version 26 of both SPSS (IBM SPSS Statistics) and Amos in the present study. EFA and CFA were used to examine the factor structure of the Persian version of the C‐19ASS. We divided our primary sample into two subsamples via a random process, such that one subsample with an allocation of 714 participants was considered for the EFA, and the second one with an allocation of 715 participants was considered for the CFA. In order to extract the number of Persian C‐19ASS's factors, we used parallel analysis (Horn, 1965). CFA using maximum likelihood estimation was conducted. Following this, based on Hu and Bentler's suggestions (1999), several fit indices were evaluated, such as comparative fit index (CFI; good fit ≥ 0.90), root mean square error of approximation (RMSEA; good fit ≤ 0.08) and standardized root mean square residual (SRMR; good fit ≤ 0.08); values close to these cutoffs were considered acceptable fit. Also, the reliability was assessed with the primary sample (n = 1429) via internal consistency (Cronbach's alpha, average variance extracted [AVE], composite reliability, maximal reliability), and the validity analysis included construct validity, concurrent validity, incremental validity, convergent and divergent validity. A path analysis was also conducted to determine whether the C19‐ASS mediated the association between the Big Five personality traits and psychopathology (GAD, CAS, PHQ and WI).
3. RESULTS
3.1. EFA for the Persian C19‐ASS
The first split‐half sample (n = 714, 50.4% female; mean age = 35.93, ±12.97) was utilized for the EFA. The Kaiser–Meyer–Olkin (KMO) and Bartlett's test of sphericity (KMO = 0.854, p < 0.001) indices for the Persian C19‐ASS revealed that the correlations between C19‐ASS items were large, and therefore factor analysis was feasible. Before factor analysis, the random Eigenvalues were compared with the observed data using a parallel analysis (Horn, 1965). The first two random Eigenvalues (i.e., 1.40 and 1.01) were below the first two observed Eigenvalues (i.e., 3.65 and 1.19), suggesting two factors.
Therefore, the EFA was conducted with two factors resulting in a solution comparable to the parent study (Nikčević & Spada, 2020). Table 2 presents the standardized factor loadings: Factor 1, perseveration (P); Factor 2, avoidance (A). In addition, the factor correlation between avoidance and perseveration (r = 0.34) indicated only moderate shared variances and acceptable separability. There were no significant cross‐loadings. Table 2 also presents the item means, standard deviations, skewness and kurtosis, as well as item‐total correlations.
TABLE 2.
Persian C19‐ASS standardized factor loadings and item descriptive statistics
| Exploratory factor analysis | Descriptive statistics | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| No. | Perseveration | Avoidance | h 2 | I‐T | I‐Ts | Skewness | Kurtosis | M | SD |
| ITEM 2 | 0.614 | 0.154 | 0.534 | 0.537 | 0.564 | 0.841 | −0.271 | 1.44 | 1.21 |
| ITEM 4 | 0.413 | 0.351 | 0.606 | 0.518 | 0.488 | −0.332 | −1.491 | 1.31 | 1.26 |
| ITEM 6 | 0.440 | 0.324 | 0.602 | 0.525 | 0.496 | 0.761 | −0.559 | 1.37 | 1.32 |
| ITEM 7 | 0.886 | 0.000 | 0.251 | 0.602 | 0.696 | 0.556 | −0.696 | 1.58 | 1.28 |
| ITEM 8 | 0.673 | 0.160 | 0.448 | 0.585 | 0.608 | 0.417 | −0.944 | 1.76 | 1.33 |
| ITEM 9 | 0.659 | 0.094 | 0.514 | 0.537 | 0.585 | 0.186 | −1.164 | 1.98 | 1.34 |
| ITEM 1 | 0.008 | 0.389 | 0.846 | 0.244 | 0.279 | 0.715 | −0.886 | 1.42 | 1.45 |
| ITEM 3 | 0.000 | 0.804 | 0.354 | 0.467 | 0.485 | 0.687 | −0.383 | 1.85 | 1.45 |
| ITEM 5 | 0.222 | 0.593 | 0.508 | 0.501 | 0.405 | 0.182 | −1.321 | 2.46 | 1.55 |
Abbreviations: h 2, communality; I‐T, item–total correlations; I‐Ts, item‐total correlations between each item and its subscale; M, mean; SD, standard deviation.
3.2. CFA for the Persian C19‐ASS
The second split‐half sample was used for the CFA (n = 715, 53.8% female, mean age = 35.73, ±12.83). The alternative model specified one latent variable that included all nine items as indicators. Then, the first split‐half sample EFA found the two‐factor model, comparable to the parent study (Nikčević & Spada, 2020), was evaluated. No cross‐loadings or correlated errors were specified. Also, there were no suggested modification indices to increase the model fit. Table 3 shows the model fit indices. The two‐factor model (χ 2 = 130.363, df = 26, χ 2/df = 5.014, SRMR = 0.0464, RMSEA = 0.070, GFI = 0.960, CFI = 0.956, normed fit index [NFI] = 0.949, Tucker–Lewis index [TLI] = 0.952, incremental fit index [IFI] = 0.961) had the best model fit. Likelihood ratio tests supported that the two‐factor model outperformed the one‐factor model (χ 2 = 63.288, df = 1, p < 0.001). It also was supported by expected cross‐validation index (ECVI), which was higher for the one‐factor solution model (ECVI = 0.312 [0.257, 0.377]) comparing to the two‐factor model solution model (ECVI = 0.244 [0.198, 0.301]). A model that has a lower value and is closer to zero fits the data better. Figure 1 shows the standardized factor loadings for the two‐factor model. Also, factor correlations between perseveration and avoidance (r = 0.39) indicated low shared variances and acceptable separability.
TABLE 3.
Model fit indices of confirmatory factor analysis for the Persian C19‐ASS
| χ 2 | DF | χ 2/df | SRMR | RMSEA | GFI | CFI | NFI | TLI | IFI | |
|---|---|---|---|---|---|---|---|---|---|---|
| One‐factor solution | 193.651 | 27 | 7.172 | 0.0529 | 0.092 | 0.941 | 0.915 | 0.903 | 0.887 | 0.916 |
| Two‐factor solution | 130.363 | 26 | 5.014 | 0.0464 | 0.070 | 0.960 | 0.956 | 0.949 | 0.952 | 0.961 |
Note. All the models were estimated with zero cross‐loadings and correlated errors.
Abbreviations: CFI, comparative fit index; GFI, goodness of fit; IFI, incremental fit index; NFI, normed fit index; RMSEA, root mean square error of approximation; SRMR, standardized root mean square residual; TLI, Tucker–Lewis index; χ 2, chi‐square index.
FIGURE 1.
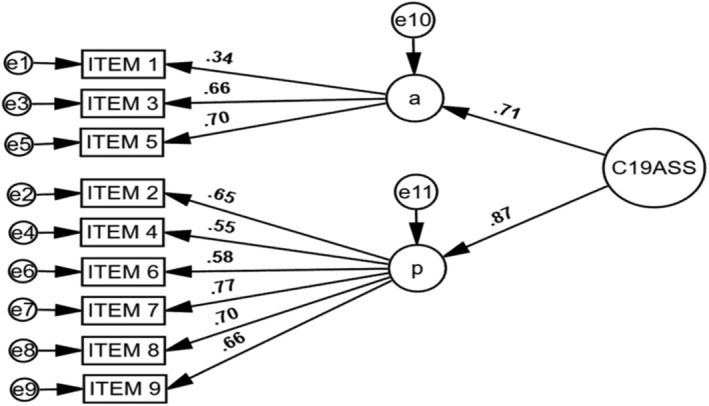
The two‐factor solution model, confirmatory factor analysis. A, avoidance subscale; P, perseveration subscale
3.3. Persian C19‐ASS measurement invariance model
In order to ensure that Persian C19‐ASS scores can be used to compare COVID‐19 anxiety syndrome across genders, a measurement invariance model with zero cross‐loadings or correlated errors was examined. We found evidence for configural invariance—where the items load on the same factors across genders—supported by good fit indices (χ 2 = 204.456, df = 52, χ 2/df = 3.932, RMSEA = 0.051, SRMR = 0.050, GFI = 0.960, CFI = 0.947). Moreover, we found evidence for metric invariance—where the factor loadings are constrained to be equal across genders—supported by good fit indices (χ 2 = 214.693, df = 61, χ 2/df = 3.520, RMSEA = 0.051, SRMR = 0.054, GFI = 0.966, CFI = 0.951). A chi‐square difference test between the unconstrained and constrained factor loadings was nonsignificant (χ 2 = 10.237, df = 9, p value = 0.35), indicating that each item contributes to the latent construct comparable extent in both genders. In contrast, we found partial evidence of scalar invariance—where item intercepts were constrained to be equal across genders. The chi‐square difference test between unconstrained and constrained item intercepts was significant (χ 2 = 56.660, df = 18, p value = 0.01). Modification indices indicated that three items (3, 4 and 6) were variant across genders. Item 3 had a higher intercept among females, while Items 4 and 6 had a higher intercept among males. Once Items 3, 4 and 6 become unconstrained, the differences between the two models become non‐significant (χ 2 = 23.293, df = 15, p value = 0.078), indicating mean differences in the latent construct could not capture all mean differences in the shared variance of the items. Thus, correlations between Persian C19‐ASS scores and other constructs are comparable across genders, though mean differences should be interpreted cautiously.
3.4. Reliability of the Persian C19‐ASS
The entire sample was used for reliability and validity analyses (n = 1429). Cronbach's alpha showed that internal consistency for the Persian C19‐ASS total score was 0.817. The subscale score reliabilities were 0.821 and 0.703, the perseveration and avoidance, respectively. It was indicating satisfactory reliability for the total scale and the perseveration subscale. Further, the internal consistencies from removing one item were never higher than those computed for the perseveration subscale score (i.e., range = 0.768–0.809).
In conclusion, each item from the perseveration subscale contributes to the scale scores with reliable variance and should be retained. However, it was different for the total scale and the avoidance subscale; removing one item suggested that if item number 1 becomes deleted, the Cronbach's alpha for the total scale increases from 0.817 to 0.830 and that for the avoidance subscale increases from 0.703 to 0.751. It is suggesting that removing item number 1 could enhance the reliability of Persian C19‐ASS.
To test model‐based indices of reliability, a two‐factor CFA model was conducted with the entire sample. The AVE for the Persian C19‐ASS was large at 0.630, indicating that about 63% of the item variances contributed to the two latent constructs. The composite reliability of the model was extensive at 0.771, indicating that the two factors explained over 70% of the C19‐ASS total score variance. Additionally, the maximum reliability (MaxR [H]) was estimated, which was 0.804, indicating that Persian C19‐ASS has low measurement errors; compared to Cronbach's alpha, it is confirmed to be at its optimal level of reliability.
3.5. Convergent and divergent validity of the Persian C19‐ASS
Table 4 presents bivariate correlations assessing construct validity of the Persian C19‐ASS scores with the studied variables. As seen, (1) C19‐ASS‐P and the total C19‐ASS are negatively and significantly associated with extraversion and agreeableness, positively with neuroticism and nonsignificantly with openness and conscientiousness. The C19‐ASS‐A was only associated with extraversion. C19‐ASS and its subscales are significantly and positively associated with depressive symptoms, generalized anxiety symptoms, work, and social adjustment, health anxiety, and COVID‐19 anxiety.
TABLE 4.
Means, standard deviations, ranges and intercorrelations of variables: Construct validity for Persian C19‐ASS
|
|
SD | Range | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. BFI‐E | 6.2 | 2.1 | 2–10 | (0.90) | |||||||||||||
| 2. BFI‐A | 6.4 | 1.8 | 2–10 | 0.22** | (0.69) | ||||||||||||
| 3. BFI‐C | 6.9 | 2.0 | 2–10 | 0.20** | 0.16** | (0.88) | |||||||||||
| 4. BFI‐N | 6.1 | 2.4 | 2–10 | −0.16** | −0.26** | −0.13** | (0.79) | ||||||||||
| 5. BFI‐O | 7.4 | 1.9 | 2–10 | 0.08* | −0.04 | 0.05 | 0.02 | (0.86) | |||||||||
| 6. PHQ | 8.5 | 7.1 | 0–27 | −0.26** | −0.20** | −0.32** | 0.39** | 0.05 | (0.96) | ||||||||
| 7. WSAS | 14.3 | 9.7 | 0–40 | −0.12** | −0.23** | −0.14** | 0.21** | −0.03 | 0.41** | (0.86) | |||||||
| 8. GAD | 5.6 | 5.3 | 0–21 | −0.18** | −0.27** | −0.19** | 0.47** | 0.06 | 0.82** | 0.38** | (0.94) | ||||||
| 9. WI | 13.8 | 5.6 | 7–35 | −0.14** | −0.26** | −.22** | 0.32** | 0.02 | 0.47** | 0.27** | 0.49** | (0.79) | |||||
| 10. CAS | 1.0 | 1.7 | 0–8 | 0.04 | −0.08* | 0.04 | 0.17** | 0.02 | 0.21** | 0.29** | 0.26** | 0.20** | (0.69) | ||||
| 11. C19‐ASS‐P | 9.6 | 5.7 | 0–24 | −0.08* | −0.14** | 0.01 | 0.14** | 0.06 | 0.19** | 0.32** | 0.23** | 0.30** | 0.33** | (0.82) | |||
| 12. C19‐ASS‐A | 5.7 | 3.2 | 0–12 | −0.12** | −0.07 | 0.03 | 0.02 | 0.03 | 0.09** | 0.26** | 0.06* | 0.12** | 0.18** | 0.48** | (0.70) | ||
| 13. C‐19ASS | 15.4 | 7.8 | 0–36 | −0.11** | −0.13** | 0.02 | 0.11** | 0.04 | 0.18** | 0.34** | 0.20** | 0.27** | 0.31** | 0.94** | 0.77** | (0.81) | |
| Age | 35.8 | 12.8 | 18–65 | 0.29** | 0.10** | 0.08** | −0.02 | −0.06 | −0.02 | 0.04 | −0.01 | 0.04 | 0.04 | 0.06 | −0.01 | 0.04 | |
| Gender | — | — | — | 0.12** | 0.09** | 0.03 | 0.06* | −0.02 | −0.03 | −0.07** | −0.02 | −0.08** | 0.05 | −0.08** | 0.05* | −0.04 | |
| Close death | — | — | — | −0.06 | −0.03 | 0.03 | 0.04 | −0.05 | 0.09** | 0.11** | 0.09** | 0.07 | 0.04 | 0.12** | 0.04 | 0.10** |
Note: Internal consistency coefficients are in the parentheses on the diagonal.
Abbreviations: BFI‐10‐Agr, Big Five Inventory‐10‐Agreeableness; BFI‐10‐Com, Big Five Inventory‐10‐Conscientiousness; BFI‐10‐Ext, Big Five Inventory‐10‐Extraversion; BFI‐10‐Neu, Big Five Inventory‐10‐Neuroticism; BFI‐10‐Ope, Big Five Inventory‐10‐Openness; C‐19ASS, COVID‐19 Anxiety Syndrome Scale; C‐19ASS‐A, COVID‐19 Anxiety Syndrome Scale‐Avoidance; C‐19ASS‐P, COVID‐19 Anxiety Syndrome Scale‐Perseveration; CAS, Coronavirus Anxiety Scale; close death, close death due to COVID‐19; GAD, generalized anxiety disorder; WI, Whiteley Index; WSAS, Work and Social Adjustment Scale.
p < 0.05.
p < 0.01.
Moreover, in a separate analysis, age, education level (academic/non‐academic), marital status (single/married) and job status (employed/unemployed) were not correlated with C19‐ASS and either of its subscales. Gender was only associated with C19‐ASS subscale's perseveration (r = −0.08, p < 0.01) and avoidance (r = −0.07, p < 0.05), but not the full scale. Besides, (1) having or not having lost someone close due to COVID‐19 and (2) having or not having psychiatric history were only associated with the full scale (1, r = 0.08, p < 0.01; 2, r = 0.08, p ≤ 0.05), and perseveration subscale (1, r = 0.12, p < 0.01; 2, r = 0.08, p ≤ 0.01). Moreover, high‐ or low‐risk status for infection was significantly and positively associated with the total scale (r = 0.19, p ≤ 0.01), perseveration (r = 0.120, p ≤ 0.01) and avoidance (r = 0.084, p ≤ 0.05) subscales.
To further assess divergent validity, a principal component analysis (PCA) by Promax rotation with Kiser normalization (Kappa = 4) and the total sample investigated whether the Persian C19‐ASS could be distinguished from GAD‐7. A three‐component PCA solution was extracted to assess whether the C19‐ASS items loaded on two components distinct from GAD. The PCA comprised the C19‐ASS items and GAD‐7 items. The loadings revealed GAD‐7 items were tightly loaded together on a component (eigenvalue 5.25), and the C19‐ASS items loaded on two components of perseveration (eigenvalue 3.27) and avoidance (1.12). The standardized loadings are presented in Appendix A. The component correlations between C19‐ASS and the GAD‐7 ranged from 0.07 (avoidance) to 0.21 (perseveration), implying that the C19‐ASS can be differentiated from GAD, supported by nonsignificant cross‐loadings between the C19‐ASS items and the GAD‐7 items.
3.6. Incremental validity of the Persian C19‐ASS
Before analysing data, assumptions were tested. The multicollinearity statistics were within acceptable limits for both models (Model 1, tolerance range: 0.73–0.99; variance inflation factor [VIF] range: 1.00–1.36; Model 2, tolerance range: 0.70–0.97; VIF range: 1.00–1.89). Using the Mahalanobis distance scores, 38 multivariate outliers were identified for both models and removed from the analysis. The residual analysis (including Loess line fitting and Q–Q plots), scatterplots and statistic coefficients demonstrated that the normality, linearity and homoscedasticity assumptions were met. We used hierarchical multiple regression to examine whether C19‐ASS can predict CAS and WSAS beyond variables studied; however, only significant predictors are retained in the model.
Table 5 represents the results for predicting CAS scores from marital, educational status (Step 1), conscientiousness and neuroticism (Step 2), GAD (Step 3) and C19‐ASS‐Perseveration subscale (Step 4). The CAS scores were significantly predicted on Step 1 by marital and educational status together, F(2, 1340) = 6.335, p < 0.001. Also, a significant regression was obtained by including the conscientiousness and neuroticism scores (Step 2), F(4, 1338) = 15.746, p < 0.001, explaining 4.2% of variance in CAS scores, ∆F(2, 1338) = 24.931, p < 0.001. Moreover, the inclusion of GAD‐7 (Step 3) also resulted in a significant equation, F(5, 1337) = 33.331, p < 0.001, accounting for a further 6.6% of variance explained in CAS scores, ∆F(1, 1337) = 99.056, p < 0.001. Finally, the addition of the C19‐ASS‐Perseveration subscale in (Step 4) resulted in a significant equation, F(6, 1336) = 48.744, p < 0.001, and accounting for an extra 6.9% of variance in CAS scores, ∆F(1, 1336) = 111.977, p < 0.001. This final model explained that marital and educational status, conscientiousness, neuroticism, GAD, and C‐19ASS‐Perseveration (all ps < 0.05) significantly predicted variability in CAS scores, accounting for a total of 17.6% of the variation in CAS scores (see Table 5). In this model, C‐19ASS‐Perseveration predicted the variance in CAS score above and beyond marital and educational status, conscientiousness, neuroticism and GAD‐7.
TABLE 5.
Hierarchical regression statistics predicting Coronavirus Anxiety Scale (CAS) scores: Incremental validity
| Predictor | β | T | sr 2 | R | R 2 | Adjusted R 2 | ∆R 2 |
|---|---|---|---|---|---|---|---|
| Step 1 | 0.097 | 0.009 | 0.008 | 0.009** | |||
| Marital status | 0.08 | 3.10** | 0.0071 | ||||
| Educational status | −0.04 | −1.76 | 0.0023 | ||||
| Step 2 | 0.212 | 0.045 | 0.042 | 0.036** | |||
| Marital status | 0.08 | 3.11** | 0.0069 | ||||
| Educational status | −0.06 | −2.42* | 0.0042 | ||||
| BFI‐C | 0.04 | 1.67 | 0.0020 | ||||
| BFI‐N | 0.19 | 7.01** | 0.0350 | ||||
| Step 3 | 0.333 | 0.111 | 0.108 | 0.066** | |||
| Marital status | 0.10 | 3.83** | 0.0098 | ||||
| Educational status | −0.07 | −2.91 | 0.0056 | ||||
| BFI‐C | 0.08 | 3.33** | 0.0074 | ||||
| BFI‐N | 0.05 | 1.74 | 0.0020 | ||||
| GAD‐7 | 0.30 | 9.95** | 0.0660 | ||||
| Step 4 | 0.424 | 0.180 | 0.176 | 0.069** | |||
| Marital status | 0.11 | 4.64** | 0.0132 | ||||
| Educational status | −0.06 | −2.56* | 0.0041 | ||||
| BFI‐C | 0.04 | 2.73* | 0.0046 | ||||
| BFI‐N | 0.02 | 1.56 | 0.0015 | ||||
| GAD‐7 | 0.23 | 7.79** | 0.0372 | ||||
| C‐19ASS‐P | 0.27 | 10.5** | 0.0686 |
Note: Marital status (0 = single, 1 = married); educational status (0 = academic, non‐academic = 1).
Abbreviations: BFI‐C, Big Five Inventory‐10‐Conscientiousness; BFI‐N, Big Five Inventory‐10‐Neuroticism; C‐19ASS‐P, COVID‐19 Anxiety Syndrome Scale‐Perseveration.
p < 0.05.
p < 0.01.
In addition to above, Table 6 represents the results for predicting WSAS scores from gender (1 = male; 0 = female), and COVID‐19 death of a person close (1 = yes, 0 = no) (Step 1), BFI‐C and BFI‐N (Step 2), GAD‐7, PHQ, and CAS (Step 3), and Perseveration subscale (Step 4). The results indicated that gender and COVID‐19 death of a close person together significantly predicted WSAS scores, F(2, 1426) = 19.735, p < 0.001. The addition of the BFI‐C and BFI‐O subscales (Step 2) resulted in a significant regression equation, F(4, 1424) = 17.962, p < 0.001, explaining an extra 2.1% of the variation in WSAS scores, ∆F(2, 1424) = 15.781, p < 0.001. The inclusion of GAD‐7, PHQ and CAS (Step 3) produced a significant equation, F(7, 1421) = 64.735, p < 0.001, accounting for an additional 9.4% of the variation explained in WSAS scores, ∆F(3, 1421) = 121.042, p < 0.001. Finally, the addition C‐19ASS‐P subscale (Step 4) resulted in a significant equation, F(8, 1420) = 66.722, p < 0.001, and accounting for an additional 3.1% of the variation in WSAS scores, ∆F(1, 1420) = 61.378, p < 0.001. This final model revealed that gender, COVID‐19 death of a person close, conscientiousness, openness, GAD‐7, PHQ, CAS and C‐19ASS‐P subscale (all ps < 0.05), predicted variability in WSAS scores and accounted for 28.8% of the variation in WSAS scores (see Table 6). In this model, the C‐19ASS‐P subscale predicted WSAS scores above and beyond gender, COVID‐19 death of a person close, conscientiousness, openness, GAD‐7 and CAS except for PHQ. Additionally, it is imperative to remark that GAD‐7 was no longer a significant predictor of WSAS following the addition of C19‐ASS‐P.
TABLE 6.
Hierarchical regression statistics predicting functional impairment (WSAS) scores: Incremental validity
| Predictor | β | t | sr 2 | R | R 2 | Adjusted R 2 | ∆R 2 |
|---|---|---|---|---|---|---|---|
| Step 1 | 0.164 | 0.02 | 0.026 | 0.027** | |||
| Gender | −0.06 | −2.45* | 0.0041 | ||||
| COVID‐19 close death | 0.14 | 5.52** | 0.0208 | ||||
| Step 2 | 0.219 | 0.048 | 0.045 | 0.021** | |||
| Gender | −0.06 | −2.27** | 0.0035 | ||||
| COVID‐19 close death | 0.14 | 5.67** | 0.0215 | ||||
| BFI‐C | −0.14 | −5.46** | 0.0200 | ||||
| BFI‐O | −0.02 | −.997 | 0.0007 | ||||
| Step 3 | 0.492 | 0.242 | 0.238 | 0.194** | |||
| Gender | −0.06 | −2.83* | 0.0043 | ||||
| COVID‐19 close death | 0.11 | 5.08** | 0.0138 | ||||
| BFI‐C | −0.04 | −1.69** | 0.0015 | ||||
| BFI‐O | −0.06 | −2.53** | 0.0034 | ||||
| GAD‐7 | 0.08 | 2.07* | 0.0023 | ||||
| PHQ | 0.27 | 6.44** | 0.0222 | ||||
| CAS | 0.21 | 8.99** | 0.0432 | ||||
| Step 4 | 0.523 | 0.273 | 0.269 | 0.031** | |||
| Gender | −0.04 | −2.11* | 0.0023 | ||||
| COVID‐19 close death | 0.10 | 4.37** | 0.0098 | ||||
| BFI‐C | −0.05 | −2.03* | 0.0021 | ||||
| BFI‐O | −0.07 | −3.01** | 0.0047 | ||||
| GAD‐7 | 0.05 | 1.40 | 0.0010 | ||||
| PHQ | 0.27 | 6.51** | 0.0217 | ||||
| CAS | 0.16 | 6.50** | 0.0217 | ||||
| C19‐ASS‐P | 0.19 | 7.83** | 0.0314 |
Note: Gender (1 = males, 0 = females); COVID‐19 close death (1 = yes, 0 = no).
Abbreviations: BFI‐C, Big Five Inventory‐10‐Conscientiousness; BFI‐O, Big Five Inventory‐10‐openness; C‐19ASS‐P, COVID‐19 Anxiety Syndrome Scale‐Perseveration; CAS, Coronavirus Anxiety Scale; PHQ, Patient Health Questionnaire‐Depression Scale.
p < 0.05.
p < 0.01.
3.7. Mediation analysis: The potential mediating role of the C19‐ASS
For further analysis on C19‐ASS, we examined whether COVID‐19 Anxiety Syndrome could mediate the relationship between the Big Five personality traits as predictors and variables such as GAD‐7, PHQ, WI and CAS as outcomes. The path analysis was conducted after assessing assumptions. An initial examination of the data showed that the openness and conscientiousness factor does not significantly influence the outcomes (ps > 0.05). Thus, it was removed from the model. All other personality traits were directly associated with outcomes (see Table 7). The mediation model was evaluated using the bootstrapping method (iteration number = 2000) at the 2.5th and 97.5th percentiles with a 95% confidence interval, to determine the mediating role of C19‐ASS in the relationship between Big Five personality traits and psychopathology.
TABLE 7.
Standardized direct effect of the variables in the mediation model
| Predictor | Outcome | β | Ll | Ul |
|---|---|---|---|---|
| Extraversion | C19‐ASS | −0.078** | −0.121 | −0.033 |
| Agreeableness | C19‐ASS | −0.055* | −0.102 | −0.012 |
| Neuroticism | C19‐ASS | 0.080** | 0.032 | 0.123 |
| Extraversion | CAS | 0.075** | 0.035 | 0.111 |
| Extraversion | PHQ | −0.164*** | −0.205 | −0.123 |
| Extraversion | GAD | −0.067** | −0.107 | −0.027 |
| Extraversion | WI | −0.040 | −0.082 | 0.000 |
| Agreeableness | CAS | −0.035 | −0.077 | 0.007 |
| Agreeableness | PHQ | −0.093*** | −0.106 | −0.053 |
| Agreeableness | GAD | −0.106*** | −0.146 | −0.067 |
| Agreeableness | WI | −0.132*** | −0.172 | −0.090 |
| Neuroticism | CAS | 0.146*** | 0.104 | 0.184 |
| Neuroticism | PHQ | 0.339*** | 0.298 | 0.375 |
| Neuroticism | GAD | 0.427*** | 0.385 | 0.463 |
| Neuroticism | WI | 0.268*** | 0.224 | 0.308 |
| C19‐ASS | CAS | 0.310*** | 0.275 | 0.346 |
| C19‐ASS | PHQ | 0.145*** | 0.105 | 0.182 |
| C19‐ASS | GAD | 0.150*** | 0.110 | 0.192 |
| C19‐ASS | WI | 0.231*** | 0.190 | 0.272 |
Abbreviations: A, agreeableness; C, conscientiousness; C19‐ASS, COVID‐19 anxiety syndrome scale; CAS, Coronavirus Anxiety Scale; E, extraversion; GAD, generalized anxiety disorder; N, neuroticism; PHQ, Patient Health Questionnaire‐Depression; WI, Whiteley Index for health anxiety.
p < 0.050.
p < 0.010.
p < 0.00.
The fit indices for this model are as follows: X 2/df = 4.69; GFI = 0.999; CFI = 0.999; RMSEA = 0.051; and SRMR = 0.010, which is acceptable. C19‐ASS partially mediated the relationship between the Big Five personality traits (extraversion, agreeableness, and neuroticism) with study outcomes (CAS, WI, GAD, PHQ), in the other paths. And, it fully mediated the relationship between agreeableness and CAS, extraversion and WI (see Table 8). In Table 7, the standardized direct, and Table 8, the standardized indirect effects of the examined variables are shown, and Figure 2 depicts the path diagram for the mediation analysis.
TABLE 8.
The indirect effect of the mediating role of C19‐ASS in the relationship between the Big Five personality traits and psychopathology
| Indirect path | B | Ll | Ul | p value | β |
|---|---|---|---|---|---|
| E → C19ASS → CAS | −0.019 | −0.032 | −0.009 | 0.004 | −0.024** |
| E → C19ASS → PHQ | −0.037 | −0.065 | −0.016 | 0.003 | −0.011** |
| E → C19ASS → GAD | −0.029 | −0.050 | −0.013 | 0.003 | −0.012** |
| E → C19ASS → WI | −0.048 | −0.080 | −0.021 | 0.004 | −0.018** |
| A → C19ASS → CAS | −0.017 | −0.031 | −0.004 | 0.029 | −0.017* |
| A → C19ASS → PHQ | −0.032 | −0.064 | −0.008 | 0.025 | −0.008* |
| A → C19ASS → GAD | −0.025 | −0.050 | −0.007 | 0.023 | −0.008* |
| A → C19ASS → WI | −0.041 | −0.078 | −0.010 | 0.029 | −0.013* |
| N → C19ASS → CAS | 0.017 | 0.007 | 0.027 | 0.003 | 0.025** |
| N → C19ASS → PHQ | 0.033 | 0.014 | 0.058 | 0.003 | 0.012** |
| N → C19ASS → GAD | 0.026 | 0.011 | 0.045 | 0.003 | 0.012** |
| N → C19ASS → WI | 0.043 | 0.017 | 0.070 | 0.004 | 0.018** |
Abbreviations: A, agreeableness; C, conscientiousness; C19‐ASS, COVID‐19 Anxiety Syndrome Scale; CAS, Coronavirus Anxiety Scale; E, extraversion; GAD, generalized anxiety disorder; N, neuroticism; PHQ, Patient Health Questionnaire‐Depression; WI, Whiteley Index for health anxiety.
p < 0.05.
p < 0.01.
FIGURE 2.
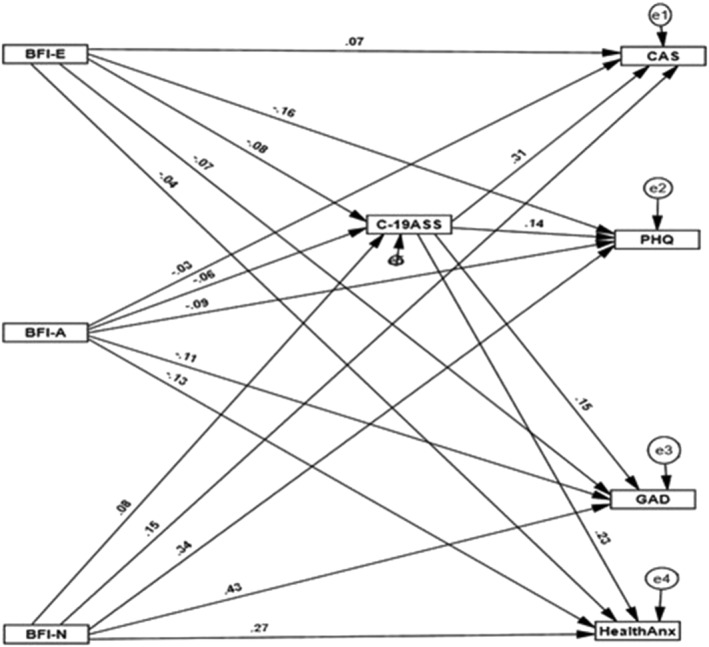
Standardized path diagram for the mediating role of C19‐ASS in relationship between the Big Five personality traits and psychopathology. To keep the model clear, the covariances are removed. BFI‐A, Big Five Inventory‐10‐Agreeableness; BFI‐E, Big Five Inventory‐10‐Extraversion; BFI‐N, Big Five Inventory‐10‐Neuroticism; CAS, Coronavirus Anxiety Scale; PHQ, depressive symptoms, Patient Health Questionnaire; GAD, generalized anxiety disorder; health Anx, health anxiety; Whiteley index
4. DISCUSSION
Early measures developed to assess psychological responses to the threat of COVID‐19 focused on fear, stress, anxiety and perceived threat. Diverging from the assessment of the symptoms of COVID‐19 anxiety and fear, Nikčević and Spada (2020) proposed that in some individuals an excessive and unhelpful pattern of coping may develop in response to the threat of COVID‐19. This coping response may ‘lock’ the person in a state of fear and threat of COVID‐19, which in turn may make a return to normal functioning difficult. They operationalized this coping style via the construct of the COVID‐19 anxiety syndrome, as consisting of avoidance, checking, worrying and threat monitoring. The current study sought to create a Persian version of the C19‐ASS and test its psychometric properties in a general community sample of Iranians so to examine the relevance of this construct in a non‐Western sample. The findings here corroborate preliminary evidence supporting the notion of COVID‐19 anxiety syndrome (Albery et al., 2021; Nikčević & Spada, 2020; Nikčević et al., 2021). The Persian C19‐ASS was similarly valid, with convergent and divergent validity, incremental validity, and a factor structure comparable to the parent study (Nikčević & Spada, 2020). The translated scale appears to be a promising tool for understanding COVID‐19‐related psychological processes, specifically anxiety syndrome.
4.1. The Persian C19‐ASS: Structure and reliability
Comparable to the parent study, the EFA suggested that the C19‐ASS has two factors corresponding to the two subscales of perseveration and avoidance. As measured by cross‐validated CFAs, the two‐factor solution model outperformed the one‐factor solution model.
The C19‐ASS items also showed invariance in both the configural and metric measurements across genders. Accordingly, correlations and regression paths can be compared across genders. However, using scalar invariance analysis, all items except for Items 3 with higher intercept for females (I have avoided going out to public places [shops, parks] because of the fear of contracting Coronavirus), 4 (I have been concerned about not having adhered strictly to social distancing guidelines for Coronavirus) and 6 (I have read about news relating to Coronavirus at the cost of engaging in work, such as writing emails, working on word documents or spreadsheets) with higher intercept for males were invariant across genders. It is therefore prudent to interpret the means of the C19‐ASS subscales with some caution. Regarding interpreting these differences, Putnick and Bornstein (2016) suggest that scalar measurement invariance tests are dynamic and informative aspects of the functioning of a construct across groups rather than gateway tests. Thus, the higher intercept for females than males in item number 3 means they avoid going to the public due to fear of COVID‐19. The higher intercepts for Item 4 mean that males are more concerned about not adhering to protocols than females. And, also the higher intercept of Item 6 for males than females means they are getting more involved in monitoring COVID‐19‐related news. In neither gender are those increased intercepts associated with higher levels of corresponding latent construct.
In terms of construct validity, the Persian C19‐ASS converged with measures of anxiety, depression and social dysfunction (see Table 4), suggesting that it indicates psychopathology. Furthermore, the EFA revealed that it is not identical with a comparable construct such as generalized anxiety and that it differs from GAD‐7, in which C19‐ASS subscales loaded on two‐component and GAD on the third (see Appendix A). This implies that the C19‐ASS assesses a concept separate from GAD, and therefore that it cannot be subsumed under generalized anxiety.
Concerning incremental validity, the Persian C19‐ASS, mainly the perseveration subscale, outperformed marital and educational status, neuroticism, consciousness and GAD by accounting for more variance in CAS, as seen in Table 5. Moreover, as seen in Table 6, only the perseveration subscale of C19‐ASS, except PHQ, outperformed gender, close death due to COVID‐19, consciousness, openness, GAD and CAS, accounting for more variance in WSAS. Although the avoidance subscale was significantly associated with WSAS (r = 0.26, p = 0.01), and CAS (r = 0.18, p = 0.01), as seen in Table 4, it was not a significant predictor of WSAS and CAS in the presence of demographics (gender, marital status, educational level and COVID‐19 close death), GAD‐7, PHQ and personality traits (neuroticism, conscientiousness, conscientiousness and openness). It could be interpreted that perseveration is not dependent on the mentioned variables in predicting WSAS and CAS, whereas the avoidance subscale is. In simple terms, an executed avoidance strategy is situation dependent, as not everyone smokes (Akbari et al., 2020), consumes alcohol (Grossman et al., 2020), or is quarantined in an agoraphobic manner (Nasrallah, 2020). Also, to enhance the results, a mediation test supported the mediating role of C19‐ASS in the relationship between Big Five personality traits (except openness and consciousness) with WI, GAD, PHQ and CAS. This is consistent with recent findings that C19‐ASS may be an underlying mechanism by which personality traits are associated with depressive and anxiety symptomology during the COVID‐19 pandemic (Nikčević et al., 2021). Finally, Cronbach's alpha, composite reliability, maximal reliability and average extracted variance support the notion that Persian C19‐ASS is a reliable measure comparable to the parent study.
4.2. Pandemic‐related psychopathology: Towards understanding underlying mechanisms
The COVID‐19 anxiety syndrome was described as a pandemic‐related phenomenon that captures coping responses in response to the threat of COVID‐19 (Nikčević & Spada, 2020). This construct is conceptually aligned with the S‐REF model of psychopathology (Wells, 2011), according to which maladaptive cognitive, behavioural and attentional processes are key in the maintenance of distress outcomes such as anxiety. Such processes are termed the CAS and are characterized by an inflexible focus on the threat and maladaptive coping, which prevents the individual from exiting the distress state.
It remains to be established in future research to what extent the COVID‐19 anxiety syndrome is a stable phenomenon and for how many people. Given that the scores on the C‐19ASS are positively associated with the attentional bias to COVID‐19‐related threat (Albery et al., 2021), it seems that this phenomenon captures the fear and anxiety responses beyond symptoms of COVID‐19 anxiety and, crucially, offers pathways to the reduction of such anxiety. Those who score high will need to release attempts at control and gradually reduce avoidance, checking, threat monitoring and worrying in order to return to normal functioning when, objectively, the risk from COVID‐19 is reduced.
4.3. Limitations and conclusion
The primary limitation of this study is the lack of a longitudinal follow‐up of the results to understand better the temporality of the findings and the causality of C19‐ASS in predicting pandemic‐related distress.
Overall, the current findings provide evidence to support the generalizability of the COVID‐19 anxiety syndrome construct in a sample of Iranians. C19‐ASS represents an effective index for assessing the coping responses in relation to COVID‐19‐related threat. Furthermore, the current findings highlight that avoidance and perseveration are theoretically relevant aspects of COVID‐19 anxiety syndrome uniquely related to psychopathology. Together, the psychometric properties of the Persian C19‐ASS demonstrate that its scores are a reliable and valid indicator of COVID‐19 anxiety syndrome in the general population. The scores relate to several measures of psychopathology, divergent from generalized anxiety, addressing the specific concern associated with COVID‐19. This important psychometric work with the C19‐ASS sets the stage for studying the COVID‐19 psychological distress in terms of its underlying mechanism, which will help us better understand how to deal with current psychological problems that may persist in communities. Aside, our finding sets the stage for further research. Future studies might further evaluate the psychometric features of the C19‐ASS in Persian‐speaking countries and probably test Items 3, 4 and 6 for larger invariance across genders. Additionally, it is worthwhile to investigate the mediating role of C19‐ASS in the association between the Big Five personality traits and depressive and anxiety symptomology, which, particularly in a longitudinal design, would help draw a firm conclusion towards recognizing C19‐ASS as an underlying mechanism of pandemic‐related psychopathology.
Overall, knowing how to recognize the COVID‐19 anxiety syndrome (avoidance, worry, checking and threat monitoring) could be helpful during and after the current health crisis (Asmundson & Taylor, 2020). Interventions aimed at interrupting perseverative thinking (e.g., metacognitive therapy; Wells, 2000), reducing checking, safety behaviours, and avoidance (e.g., graded exposure and response prevention; Barlow et al., 2014) and training and recalibrating attention (e.g., attention training technique; Wells, 2000) may all help to weaken the COVID‐19 anxiety syndrome and possibly reduce the longer term occurrence of psychological distress which is typically linked to pandemic events, in particular post‐traumatic stress, general stress, anxiety, health anxiety and suicidality (Chong et al., 2004; Lee, Mathis, Jobe, & Pappalardo, 2020; Wheaton et al., 2012; Wu et al., 2009).
CONFLICT OF INTEREST
Two of the authors were involved in developing the original version of the C19‐ASS for English‐speaking populations. The authors have no known competing financial interests or personal relationships that could have influenced this work.
ACKNOWLEDGEMENTS
This research did not receive specific grant funding from agencies in the public, commercial or not‐for‐profit sectors.
APPENDIX A.
TABLE A1 Factor analysis for differentiating C19‐ASS from GAD‐7: Divergent validity
| GAD | p | A | |
|---|---|---|---|
| 1. I have avoided using public transport because of the fear of contracting coronavirus | 0.052 | −0.202 | 0.779 |
| 2. I have checked myself for symptoms of coronavirus | 0.090 | 0.740 | −0.042 |
| 3. I have avoided going out to public places (shops, parks) because of the fear of contracting coronavirus | 0.048 | 0.082 | 0.756 |
| 4. I have been concerned about not having adhered strictly to social distancing guidelines for coronavirus | 0.181 | 0.498 | 0.223 |
| 5. I have avoided touching things in public spaces because of the fear of contracting coronavirus | 0.035 | 0.292 | 0.567 |
| 6. I have read about news relating to coronavirus (COVID‐19) at the cost of engaging in work | 0.195 | 0.628 | 0.103 |
| 7. I have checked my family members and loved one for the signs of coronavirus | 0.144 | 0.912 | −0.164 |
| 8. I have been paying close attention to others displaying possible symptoms of coronavirus | 0.140 | 0.795 | 0.000 |
| 9. I have imagined what could happen to my family members if they contracted coronavirus | 0.276 | 0.724 | −0.067 |
| GAD‐7 ITEM 1 | 0.875 | 0.201 | 0.066 |
| GAD‐7 ITEM 2 | 0.863 | 0.210 | 0.126 |
| GAD‐7 ITEM 3 | 0.847 | 0.173 | 0.114 |
| GAD‐7 ITEM 4 | 0.821 | 0.228 | 0.082 |
| GAD‐7 ITEM 5 | 0.778 | 0.171 | 0.060 |
| GAD‐7 ITEM 6 | 0.774 | 0.132 | −0.018 |
| GAD‐7 ITEM 7 | 0.754 | 0.152 | −0.009 |
TABLE A2 Component correlation matrix
| Component | 1 | 2 | 3 |
|---|---|---|---|
| 1. GAD‐7 | — | ||
| 2. C19‐ASS‐Perseverance | 0.218 | — | |
| 3. C19‐ASS‐Avoidance | 0.073 | 0.438 | — |
Akbari, M. , Seydavi, M. , Zamani, E. , Nikčević, A. V. , & Spada, M. M. (2022). The Persian COVID‐19 Anxiety Syndrome Scale (C‐19ASS): Psychometric properties in a general community sample of Iranians. Clinical Psychology & Psychotherapy, 29(3), 906–921. 10.1002/cpp.2686
REFERENCES
- Abba‐Aji, A. , Li, D. , Hrabok, M. , Shalaby, R. , Gusnowski, A. , Vuong, W. , Surood, S. , Nkire, N. , Li, X. M. , Greenshaw, A. J. , & Agyapong, V. I. (2020). COVID‐19 pandemic and mental health: Prevalence and correlates of new‐onset obsessive‐compulsive symptoms in a Canadian province. International Journal of Environmental Research and Public Health, 17(19), 6986. 10.3390/ijerph17196986 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Akbari, M. , Hasani, J. , & Seydavi, M. (2020). Negative affect among daily smokers: A systematic review and meta‐analysis. Journal of Affective Disorders, 274, 553–567. 10.1016/j.jad.2020.05.063 [DOI] [PubMed] [Google Scholar]
- Akbari, M. , Hosseini, Z. S. , Seydavi, M. , Zegel, M. , Zvolensky, M. J. , & Vujanovic, A. A. (2021). Distress tolerance and post‐traumatic stress disorder: A systematic review and meta‐analysis. Cognitive Behaviour Therapy, 1–30. 10.1080/16506073.2021.1942541 [DOI] [PubMed] [Google Scholar]
- Akbari, M. , Seydavi, M. , & Zamani, E. (2021). The mediating role of personalized psychological flexibility in the association between distress intolerance and psychological distress: A national survey during the fourth waves of COVID‐19 pandemic in Iran. Clinical Psychology & Psychotherapy, 1–11. 10.1002/cpp.2685 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Akbari, M. , Spada, M. M. , Nikčević, A. V. , & Zamani, E. (2021). The relationship between fear of COVID‐19 and health anxiety among families with COVID‐19 infected: The mediating role of metacognitions, intolerance of uncertainty and emotion regulation. Clinical Psychology & Psychotherapy, 1–13. 10.1002/cpp.2628 [DOI] [PubMed] [Google Scholar]
- Albery, I. P. , Spada, M. M. , & Nikčević, A. (2021). The COVID‐19 anxiety syndrome and selective attentional bias towards COVID‐19‐related stimuli in UK residents during the 2020‐2021 pandemic. Clinical Psychology Psychotherapy. 10.1002/cpp.2639 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arslan, G. , Yıldırım, M. , Tanhan, A. , Buluş, M. , & Allen, K. A. (2020). Coronavirus stress and psychological health among adults: Exploring the effect of optimism‐pessimism and psychological inflexibility. International Journal of Mental Health and Addiction. 10.1007/s11469-020-00337-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Asmundson, G. J. G. , & Taylor, S. (2020). Coronaphobia: Fear and the 2019‐nCoV outbreak. Journal of Anxiety Disorders, 70, 102196. 10.1016/j.janxdis.2020.102196 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barlow, D. H. , Sauer‐Zavala, S. , Carl, J. R. , Bullis, J. R. , & Ellard, K. K. (2014). The nature, diagnosis, and treatment of neuroticism: Back to the future. Clinical Psychology Science, 2, 344–365. 10.1177/2167702613505532 [DOI] [Google Scholar]
- Brailovskaia, J. , Cosci, F. , Mansueto, G. , & Margraf, J. (2021). The relationship between social media use, stress symptoms and burden caused by Coronavirus (Covid‐19) in Germany and Italy: A cross‐sectional and longitudinal investigation. Journal of Affective Disorders Reports, 3, 100067. 10.1016/j.jadr.2020.100067 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cao, W. , Fang, Z. , Hou, G. , Han, M. , Xu, X. , Dong, J. , & Zheng, J. (2020). The psychological impact of the COVID‐19 epidemic on college students in China. Psychiatry Research, 287, 112934. 10.1016/j.psychres.2020.112934 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen, L. , Zhao, H. , Razin, D. , Song, T. , Wu, Y. , Ma, X. , HuerxidaAji, Wang, G. , Wang, M. , & Yan, L. (2021). Anxiety levels during a second local COVID‐19 pandemic breakout among quarantined people: A cross sectional survey in China. Journal of Psychiatric Research, 135, 37–46. 10.1016/j.jpsychires.2020.12.067 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chong, M.‐Y. , Wang, W.‐C. , Hsieh, W.‐C. , Lee, C.‐Y. , Chiu, N.‐M. , Yeh, W.‐C. , Huang, T.‐L. , Wen, J.‐K. , & Chen, C.‐L. (2004). Psychological impact of severe acute respiratory syndrome on health workers in a tertiary hospital. British Journal of Psychiatry, 185, 127–133. 10.1192/bjp.185.2.127 [DOI] [PubMed] [Google Scholar]
- Czeisler, M. É. , Lane, R. I. , Petrosky, E. , Wiley, J. F. , Christensen, A. , Njai, R. , Weaver, M. D. , Robbins, R. , Facer‐Childs, E. R. , Barger, L. K. , & Rajaratnam, S. M. (2020). Mental health, substance use, and suicidal ideation during the COVID‐19 pandemic—United States, June 24–30, 2020. Morbidity and Mortality Weekly Report, 69(32), 1049–1057. 10.15585/mmwr.mm6932a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duong, C. D. (2021). The impact of fear and anxiety of Covid‐19 on life satisfaction: Psychological distress and sleep disturbance as mediators. Personality and Individual Differences, 178, 110869. 10.1016/j.paid.2021.110869 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grossman, E. R. , Benjamin‐Neelon, S. E. , & Sonnenschein, S. (2020). Alcohol consumption during the COVID‐19 pandemic: A cross‐sectional survey of US adults. International Journal of Environmental Research and Public Health, 17(24), 9189. 10.3390/ijerph17249189 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hacimusalar, Y. , Kahve, A. C. , Yasar, A. B. , & Aydin, M. S. (2020). Anxiety and hopelessness levels in COVID‐19 pandemic: A comparative study of healthcare professionals and other community sample in Turkey. Journal of Psychiatric Research, 129, 181–188. 10.1016/j.jpsychires.2020.07.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hou, T. , Zhang, R. , Song, X. , Zhang, F. , Cai, W. , Liu, Y. , Dong, W. , & Deng, G. (2020). Self‐efficacy and fatigue among non‐frontline health care workers during COVID‐19 outbreak: A moderated mediation model of posttraumatic stress disorder symptoms and negative coping. PLoS ONE, 15(12), e0243884. 10.1371/journal.pone.0243884 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu, L. T. , & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- Huang, Y. , & Zhao, N. (2020). Generalized anxiety disorder, depressive symptoms and sleep quality during COVID‐19 outbreak in China: A web‐based cross‐sectional survey. Psychiatry Research, 288, 112954. 10.1016/j.psychres.2020.112954 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jahrami, H. , BaHammam, A. S. , Bragazzi, N. L. , Saif, Z. , Faris, M. , & Vitiello, M. V. (2021). Sleep problems during the COVID‐19 pandemic by population: A systematic review and meta‐analysis. Journal of Clinical Sleep Medicine, 17(2), 299–313. 10.5664/jcsm.8930 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson, S. U. , Ebrahimi, O. V. , & Hoffart, A. (2020). PTSD symptoms among health workers and public service providers during the COVID‐19 outbreak. PLoS ONE, 15(10), e0241032. 10.1371/journal.pone.0241032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kontoangelos, K. , Economou, M. , & Papageorgiou, C. (2020). Mental health effects of COVID‐19 pandemia: A review of clinical and psychological traits. Psychiatry Investigation, 17(6), 491–505. 10.30773/pi.2020.0161 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kroenke, K. , Spitzer, R. L. , & Williams, J. B. (2001). The PHQ‐9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. 10.1046/j.1525-1497.2001.016009606.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, S. A. (2020). Coronavirus Anxiety Scale: A brief mental health screener for COVID‐19 related anxiety. Death Studies, 44(7), 393–401. 10.1080/07481187.2020.1748481 [DOI] [PubMed] [Google Scholar]
- Lee, S. A. , Mathis, A. A. , Jobe, M. C. , & Pappalardo, E. A. (2020). Clinically significant fear and anxiety of COVID‐19: A psychometric examination of the Coronavirus Anxiety Scale. Psychiatry Research, 290, 113112. 10.1016/j.psychres.2020.113112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu, C. H. , Zhang, E. , Wong, G. T. F. , & Hyun, S. (2020). Factors associated with depression, anxiety, and PTSD symptomatology during the COVID‐19 pandemic: Clinical implications for US young adult mental health. Psychiatry Research, 290, 113172. 10.1016/j.psychres.2020.113172 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mansueto, G. , Lopes, F. L. , Grassi, L. , & Cosci, F. (2021). Impact of COVID‐19 outbreak on Italian healthcare workers versus general population: Results from an online survey. Clinical Psychology & Psychotherapy. 10.1002/cpp.2644 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ministry of Health and Medical Education of Iran . (2021). COVID‐19 news dashboard. Retrieved from http://ird.behdasht.gov.ir/index.aspx
- Mohammadpour, M. , Ghorbani, V. , Moradi, S. , Khaki, Z. , Foroughi, A. A. , & Rezaei, M. R. (2020). Psychometric properties of the Iranian version of the Coronavirus Anxiety Scale. Iranian Journal of Psychiatry and Clinical Psychology, 26(3), 374–387. 10.32598/ijpcp.26.3482.1 [DOI] [Google Scholar]
- Mundt, J. C. , Marks, I. M. , Shear, M. K. , & Greist, J. M. (2002). The Work and Social Adjustment Scale: A simple measure of impairment in functioning. The British Journal of Psychiatry, 180(5), 461–464. 10.1192/bjp.180.5.461 [DOI] [PubMed] [Google Scholar]
- Nasrallah, H. A. (2020). During a viral pandemic, anxiety is endemic: The psychiatric aspects of COVID‐19. Current Psychiatry, 19(4), e3–e5. [Google Scholar]
- Nikčević, A. V. , & Spada, M. (2020). The COVID‐19 anxiety syndrome scale: Development and psychometric properties. Psychiatry Research, 292, 113322. 10.1016/j.psychres.2020.113322 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nikčević, A. V. , Marino, C. , Kolubinski, D. C. , Leach, D. , & Spada, M. M. (2021). Modelling the contribution of the Big Five personality traits, health anxiety, and COVID‐19 psychological distress to generalised anxiety and depressive symptoms during the COVID‐19 pandemic. Journal of Affective Disorders, 279, 578–584. 10.1016/j.jad.2020.10.053 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oh, H. , Marinovich, C. , Rajkumar, R. , Besecker, M. , Zhou, S. , Jacob, L. , Koyanagi, A. , & Smith, L. (2021). COVID‐19 dimensions are related to depression and anxiety among US college students: Findings from the Healthy Minds Survey 2020. Journal of Affective Disorders, 292, 270–275. 10.1016/j.jad.2021.05.121 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Özdin, S. , & Özdin, B. S. (2020). Levels and predictors of anxiety, depression and health anxiety during COVID‐19 pandemic in Turkish society: The importance of gender. International Journal of Social Psychiatry, 66(5), 504–511. 10.1177/0020764020927051 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Putnick, D. L. , & Bornstein, M. H. (2016). Measurement invariance conventions and reporting: The state of the art and future directions for psychological research. Developmental Review, 41, 71–90. 10.1016/j.dr.2016.06.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seçer, İ. , & Ulaş, S. (2020). An investigation of the effect of COVID‐19 on OCD in youth in the context of emotional reactivity, experiential avoidance, depression and anxiety. International Journal of Mental Health and Addiction, 1–14. 10.1007/s11469-020-00322-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shevlin, M. , McBride, O. , Murphy, J. , Miller, J. G. , Hartman, T. K. , Levita, L. , Mason, L. , Martinez, A. P. , McKay, R. , Stocks, T. V. A. , Bennett, K. M. , Hyland, P. , Karatzias, T. , & Bentall, R. P. (2020). Anxiety, depression, traumatic stress and COVID‐19‐related anxiety in the UK general population during the COVID‐19 pandemic. BJPsych Open, 6(6), 1–9. 10.1192/bjo.2020.109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spitzer, R. L. , Kroenke, K. , Williams, J. B. , & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD‐7. Archives of Internal M Medicine, 166(10), 1092–1097. 10.1001/archinte.166.10.1092 [DOI] [PubMed] [Google Scholar]
- Voitsidis, P. , Dialechti Kerasidou, M. , Nikopoulou, A. V. , Tsalikidis, P. , Parlapani, E. , Holeva, V. , & Diakoginnis, I. (2021). A systematic review of questionnaires assessing the psychological impact of COVID‐19. Psychiatry Research, 305, 114183. 10.1016/j.psychres.2021.114183 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wallace, C. L. , Wladkowski, S. P. , Gibson, A. , & White, P. (2020). Grief during the COVID‐19 pandemic: Considerations for palliative care providers. Journal of Pain and Symptom Management, 60(1), e70–e76. 10.1016/j.jpainsymman.2020.04.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang, C. , Pan, R. , Wan, X. , Tan, Y. , Xu, L. , Ho, C. S. , & Ho, R. C. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID‐19) epidemic among the general population in China. International Journal of Environmental Research and Public Health, 17(5). 10.3390/ijerph17051729 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wells, A. (2000). Emotional disorders and metacognition: Innovative cognitive therapy. Wiley. [Google Scholar]
- Wells, A. (2011). Metacognitive therapy for anxiety and depression. Guilford Press. [Google Scholar]
- Wheaton, M. G. , Abramowitz, J. S. , Berman, N. C. , Fabricant, L. E. , & Olatunji, B. O. (2012). Psychological predictors of anxiety in response to the H1N1 (swine flu) pandemic. Cognitive Therapy and Research, 36, 210–218. 10.1007/s10608-011-9353-3 [DOI] [Google Scholar]
- Wheaton, M. G. , Ward, H. E. , Silber, A. , McIngvale, E. , & Björgvinsson, T. (2021). How is the COVID‐19 pandemic affecting individuals with obsessive‐compulsive disorder (OCD) symptoms? Journal of Anxiety Disorders, 81, 102410. 10.1016/j.janxdis.2021.102410 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wierenga, K. L. , Moore, S. E. , Pressler, S. J. , Hacker, E. D. , & Perkins, S. M. (in press). Associations between COVID‐19 perceptions, anxiety, and depressive symptoms among adults living in the United States. Nursing Outlook, 69, 755–766. 10.1016/j.outlook.2021.03.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization . (2021). Coronavirus disease (COVID‐19) situation dashboard. Retrieved from https://covid19.who.int/
- Wu, P. , Fang, Y. , Guan, Z. , Fan, B. , Kong, J. , Yao, Z. , Liu, X. , Fuller, C. J. , Susser, E. , Lu, J. , & Hoven, C. W. (2009). The psychological impact of the SARS epidemic on hospital employees in China: Exposure, risk perception, and altruistic acceptance of risk. Canadian Journal of Psychiatry, 54, 301–311. 10.1177/070674370905400504 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu, P. E. , Styra, R. , & Gold, W. L. (2020). Mitigating the psychological effects of COVID‐19 on health care workers. CMAJ, 192(17), E459–E460. 10.1503/cmaj.200519 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhai, Y. , & Du, X. (2020). Loss and grief amidst COVID‐19: A path to adaptation and resilience. Brain, Behavior, and Immunity, 87, 80–81. 10.1016/j.bbi.2020.04.053 [DOI] [PMC free article] [PubMed] [Google Scholar]