

Abstract
Background
Individuals with severe and persistent mental illness (SPMI) have a higher risk of contracting COVID‐19 than individuals without SPMI. In combination with physical distancing, hygiene protocols, and vaccines, quarantine and self‐isolation are primary means of viral containment. However, individuals with SPMI may experience more difficulties with mandated quarantine or self‐isolation because of their illness(es), stigma, and marginalization. To date, there is a lack of consensus on strategies that could aid such individuals in completing isolation.
Aim
This review aimed to synthesize evidence for interventions to support self‐isolation and mandated quarantine for COVID‐19 among individuals with SPMIs.
Methods
We followed the PRISMA guidelines, searching 19 electronic databases (9 published literature registries and 10 gray literature sources). We looked for relevant randomized controlled trials, quasi‐experimental studies, and program evaluations of the effectiveness of relevant psychosocial, pharmacological, harm reduction, and addiction management strategies to support isolation settings or quarantine requirements for individuals with any SPMI (e.g., any mental disorder, substance use disorder, or their combination).
Findings
Of 10,298 total records that were located, 5582 were duplicate citations. Upon screening the remaining 4716 unique records by title and abstract, we excluded a further 3562 records. Only one original article met our inclusion criteria after reviewing the full texts of the remaining 1154 citations. To support individuals experiencing homelessness during the COVID‐19 pandemic, San Francisco developed an isolation hotel that reduced COVID‐19 hospital strain for 1009 participants (25% had a mental health disorder and 26% had a substance use disorder). While 81% completed their hotel stay, 48 patients had behavioral health needs that exceeded the hotel's capabilities. No other studies met our review's eligibility criteria. Most articles located by the search simply proposed solutions or discussed the challenges brought by COVID‐19 for people with SPMIs. While some documents went a step further (e.g., shelter guidance documents to support individuals experiencing homelessness), these rarely addressed individuals with SPMIs directly.
Conclusions
This systematic review evaluated evidence from published and gray literature on interventions to support self‐isolation and mandated COVID‐19 quarantine for individuals with SPMIs. Only one study met our inclusion criteria. This study found a beneficial effect of a dedicated isolation hotel for individuals experiencing homelessness and COVID‐19—where approximately 25%–50% of the study sample had a mental or substance use disorder. While there has been an abundance of COVID‐19 protocols in general, information for SPMIs is lacking. As the pandemic continues and we better prepare for future pandemics, developing protocols for supporting SPMIs in this context is imperative.
Highlights
Individuals with severe and persistent mental illness (SPMI) have a higher risk of contracting COVID‐19 than individuals without SPMI.
This review aimed to synthesize evidence for interventions to support self‐isolation and mandated quarantine for COVID‐19 among individuals with SPMIs.
Only one study met our inclusion criteria. This study found a beneficial effect of a dedicated isolation hotel for individuals experiencing homelessness and COVID‐19—where approximately 25%–50% of the study sample had a mental or substance use disorder.
While there has been an abundance of COVID‐19 protocols in general, information for SPMIs is lacking.
As the pandemic continues and we better prepare for future pandemics, developing protocols for supporting SPMIs in this context is imperative.
As of March 2020, the World Health Organization declared the respiratory disease caused by SARS‐CoV‐2 coronavirus (COVID‐19) a global pandemic (1). As a result, governments mandated various containment procedures, such as self‐isolation or quarantine lasting up to 2 weeks, regional lockdowns, travel restrictions, and physical distancing requirements to slow the spread of the virus. However, while these measures mitigated the risk of spread, there were harmful impacts on mental health (2, 3, 4, 5, 6, 7, 8).
To that end, the literature has extensively reviewed the psychological impact of isolation and quarantine (9, 10, 11, 12, 13). However, the effects of quarantine and self‐isolation on individuals with severe and persistent mental illnesses (SPMIs)—such as psychotic, mood, and substance use disorders (SUDs)—are unclear (14). Compared to individuals without SPMIs, individuals with SPMIs are at greater risk for acquiring COVID‐19 (15, 16, 17) due to several co‐occurring risk factors. First, individuals with SPMIs have more limited healthcare access within their respective communities, making it more challenging to access routine COVID‐19 screening facilities (18). Second, individuals with SPMIs carry a disproportionately more significant burden of comorbid conditions, including disorders that increase their vulnerability to acquiring COVID‐19 and experiencing severe COVID‐19 illness (19). Third, individuals with SPMIs are more likely to have poorer social determinants of health, such as unstable housing (20), stigma, marginalization, and fewer resources to practice physical distancing and basic hygiene (21). Fourth, individuals with SPMIs residing in crowded spaces, particularly those in criminal justice settings and shelters, are at higher risk for acquiring COVID‐19 (22). These circumstances and low treatment adherence raise the risk for contracting COVID‐19 and may worsen compliance with public health protocols for COVID‐19. For example, impaired cognition could decrease awareness of the need for physical distancing (21).
Interim clinical guidance from several medical agencies aims to provide recommendations to support SPMIs and people who use drugs throughout the COVID‐19 pandemic (23). While there are pharmacotherapy and harm reduction protocols for some psychoactive substances (24), there is a need for specific guidance around concurrent behavior management beyond overdose and withdrawal risk for individuals with SPMIs. In addition, targeted quarantine support strategies for individuals with SPMIs, particularly those who try to leave self‐isolation prematurely, are needed, as these create significant behavior management issues, putting staff, and others in the community at risk.
Given the expected longevity of the COVID‐19 pandemic and the possibility that similar situations may occur in the future, developing guidance for deciding how to manage concerns would prioritize limiting outbreaks and the spread of the virus. Therefore, the present systematic review aimed to synthesize the evidence of pharmacological and psychosocial interventions for supporting isolation among individuals living with SPMIs.
METHODS
Protocol and Registration
We prospectively registered this review with PROSPERO (CRD42020208155). We adhered to the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) guidelines (25). As a systematic review of previously published studies, the University of Calgary Conjoint Health Ethics Board determined the study was exempt.
Eligibility Criteria
We used the population‐intervention‐comparison‐outcome‐study design (PICOS) framework to determine eligibility criteria (26). Eligible populations were any individuals with SPMIs who are facing COVID‐19 isolation conditions. While there is no standard definition of SPMIs (27), we considered all major psychiatric disorder categories (e.g., mood, anxiety, psychotic, personality, substance, and neurocognitive disorders). We did not place any restrictions on individuals' type of disorder, symptom severity, or treatment status. Eligible interventions were those aiming to support self‐isolation or mandatory quarantine for COVID‐19, including harm reduction strategies, pharmacotherapy (e.g., opioid agonist therapy for treating opioid withdrawal due to forced isolation), psychotherapies (e.g., cognitive behavioral therapy), or other psychosocial interventions (e.g., isolation hotels). We did not implement a comparator requirement. However, we considered comparisons (e.g., if a study compared two or more interventions against each other). Eligible outcomes were containment measures (e.g., proportion who remain in isolation before and after the studied intervention) and effectiveness/efficacy measures (e.g., change in infection risk behaviors and infection transmission rates). There were no restrictions based on study design, language, or year of publication.
Information Sources
We consulted a health sciences research librarian to develop a comprehensive search strategy for peer‐reviewed published literature and gray literature, such as government documents, guidelines, rapid clinical guidance documents, and relevant websites. Electronic databases for the peer‐reviewed literature search included PubMed, MEDLINE, PsycINFO, Cochrane, and EMBASE. Gray literature sources included websites from leading addictions and psychiatric institutions, such as the American Psychiatric Association (APA), the Canadian Psychiatric Association, British Columbia Center for Substance Use, the American Society of Addiction Medicine (ASAM), and the Canadian Society of Addiction Medicine. We also searched the reference lists of included studies and related reviews for other studies that may meet eligibility criteria. Finally, we searched for unpublished, ongoing trials using the FDA website (www.clinicaltrials.gov) as well as the World Health Organization International Clinical Trial Registry (www.who.int/ictrp/en).
Search Strategy
We present our full search strategies for all databases, registers, and websites, including filters and limits used, in the online supplement (Appendix 1 in Supporting Information S1). We include additional references for review as an online supplement (Appendix 2 in Supporting Information S2).
Selection Process
We used Cochrane's Covidence, a web‐based systematic review manager, to remove duplicate citations and screen records (28). One co‐author (AB) independently screened all articles and gray literature results against the pre‐specified eligibility criteria by title and abstract, and then in full. A second co‐author (DC) reviewed a subset of 150 randomly selected abstracts and titles to ensure the fidelity of the process. The resulting agreement was sufficient (kappa >99%), justifying the use of a single reviewer in combination with automated screening.
Data Collection Process
Using Covidence, one co‐author (AB) extracted data from reports. We contacted study investigators to obtain and confirm data where necessary. We used automation tools supplied by Covidence to find the key PICOS characteristics of each included study.
Data Items
We extracted the following PICOS data items from relevant studies using Covidence, including study name, location, sample characteristics (age, sex, SPMI type, sample size), intervention, comparator (if used), measured outcomes, and study design.
Study Risk of Bias Assessment
One co‐author (AB) independently appraised study quality using the Cochrane Risk of Bias Tool for randomized controlled trials (29) and the risk of bias in non‐randomized studies (ROBIN‐I) for non‐randomized trials (30). In addition, we used Covidence's automated risk of bias feature to support the identification of individual risk of bias domains in each study (e.g., randomization quality, allocation concealment, blinding, selective reporting). We also collected information on study registration and report of funding sources.
Synthesis of Results
We undertook a descriptive synthesis as a meta‐analysis was not possible given available data.
RESULTS
Study Selection
Of the 10,298 total records found by our search strategy, 5582 were duplicate citations. Upon screening the remaining 4716 unique records by title and abstract, we excluded a further 3562 records. Thus, only one original article met our inclusion criteria after reviewing the full texts of the remaining 1154 citations (Figure 1).
FIGURE 1.
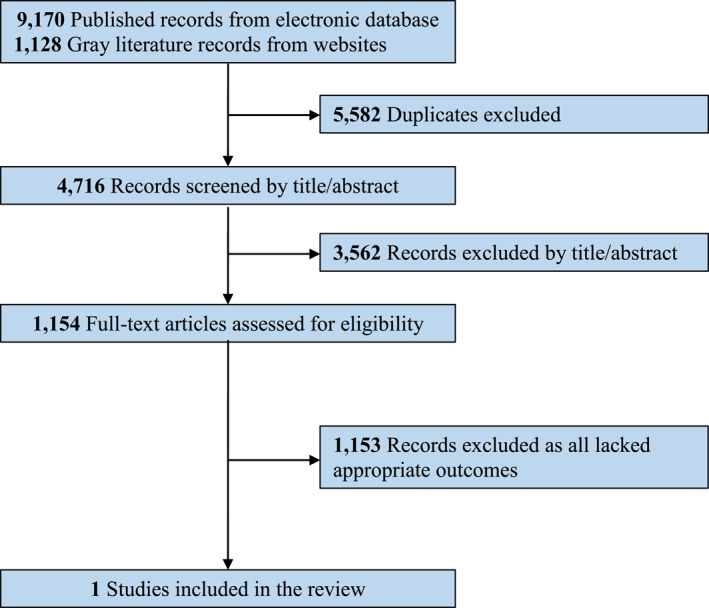
PRISMA flow diagram
Study Characteristics
In San Francisco, Fuchs et al. (31) retrospectively evaluated the effectiveness of an isolation hotel for individuals experiencing homelessness during the COVID‐19 pandemic before vaccines became available. Of the 1009 participants included in the study, 225 (25%) had a diagnosed mental health disorder, 236 (26%) had a diagnosed substance use disorder, and 91 (10%) had been in jail in the past year. In total, 81% completed their hotel stay, and the factors associated with premature discontinuation of isolation conditions were unsheltered homelessness and requiring quarantine as a close contact. However, the study did not report whether the factors associated with discontinuation were the same across individuals with or without SPMIs. In addition, although direct transfers to isolation hotels from the emergency and outpatient departments were associated with averting hospital admissions, 48 patients had behavioral health needs that exceeded the hotel capabilities; for these individuals, their ultimate disposition was unclear. For these reasons, according to the ROBINS‐I tool, the study had a serious risk of bias due to missing data (as described for individuals with SPMI) and selection bias. Consequently, strategies to improve guest retention and address behavioral health needs not met in hotel settings are intervention priorities, as described by the study authors.
Other Findings
Despite finding many potentially relevant articles, no other articles met our review's eligibility criteria. Instead, most reports proposed solutions or discussed the challenges brought by COVID‐19 for people with SPMIs. While some documents went a step further (e.g., shelter guidance documents to support individuals experiencing homelessness), these rarely addressed individuals with SPMIs directly. However, in some of these shelter guidance documents obtained from the gray literature search, sections were devoted to psychosocial supports and protocols for people with mental disorders, which we will summarize below.
Alberta Health Services developed a rapid review guidance document for preventing, controlling, and managing COVID‐19 for homeless shelter operators, staff, and volunteers to prepare and know what will happen during an outbreak (32). Recommendations for psychosocial support to individuals with pre‐existing or COVID‐related mental illness were outlined, including offering designated bedrooms and bathrooms, limiting visitors, maintaining physical distance from ill individuals, avoiding sharing of household items, frequent hand hygiene and sanitation, and self‐monitoring for COVID‐19 symptoms. In addition, psychosocial supports for individuals with pre‐existing addiction or mental health concerns were described, including the risk of becoming more acutely ill, unplanned detox, increased stress, and grief. Furthermore, the document outlined a protocol for providing a private hotel unit or a designated isolation space and adequate psychosocial and medical/pharmacy support for highly vulnerable clients. Finally, the article references an outbreak team, which guides the shelter and isolation units on how to manage clients who leave the shelter space prematurely, and including providing such clients with additional supports, but does not go into detail to describe the nature or extent of those supports or an evaluation of their effectiveness.
In a similar vein, a policy briefing report prepared by the Royal Society of Canada outlined the vulnerability of people experiencing homelessness during COVID‐19. The report described the impact upon those who experience homelessness and those who serve them and made recommendations to reduce or prevent further negative consequences of this or another similar crisis (33). Specifically, the policy brief provides a series of recommendations to inform shelter care for individuals with mental illness, based on informal feedback from clients in shelter care during COVID‐19. In addition, the authors developed a list of potential “rewards” they could offer to incentivize adherence to isolation protocols based on client feedback and the support workers; these included access to snacks, drinks, cash‐equivalent vouchers, cigarettes, cannabis, alcohol, and other substances. To that end, the authors recommended implementing co‐location of onsite programs for supporting mental health and substance use as an essential strategy for improving retention. One example was harm reduction resources, including intravenous or oral opioid replacement programs and overdose prevention services on site.
To maximize the available data, our review also examined peripheral populations and looked for data on individuals with SPMIs, including incarcerated individuals, homeless populations, and rapid medical guideline documents (Appendix 2 in supporting information S1). Most outlined general concerns about COVID‐19 and mentioned that supporting mental health throughout the pandemic is a priority. For example, the literature covered by our review points to group counseling, contingency management, and residential dual diagnosis treatment as three potentially effective interventions for homeless individuals with SUDs. However, from the perspective of our review question, the issue is that these interventions focus on improving substance use outcomes and not how to support individuals with SPMIs temporarily housed in isolation settings. From commentaries, there was also a lack of consensus about how to promote self‐isolation in this population.
DISCUSSION
To our knowledge, the present review is the first to synthesize the state of evidence for interventions in supporting COVID‐19 isolation and mandatory quarantine for individuals with SPMIs. For individuals with SPMIs entering quarantine, the goal is to improve retention and prevent certification and mandated hospital stay on a public health warrant. We identified many proposed strategies that could enhance the likelihood of self‐isolation or quarantine, such as safe supply, withdrawal management, virtual care platforms, mobile response teams, institution‐based programming (e.g., for incarcerated individuals or those experiencing homeless), isolation hotels, and stable housing. The common thread aligning these interventions was the emphasis on continuity of treatment, making them likely helpful to the overall care of individuals with SPMIs, regardless of whether specific data show they support mandated quarantine or isolation. Only one study met our eligibility criteria across the 4716 unique studies identified by our review (31). However, even that study did not directly address SPMIs, but homeless individuals, where roughly one‐quarter had a mental disorder or a substance use disorder. While the isolation hotel halved the hospital stay for homeless people with COVID‐19, most SPMIs had behavioral needs exceeding what the hotels could provide. Therefore, strategies to improve retention and address unmet behavioral health needs in isolation hotel settings remain an intervention priority.
COVID‐19 substantially impacts researching interventions supporting self‐isolation and quarantine for individuals with SPMIs, such as participant recruitment, reduced staff availability, inconsistent access to treatment, less health literacy, stigma, and discrimination. Future research should develop such guidance, explore whether interventions improve isolation retention, and embed findings into risk stratification strategies. For example, for individuals with substance use disorders, one approach may parallel ASAM's Patient Placement Criteria 2 Revised, which addresses substance use severity, types of substances used, method of use, stage of change around use, intoxication/withdrawal risk potential, medical comorbidity/complications, history of intrusive/aggressive behavior, risk of flight, mental illness (especially psychosis), relapse potential, and client perception of the need to physically distance (insight) (34).
Consequently, we can make educated suggestions based on clinical guidance and the limited available research data. Historically, pandemic responses blame and stigmatize marginalized groups, including individuals with SPMIs (35). Geography is also an important consideration, and, consequently, the best strategies involve utilizing evidence‐based information to mitigate fear and stigma in the local context (36). Potential interventions for supporting self‐isolation for people with SPMIs should be mindful of their mental health needs, acknowledge limited trust and proneness to paranoia, avoid coerciveness, improve engagement, supply a safe environment, and limit the potential for substance withdrawal and supporting immediate health needs (37, 38). Oral pharmacotherapy to help manage agitation, irritability, withdrawal, and sleeplessness might also be helpful alongside coordinated medical care (37, 39). Culturally appropriate and trauma‐informed mental and physical health services remain helpful in this context (40, 41, 42). We support interventions designed to engage patients with SPMIs in treatment. Some form of contingency management, where rewards can incentivize the desired behavior, would likely help individuals with SPMIs stay isolated (24).
Strengths and Limitations
To our knowledge, this study is the first review of interventions to support COVID‐19 self‐isolation and quarantine for individuals with SPMIs. However, only one study met our eligibility criteria. While this reflects the current span of the literature on this topic, we may have missed relevant studies. Second, we broadly defined SPMIs and included participants with any mental health problems. However, most definitions of SPMI include some measure of disability and duration, such that transient increases in anxiety and depressive symptoms associated with COVID‐19 would typically not be considered SPMIs. Third, we were unable to conduct a quantitative meta‐analysis. Although we did not restrict articles by language in the present review, it is still possible that our findings are biased because we used databases that are geared towards finding English language articles (e.g., PubMed, MEDLINE, EMBASE). Finally, we limited the search strategy to the current pandemic. While there may be a benefit in widening the search criteria to other pandemics or disasters, the results of a widened search may be of limited clinical applicability to the current situation.
CONCLUSION
This systematic review evaluated interventions to support self‐isolation and mandated COVID‐19 quarantine for individuals with SPMIs. Only one study met our inclusion criteria, which found a beneficial effect of a COVID‐19 isolation hotel for individuals experiencing homelessness, where approximately half the sample had a mental or substance use disorder. There is a need for added research on this topic and a need for consensus on related research priorities.
Supporting information
Supporting information S1
Supporting information S2
We would like to thank the American Psychiatric Association (APA), American Psychiatric Association Foundation (APAF), and the APA Council on Research for their biweekly mentorship meetings and support of this project. We would also like to thank the Health Sciences Research Librarians at the University of Calgary for their help in developing our systematic review search strategy. We received financial support from a 2020 Research Grant on the Impact of COVID‐19 on Psychiatry by the APA and the APAF.
Dr. Danilewitz reports personal fees from Eisai Ltd and Winterlight Labs outside the submitted work. Dr. Bahji reports research grants from the National Institutes of Health/National Institute on Drug Abuse (NIDA) (R25‐DA037756, R25DA033211) through the International Collaborative Addiction Medicine Research Fellowship and the Research in Addiction Medicine Scholars Program through Boston University School of Medicine. In addition, Dr. Bahji is a recipient of the 2020 Friends of Matt Newell Endowment from the University of Calgary Cumming School of Medicine.
REFERENCES
- 1. World Health Organization . Coronavirus Disease (COVID‐19). World Health Organization; [Internet]. 2021. [cited 2021 Apr 24]. Available from: https://www.who.int/emergencies/diseases/novel‐coronavirus‐2019 [Google Scholar]
- 2. Wu T, Jia X, Shi H, Niu J, Yin X, Xie J, et al. Prevalence of mental health problems during the COVID‐19 pandemic: a systematic review and meta‐analysis. J Affect Disord. 2021;281:91–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Wang Y, Shi L, Que J, Lu Q, Liu L, Lu Z, et al. The impact of quarantine on mental health status among general population in China during the COVID‐19 pandemic. Mol Psychiatry. 2021:1–10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Tang S, Xiang M, Cheung T, Xiang Y‐T. Mental health and its correlates among children and adolescents during COVID‐19 school closure: the importance of parent‐child discussion. J Affect Disord. 2021;279:353–60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Simon J, Helter TM, White RG, van der Boor C, Łaszewska A. Impacts of the Covid‐19 lockdown and relevant vulnerabilities on capability well‐being, mental health and social support: an Austrian survey study. BMC Public Health. 2021;21(1):314 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Shah SMA, Mohammad D, Qureshi MFH, Abbas MZ, Aleem S. Prevalence, psychological responses and associated correlates of depression, anxiety and stress in a global population, during the coronavirus disease (COVID‐19) pandemic. Community Ment Health J. 2021;57(1):101–10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Niedzwiedz CL, Green MJ, Benzeval M, Campbell D, Craig P, Demou E, et al. Mental health and health behaviours before and during the initial phase of the COVID‐19 lockdown: longitudinal analyses of the UK Household Longitudinal Study. J Epidemiol Community Health. 2021;75(3):224–31 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Kshirsagar MM, Dodamani AS, Dodamani GA, Khobragade VR, Deokar RN. Impact of Covid‐19 on mental health: an overview. Rev Recent Clin Trials. 2021;16(3):227–31 [DOI] [PubMed] [Google Scholar]
- 9. Harvey PD. Mood symptoms, cognition, and everyday functioning. Innov Clin Neurosci. 2011;8(10):14–18 [PMC free article] [PubMed] [Google Scholar]
- 10. Alfawaz HA, Wani K, Aljumah AA, Aldisi D, Ansari MGA, Yakout SM, et al. Psychological well‐being during COVID‐19 lockdown: insights from a Saudi State University’s Academic Community. J King Saud Univ Sci. 2021;33(1):101262 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Chen L, Zhao H, Razin D, Song T, Wu Y, Ma X, et al. Anxiety levels during a second local COVID‐19 pandemic breakout among quarantined people: a cross sectional survey in China. J Psychiatr Res. 2021;135:37–46 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Huang S, Zhuang W, Wang D, Zha L, Xu X, Li X, et al. Persistent somatic symptom burden and sleep disturbance in patients with COVID‐19 during hospitalization and after discharge: a prospective cohort study. Med Sci Monit. 2021;27:e930447 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Lev Bar‐Or R, Shalit N, Shpitzer R, Kor A, Lev‐Ran S. Self‐reported changes in use of addictive substances and behaviors among patients treated in an addiction treatment clinic during the COVID‐19 quarantine. Isr Med Assoc J. 2021;23(1):11 [PubMed] [Google Scholar]
- 14. Hategan A, Abdurrahman M. Hidden in plain sight: addressing the unique needs of high‐risk psychiatric populations during the COVID‐19 pandemic. Psychiatry Clin Neurosci [Internet]. 2020. [cited 2021 Apr 24];74(8):439. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7267453/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Nemani K, Li C, Olfson M, Blessing EM, Razavian N, Chen J, et al. Association of psychiatric disorders with mortality among patients with COVID‐19. JAMA Psychiatry. 2021;78(4):380–6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Wang QQ, Kaelber DC, Xu R, Volkow ND. COVID‐19 risk and outcomes in patients with substance use disorders: analyses from electronic health records in the United States. Mol Psychiatry. 2020;26(1):30–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Wang Q, Xu R, Volkow ND. Increased risk of COVID‐19 infection and mortality in people with mental disorders: analysis from electronic health records in the United States. World Psychiatry. 2021;20(1):124–30 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.xGrover A, Kennedy Bailey R. Mental health and substance use disorders in COVID‐19 pandemic. Addict Res [Internet]. 2020. [cited 2021 Apr 24];4(1). Available from: http://www.scivisionpub.com/pdfs/mental‐health‐and‐substance‐use‐disorders‐in‐covid19‐pandemic‐1317.pdf [Google Scholar]
- 19. Taquet M, Luciano S, Geddes JR, Harrison PJ. Bidirectional associations between COVID‐19 and psychiatric disorder: retrospective cohort studies of 62 354 COVID‐19 cases in the USA. Lancet Psychiatry. 2021;8(2):130–40 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Sharma M, Aggarwal S. Homeless individuals with mental illness during COVID‐19. Asian J Psychiatr. 2020;53:102408 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Tobolowsky FA. COVID‐19 outbreak among three affiliated homeless service sites—King County, Washington. MMWR Morb Mortal Wkly Rep [Internet]. 2020. [cited 2020 May 26];69(17):523–6. Available from: http://www.cdc.gov/mmwr/volumes/69/wr/mm6917e2.htm [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Brito C, Silva LNda, Xavier CCL, Antunes VH, Costa MS, Filgueiras SL. The way of life of the unhoused people as an enhance for COVID‐19 care. Rev Bras Enferm. 2021;74(Suppl 1):e20200832 [DOI] [PubMed] [Google Scholar]
- 23. Bahji A, Danilewitz M, Crockford D. Supporting individuals who Use drugs during the COVID‐19 pandemic: a rapid review of international guidelines. Can J Addict. 2021;12(2):6–19 [Google Scholar]
- 24. Bach P, Robinson S, Sutherland C, Brar R. Innovative strategies to support physical distancing among individuals with active addiction. Lancet Psychiatry. 2020;7(9):731–3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta‐analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Methley AM, Campbell S, Chew‐Graham C, McNally R, Cheraghi‐Sohi S. PICO, PICOS and SPIDER: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv Res [Internet]. 2014. [cited 2019 Apr 9];14(1):579. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4310146/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Zumstein N, Riese F. Defining severe and persistent mental illness – a pragmatic utility concept analysis. Front Psychiatry. 2020;11:648 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Veritas Health Innovation . Covidence systematic review software. 2019. [Google Scholar]
- 29. Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Wells G, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle‐Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta‐Analyses. Ottawa Hospital Research Institute; [Internet]. 2019. [cited 2019 May 23]. Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp [Google Scholar]
- 31. Fuchs JD, Carter HC, Evans J, Graham‐Squire D, Imbert E, Bloome J, et al. Assessment of a hotel‐based COVID‐19 isolation and quarantine strategy for individuals experiencing homelessness. JAMA Netw Open. 2021;4(3):e210490 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Alberta Health Services . Shelter Guidance: Preventing, Controlling and Managing COVID‐19. Alberta Health Services; [Internet]. 2020. [cited 2021 Apr 12]. Available from: https://www.albertahealthservices.ca/assets/info/ppih/if‐ppih‐covid‐19‐outbreak‐shelter.pdf [Google Scholar]
- 33. Royal Society of Canada, Turnbull J, Baral S, Bond A, Boozary A, Bruketa E, et al. Seeking Shelter: Homelessness and COVID‐19. Royal Society of Canada; [Internet]. 2021. [cited 2021 Apr 12]. Available from: https://rsc‐src.ca/sites/default/files/Homelessness%20PB_EN_0.pdf [Google Scholar]
- 34. American Society of Addiction Medicine . About the ASAM Criteria. American Society of Addiction Medicine; [Internet]. 2021. [cited 2021 Jun 11]. Available from: https://www.asam.org/asam‐criteria/about [Google Scholar]
- 35. Jones DS. History in a crisis—lessons for Covid‐19. N Engl J Med. 2020;382(18):1681–3 [DOI] [PubMed] [Google Scholar]
- 36. Shalev D, Shapiro PA. Epidemic psychiatry: the opportunities and challenges of COVID‐19. Gen Hosp Psychiatry. 2020;64:68–71 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Canadian Research Initiative in Substance Misuse, Canadian Institute for Health Research . Medications and Other Approaches to Support Physical Distancing for People Who Use Substances during the COVID‐19 Pandemic: National Rapid Guidance; [Internet]. 2020. [cited 2020 Aug 30]. Available from: https://crism.ca/wp‐content/uploads/2020/06/CRISM‐Guidance‐Medications‐and‐other‐clinical‐approaches‐22062020‐final.pdf [Google Scholar]
- 38. Ness MM, Saylor J, Di Fusco LA, Evans K. Healthcare providers’ challenges during the coronavirus disease (COVID‐19) pandemic: a qualitative approach. Nurs Health Sci. 2021;23(2):389–97 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Canadian Research Initiative in Substance Misuse, Canadian Institute for Health Research . Telemedicine Support for Addiction Services: National Rapid Guidance [Internet]. 2020. [cited 2020 Aug 30]. Available from: https://crism.ca/wp‐content/uploads/2020/05/CRISM‐National‐Rapid‐Guidance‐Telemedicine‐V1.pdf [Google Scholar]
- 40. Furlong Y, Finnie T. Culture counts: the diverse effects of culture and society on mental health amidst COVID‐19 outbreak in Australia. Ir J Psychol Med. 2020;37(3):237–42 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Banducci AN, Weiss NH. Caring for patients with posttraumatic stress and substance use disorders during the COVID‐19 pandemic. Psychol Trauma. 2020;12(S1):S113–4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Sweeney A, Filson B, Kennedy A, Collinson L, Gillard S. A paradigm shift: relationships in trauma‐informed mental health services. BJPsych Adv. 2018;24(5):319–33 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information S1
Supporting information S2