

Abstract
Background
The COVID‐19 pandemic demanded changes in societal behavior and health care worldwide. Previous studies have compared trauma patient admissions in COVID‐19‐related lockdowns to prior years. This study describes the COVID‐19 impact on trauma patient admissions during entire 2020 at a major trauma center in Denmark.
Methods
We retrospectively analyzed trauma patients received by a trauma team and admitted at Aarhus University Hospital in 2020 compared with 2018–2019. The incidence of injuries, mechanism of injury, 30‐day mortality, and Injury Severity Score (ISS) were investigated.
Results
The incidence of minor injuries (ISS 1–15) increased by 24% in 2020 compared with 2018–2019 (incidence rate ratio 1.24 [95% CI: 1.11–1.39]). The incidence of severe injuries (ISS >15) in 2020 did not change compared with 2018–2019 (incidence rate ratio 0.97 [95% CI: 0.80–1.17]). The 30‐day mortality was similar in 2020 compared with 2018–2019. Comparing 2020 with 2018–2019, the risk ratio of traffic injuries decreased (0.90 [95% CI: 0.82–0.99]), risk ratio for fall injuries was 1.13 (95% CI: 0.97–1.30), for violence 1.13 (95% CI: 0.51–2.50), and for self‐harm 1.94 (95% CI: 0.95–3.94). During the first lockdown of 2020, trauma team activations declined from 49.5 to 42 and the risk ratio for traffic injuries was 0.74 (95% CI: 0.50–1.10) compared with the same period in 2018–2019.
Conclusion
The incidence of minor injuries increased, but the incidence of severe injuries was similar in 2020 compared with 2018–2019. Societal restrictions might alter the mechanism of injuries. The first lockdown indicated an association with reduced traffic injuries.
Keywords: COVID‐19, Denmark, injury, lockdown, pandemic, Scandinavia, trauma, trauma center
Editorial Comment.
COVID‐19 including lockdown may have had an effect on the incidence and type of trauma referrals in the same time period, according to the analysis of this cohort from a single Danish center.
1. INTRODUCTION
Since the outbreak of the disease caused by the new coronavirus SARS‐CoV‐2 (COVID‐19) in Wuhan, China, COVID‐19 has caused a pandemic and demanded changes in societal behavior and health care worldwide. 1 , 2 The Danish government instituted a full lockdown from March 13 to April 13, 2020, and a gradual lockdown in the fall of 2020. The first lockdown introduced a series of restrictions. For example, people working in noncritical jobs were sent home and encouraged to work from home for the remainder of 2020. Elderly and vulnerable persons were recommended to self‐isolate. Daycare centers, schools, universities, bars, restaurants, and entertainment industries were closed. 3 Construction and industrial production continued, but borders were closed. During the summer of 2020, gathering prohibitions and attendance restrictions were eased although a considerable proportion of the population worked from home. A gradual lockdown was imposed from 18 September 2020 and further restrictions on gatherings, attendance at work and educational facilities, bars and restaurants, social activities, etc. The second full lockdown was instituted on 16 December 2020. A timeline of COVID‐19‐related events and restrictions in Denmark is available in Table S1. 4 Previous studies have compared trauma patient admissions in COVID‐19‐related lockdowns to a control period in prior years. 5 , 6 , 7 , 8 One of the first COVID‐19 studies on trauma patients, by Christey et al., reported data from New Zealand. They found a 43% decrease in trauma admissions during lockdown compared with the same period in 2019. 6 Waseem et al. published a scoping review in November 2020 and found a global reduction in trauma admissions and a change in trauma mechanisms that differed by county. 9 Olding et al. reported a 35% decrease in trauma admissions and a significant increase in self‐harm cases in the United Kingdom. 8 Additionally, Ishii et al., in a study from Japan, found a 45% decrease in trauma‐related surgical procedures with the exception of an increase in hip fracture surgery. 7 A recent study in Finland by Riuttanen et al. found no significant difference in the incidence of severe injuries during the lockdown. 10 Although there have been several studies describing the effect on the trauma of the first COVID‐19 wave, reports describing the effect of reopening the society and the second wave are scarce, as are studies from Scandinavian countries. The aim of the present study is to describe trauma patients during 2020 at a major trauma center in Denmark and to compare it with 2018–2019. We will further investigate patients admitted in the first lockdown in a subgroup analysis and compare them with an equivalent period in 2018–2019.
2. METHODS
This was a retrospective cohort study at a major trauma center comparing the incidence of injuries, severity, mechanism of injury, and 30‐day mortality during the COVID‐19 pandemic in the year 2020 with the years 2018–2019. The STROBE guidelines were followed. 11
2.1. Setting
Aarhus University Hospital Trauma Center (AUH‐TC) is one of the four major trauma centers in Denmark and admits approximately 600 patients annually through trauma team activations, more than 150 of which have an Injury Severity Score (ISS) >15. AUH‐TC is a tertiary trauma unit and receives all trauma patients from Aarhus Municipality (population 350,000) along with major trauma, neurotrauma, thorax trauma, jaw surgery, and vascular injuries from the central region of Denmark (1.3 million inhabitants). The regional trauma system consists of four acute‐care referral hospitals in addition to AUH‐TC. Emergency medical services in the central region of Denmark comprise 69 ambulances (staffed by paramedics and emergency medical technicians) and 10 rapid response vehicles (staffed by anesthesiologists and paramedics). In addition, the region is covered by the national helicopter emergency service consisting of four helicopters (staffed with anesthesiologists, paramedics, and a pilot).
2.2. Patients
Patients of all ages admitted by trauma team activation (TTA) to AUH‐TC with ISS >0 were included. TTA is requested by the prehospital unit according to predefined criteria (Appendix, Table S2). No changes of the TTA criteria or the organization of AUH‐TC were made during the study period 2018–2020. TTA involves a minimum of 10–12 professionals, including an emergency physician, orthopedic surgeon, anesthesiologist, nurse anesthetist, trauma nurse, medical laboratory technologist, radiographer, medical secretary, support staff, and physicians from relevant medical specialties. Minor injuries without TTA in the emergency department (ED) and trauma patients treated at acute‐care referral hospitals were not included. Patients with major trauma initially admitted to an acute‐care referral hospital with a secondly transfer to AUH‐TC within 24 h were included.
Inclusion criteria
Patients of all ages admitted by TTA to AUH‐TC.
Injury Severity Score >0.
Patients with major trauma transferred to AUH‐TC within 24 h.
Exclusion criteria
42 noncitizens with missing or incomplete Civil Registration System numbers were excluded from mortality analysis.
2.3. Data
Data collection was completed using a regional trauma registry (AUH‐TR). Data in AUH‐TR are recorded by hospital administrative staff in real time as the patient is treated in the resuscitation room and follows the Utstein Trauma Template. 12 Data include age, sex, timeline, and mechanism of injury. Mechanism of injury is subcategorized into road traffic collision, motorcycle, scooter, bicycle, fall, horse, pedestrian, violence, stabbing, gunshot, self‐harm, and other cause. The category of fall injuries includes falls from all heights. The category of other causes includes crushing between objects, work injuries, and sports injuries. Patients included in this study were divided into two cohorts according to timeframe:
-
1
Cohort 2020: these include the first lockdown and reopening in 2020 (1 January to 31 December 2020).
-
2
Cohort 2018–2019: equivalent control periods in 2018 and 2019 (1 January 2018 to 31 December 2019).
Subgroup analysis of lockdown cohorts to assess the impact of the first lockdown:
-
3
First lockdown (13 March to 13 April 2020).
-
4
Reference periods in 2018 (13 March to 13 April 2018) and 2019 (13 March to 13 April 2019).
A COVID‐19 timeline for 2020 in Denmark is available in Table S1. 4 The second COVID‐19‐related lockdown reintroduced societal restrictions gradually from September 2020 to December 2020 (Table S1). As the number, demography, and mechanism of injuries vary through time, we selected the reference incidence of injuries based on a 2‐year average (2018–2019).
2.4. Outcome
After the management and treatment of the patient, a trauma score is calculated. Danish trauma centers use the ISS which is based on the Abbreviated Injury Scale (AIS) for each anatomical region. 13 , 14 ISS scores are coded by AIS‐trained physicians or medical students. ISS scores are validated by sample checking of consistency. Thirty‐day mortality data were extracted from the patient's medical record using the Danish Civil Registration number. The Danish Civil Registration System contains a vital status for all Danish citizens and noncitizens who take up residence in Denmark. 15
2.5. Statistics
Ordinal data are reported as numbers and percentages. Continuous data are reported as mean and standard deviation for normally distributed data and median and quartiles for non‐normal distributed data. Comparison of the incidence of injuries between time periods was calculated using the incidence rate ratio. Patients living in the catchment area according to Danish Statistics contributed with one person‐year and were used as denominator in incidence rate calculations. 16 Risk ratios were calculated to compare the mechanism of injury between 2020 and 2018–2019. Missing values were noted as percentages in the footnotes accompanying tables. STATA version STATA/IC 16.1 (StataCorp. 2019. Texas, USA) was used for all statistical analyses. A two‐sided p value of <.05 was considered statistically significant.
2.6. Ethics and approvals
This study was a registry study. Trial registration or approval from Ethics Committee was not required according to Danish law by the retrospective and anonymized form of data. The study was approved by the hospital board of directors.
3. RESULTS
3.1. 2018–2019 vs. 2020
Patient characteristics and outcomes are seen in Table 1. In 2020, 684 trauma patients were admitted by TTA at AUH‐TC compared with 616 and 543 in 2018 and 2019, respectively (Table 1). The incidence of minor injuries (ISS 1–15) per 100,000 inhabitants during 2020 was 148.3 (95% CI: 135.8–161.6) compared with 119.6 (95% CI: 111.5–128.0) in 2018–2019 (Table 2, Figure 1). The incidence of minor injuries increased by 24% (incidence rate ratio 1.24 [95% CI: 1.11–1.39]). The incidence of severe injuries (ISS >15) per 100,000 inhabitants during 2020 was 12.4 (95% CI: 10.6–14.5) compared with 12.9 (95% CI: 11.5–14.3) in 2018–2019 (Table 2, Figure 2). The incidence of severe injuries did not change in 2020 compared with 2018–2019 (incidence rate ratio 0.97 [95% CI: 0.80–1.17]). The second COVID‐19 wave and accompanying gradual lockdown in the autumn of 2020 did not reduce the incidence of trauma patients considering that the monthly incidence of trauma patients remained elevated throughout 2020 after the first lockdown (Table S1, Figures 1 and 3).
TABLE 1.
Patient characteristics
|
2018–2019, average n total = 1,159 average n = 579.5 |
2020 n = 684 |
|||
|---|---|---|---|---|
| Gender, Male n (%) | 405.5 | (70.0) | 467 | (68.3) |
| Age, Mean (SD) | 42.7 | (23.0) | 43.6 | (23.1) |
| ISS >15, n (%) | 169.5 | (29.2) | 165 | (24.1) |
| ISS, Median (Q1–Q3) | 9 | (2–17) | 6 | (1–14) |
| 30‐day mortality, n (%) | 36 | (6.4) a | 40 | (5.9) a |
Abbreviations: ISS, Injury Severity Score; Q1, 25th quartile; Q3, 75th quartile; SD, Standard deviation.
20, 15, and 7 patients were lost to follow up in 2018, 2019, and 2020, respectively.
TABLE 2.
Incidence of trauma patients with minor injuries (ISS 1–15) per 100,000 inhabitants in Aarhus Municipality and severe injuries (ISS >15) per 100,000 inhabitants in the central region of Denmark
| 2018–2019 | 2020 | ||||||
|---|---|---|---|---|---|---|---|
| n | Mean population | Incidence (95% CI) | n |
Mean population |
Incidence (95% CI) | Incidence rate ratio (95% CI) | |
| ISS 1–15 | 410 | 342,877 a | 119.6 (111.5–128.0) | 519 | 349,983 a | 148.3 (135.8–161.6) | 1.24 (1.11–1.39) |
|
FL ISS 1–15 |
36 | 10.5 (8.2–13.2) | 32 | 9.1 (6.3–12.9) | 0.87 (0.56–1.34) | ||
| ISS >15 | 169.5 | 1,317,137 b | 12.9 (11.5–14.3) | 165 | 1,326,340 b | 12.4 (10.6–14.5) | 0.97 (0.80–1.17) |
|
FL ISS >15 |
13.5 | 1.0 (0.7–1.5) | 10 | 0.8 (0.4–1.4) | 0.74 (0.32–1.57) | ||
Abbreviations: CI, confidence interval; FL, first lockdown; ISS, injury severity score.
The catchment area for minor injuries is Aarhus Municipality. The catchment area for severe injuries is the central region of Denmark.
Population in Aarhus Municipality.
Population in the central region of Denmark.
FIGURE 1.

Number of monthly trauma patients with ISS >0 in years 2018–2019 and 2020
FIGURE 2.

Number of monthly trauma patients with ISS >15 in 2018–2019 and 2020
FIGURE 3.

Number of monthly trauma patients in 2018, 2019, and 2020. The mean number of trauma patients is plotted for 2018, 2019, and 2020
Median ISS of all trauma patients is seen in Figure 4. The 30‐day mortality was 5.9% in 2020 compared with 6.4% in 2018–2019 (Table 1).
FIGURE 4.
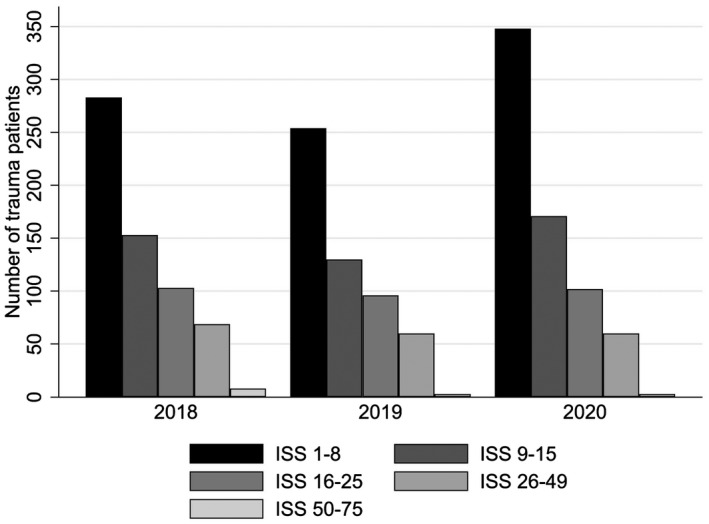
Distribution of Injury Severity Score (ISS) in 2018, 2019, and 2020
The risk ratio of traffic injuries combined decreased in 2020 (0.90 [95% CI: 0.82–0.99]) compared with 2018–2019 (Table 3 and Figure 5) and was mainly driven by a reduction in risk ratio for motorcycle injuries (0.50 [95% CI: 0.30–0.83]) and pedestrian injuries (0.49 [95% CI: 0.27–0.89]). The risk ratio of fall injuries, violence, and self‐harm can be seen in Table 3 and Figure 5. The number of trauma patients with ISS >0 transferred to AUH‐TC within 24 hours was 50, 42, and 76 in 2018, 2019, and 2020, respectively.
TABLE 3.
Mechanism of injury in 2020 compared with 2018–2019
| 2018–2019, average n (%) | 2020, n (%) | Risk ratio (95% CI) | |
|---|---|---|---|
| Total | 579.5 | 684 | |
| Traffic injuries combined a | 322 (55.6) | 343 (50.2) | 0.90 (0.82–0.99) |
| Road traffic collision | 165.5 (28.6) | 206 (30.1) | 1.05 (0.91–1.22) |
| Motorcycle | 32 (5.5) | 19 (2.8) | 0.50 (0.30–0.83) |
| Scooter | 15 (2.6) | 20 (2.9) | 1.13 (0.65–1.97) |
| Bicycle | 85.5 (14.8) | 84 (12.3) | 0.83 (0.65–1.06) |
| Fall | 159.5 (27.5) | 212 (31.0) | 1.13 (0.97–1.30) |
| Horse | 18 (3.1) | 18 (2.6) | 0.85 (0.48–1.48) |
| Pedestrian | 24 (4.1) | 14 (2.1) | 0.49 (0.27–0.89) |
| Violence | 7.5 (1.3) | 10 (1.5) | 1.13 (0.51–2.50) |
| Stabbing | 23 (4.0) | 23 (3.4) | 0.85 (0.52–1.39) |
| Gunshot | 5 (0.9) | 6 (0.9) | 1.02 (0.37–2.78) |
| Self‐harm | 7 (1.2) | 16 (2.3) | 1.94 (0.95–3.94) |
| Other cause b | 37.5 (6.5) | 56 (8.2) | 1.27 (0.91–1.77) |
Abbreviation: CI, confidence interval.
The risk ratio with a 95% confidence interval (CI) was calculated between 2020 and 2018–2019.
Traffic injuries combined include road traffic collisions, motorcycle, scooter, bicycle, and pedestrian injuries.
Other causes include crushing between objects, work injuries, and sports injuries.
FIGURE 5.

Mechanism of injuries in 2020 compared with 2018–2019. RTC, road traffic collision
3.2. The first lockdown in 2020 (13 March to 13 April 2020)
The total number of trauma patients decreased to 42 patients in the first lockdown of 2020 from 49.5 patients in the equivalent period in 2018–2019 (Table 4). However, we did not detect statistically significant changes in incidence rate ratios in the first lockdown compared with reference periods (Table 2). The risk ratio of traffic injuries combined was 0.74 (95% CI: 0.50–1.10) in the first lockdown in 2020 compared with reference periods in 2018–2019.
TABLE 4.
Mechanism of injury in the first lockdown 2020 compared with reference periods in 2018–2019 (13 March to 13 April)
| Mechanism of injury | 2018 and 2019, average n (%) | 2020, n (%) | Risk ratio (95% CI) |
|---|---|---|---|
| Total | 49.5 | 42 | |
| Traffic injuries combined a | 28.5 (57.6) | 18 (42.9) | 0.74 (0.50–1.10) |
| Fall | 13.5 (27.3) | 14 (33.3) | 1.22 (0.72–2.09) |
| Horse | 2 (4.0) | 4 (9.5) | 2.36 (0.62–8.98) |
| Violence | 0.5 (1.0) | 0 (0.0) | No cases in FL |
| Stabbing | 1.5 (3.0) | 2 (4.8) | 1.57 (0.27–9.06) |
| Gunshot | 1 (2.0) | 0 (0.0) | No cases in FL |
| Self‐harm | 0 (0.0) | 0 (0.0) | No cases in FL |
| Other cause b | 2.5 (5.1) | 4 (9.5) | 1.89 (0.53–6.68) |
Abbreviations: CI, confidence interval; FL, first lockdown.
The risk ratio with a 95% confidence interval (CI) was calculated between 2020 and 2018–2019.
Traffic injuries combined include road traffic collisions, motorcycle, scooter, bicycle, and pedestrian injuries.
Other causes include crushing between objects, work injuries, and sports injuries.
4. DISCUSSION
This study elaborates on the impact of societal restrictions and changes in behavior on trauma patient admissions during the COVID‐19 pandemic in the central region of Denmark. The incidence of minor injuries increased and the mechanism of injured changed in 2020 compared with 2018–2019. Conversely, the incidence of severe injuries with ISS >15 and 30‐day mortality did not change in 2020 compared with 2018–2019. There was a reduced risk of traffic injuries during the first lockdown in 2020 compared with the same period in 2018–2019, but the confidence intervals were wide and included 1.00. In addition, other differences cannot be excluded.
The risk ratio for all traffic injuries combined decreased significantly in 2020 compared with 2018–2019 (0.90 [95% CI: 0.82–0.99]). This finding is consistent with the trend in a preliminary report from Danish Road Directorate showing a 22.1% decrease in traffic deaths and a 10.3% decrease in traffic injuries in 2020 compared with 2019. 17 The 30‐day mortality in our study was 5.9% in 2020 compared with 6.4% in 2018–2019. However, our data include deaths from all injuries and deaths at the scene are not included in our registry. Additionally, we compared 2020 to data from both 2018 and 2019. The number of patients who sustained pedestrian injuries decreased significantly in 2020 which could explain some of the reduction in traffic deaths registered by the Danish Road Directorate. Similar decreases in traffic injuries during the first lockdown were observed in Spain, Australia, and the United Kingdom. 5 , 18 , 19
Fall injuries increased numerically but not statistically in 2020 compared with the average of 2018–2019 (risk ratio: 1.13 [95% CI: 0.97–1.30]). Yearly increases in fall injuries follow a long‐term trend of changes in demographics and increases in low falls. 20 At a major trauma center in London, falls <1.5 m increased from 49% to 58% and falls >1.5 m increased from 5% to 10% during the first lockdown. 21 Increases in fall from heights in lockdown were also reported in other studies. 5 , 10 Staunton et al. reported an increase in falls at home from 33% to 59% and an increase in falls from a ladder at home from 4% to 7% in lockdown in Ireland. 22 Lockdown‐related increases in incidents at home were found by numerous studies. 5 , 22 , 23 Do it yourself, repair, or garden work may also have contributed to the increase in trauma patients in 2020.
In 2020, the risk ratio for violence against others was 1.13 (95% CI: 0.51–2.50) and for self‐harm 1.94 (95% CI: 0.94–3.94) compared with 2018–2019 but the numbers were low, and the confidence intervals were wide and included 1.00. Rohde et al. found steep increases in COVID‐19 and pandemic‐related psychopathology in the central region of Denmark during the first lockdown, suggesting that social isolation can worsen psychiatric symptoms. 24 Self‐harming patients are routinely admitted to the ED without TTA, hence the true increase in suicide attempts and self‐harm might be underestimated in this study. Similar studies have found increased self‐harm and violence during COVID‐related lockdowns in France, Ireland, Korea, and the United Kingdom. 8 , 22 , 23 , 25 Long‐term consequences of societal restrictions and isolation may be prevalent.
When focusing on trauma admissions in the first lockdown, Waseem et al. published a scoping review including 57 studies on trauma patients during national COVID‐19‐related lockdowns compared with previous years and found a global reduction in trauma admissions ranging from 20.3% to 84.6%. 9 In their review, the mechanism of injury analysis showed a lower proportion of traffic injuries and increases in assault and incidents at home during the lockdown. A nationwide study from Norway compared all injuries from a national registry of emergencies in the 3 weeks of lockdown to three prior weeks in 2020 and found a 43.4% reduction in overall admissions. 26 Our numerical but not statistically significant reduction in trauma admissions in the first month of lockdown was smaller than at other major trauma centers. The absolute decrease of trauma patients (7.5 patients) and traffic injuries combined (10.5 patients) were limited and therefore hampers interpretation. A possible explanation for this could be that fewer restrictions were imposed in Denmark compared with other countries. 5 , 7 , 27 Comparable with our results, the incidence of severe injuries (ISS >15) in Finland 10 and major injuries (ISS >12) in Australia 19 were the same during lockdown compared with earlier years.
The overall increase in trauma patients is predominantly attributable to a significant increase in minor injuries with ISS 1–15. A possible cause for the seasonal increase in the incidence of minor injuries during the summer of 2020 could be the imposition of travel restrictions and more people staying in Denmark instead of vacationing abroad. On the other hand, there was a decrease in tourists from abroad. 28 In Denmark, the incidence of severe injuries appears to have been unaffected by the COVID‐19 pandemic despite societal restrictions, in contrast to the increase in minor injuries. Mechanism of injuries in 2020 changed compared with 2018–2019, however, further research is needed to study alterations in demographics and trauma epidemiology over time in a nationwide study. Societal restrictions might have been the explanation for the difference in mechanism of injuries. Future studies of traffic and fall prevention are needed.
4.1. Strengths and limitations
Strengths of this study are that the percentage of patients lost to follow up is low and most major trauma patients in the central region of Denmark (22% of the Danish population) are admitted to our trauma center. Furthermore, this study examined the entire 2020 compared with previous studies with shorter study periods. Two years (2018–2019) were chosen as controls to minimize short‐term yearly fluctuations in trauma admissions. Additional years were not included to avoid influence from long‐term changes in the incidence of injuries and demographics over time. At the organizational level, AUH‐TC and the regional trauma hospitals provided full trauma service during the pandemic with no scarcity of resources as feared. COVID‐19 suspected trauma patients were treated as all other trauma patients and only minor delays due to personal protection equipment were reported. Even though the TTA criteria (Table S2) and organization of trauma care did not change in the study period (2018–2020), we cannot rule out that emergency physicians could alter the threshold of TTA resulting in an increase in minor injuries in 2020. The best‐fitting AIS was chosen by consensus when patients sustained injuries with ambiguous interpretations. We do not expect any misclassification of ISS scores to affect the results. A limitation is that fewer noncitizens lacking a Civil Registration System number were lost to follow up in the 2020 group (seven patients, four with ISS >15) compared with the 2018–2019 group (mean 17.5 patients, mean 6.5 patients with ISS >15); thus 30‐day mortality might be underestimated in the 2018–2019 control group. This was a single‐center study and the incidence of trauma patients with ISS >15 was limited. The percentage of patients older than 60 years was lower at AUH‐TC compared with other major Danish trauma centers. 13 , 29 Nonetheless, the demographics and landscape are similar to other regions in Denmark and we presume that these results are generalizable to the Danish population. The assessment of COVID‐19’s effect on trauma admissions may be hampered by weather conditions, registry completeness, and long‐term trends in the trauma patient population.
5. CONCLUSION
In the COVID‐19 pandemic year 2020, the incidence of minor injuries increased, but the incidence of severe injuries was similar compared with 2018–2019. Societal restrictions might alter the mechanism of injury. The study indicated that the first COVID‐19‐related lockdown was associated with a reduction in traffic injuries.
CONFLICT OF INTEREST
The authors have nothing to declare.
AUTHOR CONTRIBUTIONS
FT, HK, JF, AHS, and NR designed this study. FT, HK, and JF contributed to data collection. FT, HK, and JF performed the data analysis and interpretation of data. FT wrote the manuscript. HK, JF, NR, and AHS critically revised the manuscript. All authors approved the final manuscript.
Supporting information
Table S1‐S2
ACKNOWLEDGMENTS
Funding: Department funding only.
Trier F, Fjølner J, Raaber N, Sørensen AH, Kirkegaard H. Effect of the COVID‐19 pandemic at a major Danish trauma center in 2020 compared with 2018–2019: A retrospective cohort study. Acta Anaesthesiol Scand. 2022;66:265–272. doi: 10.1111/aas.13997
REFERENCES
- 1. Wang D, Hu BO, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel Coronavirus‐infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061‐1069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. WHO . WHO announces COVID‐19 outbreak a pandemic. World Health Organisation. 2020. https://www.euro.who.int/en/health‐topics/health‐emergencies/coronavirus‐covid‐19/news/news/2020/3/who‐announces‐covid‐19‐outbreak‐a‐pandemic. Accessed 04 July 2021. [Google Scholar]
- 3. The Danish Goverment . Pressemøde 11. marts i Spejlsalen (Danish). 2020. https://www.regeringen.dk/nyheder/2020/pressemoede‐11‐marts‐i‐spejlsalen/. Accessed 04 July 2021.
- 4. Think Europa . Timeline for Corona crisis: What happened and when? 2021. http://thinkeuropa.dk/politik/tidslinje‐over‐coronakrisen‐hvad‐skete‐der‐og‐hvornaar. Updated 28‐06‐2021. Accessed 04 July 2021.
- 5. Rajput K, Sud A, Rees M, Rutka O. Epidemiology of trauma presentations to a major trauma centre in the North West of England during the COVID‐19 level 4 lockdown. Eur J Trauma Emerg Surg. 2021;47(3):631‐636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Christey G, Amey J, Campbell A, Smith A. Variation in volumes and characteristics of trauma patients admitted to a level one trauma centre during national level 4 lockdown for COVID‐19 in New Zealand. N Z Med J. 2020;133(1513):81‐88. [PubMed] [Google Scholar]
- 7. Ishii K, Kurozumi T, Suzuki T, et al. Impact of the COVID‐19 pandemic on a trauma center of a university hospital in Japan. J Orthop Sci. 2020. [Epub ahead of print]. doi: 10.1016/j.jos.2020.11.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Olding J, Zisman S, Olding C, Fan K. Penetrating trauma during a global pandemic: changing patterns in interpersonal violence, self‐harm and domestic violence in the Covid‐19 outbreak. Surgeon. 2021;19(1):e9‐e13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Waseem S, Nayar SK, Hull P, et al. The global burden of trauma during the COVID‐19 pandemic: a scoping review. J Clin Orthop Trauma. 2021;12(1):200‐207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Riuttanen A, Ponkilainen V, Kuitunen I, Reito A, Sirola J, Mattila VM. Severely injured patients do not disappear in a pandemic: incidence and characteristics of severe injuries during COVID‐19 lockdown in Finland. Acta Orthop. 2021;92(3):249‐253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. Epidemiology. 2007;18(6):805‐835. [DOI] [PubMed] [Google Scholar]
- 12. Ringdal KG, Coats TJ, Lefering R, et al. The Utstein template for uniform reporting of data following major trauma: a joint revision by SCANTEM, TARN, DGU‐TR and RITG. Scand J Trauma Resusc Emerg Med. 2008;16:7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Baker SP, O'Neill B. The injury severity score: an update. J Trauma. 1976;16(11):882‐885. [DOI] [PubMed] [Google Scholar]
- 14. Copes WS, Champion HR, Sacco WJ, Lawnick MM, Keast SL, Bain LW. The injury severity score revisited. J Trauma. 1988;28(1):69‐77. [DOI] [PubMed] [Google Scholar]
- 15. Pedersen CB. The danish civil registration system. Scand J Public Health. 2011;39(7 Suppl):22‐25. [DOI] [PubMed] [Google Scholar]
- 16. Danish Statistics . Population statistics. 2021. https://www.dst.dk/da/Statistik/emner/befolkning‐og‐valg/befolkning‐og‐befolkningsfremskrivning/folketal. Accessed 04 August 2021.
- 17. The Danish Road Directorate . Injuries December 2020. 2021. https://www.vejdirektoratet.dk/udgivelse/ulykkestal‐december‐2020. Updated 22‐01‐2021. Accessed 04 July 2021.
- 18. Nuñez JH, Sallent A, Lakhani K, et al. Impact of the COVID‐19 pandemic on an emergency traumatology service: experience at a tertiary trauma centre in Spain. Injury. 2020;51(7):1414‐1418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Jacob S, Mwagiru D, Thakur I, Moghadam A, Oh T, Hsu J. Impact of societal restrictions and lockdown on trauma admissions during the COVID‐19 pandemic: a single‐centre cross‐sectional observational study. ANZ J Surg. 2020;90(11):2227‐2231. [DOI] [PubMed] [Google Scholar]
- 20. Kehoe A, Smith JE, Edwards A, Yates D, Lecky F. The changing face of major trauma in the UK. Emerg Med J. 2015;32(12):911‐915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Park C, Sugand K, Nathwani D, Bhattacharya R, Sarraf KM. Impact of the COVID‐19 pandemic on orthopedic trauma workload in a London level 1 trauma center: the “golden month”. Acta Orthop. 2020;91(5):556‐561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Staunton P, Gibbons JP, Keogh P, Curtin P, Cashman JP, O'Byrne JM. Regional trauma patterns during the COVID‐19 pandemic. Surgeon. 2021;19(2):e49‐e52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Pichard R, Kopel L, Lejeune Q, Masmoudi R, Masmejean EH. Impact of the COronaVIrus disease 2019 lockdown on hand and upper limb emergencies: experience of a referred university trauma hand centre in Paris, France. Int Orthop. 2020;44(8):1497‐1501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Rohde C, Jefsen OH, Nørremark B, Danielsen AA, Østergaard SD. Psychiatric symptoms related to the COVID‐19 pandemic. Acta Neuropsychiatr. 2020;32(5):274‐276. [DOI] [PubMed] [Google Scholar]
- 25. Chang YR, Kim KM, Kim HJ, et al. Impacts of social distancing during the COVID‐19 outbreaks in korea: level 1 trauma center data of domestic incidents and intentional injury. Osong Public Health Res Perspect. 2020;11(6):345‐350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Ohm E, Hauge LJ, Madsen C, Grøholt EK, Evensen M, Reneflot A. Impact of the COVID‐19 pandemic on the treatment of injuries during lockdown in Norway. Scand J Public Health. 2021;49(7):689‐696. [DOI] [PubMed] [Google Scholar]
- 27. Navsaria PH, Nicol AJ, Parry CDH, Matzopoulos R, Maqungo S, Gaudin R. The effect of lockdown on intentional and nonintentional injury during the COVID‐19 pandemic in Cape Town, South Africa: a preliminary report. S Afr Med J. 2020;13183. [PubMed] [Google Scholar]
- 28. VisitDenmark . Aktuelle overnatningstal (Danish). 2021. https://www.visitdenmark.dk/corporate/videncenter/aktuelle‐overnatningstal. Accessed 04 July 2021.
- 29. Danish Trauma Registry . Annual report 2018. 2018. https://www.sundhed.dk/content/cms/19/97019_dansktraumeregister‐aarsrapport_2018_offentligversion.pdf. Updated October 2019. Accessed 04 August 2021.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1‐S2