

Abstract
The global COVID‐19 outbreak has put the human race's distress tolerance abilities to the test. And, the distress experienced getting worse with each pandemic wave; however, the more flexible the person, the greater the chance of surviving. Thus, the current study aimed to examine the mediating role of personalized psychological flexibility (PPF) in the link between distress intolerance to psychological distress during the fourth wave of the pandemic in Iran. A total of 576 individuals (Meanage 34.80, ±10.9, females 55.6%) took part in the online survey. In this national sample, PPF partially played a role in mediating the association mentioned above. Interestingly, this mediation was independent of demographic factors (age, gender, marital status, and educational level) and fear of COVID‐19, mindfulness, and satisfaction with life. So, despite the mentioned variables, accepting and using unpleasant emotions as fuel to achieve valued goals rather than avoiding them would mitigate the psychological distress during the pandemic. Consequently, public health services can aim to provide psychological flexibility enhancing interventions to decay COVID‐19‐related mental distress.
Keywords: COVID‐19, distress intolerance, pandemic, psychological distress, psychological flexibility
Key Practitioner Message.
Personalized psychological flexibility can be implemented into an intervention to decay mental distress due to the COVID‐19 pandemic.
Accepting and using unpleasant emotions as fuel to achieve valued goals rather than avoiding them would mitigate the psychological distress during the pandemic.
Independent of demographic factors (age, gender, marital status, and educational level) and fear of COVID‐19, mindfulness, and satisfaction with life, personalized psychological flexibility underlies the association between distress intolerance and psychological distress.
Distress intolerance and personalized psychological flexibility explained 52% of the variance in psychological distress, increasing to 66% after controlling for demographics, fear of COVID‐19, satisfaction with life, and mindfulness.
1. INTRODUCTION
An unexpected event from the end of 2019 until this moment has become a global public concern across the world, which has overshadowed all aspects of human life. While almost every government has adopted various forms of guidelines and strategies to expose this issue (e.g., Abouk & Heydari, 2020; Dawson & Golijani‐Moghaddam, 2020; Qiu et al., 2020), the world is still suffering from this disease. According to the reports of the World Health Organization (WHO; World Health Organization, 2021), the Coronavirus disease has infected over 243 million people and caused over 4.9 million deaths at the time of writing (October 2021). In Iran, over 5 million people have received a definitive diagnosis of the COVID‐19, and the total number of deaths has reached over 125 thousand (Ministry of Health and Medical Education of Iran, 2021).
According to the existing evidence, the current pandemic and quarantine resulted in the experience of moderate to high levels of indices of psychological distress (i.e., anxiety, depression and stress; e.g., Daly & Robinson, 2021; Dawson & Golijani‐Moghaddam, 2020; Wang et al., 2020; Zhang et al., 2020). Barzilay et al. (2020) with a large sample study (n = 3042), reported that people experience high rates of COVID‐19 related worry and stress, anxiety, and depression during the COVID‐19 pandemic. In a systematic review, Yasegnal (2021) have counted anxiety and distress as common psychological outcomes of the current pandemic. Also, nationwide surveys have shown almost high levels of psychological distress symptoms across different populations and different types of workers during the pandemic, for example among Italians, Germans and Chinese people (Akbari, Spada, et al., 2021; Brailovskaia et al., 2021; Busch et al., 2021; Mansueto, Lopes, et al., 2021; Mazza et al., 2020; Qiu et al., 2020). In accordance with these results, Karimi et al. (2020) in a systematic review, found moderate to high levels of stress, anxiety, depression, and mental distress among Iranians.
What is more worrying is that the rapid spread of this virus has reached such a level that the fourth wave of the virus outbreak in Iran has started since the end of March 2021. Under prolonged stressful conditions like the lockdown, which can lead to loss of connection with others and social support sources, so finding the importance of personal protective variables for individuals, people may experience increased levels of psychological distress (Losada‐Baltar et al., 2021).
1.1. Distress intolerance with psychological distress
Distress tolerance is conceptualized by Simons and Gaher (2005) as one's capacity to resist negative and undesirable psychological conditions, and distress intolerance is defined on the opposite side. It is a subjective inability to tolerating negative emotions and physical states (McHugh & Otto, 2012). Distress (in)tolerance is known as a stable construct (Kiselica et al., 2014). There is growing empirical support for the associationbetween distress intolerance and psychological distress and its indices of (i.e., anxiety, depression, and stress; e.g., Akbari, Hosseini, et al., 2021; Keough et al., 2010; Patel et al., 2020). In a recent research, McHugh et al. (2019) found that distress intolerance correlates with poor tolerance of stressors and negative affect following the psychological stressors (here the current pandemic).
Distress intolerance as a transdiagnostic factor (Macatee et al., 2016; Patel et al., 2020), is considered as an underlying construct in a wide array of psychopathology, including depressive symptoms and worry, major depression, generalized anxiety disorder, panic disorder, hoarding disorder, PTSD symptoms, obsessive–compulsive disorder (e.g., Allan et al., 2014; Cho et al., 2021; Macatee et al., 2016; McGrew et al., 2020; Norberg et al., 2020; Robinson & Freeston, 2014). Distress tolerance is considered a meta‐emotion construct, and a higher‐order construct (Simons & Gaher, 2005). Given these evidences, this meta‐emotion vulnerability factor is considered as the predictive factor in the current study. We expect a direct and an indirect link between distress intolerance and psychological distress.
1.2. The linkage between personalized psychological flexibility with psychological distress
A growing body of literature shows that psychological flexibility associates with psychological distress and its indicators (Chong et al., 2020; Grégoire et al., 2020; Kroska et al., 2020; Tyndall et al., 2018). Psychological flexibility is conceptualized by Hayes et al. (2006, p. 7) as the ‘ability to contact the present moment more fully as a conscious human being and to change or persist in behavior when doing so serves valued ends’. Psychological flexibility is an individual's ability to detect and adapt to different situational requirements in following long‐term goals (Dawson & Golijani‐Moghaddam, 2020). Psychological flexibility includes 6 main components: 1. acceptance, 2. self as context, 3. cognitive defusion, 4. being present, 5. Contact with values and 6. committed action (Hayes et al., 2006). Recently, Kashdan et al. (2020), have conceptualized a new concept called personalized psychological flexibility. This well‐established concept refers to adaptive reactions to any existing distress and obstacles in pursuit of completely personalized meaningful goals. Personalized psychological flexibility describes how people avoid, accept, and harness the discomforts of their individual goals.
Dawson and Golijani‐Moghaddam (2020) found a negative association between psychological flexibility and distress; which comprises depression, anxiety, and COVID‐19 related distress and worry. According to the findings by Bhambhani et al. (2020) psychological flexibility mediated the relation between experiencing sexual racism and depression, anxiety, and stress (i.e., psychological distress) after controlling for demographic characteristics. More recent studies by Kashdan et al. (2020) and Akbari, Disabato, et al. (2021) found a negative association between personalized psychological flexibility and distress intolerance. One candidate mediator in our belief is personalized psychological flexibility. We hypothesized that this superior new factor would mediate the association between a meta‐emotional vulnerability, distress intolerance and psychological distress.
1.3. Aim of the current study
After the beginning of the fourth wave was confirmed by official sources in Iran, restrictions such as isolation were once again seriously considered. In circumstances such as this, people experience negative emotional impacts like symptoms of psychological distress (Brooks et al., 2020; Xiao et al., 2020).
The current study conducted in this stressful time to explore central keys in psychological distress and response to this question that does personalized psychological flexibility play a mediational role in the relation between distress intolerance and psychological distress? It's notable that in respect to this reality that most of our knowledge (or our perception) of psychological flexibility is based on the acceptance and action questionnaire (AAQ and AAQ‐II; which aren't without deficits), we have especially focused on personalized psychological flexibility (for review see Doorley et al., 2020).
Overall, the current study aims to investigate the direct route between distress intolerance and psychological distress, also the indirect route with the mediation of a new well‐documented construct (personalized psychological flexibility), after controlling for demographic variables, fear of Covid‐19, life satisfaction, and mindfulness.
2. METHOD
2.1. Participants and procedure
A sample of 576 participants (M age = 34.80 ± 10.9 years) from the general population of Iran was recruited to participate in the present study. We have gathered data from people who are at least 16 years old, through sharing our invitation link in digital apps. As stated earlier, in the present study, participants were invited to participate via advertisements in digital apps. At the end of the consent form, a link containing explanations about the purpose of the current research, how to complete the questionnaires, demographic information, and a package of questionnaires was placed for the participants. All participants were assigned the provided consent form to participate in the current study. Participants were assured that their information would be kept confidential, also they were informed that the right of discontinuing the present study is accepted by the authors at any time. In order to detect careless responders, 2 additional items (i.e., attention check items; e.g., ‘Please select slightly’) were inserted in the final package of questionnaires. This option resulted in the removal of 23 careless participants, and finally, 576 were analysed. Most of the participants were female (55.6%), single (46.9%), employed (67.3%), and with bachelor degree (52.1%). Table 1 represents more additional data from participants. The current study was conducted in accordance with the 1989 Helsinki Declaration.
TABLE 1.
Demographic features and additional data of the sample (N = 576)
| N | % | ||
|---|---|---|---|
| Gender | Female | 320 | 55.6 |
| Male | 256 | 44.4 | |
| Marital status | Single | 270 | 46.9 |
| Married | 306 | 53.1 | |
| Educational level | High school | 15 | 2.6 |
| Diploma | 119 | 20.7 | |
| Advanced diploma | 23 | 4.0 | |
| Bachelor | 300 | 52.1 | |
| Master | 108 | 18.8 | |
| PhD | 11 | 1.9 | |
| Employment status | Employed | 387 | 67.3 |
| Unemployed | 189 | 32.7 | |
| Covid‐19 infection | Yes | 109 | 18.9 |
| No | 467 | 81.1 | |
| If yes: | |||
| Diagnosis based on the test | Yes | 36 | 33.0 |
| No | 73 | 67.0 | |
| Severity of Covid‐19 symptoms | Mild | 42 | 38.5 |
| Moderate | 54 | 49.5 | |
| Severe | 13 | 11.9 | |
| Hospitalization due to Covid‐19 disease | Yes | 6 | 5.5 |
| No | 103 | 94.5 | |
| Hope for the end of the epidemic and the return of life to normal condition (before the epidemic) | Not at all | 16 | 2.8 |
| Slightly | 71 | 12.3 | |
| No idea | 74 | 12.8 | |
| Somewhat hopeful | 240 | 41.7 | |
| Very hopeful | 175 | 30.4 | |
| Adherence to health protocols | Not at all | 7 | 1.2 |
| Slightly | 16 | 2.8 | |
| Somewhat | 204 | 35.4 | |
| Very much | 349 | 60.6 |
2.2. Measures
In the current study, the Persian forms of the following measures were used.
2.2.1. Depression anxiety stress Scale‐21 (DASS‐21)
Lovibond and Lovibond (1995) have developed this measure to assess various symptoms of anxiety, depression, and stress. The DSAA‐21 consists of 21 items split into 3 subscales: depression (7 items, e.g., ‘I felt that life was meaningless’), anxiety (7 items, e.g., ‘I was aware of dryness of my mouth’) and stress (7 items, e.g., ‘I tended to over‐react to situations’). The total score for subscales ranging between 0 and 21. High scores reflect high levels of depression, anxiety, or stress. Items are rated on a 4‐point Likert scale (from 0 = Did not apply to me at all to 3 = Applied to me very much). Lovibond and Lovibond (1995) found good psychometric properties. Persian form has acceptable internal consistency, convergent validity, discriminant validity and criterion validity (Asghari et al., 2008; Sahebi et al., 2005).
2.2.2. Distress tolerance scale
The DTS was developed by Simons and Gaher (2005) to assess emotional distress tolerance. The DTS comprises 15 items and 4 subscales: 1. Tolerance (e.g., ‘I can't handle feeling distressed or upset’), 2. Absorption (e.g., ‘When I feel distressed or upset, all I can think about is how bad I feel’), 3. Appraisal (e.g., ‘My feelings of distress or being upset are not acceptable’), 4. Regulation (e.g., ‘I'll do anything to stop feeling distressed or upset’). Each item is rated on a 5‐point Likert scale from 1 = Strongly agree to 5 = Strongly disagree. The total score ranges from 15 to 75, with a higher score reflecting higher tolerance of distress. One item has reverse scoring. The original version had good psychometric properties. Also, the Persian version of this scale has shown acceptable reliability and concurrent validity (Kelishadi & Yazdkhasti, 2016; Modares, 2011). In the present study, all the items are reverse scored (except one) such that high scores indicate distress intolerance.
2.2.3. Personalized psychological flexibility index
Recently, Kashdan et al. (2020) have developed a new measure of psychological flexibility to assess individual's ability to pursue their valued life goals while different obstacles may exist in the way. Participants are asked to think about their personal main goal and answer the items in the following. Notably, 4 additional items are located in this scale concerning individuals' goals, which are not scored. The PPFI comprises 15 items, and three 5‐item subscales, including avoidance (e.g., ‘When I feel discouraged, I let my commitment for this goal slide’.), acceptance (e.g., ‘I accept the setbacks when pursuing this goal’.) and harnessing (e.g., ‘I find unpleasant emotions useful for reaching this goal’.). Items are rated on a 7‐point Likert scale ranging from 1 = Strongly disagree to 7 = Strongly agree. The reliability (Cronbach's alphas = 0.77 to 0.84), test–retest reliability (over 4 and 6 months), incremental validity, and construct validity, all have confirmed for the PPFI subscales among three samples (college students, general population, and working professionals; Kashdan et al., 2020). The Persian version has demonstrated excellent psychometric properties, including internal consistency (Cronbach's alphas = 0.79 to 0.81), construct validity, and divergent validity, incremental variance (Akbari, Disabato, et al., 2021).
2.2.4. Fear of COVID‐19 scale (FCV‐19S)
This scale was developed by Ahorsu et al. (2020) to assess fear of Covid‐19. The 7 items are rated on a 5‐point scale from 1 = Strongly disagree to 5 = Strongly agree. In this measure, higher scores indicate higher levels of fear of COVID‐19. Scores can range from 7 to 35. Internal consistency, test–retest reliability, composite reliability, and concurrent validity of the FCV‐19S, all have been robustly confirmed (Ahorsu et al., 2020). The Persian version (Alizadehfard & Alipour, 2020) has shown good internal consistency (Cronbach's alpha = 0.86).
2.2.5. Satisfaction with life scale
The satisfaction with life scale (SWLS) was developed by Diener et al. (1985 ) to assess the global degree of satisfaction of life. The 5‐items of the SWLS are rated on a 7‐point Likert scale, which is ranging from 1 = Strongly disagree to 7 = Strongly agree. The SWLS presents a total score (ranging from 5 to 35), such that higher scores reflect greater satisfaction of life. Diener et al. (1985) have reported good internal consistency, temporal reliability, and test–retest reliability for this scale. The Persian version was validated by Maroufizadeh et al. (2016), showed good reliability and convergent validity.
2.2.6. Mindfulness attention awareness scale
Brown and Ryan (2003) have developed a measure to assess the frequency of mindful states over time. The mindfulness attention awareness scale (MAAS) is made up of 15 items. A 6‐point Likert scale (ranging from 1 = Almost always to 6 = Almost never) is considered for the rating of items. The MAAS presents a total score (ranging from 15 to 90), such that higher scores reflect greater mindful states. The original version (Brown & Ryan, 2003) showed a good 4‐week test–retest reliability. Ghorbani et al. (2009) have reported good psychometric properties (reliability, discriminant and concurrent validity) among a group of Iranian college students.
2.3. Data analysis
Statistical analysis was performed using version 26 of both SPSS (IBM SPSS Statistics) and Amos. First, correlations were conducted in order to test the associations between the variables of the current study. Second, the proposed model was examined through structural equation modelling. Also, the bootstrap (iteration number = 2000) was used to test for the mediational path. According to Hu and Bentler (1999) for structural equation models, the following indexes were considered for test the fit of the model: Normed Fit Index (NFI; good fit: ≥0.90); Comparative‐Fit Index (CFI; good fit: ≥0.90); Goodness of Fit Index (GFI; good fit: ≥0.90); Root‐Mean‐Square Error of Approximation (RMSEA; good fit: ≤0.06); and Standardized Root‐Mean‐Square Residual (SRMR; good fit: ≤0.08) (see Figure 1). In the current study, in addition to demographic variables, we also added a series of variables as control variables, which may impact psychological distress, including fear of Covid‐19 (Duong, 2021; Satici et al., 2020), life satisfaction (Duong, 2021; Guney et al., 2010; Kumar et al., 2016), and mindfulness (Coffey & Hartman, 2008; Parto & Besharat, 2011).
FIGURE 1.
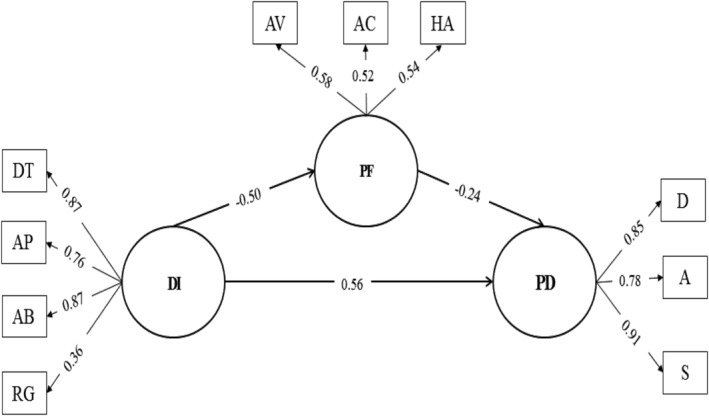
DI = distress intolerance, PF = psychological flexibility, PD = psychological distress. The partial mediation path model with standardized path coefficients. At the p < 0.05 level, all paths are significant
3. RESULTS
3.1. Data description
Table 2 displays descriptive statistics for all study variables. Internal consistency coefficients for all variables exceeded 0.70, which was acceptable and consistent with previous research. Moreover, all variables were symmetrically distributed, according to an examination of histograms, kurtosis, and skewness coefficients were in an acceptable range. According to Chou and Bentler (1995), the skewness index of the measured variables was between −0.444 and 0.557, which is within the acceptable range (±3). Also, according to Kline (2011), the kurtosis index was between −0.546 and 0.077, which is within the acceptable range (±10). As shown in Table 1, the lack of multicollinearity between variables was confirmed (r < 0.85; Kline, 2011). Furthermore, Pearson product–moment correlations revealed a fair relationship between distress intolerance, psychological distress, and psychological flexibility. Except for education level, all demographic factors were related to one of the study's conceptual model variables. These findings are consistent with the proposed mediation model.
TABLE 2.
Pearson correlations, internal consistencies, means, standard deviations and distribution of studied variables (N = 576)
| Variables | DITS | DASS | PPFI | SWLS | MAAS | COV‐fear | Age | Gender | Marital status | Job status |
|---|---|---|---|---|---|---|---|---|---|---|
| DITS | (0.86) | |||||||||
| DASS | 0.561** | (0.93) | ||||||||
| PPFI | −0.292** | −0.391** | (0.81) | |||||||
| SWLS | −0.284** | −0.502** | 0.331** | (0.84) | ||||||
| MAAS | −0.403** | −0.533** | 0.280** | 0.156** | (0.83) | |||||
| COV‐fear | 0.115** | 0.114** | −0.03 | −0.04 | −0.114** | (0.81) | ||||
| Age | −0.05 | −0.113** | 0.05 | 0.114** | 0.01 | 0.05 | — | |||
| Gender | −0.093* | −0.05 | −0.01 | −0.01 | −0.07 | −0.088* | 0.113** | — | ||
| Marital status | −0.030 | −0.129** | 0.087* | 0.214** | −0.007 | 0.027 | 0.556** | −0.058 | — | |
| Job status | −0.113* | −0.115** | 0.06 | 0.156** | −0.02 | 0.07 | 0.228** | 0.215** | −0.125** | — |
| Education level | 0.08 | 0.06 | 0.04 | −0.083* | −0.04 | −0.02 | −0.162** | −0.05 | −0.03 | −0.205** |
| Mean (SD) | 46.48 (10.88) | 19.71 (12.87) | 69.92 (11.95) | 20.72 (6.75) | 66.07 (10.37) | 17.20 (5.33) | — | — | — | — |
| Skewness | −0.057 | 0.575 | −0.117 | −0.241 | −0.444 | 0.084 | — | — | — | — |
| Kurtosis | −0.049 | −0.454 | −0.136 | −0.439 | 0.077 | −0.546 | — | — | — | — |
Note: DITS = distress intolerance, DASS = depression, anxiety, stress scale, PPFI = personalized psychological flexibility scale, SWLS = satisfaction with life scale, MAAS = mindfulness attention awareness scale, COV‐fear = fear of COVID‐19 scale. Gender (male = 1, female = 0), marital status (single = 0, married = 1), job status (unemployed = 0, employed = 1). Internal consistency coefficients are in the parentheses on the diagonal.
p < 0.01.
p < 0.05.
3.2. Structural equation modelling
All three variables, distress intolerance, psychological distress and psychological flexibility were specified as latent variables and their sub‐scales as indicators. Also, all indicators in the measurement model were defined as continuous measures of the corresponding latent variables. The measurement model's fit was not satisfactory (χ 2 = 191.504; df = 32; χ 2/df = 5.985, p < 0.001). Besides, the main indices of the goodness of fit (GFI = 0.937; CFI = 0.941; NFI = 0.93) did not exceed the cut‐off criterion of 0.95 proposed by Hu and Bentler (1999). Also, RMSEA = 0.093, was above 0.08, but SRMR = 0.06, was acceptable. The modification indices suggested adding covariance error between subscales of distress intolerance (from regulation to absorption, appraisal, and tolerance) and between subscales of psychological flexibility (from avoidance to acceptance and harnessing). Following this, the measurement model achieved the satisfactory fit indices, which are as follows (chi‐square = 97.108; df = 27; χ2/df = 3.597, p < 0.001). Also, the main indices of the goodness of fit, GFI = 0.966; CFI = 0.974; and NFI = 0.964 exceeds the criterion 0.95, and also RMSEA = 0.067 and SRMR = 0.03 was in the good range, allowing for the examination of the structural model.
3.3. Test of mediation
Three structural equations are added to the measurement model: (a) a path from distress intolerance to psychological distress, (b) a path from distress intolerance to psychological flexibility, and (c) a path from psychological flexibility to psychological distress. These paths represent the correlated antecedents of psychological distress, which are consistent with a partial mediation model. Distress intolerance has a direct effect on psychological distress (β = 0.56 [0.46, 0.66]) and an indirect effect via the mediation of psychological flexibility. Also, the fit indices were well (GFI = 0.966; CFI = 0.974; NFI = 0.964; RMSEA = 0.06; SRMR = 0.03), allowing for the examination of the mediation model.
All three computed paths were significant at the p < 0.05 level, depicted in Figure—1 with the standardized path coefficients. In the present study, bootstrap (Efron & Tibshirani, 1994) (iteration number = 2000) was used to evaluate the mediation model. That is, with a 95% confidence interval, the bootstrapping process of the indirect effects at the 2.5th and 97.5th percentiles revealed the significant mediating role of psychological flexibility (β = 0.122; B = 0.511 [0.196, 1.043], p < 0.001) in the relationship between distress intolerance and psychological distress. Furthermore, this model explained half of the variance of psychological distress (R 2 = 0.518). The direct, indirect and total effects of the model are displayed in Table 3.
TABLE 3.
Unadjusted and adjusted structural model standardized path coefficients
| Path | Direct effect | Indirect effect | Total effect |
|---|---|---|---|
| Unadjusted model | |||
| DI = > PF | −0.50 [−0.62, −0.34] | — | −0.50 [−0.62, −0.34] |
| DI = > PF = > PD | 0.56 [0.46, 0.66] | 0.12 [0.043, 0.215] | 0.68 [0.64, 0.73] |
| PF = > PD | −0.24 [−0.37, −0.11] | — | −0.24 [−0.37, −0.11] |
| Adjusted model | |||
| DI = > PF | −0.39 [−0.46, −0.21] | — | −0.39 [−0.46, −0.21] |
| DI = > PF = > PD | 0.44 [0.27, 0.44] | 0.038 [0.007, 0.094] | 0.40 [0.33, 0.47] |
| PF = > PD | −0.11 [−0.23, −0.016] | — | −0.11 [−0.23, −0.016] |
Note: DI = distress intolerance, PF = psychological flexibility, PD = psychological distress. The unadjusted model is depicted in Figure 1 and is not statistically controlled for any variables. The adjusted model is statistically controlled for demographic variables (age, gender, job and marital status and education level), fear of COVID‐19, mindfulness, and life satisfaction.
Following this, demographic variables (i. e., age, gender, job, and marital status, and education level) in addition to fear of COVID‐19, mindfulness, and life satisfaction included in the model, to see after controlling these variables whether the mediating role of psychological flexibility remain significant or not. With 2000 iterations and a 95% confidence interval, the bootstrapping process of the indirect effects at the 2.5th and 97.5th percentiles, revealed that mediating role of psychological flexibility (β = 0.038; B = 0.17 [0.29, 0.448], p = 0.036) even after controlling for those mentioned above remained significant in the relationship between distress intolerance and psychological distress. Furthermore, the adjusted model explained 14% more of the variance in psychological distress (R 2 = 0.659) than the unadjusted model.
4. DISCUSSION
Given the longevity of pandemic, lockdown, lack of extended vaccination and the fourth wave of COVID‐19 outbreak in Iran, the present study aimed to investigate the mediating role of personalized psychological flexibility in the association between distress intolerance and psychological distress. Furthermore, the mediating role of personalized psychological flexibility is also examined after incorporating the demographic factors (age, gender, marital status and education level) and psychological variables (fear of COVID‐19, mindfulness and life satisfaction), which in turn can influence the endurance of those mentioned above.
Demographically, being female was negatively associated with distress intolerance and fear of COVID‐19. Increases in age were linked with lower psychological distress and higher satisfaction with life. Being single was associated negatively with psychological distress and positively with life satisfaction. Moreover, being unemployed was negatively associated with distress intolerance, psychological distress, and satisfaction with life. And a higher educational level also was associated with lower satisfaction with life. In sum, females, elders, and unemployed people, might have less complicated and lesser challenging times during the pandemic. While women are disproportionately affected by pandemics, given the increased risk of sexual and domestic violence (Wenham et al., 2020), and elderly are most exposed to mortality and severe mental health due to the pandemic (Banerjee, 2020), the favourable result for women and elderly participants would be interpreted dynamically, as being female and elderly was associated with a greater capacity to tolerate distress. Also, unemployed individuals' situations are somewhat inconsistent with previous findings, as they underwent significant psychological distress during the pandemic (Achdut & Refaeli, 2020). It should be interpreted in light of the fact that we did not inquire about participants' reasons for being unemployed, specifically whether they lost their jobs due to the pandemic or were already unemployed before the pandemic. However, the findings may partly be explained by Iranian cultural tradition, which implies that parents support their children even as adults, suggesting that unemployed participants may have had also secure insurance or economic background.
As relates to the pandemic, distress intolerance and psychological distress were positively associated with fear of COVID‐19. This is consistent with previous research indicating that the greater one's fear of COVID‐19, the increased one's psychological distress (Satici et al., 2020), and theoretically the higher one's distress intolerances. This could be explained by the fact that COVID‐19 is an unpredictable virus, and the end date of this pandemic is unknown to anyone, turning the pandemic into a distressing chronic condition. Individuals with a greater capacity for enduring objective, emotional and physical distress (Simons & Gaher, 2005) are likely to experience less fear and distress associated with COVID‐19.
The fear of COVID‐19, however, showed a negative correlation with mindfulness and no correlation with personalized psychological flexibility. The null association can be explained in two ways. First would be the idiographic nature of measure used for psychological flexibility, which will consider individual differences, but the measure related to fear of COVID‐19 is not an idiographic measure and sensitive to individual differences. The second takes into place when we disagree with the first explanation. Namely, the null association means that fear of COVID‐19 does not affect pursuing valued goals in this distressing condition of the pandemic, that is, the fourth wave, which is consistent with the theory that psychological flexibility means pursuing valued goals despite distressful situations (Kashdan et al., 2020).
Regarding the proposed model, there was a significant positive association between distress intolerance and psychological distress, and also a significant negative association between psychological flexibility and psychological distress, comparable to the literature (Chong et al., 2020; Grégoire et al., 2020; Kroska et al., 2020; Tyndall et al., 2018). Moreover, Personalized psychological flexibility was the significant partial mediator of the mentioned relation during the fourth wave of the pandemic.
Consequently, people with higher distress intolerance cannot fully be in touch with their unpleasant emotional experiences, a state that is being joint with a desire to escape from what is being experienced (Lynch & Mizon, 2011; Simons & Gaher, 2005). Therefore, they are more likely to suffer from psychological distress due to the paradoxical effect of suppressing or avoiding what they are going through (Petkus et al., 2012). Psychologically flexible individuals, however, are not averse to their experiences; they accept the inevitability of the situation and harness it as fuel to propel them forward (Kashdan et al., 2020). Thus, by pursuing valued goals in the face of the pandemic, psychological distress could be buffered. However, it was inquiring how putative the mediating role of psychological flexibility will be if the demographics and psychological variables relevant to the pandemic enduring were taken into account. Interestingly, the psychological flexibility remained a significant mediator of the association between distress intolerance and psychological distress while adjusting the model for demographics factors (age, gender, marital status, and education level) and psychological variables (fear of COVID‐19, mindfulness, and life satisfaction). Thus, Psychological flexibility is a ubiquitous process underlying the association between distress intolerance and psychological distress, despite demographics and the variables mentioned above, consistent with the literature (Bhambhani et al., 2020; Dawson & Golijani‐Moghaddam, 2020).
In other words, regardless of context, i.e., variables adjusted for in the model, pursuing valued goals during the pandemic can diminish psychological distress. To be more specific, the mediating role of personalized psychological flexibility can be more explained by its dimension: (a) avoidance, not avoiding negative emotions related to meaningful goals, or postponing pursuing those goals. (b) acceptance, accepting the negative emotions related to the goals or temporary setbacks in valued goal pursuit. And (c) harnessing, using problems and negative emotions as a motivation towards pursuing valued goals. In summary, despite the adjusted variables, accepting and using unpleasant emotions as fuel to achieve valued goals rather than avoiding them would mitigate the psychological distress during the pandemic. Given the psychological flexibility we have used (Kashdan et al., 2020), there was no study to compare these findings based on this index. However, Dawson and Golijani‐Moghaddam (2020) has found psychological flexibility is associated with lower COVID‐19 related distress, which to some extent corroborate the findings. However, the findings implicate that future research would benefit more by using PPFI to measure psychological flexibility as it is in more line with the theoretical definition of psychological flexibility as flexible contact with the present moment while acting in the service of chosen values (Kashdan et al., 2020).
In this study, the strengths are the large sample size, adjusting the mediation model for possible influence variables, and using an idiographic measure of psychological flexibility that addressed the criticisms regarding its measurement (Kashdan et al., 2020; Ong et al., 2020). Any finding, however, should be interpreted in light of its limitations. First, the lockdown and lack of interviews made it impossible to homogenize the sample based on their valued goals, which is essential for future research. Second, cultural differences may also limit the generalizability, which may improve our understanding of personalized psychological flexibility during distressful conditions by replicating the findings in other cultures. Third, the cross‐sectional data limited the ability to test causality formally and limited the generalizability of our results, so longitudinal studies are suggested in future research. Forth, some control variables that may impact distress intolerance, psychological flexibility and psychological distress are not investigated: for example, data on past of current pharmacological treatments (e.g., using or not BZDs, z drugs, SSRI/SNRI; using psychotropic drugs in poly‐therapy or mono‐therapy) and data on past or current psychological treatments (Bright et al., 2020; Cosci et al., 2016; Hausken et al., 2007; Mansueto, Lugoboni, et al., 2021; Swartz, 2020). Considering and assessing these variables is an important direction for future research. Also, future research may wish to replicate the study with some follow‐up time points in order to reach a firm conclusion about the role of personalized psychological flexibility as an underlying mechanism in the relationship between distress intolerance and psychological distress during the pandemic. Additionally, it would be interesting to replicate the model in individuals who recovered from COVID‐19 versus those who were never infected and are now infected (positive COVID‐19 PCR‐test) to examine any differences or similarities in the patterns.
Overall, our findings have an essential suggestion that public health services may consider aiming to provide psychological flexibility enhancing interventions to decay COVID‐19‐related mental distress, particularly in clinical practice. Acceptance and commitment therapy (ACT; Hayes et al., 2006) may be used to address psychological flexibility, with a particular emphasis on personalized form, in order to assist individuals in harnessing pandemic‐related negative emotions towards achieving valued goals, which would result in improved coping and living during this challenging time.
CONFLICT OF INTEREST
The authors have no known competing financial interests or personal relationships that could have influenced this work.
ACKNOWLEDGEMENT
This research did not receive specific grant funding from agencies in the public, commercial or not‐for‐profit sectors.
Akbari, M. , Seydavi, M. , & Zamani, E. (2021). The mediating role of personalized psychological flexibility in the association between distress intolerance and psychological distress: A national survey during the fourth waves of COVID‐19 pandemic in Iran. Clinical Psychology & Psychotherapy, 28(6), 1416–1426. 10.1002/cpp.2685
DATA AVAILABILITY STATEMENT
The datasets analysed during the current study are available from the corresponding author on reasonable request.
REFERENCES
- Abouk, R. , & Heydari, B. (2020). The immediate effect of COVID‐19 policies on social distancing behavior in the United States. SSRN Electronic Journal, 136, 245–252. 10.1177/0033354920976575 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Achdut, N. , & Refaeli, T. (2020). Unemployment and psychological distress among young people during the COVID‐19 pandemic: Psychological resources and risk factors. International Journal of Environmental Research and Public Health, 17(19), 7163. 10.3390/ijerph17197163 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ahorsu, D. K. , Lin, C. Y. , Imani, V. , Saffari, M. , Griffiths, M. D. , & Pakpour, A. H. (2020). The fear of COVID‐19 scale: Development and initial validation. International Journal of Mental Health and Addiction, 1–9. 10.1007/s11469-020-00270-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Akbari, M. , Disabato, D. , Seydavi, M. , & Zamani, E. (2021). The Persian Personalized Psychological Flexibility Index (P‐PPFI): Psychometric properties in a general population sample of Iranians. Journal of Contextual Behavioral Science, 10), October 2021, 32–43. 10.1016/j.jcbs.2021.09.004 [DOI] [Google Scholar]
- Akbari, M. , Hosseini, Z. S. , Seydavi, M. , Zegel, M. , Zvolensky, M. J. , & Vujanovic, A. A. (2021). Distress tolerance and posttraumatic stress disorder: A systematic review and meta‐analysis. Cognitive Behaviour Therapy, Advance online publication, 1–30. 10.1080/16506073.2021.1942541 [DOI] [PubMed] [Google Scholar]
- Akbari, M. , Spada, M. M. , Nikčević, A. V. , & Zamani, E. (2021). The relationship between fear of COVID‐19 and health anxiety among families with COVID‐19 infected: The mediating role of metacognitions, intolerance of uncertainty, and emotion regulation. Clinical Psychology & Psychotherapy. 10.1002/cpp.2628 [DOI] [PubMed] [Google Scholar]
- Alizadehfard, S. , & Alipour, A. (2020). The path analysis model in prediction of corona phobia based on intolerance of uncertainty and health anxiety. Journal of Research in Psychological Health, 14(1), 16–27. http://rph.khu.ac.ir/article-1-3756-en.html [Google Scholar]
- Allan, N. P. , Macatee, R. J. , Norr, A. M. , & Schmidt, N. B. (2014). Direct and interactive effects of distress tolerance and anxiety sensitivity on generalized anxiety and depression. Cognitive Therapy and Research, 38(5), 530–540. 10.1007/s10608-014-9623-y [DOI] [Google Scholar]
- Asghari, A. , Saed, F. , & Dibajnia, P. (2008). Psychometric properties of the depression anxiety stress Scales‐21 (DASS‐21) in a non‐clinical Iranian sample. International Journal of Psychology, 2(2), 82–102. [Google Scholar]
- Banerjee, D. (2020). The impact of Covid‐19 pandemic on elderly mental health. International Journal of Geriatric Psychiatry, 35, 1466–1467. 10.1002/gps.5320 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barzilay, R. , Moore, T. M. , Greenberg, D. M. , DiDomenico, G. E. , Brown, L. A. , White, L. K. , Gur, R. C. , & Gur, R. E. (2020). Resilience, COVID‐19‐related stress, anxiety and depression during the pandemic in a large population enriched for healthcare providers. Translational Psychiatry, 10(1), 1–8. 10.1038/s41398-020-00982-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bhambhani, Y. , Flynn, M. K. , Kellum, K. K. , & Wilson, K. G. (2020). The role of psychological flexibility as a mediator between experienced sexual racism and psychological distress among men of color who have sex with men. Archives of Sexual Behavior, 49(2), 711–720. 10.1007/s10508-018-1269-5 [DOI] [PubMed] [Google Scholar]
- Brailovskaia, J. , Cosci, F. , Mansueto, G. , & Margraf, J. (2021). The relationship between social media use, stress symptoms and burden caused by coronavirus (Covid‐19) in Germany and Italy: A cross‐sectional and longitudinal investigation. Journal of Affective Disorders Reports, 3, 100067. 10.1016/j.jadr.2020.100067 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brooks, S. K. , Webster, R. K. , Smith, L. E. , Woodland, L. , Wessely, S. , Greenberg, N. , & Rubin, G. J. (2020). The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. The Lancet, 395(10227), 912–920. 10.1016/S0140-6736(20)30460-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown, K. W. , & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its role in psychological well‐being. Journal of Personality and Social Psychology, 84(4), 822–848. 10.1037/0022-3514.84.4.822 [DOI] [PubMed] [Google Scholar]
- Busch, I. M. , Moretti, F. , Mazzi, M. , Wu, A. W. , & Rimondini, M. (2021). What we have learned from two decades of epidemics and pandemics: A systematic review and meta‐analysis of the psychological burden of frontline healthcare workers. Psychotherapy and Psychosomatics, 1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cho, J. , Bello, M. S. , Christie, N. C. , Monterosso, J. R. , & Leventhal, A. M. (2021). Adolescent emotional disorder symptoms and transdiagnostic vulnerabilities as predictors of young adult substance use during the COVID‐19 pandemic: Mediation by substance‐related coping behaviors. Cognitive Behaviour Therapy, 50(4), 276–294. 10.1080/16506073.2021.1882552 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chong, Y. Y. , Mak, Y. W. , & Loke, A. Y. (2020). The role of parental psychological flexibility in childhood asthma management: An analysis of cross‐lagged panel models. Journal of Psychosomatic Research, 137, 110208. 10.1016/j.jpsychores.2020.110208 [DOI] [PubMed] [Google Scholar]
- Chou, C. P. , & Bentler, P. M. (1995). Estimates and tests in structural equation modeling: Concepts, issues, and applications. Sage. [Google Scholar]
- Coffey, K. A. , & Hartman, M. (2008). Mechanisms of action in the inverse relationship between mindfulness and psychological distress. Complementary Health Practice Review, 13(2), 79–91. 10.1177/1533210108316307 [DOI] [Google Scholar]
- Cosci, F. , Mansueto, G. , Faccini, M. , Casari, R. , & Lugoboni, F. (2016). Socio‐demographic and clinical characteristics of benzodiazepine long‐term users: Results from a tertiary care center. Comprehensive Psychiatry, 69, 211–215. 10.1016/j.comppsych.2016.06.008 [DOI] [PubMed] [Google Scholar]
- Daly, M. , & Robinson, E. (2021). Psychological distress and adaptation to the COVID‐19 crisis in the United States. Journal of Psychiatric Research, 136, 603–609. 10.1016/j.jpsychires.2020.10.035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dawson, D. L. , & Golijani‐Moghaddam, N. (2020). COVID‐19: Psychological flexibility, coping, mental health, and wellbeing in the UK during the pandemic. Journal of Contextual Behavioral Science, 17, 126–134. 10.1016/j.jcbs.2020.07.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diener, E. , Emmons, R. A. , Larsen, R. J. , & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49, 71–75. 10.1207/s15327752jpa4901_13 [DOI] [PubMed] [Google Scholar]
- Doorley, J. D. , Goodman, F. R. , Kelso, K. C. , & Kashdan, T. B. (2020). Psychological flexibility: What we know, what we do not know, and what we think we know. Social and Personality Psychology Compass, 14(12), 1–11. 10.1111/spc3.12566 [DOI] [Google Scholar]
- Duong, C. D. (2021). The impact of fear and anxiety of Covid‐19 on life satisfaction: Psychological distress and sleep disturbance as mediators. Personality and Individual Differences, 178, 110869. 10.1016/j.paid.2021.110869 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Efron, B. , & Tibshirani, R. J. (1994). An introduction to the bootstrap. CRC press. 10.1201/9780429246593 [DOI] [Google Scholar]
- Ghorbani, N. , Watson, P. J. , & Weathington, B. L. (2009). Mindfulness in Iran and the United States: Cross‐cultural structural complexity and parallel relationships with psychological adjustment. Current Psychology, 28(4), 211–224. 10.1007/s12144-009-9060-3 [DOI] [Google Scholar]
- Grégoire, S. , Gagnon, J. , Lachance, L. , Shankland, R. , Dionne, F. , Kotsou, I. , Monestès, J. L. , Rolffs, J. L. , & Rogge, R. D. (2020). Validation of the english and french versions of the multidimensional psychological flexibility inventory short form (MPFI‐24). Journal of Contextual Behavioral Science, 18, 99–110. 10.1016/j.jcbs.2020.06.004 [DOI] [Google Scholar]
- Guney, S. , Kalafat, T. , & Boysan, M. (2010). Dimensions of mental health: Life satisfaction, anxiety and depression: A preventive mental health study in Ankara University students population. Procedia‐Social and Behavioral Sciences, 2(2), 1210–1213. 10.1016/j.sbspro.2010.03.174 [DOI] [Google Scholar]
- Hausken, A. M. , Skurtveit, S. , Rosvold, E. O. , Bramness, J. G. , & Furu, K. (2007). Psychotropic drug use among persons with mental distress symptoms: A population‐based study in Norway. Scandinavian Journal of Public Health, 35(4), 356–364. 10.1002/pds.1417 [DOI] [PubMed] [Google Scholar]
- Hayes, S. C. , Luoma, J. B. , Bond, F. W. , Masuda, A. , & Lillis, J. (2006). Acceptance and commitment therapy: Model, processes and outcomes. Behaviour Research and Therapy, 44(1), 1–25. 10.1016/j.brat.2005.06.006 [DOI] [PubMed] [Google Scholar]
- Hu, L. , & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- Karimi, L. , Khalili, R. , & SiratiNir, M. (2020). Prevalence of various psychological disorders during the COVID‐19 pandemic: Systematic review. Journal of Military Medicine, 22(6), 648–662. 10.30491/JMM.22.6.648 [DOI] [Google Scholar]
- Kashdan, T. B. , Disabato, D. J. , Goodman, F. R. , Doorley, J. D. , & McKnight, P. E. (2020). Understanding psychological flexibility: A multimethod exploration of pursuing valued goals despite the presence of distress. Psychological Assessment, 32(9), 829–850. 10.1037/pas0000834 [DOI] [PubMed] [Google Scholar]
- Kelishadi, F. , & Yazdkhasti, F. (2016). Impact of perception of parental rejection–acceptance and control on moral intelligence and distress tolerance. Strategy for Culture, 9(33), 155–169. [Google Scholar]
- Keough, M. E. , Riccardi, C. J. , Timpano, K. R. , Mitchell, M. A. , & Schmidt, N. B. (2010). Anxiety symptomatology: The association with distress tolerance and anxiety sensitivity. Behavior Therapy, 41(4), 567–574. 10.1016/j.beth.2010.04.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kiselica, A. M. , Webber, T. , & Bornovalova, M. A. (2014). Stability and change in distress tolerance and its prospective relationship with borderline personality features: A short‐term longitudinal study. Personality Disorders, Theory, Research, and Treatment, 5(3), 247–256. 10.1037/per0000076 [DOI] [PubMed] [Google Scholar]
- Kline, R. B. (2011). Principles and practice of structural equation modeling (3rd ed.). Guilford. [Google Scholar]
- Kroska, E. B. , Roche, A. I. , Adamowicz, J. L. , & Stegall, M. S. (2020). Psychological flexibility in the context of COVID‐19 adversity: Associations with distress. Journal of Contextual Behavioral Science, 18, 28–33. 10.1016/j.jcbs.2020.07.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kumar, H. , Shaheen, A. , Rasool, I. , & Shafi, M. (2016). Psychological distress and life satisfaction among university students. Journal of Psychologu & Clinical Psychiatry, 5(3), 00283. 10.15406/jpcpy.2016.05.00283 [DOI] [Google Scholar]
- Losada‐Baltar, A. , Jiménez‐Gonzalo, L. , Gallego‐Alberto, L. , Pedroso‐Chaparro, M. D. S. , Fernandes‐Pires, J. , & Márquez‐González, M. (2021). “We Are Staying at Home.” Association of Self‐perceptions of Aging, Personal and Family Resources, and Loneliness With Psychological Distress During the Lock‐Down Period of COVID‐19. The Journals of Gerontology: Series B, 76(2), e10–e16. 10.1093/geronb/gbaa048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lovibond, P. F. , & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of the depression anxiety stress scales (DASS) with the Beck depression and anxiety inventories. Behaviour Research and Therapy, 33(3), 335–343. 10.1016/0005-7967(94)00075-U [DOI] [PubMed] [Google Scholar]
- Lynch, T. R. , & Mizon, G. A. (2011). Distress overtolerance and distress intolerance: A behavioral perspective. In Zvolensky M. J., Bernstein A., & Vujanovic A. A. (Eds.), Distress tolerance: Theory, research, and clinical applications (pp. 52–79). Guilford Press. [Google Scholar]
- Macatee, R. J. , Albanese, B. J. , Allan, N. P. , Schmidt, N. B. , & Cougle, J. R. (2016). Distress intolerance as a moderator of the relationship between daily stressors and affective symptoms: Tests of incremental and prospective relationships. Journal of Affective Disorders, 206, 125–132. 10.1016/j.jad.2016.07.035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mansueto, G. , Lopes, F. L. , Grassi, L. , & Cosci, F. (2021). Impact of COVID‐19 outbreak on Italian healthcare workers versus general population: Results from an online survey. Clinical Psychology & Psychotherapy, 1–12. 10.1002/cpp.2644 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mansueto, G. , Lugoboni, F. , Casari, R. , Bertoldi, A. , & Cosci, F. (2021). Mono‐and poly‐therapy with benzodiazepines or Z‐drugs: Results from a tertiary‐care addiction unit study. The International Journal of Risk & Safety in Medicine, (Preprint), 1–26. [DOI] [PubMed] [Google Scholar]
- Maroufizadeh, S. , Ghaheri, A. , Samani, R. O. , & Ezabadi, Z. (2016). Psychometric properties of the satisfaction with life scale (SWLS) in Iranian infertile women. International Journal of Reproductive BioMedicine, 14(1), 57–62. 10.29252/ijrm.14.1.57 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mazza, C. , Ricci, E. , Biondi, S. , Colasanti, M. , Ferracuti, S. , Napoli, C. , & Roma, P. (2020). A nationwide survey of psychological distress among Italian people during the COVID‐19 pandemic: Immediate psychological responses and associated factors. International Journal of Environmental Research and Public Health, 17(9), 3165–3179. 10.3390/ijerph17093165 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGrew, S. J. , Ennis, C. R. , Vujanovic, A. , Franklin, C. L. , & Raines, A. M. (2020). An initial investigation of the association between distress intolerance and posttraumatic stress within military sexual trauma survivors. Psychological Trauma Theory Research Practice and Policy, 12(3), 306–312. 10.1037/tra0000516 [DOI] [PubMed] [Google Scholar]
- McHugh, L. , Stewart, I. , & Almada, P. (2019). A contextual behavioral guide to the self: Theory and practice. New Harbinger Publications. [Google Scholar]
- McHugh, R. K. , & Otto, M. W. (2012). Refining the measurement of distress intolerance. Behavior Therapy, 43(3), 641–651. 10.1016/j.beth.2011.12.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ministry of Health and Medical Education of Iran . (2021). COVID‐19 news dashboard. Retrieved from http://ird.behdasht.gov.ir/index.aspx
- Modares, M. (2011). Effectiveness of group dialectical behavior therapy (based on core mindfulness, distress tolerance and emotion regulation components) on depressive symptoms in university students. Journal of Fundamentals of Mental Health, 13(50), 35–124. 10.22038/JFMH.2011.881 [DOI] [Google Scholar]
- Norberg, M. M. , Beath, A. P. , Kerin, F. J. , Martyn, C. , Baldwin, P. , & Grisham, J. R. (2020). Trait versus task‐induced emotional reactivity and distress intolerance in hoarding disorder: Transdiagnostic implications. Behavior Therapy, 51(1), 123–134. 10.1016/j.beth.2019.05.010 [DOI] [PubMed] [Google Scholar]
- Ong, C. W. , Pierce, B. G. , Petersen, J. M. , Barney, J. L. , Fruge, J. E. , Levin, M. E. , & Twohig, M. P. (2020). A psychometric comparison of psychological inflexibility measures: Discriminant validity and item performance. Journal of Contextual Behavioral Science, 18, 34–47. 10.1016/j.jcbs.2020.08.007 [DOI] [Google Scholar]
- Parto, M. , & Besharat, M. A. (2011). Mindfulness, psychological well‐being and psychological distress in adolescents: Assessing the mediating variables and mechanisms of autonomy and self‐regulation. Procedia‐Social and Behavioral Sciences, 30, 578–582. 10.1016/j.sbspro.2011.10.112 [DOI] [Google Scholar]
- Patel, Z. S. , Casline, E. , Jensen‐Doss, A. , & Timpano, K. R. (2020). Parent distress intolerance, repetitive negative thinking, and mental health service use. Child Psychiatry & Human Development, 52(3), 365–375. 10.1007/s10578-020-01017-1 [DOI] [PubMed] [Google Scholar]
- Petkus, A. J. , Gum, A. , & Wetherell, J. L. (2012). Thought suppression is associated with psychological distress in homebound older adults. Depression and Anxiety, 29(3), 219–225. 10.1002/da.20912 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Qiu, J. , Shen, B. , Zhao, M. , Wang, Z. , Xie, B. , & Xu, Y. (2020). A nationwide survey of psychological distress among Chinese people in the COVID‐19 epidemic: Implications and policy recommendations. General Psychiatry, 33(2), e100213. 10.1136/gpsych-2020-100213 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson, L. J. , & Freeston, M. H. (2014). Emotion and internal experience in obsessive‐compulsive disorder: Reviewing the role of alexithymia, anxiety sensitivity and distress tolerance. Clinical Psychology Review, 34(3), 256–271. 10.1016/j.cpr.2014.03.003 [DOI] [PubMed] [Google Scholar]
- Sahebi, A. , Asghari, M. J. , & Salari, R. S. (2005). Validation of depression anxiety and stress scale (DASS‐21) for an Iranian population.
- Satici, B. , Gocet‐Tekin, E. , Deniz, M. E. , & Satici, S. A. (2020). Adaptation of the fear of COVID‐19 scale: Its association with psychological distress and life satisfaction in Turkey. International Journal of Mental Health and Addiction, 1–9. 10.1007/s11469-020-00294-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simons, J. S. , & Gaher, R. M. (2005). The distress tolerance scale: Development and validation of a self‐report measure. Motivation and Emotion, 29(2), 83–102. 10.1007/s11031-005-7955-3 [DOI] [Google Scholar]
- Swartz, H. A. (2020). The role of psychotherapy during the COVID‐19 pandemic (Vol. 73) (pp. 41–42). 10.1176/appi.psychotherapy.20200015 [DOI] [PubMed] [Google Scholar]
- Tyndall, I. , Waldeck, D. , Riva, P. , Wesselmann, E. D. , & Pancani, L. (2018). Psychological flexibility and ostracism: Experiential avoidance rather than cognitive fusion moderates distress from perceived ostracism over time. Journal of Contextual Behavioral Science, 7, 72–80. [Google Scholar]
- Wang, C. , Pan, R. , Wan, X. , Tan, Y. , Xu, L. , Ho, C. S. , & Ho, R. C. (2020). Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID‐19) epidemic among the general population in China. International Journal of Environmental Research and Public Health, 17(5), 1729. 10.3390/ijerph17051729 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wenham, C. , Smith, J. , Davies, S. E. , Feng, H. , Grépin, K. A. , Harman, S. , Herten‐Crabb, A. , & Morgan, R. (2020). Women are most affected by pandemics—lessons from past outbreaks. [DOI] [PubMed]
- World Health Organization . (2021). Coronavirus disease (COVID‐19) situation dashboard. Retrieved from https://covid19.who.int/
- Xiao, H. , Zhang, Y. , Kong, D. , Li, S. , & Yang, N. (2020). Social capital and sleep quality in individuals who self‐isolated for 14 days during the coronavirus disease 2019 (COVID‐19) outbreak in January 2020 in China. Medical Science Monitor: International Medical Journal of Experimental and Clinical Research, 26, e923921‐1. 10.12659/MSM.923921 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yasegnal, A. S. (2021). Systematic review on psychological impacts and mitigating strategies of COVID‐19: The lesson every one shall learn from the our time pandemic. Illness, Crisis & Loss. 10.1177/10541373211005110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhang, J. , Lu, H. , Zeng, H. , Zhang, S. , Du, Q. , Jiang, T. , & Du, B. (2020). The differential psychological distress of populations affected by the COVID‐19 pandemic. Brain, Behavior, and Immunity, 87, 49–50. 10.1016/j.bbi.2020.04.031 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets analysed during the current study are available from the corresponding author on reasonable request.