

Vaccines are a fundamental weapon against a number of infections that may cause severe disease or sequelae, both in the absence or presence of etiologic therapy, or have a high socio‐economic impact in terms of hospital admissions or requests for medical examination. COVID‐19, a serious infection due to SARS‐CoV‐2, exemplifies all these characteristics.
In Italy, paediatric SARS‐CoV‐2 infection presented in most cases with few symptoms or even in asymptomatic form, although nearly 20% of children enrolled in a nationwide registry developed complications, especially in the presence of comorbidities. 1 However, in some children and adolescents, SARS‐CoV‐2 infection was associated with the so‐called multisystemic inflammatory disease (MIS‐C), which required hospitalisation and therapies. MIS‐C is thought to be caused by a postinfectious inflammatory process and manifests clinically with signs and symptom like those of Kawasaki disease (KD) but is also marked by clinical manifestations unusual in KD, particularly gastrointestinal complaints and myocarditis, often leading to myocardial failure and shock. 2 Despite the occurrence of this potentially life‐threatening condition because of the general notion of a modest clinical severity of COVID‐19 in paediatrics, especially when compared with its massive impact in adults, the opinion that SARS‐CoV‐2 ‘does not harm children’ has become widespread among doctors and, consequently, in the mass media and public opinion. This has led to an increase in perplexity, especially among families, regarding the need to vaccinate children against SARS‐CoV‐2.
To investigate whether this impression of the absence of serious illness was supported by epidemiological data, we evaluated the rate of MIS‐C per 100 000 (DR) residents <19 years of Liguria, a region located in northwest Italy. On January 1st 2021, Liguria had a total of 1 509 805 residents, with 214 395 <19 years. 3
From March 2020 to June 2021, all cases of MIS‐C observed in the region were centralised, and 22 patients were diagnosed according to predefined criteria for MIS‐C 2 (although seven of them also met the American Heart Association criteria for KD), 4 leading to a DR of 10.3. Noteworthy, there were 10 (45%) patients with myocardial disfunction, 6 (60%) of them with an ejection fraction <50%. Moreover, 4 (18%) of patients underwent abdominal surgery for suspect acute appendicitis, which eventually was not confirmed by laparotomy.
To compare the frequency of SARS‐CoV‐2‐related MIS‐C with other severe infections observed in the same age group, we evaluated the DR of tuberculosis and invasive disease due to Neisseria meningitidis, starting from episodes recorded in a regional registry in the period 2007–2020. The mean number of episodes per year was 5 (range 1–14) for tuberculosis and 3 (range 0–7) for invasive meningococcal disease. Figure 1 reports the DR for the three conditions. The DR for tuberculosis and invasive meningococcal disease are very similar, whereas that for MIS‐C is about 5‐ to 10‐fold higher.
FIGURE 1.
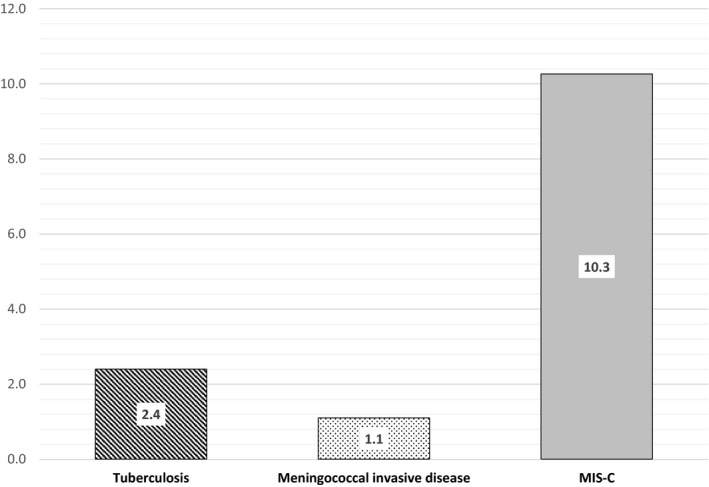
Rates/100 000 residents <19 years in Liguria, Italy, of tuberculosis, invasive meningococcal disease and multisystem inflammatory syndrome—coronavirus‐related disease
The major weakness of this analysis is that the DR for tuberculosis and meningococcal infection could be somewhat inaccurate, considering the method used for their estimation. However, we believe that the possible reduced accuracy in the calculation of DR for these two diseases should not significantly change the order of magnitude of the rates and, therefore, the difference with MIS‐C.
In conclusion, our data show that although children rarely develop severe COVID‐19, they have a significant risk of developing a serious and potentially life‐threatening condition secondary to a delayed, immune‐mediated reaction to SARS‐CoV‐2, with rates higher than those of other serious paediatric infections. Importantly, the long‐term outcome of MIS‐C is still unclear, and the risk of residual cardiac damage is not yet established. In our opinion, in addition to the general need to interrupt the chain of contagion, the high DR for MIS‐C and its unknown long‐term consequences represent important reasons for carrying out anti‐COVID vaccination in children and adolescents.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
ACKNOWLEDGEMENT
Open Access Funding provided by Universita degli Studi di Genova within the CRUI‐CARE Agreement.
FUNDING INFORMATION
No funds, grants, or other support was received.
[Correction added on 14 May 2022, after first online publication: CRUI‐CARE funding statement has been added.]
REFERENCES
- 1. Garazzino S, Lo Vecchio A, Pierantoni L, et al. Epidemiology, clinical features and prognostic factors of pediatric SARS‐CoV‐2 infection: results from an Italian multicenter study. Front Pediatr. 2021;9:649358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Centers for Diseases Control (CDC) Health Advisory . Multisystem Inflammatory Syndrome in Children (MIS‐C) Associated with Coronavirus Disease 2019 (COVID‐19); 2020. https://emergency.cdc.gov/han/2020/han00432.asp. Accessed June 19, 2021.
- 3. ISTAT Istituto Italiano di Statistica; 2021. http://dati.istat.it/Index.aspx?QueryId=18541. Accessed June 18, 2021.
- 4. McCrindle BW, Rowley AH, Newburger JW, et al. Diagnosis, treatment, and long‐term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017;135:e927‐e999. [DOI] [PubMed] [Google Scholar]