

Abstract
Introduction:
Globally speaking, cardiovascular disease is the leading cause of mortality, with coronary artery disease (CAD) contributing to half of the cases. A major complication of CAD is myocardial infarction (MI). The clinical outcomes of MI are predominantly time-dependent; therefore, it is paramount that the general public is familiar with the early symptoms of MI.
Aim:
The main objective is to gauge the local public awareness of the early symptoms of MI, and their knowledge of the best course of action to be taken from the onset of symptoms.
Method:
A cross-sectional study was conducted using google forms. Participants were randomly selected through multiple social media platforms. The study included Saudi citizens who were 18 years or older, with no current or prior experience in the health care field. The questionnaire assessed the participants' awareness of 14 risk factors for CAD. The variables investigated were participants' knowledge of the symptoms, causes, appropriate course of action to be taken, and the risk factors of CAD.
Results:
A total of 1689 participants were involved in this study. Sixty percent were females, and 29.2% were in the age group of 18–24 years. Seventy-three percent of the participants knew the definition of heart attack, and 90% knew that chest pain is a symptom of a heart attack. Approximately, 75% of the participants recognized that hypertension, cigarette smoking, and high cholesterol are the risk factors of MI. In terms of knowledge, Al Madinah province obtained the highest score when compared with other regions.
Conclusion:
This study showed the overall knowledge and awareness of CAD was suboptimal, indicating that awareness initiatives and patient education of CAD need more work in Saudi Arabia, especially in high-risk groups and lower education groups. More studies are needed to identify the efficiency and population access of different approaches for CAD awareness.
Keywords: Acute myocardial infarction, awareness, early symptoms, risk factor, Saudi Arabia
Introduction
Cardiovascular disease (CVD) is an umbrella term describing pathologies that involve the cardiovascular system, with the commonest being CAD. CVD is the leading cause of morbidity and mortality globally, constituting significant public health and economical burdens around the world.[1] MI is a consequence of CAD, and the general prevalence of MI in the US is around 2.8% in grown-ups aged 20 years. Additionally, the American Heart Association estimates that an American will have an MI every 42 s.[2]
Over the past years, Saudi Arabia has undergone significant urbanization, which has been followed by a rise in CVD rates, with an overall prevalence of 5.5%.[3] In Saudi Arabia, CAD represents the third most common cause of mortality in hospitals, coming after road traffic accidents and senility,[4] making it a growing health concern in the Kingdom. Additionally, acute coronary syndrome (ACS) death rates in Saudi Arabia were 4%, 5.8%, and 8.1%, in-hospital, at 1 month, and 1 year, respectively.[5]
Clinical outcomes in MI are predominantly time-dependent; it is, therefore, vital that patients recognize the early symptoms of MI and seek medical intervention as early as possible. A number of studies in the past have investigated the general public awareness of theearly symptoms of MI; however, there are few studies in the literature that were conducted locally. A study by Hee-Sook Kim et al.[6] had concluded that the general public in South Korea had poor awareness of early MI symptoms and the appropriate action to make after the manifestation of symptoms. Additionally, a similar study was done in the UK to assess the public knowledge of MI, and the outcome was that over half of the sample (n = 302) knew only two or fewer MI symptoms.[7] Recently, a local study was conducted in Jeddah assessing population awareness of coronary artery disease and its risk factors. Amongst 468 participants, the mean score was 4.31 ± 1.36 out of 8.[8]
Previous literature has shown that patients' knowledge of the symptoms of MI correlates with their clinical outcomes. The objectives of this study are to gauge the local public awareness of the early symptoms of MI, and their knowledge of the best course of action to be taken from the onset of symptoms.
Method
This cross-sectional study was conducted using google forms, participants were selected through multiple social media platforms. The questionnaire was designed in both languages Arabic and English. The study included any 18 years or older Saudi citizens with no current or prior experience in the health work field.
The data were collected by the research team using an online-based questionnaire after obtaining approval from the institutional review board (IRB), which was completed by eligible participants who consented to take part in the study. A validated questionnaire was adopted from the Nigerian Journal of Cardiology, and a request for permission to use the questionnaire was given.[9] This questionnaire had been evaluated by a panel of two experts at King Abdulaziz Cardiac Center. The questionnaire included knowledge about symptoms, causes, the appropriate course of action to be taken, and the risk factors of MI. The first section of the questionnaire asked about the participant's demographical data such as age, gender, education level, and household income. In the second section, the participants were asked about the definition, the symptoms of acute MI, and the proper action that they should take as well as the causes and risk factors of MI. The participants had a total of 15 questions related to MI knowledge.
The knowledge was scored as the total number of correct answers which was then categorized as inadequate knowledge if the score was less than 8. The data collection and analysis were done using IBM SPSS Statistics for Windows, Version 20.0 Armonk, NY, IBM Corp. The qualitative data were presented as percentages and frequencies. Whereas the numerical data were presented by mean and standard deviation. Chi-square or Fisher's exact tests were used to assess the association between MI knowledge and other qualitative data for categorical variables to assess associations between MI knowledge and demographics. A test with a P value (≤0.05) was considered to be significant.
Result
The total number of participants involved in this study was 1689, distributed in all regions of Saudi Arabia, with the majority from Riyadh province (46.1%). About one-third were in the age group of 18 to 24 years. Sixty percent were female, and 58% were married. Most were highly educated (university and above). As shown in Table 1.
Table 1.
Demographic characteristic
| Variables | Categories | n | % |
|---|---|---|---|
| Age | 18-24 | 494 | 29.2% |
| 25-34 | 297 | 17.6% | |
| 35-44 | 331 | 19.6% | |
| 45-54 | 356 | 21.1% | |
| 55 and above | 211 | 12.5% | |
| Gender | Male | 662 | 39.2% |
| Female | 1027 | 60.8% | |
| Marital status | Married | 987 | 58.4% |
| Unmarried | 702 | 41.6% | |
| Education | High school or less | 417 | 24.7% |
| University or higher | 1272 | 75.3% | |
| Household income/thousands | <5 | 579 | 34.3% |
| between 5 and 10 | 393 | 23.3% | |
| between 10 and 20 | 539 | 31.9% | |
| More than 20 | 178 | 10.5% | |
| Region/province | Riyadh | 778 | 46.1% |
| Eastern | 161 | 9.5% | |
| Makkah | 150 | 8.9% | |
| Al-Qassim | 146 | 8.6% | |
| Northen Borders | 106 | 6.3% | |
| Al madinah | 101 | 6.0% | |
| Najran | 70 | 4.1% | |
| Jazan | 59 | 3.5% | |
| Al-baha/Aseer | 67 | 4.0% | |
| Other* | 51 | 3.0% |
*Tabuk, Jawf and Hail
Figure 1 demonstrates the participants' knowledge about heart attacks. A total of 73% of the participants correctly answered the question about the definition of a heart attack. Most of them were aware of the symptoms of heart attack, between 79% and 90% realize that shortness of breath and chest pain, respectively are symptoms of a heart attack. About half of them recognized arm or shoulder discomfort and jaw or neck pain as a symptom.
Figure 1.

Participants knowledge about the causes and signs of MI
When asked about the causes of heart attack, three-fourths of the participants could recognize hypertension, cigarette smoking, and high cholesterol as a cause. Whereas 25% mentioned excessive salt intake and 12% reported alcoholism.
The relationship of different sociodemographic characteristics with the knowledge about heart attack was studied. There was a statistically significant relationship with the age (P: 0.002), in which the age group 35–44 was more knowledgeable when compared with the younger and older age groups. Other factors which were statistically significant included marital status, household income, and the regions.
The married were more knowledgeable than nonmarried (P: 0.012), the participants with higher income scored higher than those withlower-income (P: 0.038), and the Almadinah region was the highest in knowledge when compared with other regions. Table 2
Table 2.
The relationship of different sociodemographic characteristic to the knowledge
| Variables | Categories | Total Knowledge | P | |||
|---|---|---|---|---|---|---|
|
| ||||||
| Low | High | |||||
|
|
|
|||||
| n | % | n | % | |||
| Age | 18-24 | 296 | 59.9% | 198 | 40.1% | 0.002 |
| 25-34 | 156 | 52.5% | 141 | 47.5% | ||
| 35-44 | 153 | 46.2% | 178 | 53.8% | ||
| 45-54 | 197 | 55.3% | 159 | 44.7% | ||
| 55 and above | 104 | 49.3% | 107 | 50.7% | ||
| Gender | Male | 357 | 53.9% | 305 | 46.1% | 0.85 |
| Female | 549 | 53.5% | 478 | 46.5% | ||
| Marital status | Married | 504 | 51.1% | 483 | 48.9% | 0.012 |
| Unmarried | 402 | 57.3% | 300 | 42.7% | ||
| Education | High school or less | 240 | 57.6% | 177 | 42.4% | 0.065 |
| University or higher | 666 | 52.4% | 606 | 47.6% | ||
| Household income/thousands | Less than 5 | 337 | 58.2% | 242 | 41.8% | 0.038 |
| between 5 and10 | 209 | 53.2% | 184 | 46.8% | ||
| between 10 and 20 | 273 | 50.6% | 266 | 49.4% | ||
| More than 20 | 87 | 48.9% | 91 | 51.1% | ||
| Region/province | Riyadh | 401 | 51.5% | 377 | 48.5% | 0.001 |
| Eastern | 79 | 49.1% | 82 | 50.9% | ||
| Makkah | 92 | 61.3% | 58 | 38.7% | ||
| Al-Qassim | 84 | 57.5% | 62 | 42.5% | ||
| Northen Borders | 74 | 69.8% | 32 | 30.2% | ||
| Al Madinah | 40 | 39.6% | 61 | 60.4% | ||
| Najran | 37 | 52.9% | 33 | 47.1% | ||
| Jazan | 37 | 62.7% | 22 | 37.3% | ||
| Al-baha/Aseer | 37 | 55.2% | 30 | 44.8% | ||
| Other* | 25 | 49.0% | 26 | 51.0% | ||
| Have you or one of your family members been diagnosed with heart attack | No | 751 | 53.40% | 656 | 46.60% | 0.625 |
| Yes | 155 | 55.00% | 127 | 45.00% | ||
*Tabuk, Jawf and Hail
Figure 2 shows the prevalence of different morbidities in the participants, in which more than 25% of the participants were having high cholesterol, and around 20% of them were obese or hypertensive. Diabetes mellitus was present in only 15%, and 20% were smokers. Only a minority (3.5%) were having a prior stroke or heart disease. There was no statistically significant relationship between knowledge and comorbidities.
Figure 2.
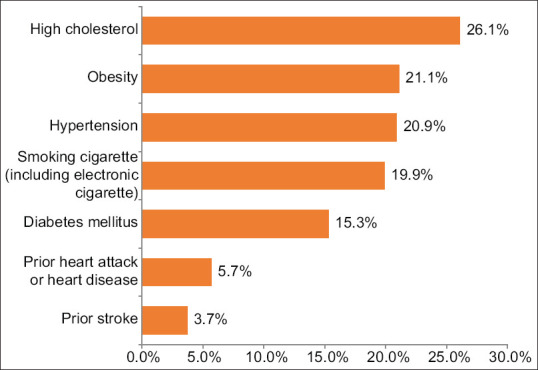
The prevalence of different morbidities in participants
Discussion
This study demonstrated that the overall knowledge and awareness of CAD in Saudi Arabia is suboptimal. This result is consistent with other studies done in the region and other developing countries in Africa and East Asia.[8,10,11,12,13,14] Better results were, however, portrayed in similar studies done in developed countries.[15,16]
Even though CAD mortality has been significantly declining in many developed countries due to advances in disease prevention, diagnosis, and treatment, CAD remains nonetheless a major killer worldwide with ischemic heart disease remaining the most common cause of death followed by CAD.[14,17] Furthermore, current projections are further expecting ischemic heart disease to be the leading cause of death even by 2030. Both CAD mortality and risk factors are inclining in developing countries, raising concern. Moreover, 82% of CAD mortality in the future is expected to occur in developing countries.[14]
Although genetic and hereditary trends are well-established risk factors for CAD, it is estimated that 90 percent of people who die of CAD have one or more major modifiable risk factors.[14,18] In this presented work, the knowledge of different risk factors varied significantly. The most commonly addressed risk factor was smoking (75%). Low rates were reported multiple times in the Saudi literature in regards to awareness of smoking as a risk factor of CAD.[8,10] In a study conducted in the western region of Saudi Arabia, 66.7% of the population recognized smoking as a risk factor for CAD.[10] Furthermore, a recent study conducted in Jeddah reported an as low as 26% awareness regarding smoking as a risk for CAD. A study done in al Qassim region, however, showed a very high awareness rate of smoking as a risk factor reaching over 95%. Good results were also reported by other neighboring developing countries.[15,19,20] In an Omani study, 98% of the population reported smoking as a risk factor for CAD.[11] Similarly, 72% and 71% of the population in our study recognized hypertension and hyperlipidemia as a risk for CAD, which is consistent with multiple studies done in the region as well.[10,13,19] However, higher rates ranging from 84% to 88% for HTN and DLP were reported in Oman and Lebanon.[11,20]
Numbers tended to be shockingly low for alcoholism (12%) which could be attributed to the Islamic culture of Saudi Arabia, in which alcoholism tends to be a sensitive subject to openly discuss and tackle. Generally, the rate of alcoholism is estimated to be significantly lower than the international average, due to sociocultural factors as well as strict drug control regulations and laws.[21,22] However, alcohol is still available illegally either through smuggling or illegal brewing factories.[21] The prevalence of alcoholism and drug abuse is generally a question mark for researchers in the region as there are no reliable epidemiological studies for alcoholism or drug abuse in Saudi Arabia.[23] Further studies are needed to assess the prevalence and magnitude of the effect of alcoholism as well as its national trend, upon which the degree of necessity of alcohol education could be assessed.
Only 25% of the population reported salt as a risk factor, which is similar to another study done in the western region in which only 27% identified an unhealthy diet as a risk factor. However, similar works in the literature showed much better reporting rates for negative dietary behavior as a risk factor of CAD.[9,13] Nonetheless, it is notable to mention that their survey tackled fast food and soft drinks, whereas our question tackled salt, a readily common ingredient quite abundantly used in every household. This possibly reflects the notion that people generally consider homemade food healthy regardless.
Furthermore, there was no significant association between high-risk groups and overall knowledge of CAD, raising a concern that people who are at higher risk might not be sufficiently educated in the matter. Awareness of individual risk for CAD is crucial and is strongly associated with the prevention and reduction in mortality.[16,24,25,26] In a study involving over 55,000 participants, a better lifestyle was associated with 50% less relative risk for CAD.[26] Furthermore, multiple studies consistently explained the significant 80% to 99% of CAD mortality decline over time, to be more significant due to risk factors trend rather than advances in treatment, further highlighting the importance of risk education and risk factor control.[24,25,27]
Only 54% of the participants answered calling an emergency hotline as their first step in case of a suspected heart attack. It is well established that the reduction in the time-to-treatment duration is of utmost cruciality as it minimizes infarct size, reduces the degree of ventricular dysfunction, and improves mortality in the setting of acute MI.[28] Delay in seeking medical care is complicated and can be influenced by many factors, ranging from the severity of the experience and symptoms, fear of consequences, fear of medical care, reticence to inconvenience others, knowledge of symptoms, and understanding the need for urgency.[29] It is upon all these factors that the patient might decide to wait and see, seek the advice of a friend, contact his primary physician, or call the emergency medical service.[29]
Conclusion
This study showed that the overall knowledge and awareness of CAD was suboptimal, indicating that awareness initiatives and patient education of CAD need more work in SA, especially in the high-risk groups, lower education groups, and rural areas. More studies are needed to identify the efficiency and population access of different approaches for CAD awareness.
Ethical approval
An IRB approval was obtained by King Abdullah International Medical Research Center, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJL. Global and regional burden of disease and risk factors, 2001: Systematic analysis of population health data. Lancet. 2006;367:1747–57. doi: 10.1016/S0140-6736(06)68770-9. [DOI] [PubMed] [Google Scholar]
- 2.Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke statistics—2016 update. Circulation. 2016;133:e38–360. doi: 10.1161/CIR.0000000000000350. [DOI] [PubMed] [Google Scholar]
- 3.Al-Nozha MM, Arafah MR, Al-Mazrou YY, Al-Maatouq MA, Khan NB, Khalil MZ, et al. Coronary artery disease in Saudi Arabia. Saudi Med J. 2004;25:1165–71. [PubMed] [Google Scholar]
- 4.Kumosani TA, Alama MN, Iyer A.P. Cardiovascular Diseases in Saudi Arabia. Prime Research on Medicine, 1. 2011:1–6. [Google Scholar]
- 5.Alhabib KF, Kinsara AJ, Alghamdi S, Al-Murayeh M, Hussein GA, AlSaif S, et al. The first survey of the Saudi acute myocardial infarction registry program: Main results and long-term outcomes (STARS-1 program) PLoS One. 2019;14:e0216551. doi: 10.1371/journal.pone.0216551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kim H-S, Lee HJ, Kim KY, Park H-K, Park K-S, Kang GW, et al. The general public's awareness of early symptoms of and emergency responses to acute myocardial infarction and related factors in South Korea: A national public telephone survey. J Epidemiol. 2016;26:233–41. doi: 10.2188/jea.JE20150074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Whitaker S, Baldwin T, Tahir M, Choudhry O, Senior A, Greenfield S. Public knowledge of the symptoms of myocardial infarction: A street survey in Birmingham, England. Fam Pract. 2012;29:168–73. doi: 10.1093/fampra/cmr079. [DOI] [PubMed] [Google Scholar]
- 8.Almalki MA, AlJishi MN, Khayat MA, Bokhari HF, Subki AH, Alzahrani AM, et al. Population awareness of coronary artery disease risk factors in Jeddah, Saudi Arabia: A cross-sectional study. Int J Gen Med. 2019;12:63–70. doi: 10.2147/IJGM.S184732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kolo PM, Ogunmodede JA, Sanya EO, Bello HS, Ghadamosi MS, Dele-Ojo BF, et al. Public knowledge of heart attack symptoms and prevalence of self-reported cardiovascular risk factors in Ilorin, Nigeria. Nig J Cardiol. 12:95–100. [serial online] 2015 [cited 2021 Sep 17] Available from: https://www.nigjcardiol.org/text.asp?2015/12/2/95/152022 . [Google Scholar]
- 10.Albugami S, Al-Husayni F, Bakhsh L, Alhameed F, Alsulami A, Abumelha K, et al. The perception of coronary artery disease and cardiac catheterization in Saudi Arabia: “What the public know”. Cureus. 2020;12:e6570. doi: 10.7759/cureus.6570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ammouri AA, Tailakh A, Isac C, Kamanyire JK, Muliira J, Balachandran S. Knowledge of coronary heart disease risk factors among a community sample in Oman: Pilot study. Sultan Qaboos Univ Med J. 2016;16:e189–96. doi: 10.18295/squmj.2016.16.02.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Boateng D, Wekesah F, Browne JL, Agyemang C, Agyei-Baffour P, de-Graft Aikins A, et al. Knowledge and awareness of and perception towards cardiovascular disease risk in sub-Saharan Africa: A systematic review. PLoS One. 2017;12:e0189264. doi: 10.1371/journal.pone.0189264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Albadrani AM, Al-Ajlan SS, Alharbi ASE, Alharbi AS, Alharbi SMR. Public awareness of coronary artery disease risk factors in Qassim, Saudi Arabia: A cross-sectional study. IJMDC. 2020;4:593–9. [Google Scholar]
- 14.The Atlas of Heart Disease and Stroke. https://www.who.int/cardiovascular_diseases/resources/atlas/en/
- 15.Wartak SA, Friderici J, Lotfi A, Verma A, Kleppel R, Naglieri-Prescod D, et al. Patients' knowledge of risk and protective factors for cardiovascular disease. Am J Cardiol. 2011;107:1480–8. doi: 10.1016/j.amjcard.2011.01.023. [DOI] [PubMed] [Google Scholar]
- 16.Schweigman K, Eichner J, Welty TK, Zhang Y. Cardiovascular disease risk factor awareness in American Indian communities: The strong heart study. Ethn Dis. 2006;16:647–52. [PubMed] [Google Scholar]
- 17.The top 10 causes of death. [[Last accessed on 2020 Dec 9]]. https://www.who.int/en/news-room/fact-sheets/detail/the-top-10-causes-of-death.
- 18.Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (The INTERHEART study): Case-control study. Lancet. 2004;364:937–52. doi: 10.1016/S0140-6736(04)17018-9. [DOI] [PubMed] [Google Scholar]
- 19.Awad A, Al-Nafisi H. Public knowledge of cardiovascular disease and its risk factors in Kuwait: A cross-sectional survey. BMC Public Health. 2014;14:1131. doi: 10.1186/1471-2458-14-1131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fahs I, Khalife Z, Malaeb D, Iskandarani M, Salameh P. The prevalence and awareness of cardiovascular diseases risk factors among the lebanese population: A prospective study comparing Urban to rural populations. Cardiol Res Pract. 2017;2017:3530902. doi: 10.1155/2017/3530902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Saquib N, Rajab AM, Saquib J, et al. Substance use disorders in Saudi Arabia: a scoping review. Subst Abuse Treat Prev Policy 15, 41. 2020 doi: 10.1186/s13011-020-00285-3. https://doi.org/10.1186/s13011-020-00285-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.World Health Organization. Atlas: substance use in the Eastern Mediterranean Region; 2015. https://applications.emro.who.int/dsaf/emropub_2017_19560.pdf. [Google Scholar]
- 23.Saquib N, Rajab AM, Saquib J, AlMazrou AR. Substance use disorders in Saudi Arabia: A scoping review. Subst Abuse Treat Prev Policy. 2020;15:41. doi: 10.1186/s13011-020-00285-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ford ES, Ajani UA, Croft JB, Critchley JA, Labarthe DR, Kottke TE, et al. Explaining the decrease in US deaths from coronary disease, 1980-2000. N Engl J Med. 2007;356:2388–98. doi: 10.1056/NEJMsa053935. [DOI] [PubMed] [Google Scholar]
- 25.Wijeysundera HC, Machado M, Farahati F. Association of temporal trends in risk factors and treatment uptake with coronary heart disease mortality. JAMA. 2010;303:1841–7. doi: 10.1001/jama.2010.580. [DOI] [PubMed] [Google Scholar]
- 26.Whayne T, Saha S. Genetic risk, adherence to a healthy lifestyle and ischemic heart disease. Curr Cardiol Rep. 2019;21:1. doi: 10.1007/s11886-019-1086-z. [DOI] [PubMed] [Google Scholar]
- 27.Palmieri L, Bennett K, Giampaoli S, Capewell S. Explaining the decrease in coronary heart disease mortality in Italy between 1980 and 2000. Am J Public Health. 2010;100:684–92. doi: 10.2105/AJPH.2008.147173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Cannon CP. Time to treatment of acute myocardial infarction revisited. Curr Opin Cardiol. 1998;13:254–66. doi: 10.1097/00001573-199807000-00006. [DOI] [PubMed] [Google Scholar]
- 29.Mackintosh JE, Murtagh MJ, Rodgers H, Thomson RG, Ford GA, White M. Why people do, or do not, immediately contact emergency medical services following the onset of acute stroke: Qualitative interview study. PLoS One. 2012;7:e46124. doi: 10.1371/journal.pone.0046124. [DOI] [PMC free article] [PubMed] [Google Scholar]