

Abstract
Objective:
While psychological issues in epilepsy patients have been studied extensively, the phenomena of self-concept and self-security have not been adequately addressed in such patients. Therefore, the aim of the current study is to assess the levels of psychological self-security and self-concept among Saudi epilepsy patients.
Methods:
A case-control study was conducted on adult patients with epilepsy from the Epilepsy Monitoring Unit at King Fahad Medical City in Riyadh, Saudi Arabia. Healthy controls were obtained from the community. Demographic data including age, gender and education level were collected. Self-concept and self-security were assessed using validated scales. Descriptive statistics were obtained, and inferential testing was conducted.
Results:
Data from 145 subjects was entered in the final analysis, including 100 patients with epilepsy and 45 controls (females = 32%). A significantly higher level of psychological insecurity was found in PWE (people with epilepsy) compared to controls. No significant difference was noticed on self-concept level between PWE versus controls. Education level was significantly lower in PWE than in controls. Those with higher education levels scored lower on psychological insecurity, although this effect disappeared when the data were split by health status.
Conclusion:
Level of psychological self-security was higher in PWE than controls, while no difference in self-concept was observed. This study highlights the areas of focus needed in epilepsy-related social services in order to improve the psychological wellbeing of patients with epilepsy.
Keywords: Epilepsy, psychology, self-security, self-concept, Saudi Arabia
Introduction
Epilepsy is a common neurological problem with a reported global prevalence of 1%[1] and a prevalence of 6.54 per 1000 in Saudi Arabia.[2] Patients with epilepsy (PWE) are not only exposed to physical risks including falls and burns, but also face social and psychological stigmatization, isolation, lack of understanding, and unemployment, and insecurity because of the unpredictable nature of seizures.[3] Psychiatric disorders and cognitive impairment are usual complications of epilepsy leading to poor prognosis.[4,5] Therefore, psychological integrity is crucial for patient acceptance and a positive attitude towards the disease and act as cornerstones of disease control and good patient outcomes.[6]
Although knowledge about epilepsy is increasing in certain societies, negative attitudes towards PWE are still widely prevalent.[7]
Life stressors, severity and type of illness, and social and family support affects the perception of self-concept in an epileptic patient. Most of the patients suffer from poor self-concept owing to frequent seizures like spouse separation and social isolation as well as poor academic performance.[8] Therefore, the adults may be susceptible to poor self-concept. An improved self-concept may lead to better patient compliance to treatment.
Self-concept defined by Baumeister as the individual's belief about himself or herself, including the person's attributes and who and what the self is[9] while psychological security denotes the level of the individual's feeling of, freedom from fear, anxiety, and disorder. Based on Maslow's definition it is comprised of the feeling of being beloved, receptive to others, and the individual recognition that environment is friendly and hopeful, that the individual doesn't have the feeling of being threatened or in danger.[10]
Social and cultural factors directly affect the psychological well-being and behavior of PWE, including fear of social stigma which leads to adverse effects on his psychological wellbeing[11] found that a large percentage of PWE felt stigmatized, and highlighted increased social support, and efforts to spread knowledge and awareness across the community, as areas of particular concern that would help counteract this stigma.
While the psychological issues faced by PWE have been studied extensively, the issues of self-concept and self-security have yet to be addressed adequately in such patients. Therefore, the aim of the current study is to investigate the effect of epilepsy on an individual's level of self-security and self-concept, to determine if there is any relationship between self-security and self-concept and psychosocial variables, and whether these phenomena are affected by demographic variables.
Methods
A case control study was conducted at King Fahad Medical City, after approval by the Institutional Review board at King Fahad Medical City. Ethics approval obtained on May 15, 2016 IRB Number: 11-183.
Participants
Participants included adult PWE from the Epilepsy Monitoring Unit at King Fahad Medical City (KFMC) in Riyadh (N = 100), and matched controls from the community (N = 45) during 2013 and 2015. 68% were male, and 32% were female. Participant mean age was 32 [SD = 11.03; see Figure 1]. Self-concept and self-security were measured in all participants.
Figure 1.
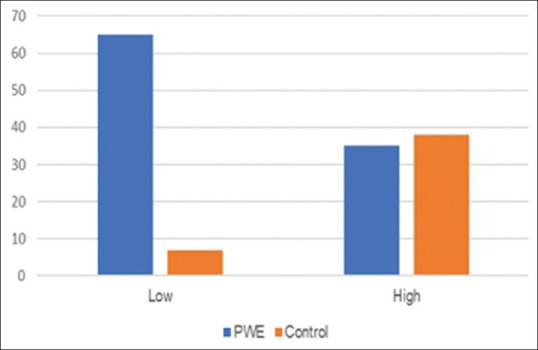
Self-security level in PWE and controls
Materials
Psychological security scale
The psychological security scale used in the study was a modified version of the scale prepared Maslow.[10] The new version was validated for a Saudi context.[12] It consists of 75 statements, each with a 3-point Likert-scale response. A higher score on this scale indicates a lack of psychological security and psychological uncertainty. Reliability analysis showed good reliability (α =0.98).
Self-concept scale
The scale was prepared by Instructional Objectives Exchange (IOX) in the United States of America, it was standardized by Fathy Mustafa Al-Zayat. Arabic version was translated and validated by Alshehri.[13] The scale was designed to examine the self-view a person brings to specific areas of experience. Each area is important to contribute to the overall self-concept. Comparing scores on the self-concept scale will provide a picture of areas of relative strength and vulnerability for subjects. It consists of 78 questions, with the dichotomous answers apply/not apply. The scale includes four dimensions of the self-concept; three of them related to other factors through them the self-concept was formulated such as the family, peers and the school, while the fourth dimension reflects the general self-concept.
Statistical analysis
Data were analyzed using SPSS computer software package for Windows (Version 22). Significance level (α) was set at (P < 0.05).
Results
Data for 145 subjects were included in the final analysis.
Self-security
Levels of self-security for the two groups were compared using an independent samples t-test. PWE showed a significantly lower level of self-security (M = 2.73, SD =0.56) compared to controls (M = 2.18, SD =0.41), t (143) =5.96, p < .001 [see Figure 1].
Self-concept
To determine if there was an effect of group membership on answers on the nominal self-concept scale, response frequency was calculated for 'yes' and for 'no' responses. Independent samples t-tests show no difference in frequency of yes responses between PWE (M = 42.4, SD = 6.83) and controls (M = 40.49, SD = 6.24), t (143) =1.6, P = .112, and no difference in frequency of no responses between PWE (M = 35.44, SD = 6.83) and controls (M = 36.13, SD = 6.12), t (143) = -.583, P = .561 [see Figure 2].
Figure 2.
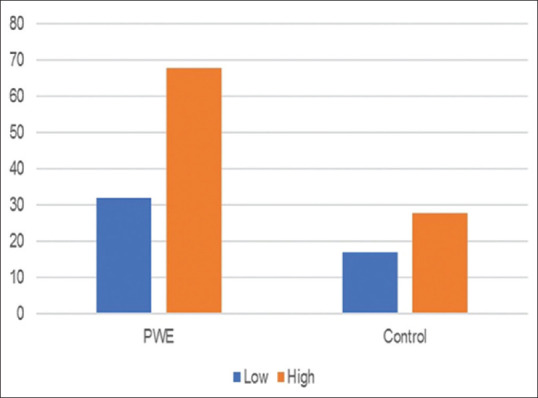
Self-concept level in PWE and controls
Education level
Educational level among the study sample results showed that 37% had a university degree. Chi-square showed that there were significant differences in education levels between groups, χ2 (4, N = 138) =25.95, p < .001, with PWE more likely to have received basic education, and controls more likely to have received a higher-level education. Furthermore, a one-way ANOVA showed that participants differed significantly on their level of self-security based on their education level, F (4, 133) =3.92, P = .005, with those in the lowest education level bracket (elementary) having higher levels of psychological insecurity (M = 2.78, SD =0.49) than those in the highest education level bracket (postgraduate; M = 1.98, SD =0.28; [see Figure 3].
Figure 3.
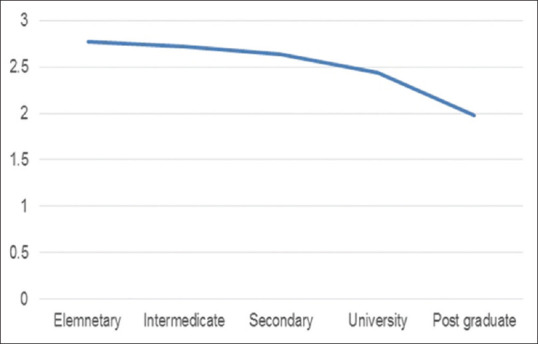
Self-security as a function of educational level
Discussion
Epilepsy is a chronic disease that affects the patients' quality of life and necessitates the development of coping strategies. Impaired self-concept or self-security may hinder this development.[6]
The current study showed that PWE differ from healthy controls on levels of self-security, but show no such difference in self-concept. This suggests that PWE have an impaired level of psychological security. This effect could be due to social and cultural beliefs towards epilepsy, which necessitates the development of defense mechanisms. This could also be exasperated by anxiety surrounding seizures.
The attitudes and opinions of the general population towards epilepsy has been studied in several countries, all of which highlight the crucial need for population awareness as it is often a taboo subject, which fuels misunderstanding regarding the nature of epilepsy, and causes PWE to fear social stigma.[11,14,15] In Saudi Arabia, a recent study showed that while the general public is becoming more knowledgeable about epilepsy, it is not adequate, and attitudes towards epilepsy remain poor.[16,17] These societal attitudes and behaviors may lead PWE to develop personal defenses, and may lead to impaired levels of psychological security.
The current study showed no significant difference between PWE and controls in self-concept. It is possible that this may be attributed to familial support and parents' understanding of the disease. Indeed, familial support was reported to have a great impact on self-concept and psychological wellbeing of PWE.[16,18,19] Patient acceptance and positive attitude are cornerstones in disease control and better outcomes.[6] Previous reports showed that knowledge and attitudes of parents of PWE were better than those of controls.[20,21] Future research should aim to measure social support for PWE to determine if this contributes to the individual's self-concept.
Education level was found to be lower in PWE than in controls, highlighting the effect that epilepsy has on education and learning. Previous research has shown that chronic diseases such as epilepsy can affect school attendance as well as cognitive functioning and learning ability.[22] It is worth noting that participants varied on their psychological security scores with respect to their education level, with those receiving lower levels of education reporting higher levels of psychological insecurity. This may be a reflection of the psychological advantages of further education, since no effect was found once the data were split based on health status. It is interesting to note the psychological advantages of education, which suggest that having an educational component to psychological interventions in PWE may help to improve their overall psychological security and wellbeing. However, further research is needed before that conclusion can be drawn.
Limitations
It would have been useful to include a measurement of the effect that epilepsy has had on the lives of the PWE who took part in this study, such as the Life Changes in Epilepsy Scale.[23] This may allow for identification of specific areas that affect an individual's psychological security.
Conclusion
Psychological security may be impaired in epilepsy patients. The current study highlights the need for the inclusion of interventions to improve psychological security in social services for PWE. The findings also highlight the role of education in developing sound psychological security, and the potential for future research in this area. It may also be useful to include measures on symptoms, such as frequency and severity of seizures, in order to determine an effect of disease severity.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Reynolds EH. The ILAE/IBE/WHO epilepsy global campaign history. International League Against Epilepsy. International Bureau for Epilepsy. Epilepsia. 2002;43((Suppl 6)):9–11. doi: 10.1046/j.1528-1157.43.s.6.5.x. [DOI] [PubMed] [Google Scholar]
- 2.Al Rajeh S, Awada A, Bademosi O, Ogunniyi A. The prevalence of epilepsy and other seizure disorders in an Arab population: A community-based study. Seizure. 2001;10:410–4. doi: 10.1053/seiz.2001.0602. [DOI] [PubMed] [Google Scholar]
- 3.Jacoby A. Epilepsy and stigma: An update and critical review. Curr Neurol Neurosci Rep. 2008;8:339–44. doi: 10.1007/s11910-008-0052-8. [DOI] [PubMed] [Google Scholar]
- 4.Edeh J, Toone BK, Corney RH. Epilepsy, psychiatric morbidity, and social dysfunction in general practice: Comparison between hospital clinic patients and clinic nonattenders. Cogn Behav Neurol. 1990;3:180–92. [Google Scholar]
- 5.Chang HJ, Liao CC, Hu CJ, Shen WW, Chen TL. Psychiatric disorders after epilepsy diagnosis: A population-based retrospective cohort study. PloS One. 2013;8:e59999. doi: 10.1371/journal.pone.0059999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Westerhuis W, Zijlmans M, Fischer K, Van Andel J, Leijten FS. Coping style and quality of life in patients with epilepsy: A cross-sectional study. J Neurol. 2011;258:37–43. doi: 10.1007/s00415-010-5677-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Teferi J, Shewangizaw Z. Assessment of knowledge, attitude, and practice related to epilepsy: A community-based study. Neuropsychiatr Dis Treat. 2015;11:1239. doi: 10.2147/NDT.S82328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Whatley AD, DiIorio CK, Yeager K. Examining the relationships of depressive symptoms, stigma, social support and regimen-specific support on quality of life in adult patients with epilepsy. Health Educ Res. 2010;25:575–84. doi: 10.1093/her/cyq001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Baumeister RF. Identity, self-concept, and self-esteem: The self lost and found. Handbook of Personality Psychology. 1997:681–710. [Google Scholar]
- 10.Maslow AH. A theory of human motivation. Psychol Rev. 1943;50:370. [Google Scholar]
- 11.Bautista RE, Shapovalov D, Shoraka AR. Factors associated with increased felt stigma among individuals with epilepsy. Seizure. 2015;30:106–12. doi: 10.1016/j.seizure.2015.06.006. [DOI] [PubMed] [Google Scholar]
- 12.Agraa I. The sense of psychological security and the impact of some variables Among Students at An-Najah National University. Master's thesis. An-Najah Nahional University, Naples Palestine. 2005. [[Last accesed on 2019 Jan 07]]. Available from: https://scholar.najah.edu/sites/default/files/all-thesis/322.pdf .
- 13.Alshehri S. Social stigma and its relationship to the self- concept in special needs subjects in Riyadh City. Master's thesis. Imam Mohammed Bin Suad Isamlic University, Riyadh, Saudi Arabia) [[Last accesed on 2019 Jan 07]]. Avaialble from: http://ecat.kfnl.gov.sa: 88/ipac20/ipac.jsp?session .
- 14.Almutairi AM, Ansari T, Sami W, Baz S. Public knowledge and attitudes toward epilepsy in Majmaah. J Neurosci Rural Pract. 2016;7:499. doi: 10.4103/0976-3147.188622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Shahbo GMAEM, Bharathi B, Daoala AL. Comparative study on knowledge, attitudes and believes of epilepsy among communities of Egypt and Kingdom of Saudi Arabia. IOSR J Nurs Health Sci. 2014;3:97–107. [Google Scholar]
- 16.Alkhamees HA, Selai CE, Shorvon SD. The beliefs among patients with epilepsy in Saudi Arabia about the causes and treatment of epilepsy and other aspects. Epilepsy Behav. 2015;53:135–9. doi: 10.1016/j.yebeh.2015.10.008. [DOI] [PubMed] [Google Scholar]
- 17.Alaqeel A, Kamalmaz H, Al-Shaar HA, AlZahrani I, Alaqeel A, Aljetaily S, et al. Evaluating the initial impact of the Riyadh epilepsy awareness campaign. Epilepsy Behav. 2015;52:251–5. doi: 10.1016/j.yebeh.2015.09.010. [DOI] [PubMed] [Google Scholar]
- 18.Amir M, Roziner I, Knoll A, Neufeld MY. Self-Efficacy and social support as mediators in the relation between disease severity and quality of life in patients with epilepsy. Epilepsia. 1999;40:216–24. doi: 10.1111/j.1528-1157.1999.tb02078.x. [DOI] [PubMed] [Google Scholar]
- 19.DiIorio C, Shafer PO, Letz R, Henry T, Schomer DL, Yeager K, et al. The association of stigma with self-management and perceptions of health care among adults with epilepsy. Epilepsy Behav. 2003;4:259–67. doi: 10.1016/s1525-5050(03)00103-3. [DOI] [PubMed] [Google Scholar]
- 20.Frank-Briggs AI, Alikor EAD. Knowledge and attitudes of parents toward children with epilepsy. Ann Afr Med. 2011;10:238–42. doi: 10.4103/1596-3519.84706. [DOI] [PubMed] [Google Scholar]
- 21.Shehata GA, Mahran DG. Egyptian students' guardians' knowledge, attitude and predictors of negative attitude of epilepsy in Assiut city. J Epidemiol Global Health. 2014;4:87–95. doi: 10.1016/j.jegh.2013.09.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Brabcova D, Krsek P, Kohout J, Jost J, Zarubova J. Academic self-concept in children with epilepsy and its relation to their quality of life. Neurol Res. 2015;37:288–94. doi: 10.1179/1743132814Y.0000000458. [DOI] [PubMed] [Google Scholar]
- 23.Miller WR, Bakas T, Weaver MT, Buelow JM, Sabau D. The life changes in epilepsy scale: Development and establishment of content and face validity. Clin Nurse Spec CNS. 2015;29:95–9. doi: 10.1097/NUR.0000000000000109. [DOI] [PMC free article] [PubMed] [Google Scholar]