

A 50-year-old man was admitted with complaints of Canadian Cardiovascular Society class III angina precipitated by exertion. He had inferior wall myocardial infarction (IWMI) a month back and received intravenous thrombolysis with alteplase. His electrocardiogram showed an incomplete right bundle branch block with Q waves in II, III, and aVF leads (Fig. 1). Transthoracic echocardiogram showed mild left ventricular dysfunction with an ejection fraction of 45% and hypokinesia in inferior and lateral walls.
Figure 1.

Baseline electrocardiogram (ECG) showing normal sinus rhythm, incomplete right bundle branch block (RBBB) with Q waves in leads II, III, and aVF
Subsequently, he was taken for a coronary angiogram, which revealed a significant stenosis in the left circumflex artery (LCx) and an anomalous diagonal artery originating from the distal left main coronary artery (LMCA) (Fig. 2). This anomalous diagonal artery was diseased, with a significant obstruction, and resulted in a lateral wall injury. Other vessels, including the left anterior descending and right coronary arteries, were normal. The patient was then analyzed by coronary computed tomography angiogram to delineate the anatomy better, which confirmed the anomalous vessel as the first diagonal branch, supplying the lateral wall of the left ventricle (Fig. 3).
Figure 2.
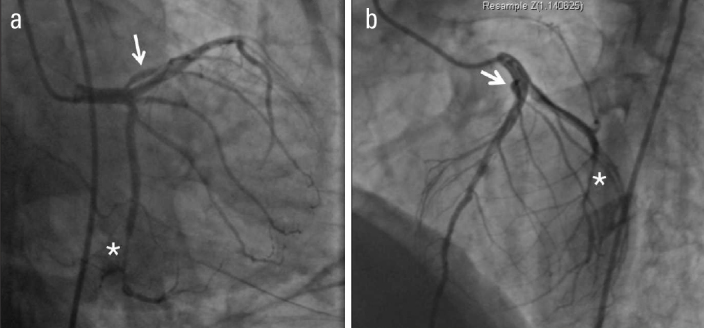
Invasive coronary angiography. Right anterior oblique-caudal view (a) and left anterior oblique-cranial view (b) showing diseased distal left circumflex coronary artery (*) and anomalous diagonal artery (arrow) arising from the distal left main artery just before the left anterior descending artery origin. There is a stenosis at the bifurcation point of this anomalous diagonal vessel
Figure 3.

Cardiac computed tomographic angiogram confirms the anomalous vessel to be a diagonal artery (arrow) arising from the distal left main coronary artery (asterisk) with a stenosis at its bifurcation in modified left anterior oblique (LAO) cranial views
Our index case had an exceptionally large anomalous diagonal artery with a huge area of myocardium being supplied by this vessel. IWMI was caused by the obstruction of LCx artery and lateral wall injury was the result of a significant stenosis in the large anomalous diagonal artery originating from LMCA. This anomaly of diagonal artery origin is very rare and can pose a significant challenge in coronary interventions. The patient underwent a successful LCx angioplasty with a drug eluting stent; however, the coronary guidewire could not be negotiated through the anomalous diagonal artery. Hence, he was managed conservatively for diagonal artery stenosis and remained stable at 1-year follow up.
Footnotes
Informed consent: Informed consent was obtained from the patient.