

Abstract
The terminal sterilization of sterile orthopedic implants is a key process that, in addition to providing sterility, changes the material properties of the product and packaging. These changes might be observed during functionality testing and/or biological evaluation. We are establishing an additional sterilization process that appears promising from both a technical and business perspective. Our project aims to add X-ray sterilization to the established gamma sterilization for metallic hip and shoulder implants. To limit complexity, we started with a narrow product range. The main steps of our project journey are described here. Given that X-ray sterilization remains relatively new in terms of understanding the changes that might occur for product materials and functionality compared with changes observed following gamma radiation processing, this article highlights key steps in the change from gamma ray to X-ray sterilization.
Gamma sterilization has been used for more than 60 years in the terminal sterilization of metal orthopedic implants. In addition to its longtime proven track record, its advantages include straightforward process monitoring, processing of large volumes at one time, process reliability, and process stability. However, gamma sterilization processes currently face obstacles. For instance, the legal/normative requirements for transport and disposal of cobalt-60 are increasing and the demand is growing faster than future capacities.1,2 As a result, delays in the sterilization supply chain are a concern.
The search for an efficient back-up solution for gamma sterilization and the introduction of new products that require better radiation penetration depth due to their design have increased focus on X-ray sterilization. X-ray is an irradiation process that has much in common with gamma. The two sterilization methods are comparable in terms of their sterilization principle (photons), with some technical advantage for X-ray regarding better dose uniformity and less oxidative stress for certain polymers.3 Principally, any sterilization change could affect the final product safety and performance and therefore must be supported by concrete scientific data. We have formed a multidisciplinary project team to cover all relevant aspects of a sterilization process change.
Initial Considerations
For some time, changing the sterilization process from gamma ray to X-ray has been discussed among internal scientific experts before a business plan was enacted. This plan highlighted the technical advantages of X-ray sterilization, such as good material compatibility, high penetration depth, fast processing times, and the potential to replace cobalt-60.3 In addition, X-ray is considered a reliable, price-stable, and sustainable irradiation source for the future. Given the project's complexity, costs, and lengthy timeline, an experienced project lead with a good technical understanding and a proven background in dealing with complex projects was selected.
In this project, it was decided to limit the product scope to the product family of cobalt-chromium-molybdenum (CoCrMo) ball implants. Because of its shielding properties, this high-density material is a challenge for radiation processing. For some implant geometries, the gamma process efficacy is low because they can only be treated at certain positions within the irradiation container (in this case, a pallet). For the purpose of this project, an X-ray facility that also uses pallets as irradiation containers was selected. A single pallet configuration accommodating all CoCrMo ball implants, from smallest to biggest, offers the best efficacy. The project was intended as a pilot to establish best practices for other products that might undergo a similar sterilization process change in the future.
Project Team and Materials
The team includes individuals from different disciplines to represent all aspects of the project (Figure 1).
Figure 1.

Interaction of task owners and project lead.
The product scope involves metallic hip and shoulder implants and their packaging and labeling materials. The implants' geometries are balls, consisting of very dense CoCrMo. Their design (blind hole inside a thick material layer) is challenging to radiation sterilization because of shielding effects of the material. Another physical challenge is that dense metal can be subject to radioactivation if exposed to X-ray, because of the higher irradiation energy level compared with gamma.4
Product packaging consists of conventional polyethylene terephthalate glycol (PETG) trays with high-density polyethylene fiber lids, and carton/paper as protective packaging and labeling components.
Project Tasks
The project consists of five essential tasks: (1) supplier qualification; (2) dose mapping/performance qualification (PQ) for the X-ray pallet configuration; (3) establishing the sterilization dose; (4) establishing the maximum acceptable dose, including packaging configuration and product validation, material activation testing, and biological evaluation; and (5) internal documentation/regulatory requirements.
The relationship of project tasks is shown in Figure 2. In the following sections, these project tasks are presented in more detail.
Figure 2.
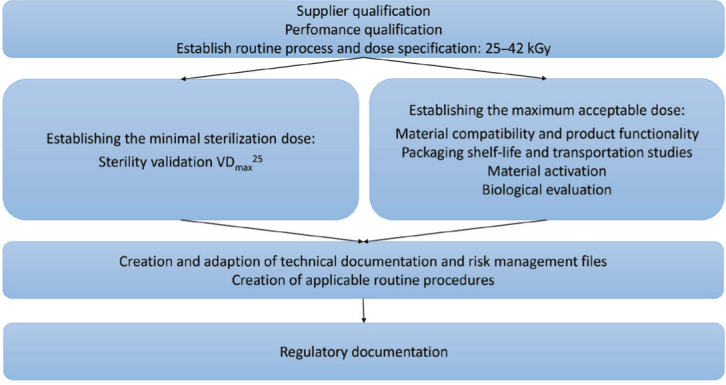
Project task organization. Abbreviation used: VDmax, verification dose maximum.
Supplier Qualification
Supplier qualification includes an on-site audit of the contract sterilizer and a thorough review of all applicable processes (i.e., of the X-ray accelerator and respective installation and operational qualification documentation and formal supplier process approval, such as related to risk management and general quality aspects). Our company had already approved this sterilization site for gamma sterilization, which simplified qualification of ther general good manufacturing practice system. Prior to execution of the X-ray PQ, the respective processes had been audited and passed.
Dose Mapping: PQ
The aim of the PQ is to provide a safe and efficient process for routine sterilization of products, within the target dose range. Before starting the PQ, an optimized X-ray pallet configuration (irradiation container) had been designed, taking into account the quantity of produced CoCrMo heads and capability of the X-ray accelerator to reach the specified sterilization parameters. First study runs have been performed and indicated good feasibility. Subsequently, dummy products have been produced to build the minimum and maximum pallet configurations, representing the biggest and the smallest products (Figures 3 and 4) and pallet loading configurations, respectively. As ball heads are known to have a shielding effect inside the conus, a nonstandard PQ, including a triplicate extended dose map (typical PQ grid plus additional strategically located dosimeters), is performed for each (the minimum and maximum configuration). The additional dosimeters are placed directly inside the product to account for localized areas of high density and the shielding effect.
Figure 3.
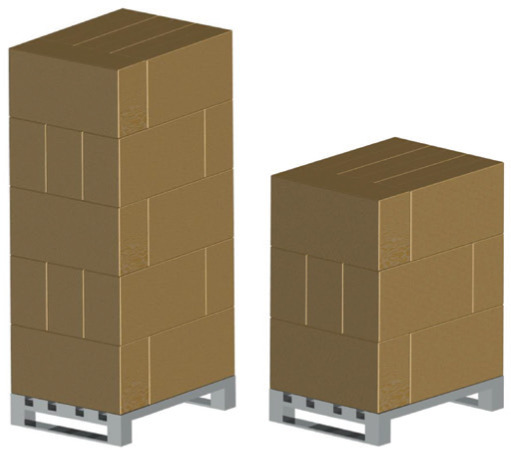
Maximal and minimal X-ray pallet configuration.
Figure 4.

Comparative thickness of maximum- and minimum-density products.
Briefly summarized, the PQ demonstrates that the new X-ray pallet configuration shown in Figure 3, which ranges from 60 × 80 × 92 to 60 × 80 × 154 cm3 and covers a density range from 0.09 to 0.21 g/cm3, can be successfully irradiated with X-rays, leading to a dose range of 25 to 42 kGy and a dose uniformity ratio (DUR) of 1.28. For comparison, the same irradiation container used in a gamma irradiator provided a DUR of 1.64.
Establishing the Sterilization Dose
The sterilization dose for this product family in gamma sterilization processing is 25 kGy. The PQ testing has demonstrated that the X-ray process is capable of treating the X-ray pallet configuration with a minimum of 25 kGy. Although gamma ray and X-ray radiation are related, clause 8.4.2 of ANSI/AAMI/ISO 11137-1 states that transference of a sterilization dose to a radiation source different from that on which the dose was originally established shall not be permitted unless data are available to demonstrate the difference in irradiation conditions of the two radiation sources have no effect on the microbicidal effectiveness.5 Further guidance recommends one dose verification experiment using X-ray.6
Because the guidance for transferring from one radiation source to another is dependent on the circumstances, it was decided to perform a full-dose establishment according to ANSI/AAMI/ISO 11137-27 and the technical information report ANSI/AAMI/ISO TIR13004.8 With constant production processes and consistently low bioburden, which previously was known from gamma validation and periodic monitoring, and assuming that the dose of gamma ray and X-ray will have the same microbicidal efficacy, the dose establishment itself is not considered a challenge. All applicable standards and processes fundamentally are the same, independent of the chosen radiation source, and existing internal procedures could be applied after addition of X-ray sterilization to the respective internal documents.
More explicitly, the subsequent steps are taken to fulfill the requirements of 11137-15 for establishing the minimal sterilization dose:
Adaption of internal processes, such as grouping, sterility validation, and dose audit to include X-ray sterilization as possible process
Review of affected product scope for X-ray group formation and determination or representative worst-case items, according to ISO 11137-17
Dose establishment based on method VDmax25 or VDmax20, according to 11137-27 or TIR13004,8 respectively
Implementation of routine monitoring dose audit processes according to 11137-27 (Figure 5)
Figure 5.
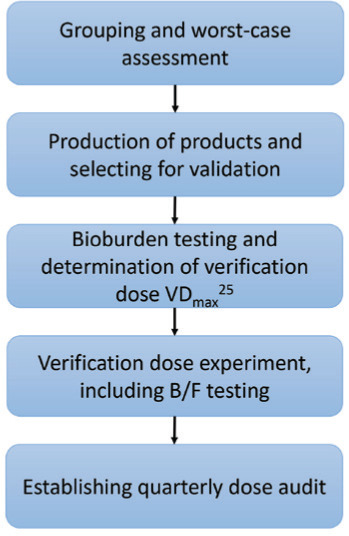
Steps for establishing the minimal sterilization dose (sterility assurance level of 10−6). Abbreviations used: B/F, bacteriostasis/fungistasis; VDmax, verification dose maximum.
Because the bioburden on product is very low (far below 1,000 cfu/item), 25 kGy is sufficient to ensure a sterility assurance level of 10−6 for gamma-sterilized CoCrMo heads and comparability of sterilization efficacy is expected. Therefore, establishing the sterilization dose using X-ray radiation was considered a lower priority and currently is in progress.
Establishing the Maximum Acceptable Dose
The maximum dose shall be established to consistently meet the specified functional requirements throughout the defined lifetime of the medical device. Functional requirements include the functionality and safety of the device and its packaging. Per 11137-1,5 assessment of the validity of the maximum acceptable dose for a radiation source other than the one used for establishing the dose originally should take into consideration dose rate and product temperature during irradiation. For our simple metallic product packaged in a blister package, the higher dose rate is not expected to have new undesired effects. A product qualified at a low-dose rate typically will require minimal qualification to demonstrate material compatibility at a higher dose rate, as stated in AAMI TIR17.9 As up to 45 kGy is known to be acceptable for gamma-sterilized CoCrMo heads and comparability of radiation source impact on product and packaging is expected, establishing the maximum acceptable dose as 45 kGy was also anticipated for X-ray. Information to substantiate this is provided below.
Product validation. The implant product scope is made of metal only. According to TIR17, metals are exceptionally stable under the influence of irradiation.9 They show excellent stability when undergoing a single sterilization process with an irradiation dose below 50 kGy and they are also likely to remain stable when resterilized with an irradiation dose up to 100 kGy. The higher dose rate of the X-ray radiation process is not expected to have any impact on the metallic product. Therefore, no further assessment of the product following exposure to X-ray processing with regard to material compatibility or product functionality testing is deemed necessary for this pure metal product family.
Packaging. Gamma ray and X-rays differ in dose rate, in that a low-dose rate of gamma is considered worst case compared with a high-dose rate of X-ray.9 The higher dose rate of X-ray leads to a drastic reduction in exposure time, resulting in considerably fewer denaturing effects on products after irradiation (e.g., material stability, color change).10 Section 5.2 of TIR17 states that, as a result of enhanced oxidative effects, material qualification performed at a low-dose rate can reveal greater degradation (e.g., embrittlement) than at a high-dose rate. “Consequently, a material that formerly qualified at a low-dose rate (gamma) typically will require minimal qualification to demonstrate material compatibility at a higher dose rate (electron beam [e-beam]).”9 Therefore, packaging stability and transportation testing with gamma can be considered to represent the worst case and cover X-ray irradiation as well.
The company has broad experience with sterilization as gamma and electron beam (e-beam) radiation, and maximal sterilization doses up to 45 kGy have been established routinely without having a negative effect on packaging configurations. As gamma is considered worst case, X-ray doses up to 45 kGy are not expected to have a negative effect on the packaging. However, this project functions as a pilot and X-ray is new to the company. Therefore, it was decided to include a full stability and performance testing validation (according ANSI/AAMI/ISO 11607-111) within this project to generate data for X-ray. This will enable us to make direct comparisons with data generated for gamma and further strengthen the approach that minimal qualification for the packaging will be sufficient to demonstrate material compatibility for X-ray—if the material already is adequately qualified for gamma irradiation. Maximum irradiation temperature has been monitored during the X-ray dose mapping and confirmed not to be a challenge for the packaging.
Packaging tests are ongoing and, thus far, only preliminary data are available. Initial analysis of packaging configurations and materials with worst-case X-ray sterilization runs (final dose >100 kGy) showed that the sterile barrier system maintained integrity/sterility until the point of use. The long-term compatibility will be investigated with a stability study that includes material characterization and interaction. The study will be performed with sealed PETG trays with high-density polyethylene fiber lids, and worst-case process limits using accelerated aging and real-time aging protocols. To represent worst-case conditions, the actual applied dose will be 50 to 84 kGy, which includes a considerable safety margin above 45 kGy. Performance of the packaging system will be conducted with the most challenging devices within a sterile barrier system. These studies will provide substitutionary evidence that the packaging material and/or system will withstand the X-ray sterilization process, attain the required conditions for sterilization within the packaging system, and ensure its suitability for use.
Material activation testing. Section 5.3 of 11137-1 requires performance of studies of the effects of radiation on product.5 Although expected to be negligible, the induction of radionuclides by X-rays (generated from a 7.5-MeV accelerator) in the irradiated products has to be assessed. Assessment should be based on available literature, measurement, and/or modeling of induced radioactivity.
For the material activation study, two different samples with representative material are provided. One container has all applicable packaging/labeling components, and a second container has samples of all represented CoCrMo alloy materials in the scope. Both containers are treated with a sterilization dose above the maximum allowed 45 kGy, then sent immediately to the analytical testing laboratory. Small activation levels for some elements can be expected for dense materials, including CoCrMo alloys. Co, Cr, and Mo are the three major elements of the CoCrMo ball heads (CoCrMo low-carbon alloy and CoCrMo high-carbon alloy per ASTM F153712).
For all used packaging and labeling components, the applied X-ray dose (>45 kGy) has not induced activation, whereas the different metal implants show very slight induction of Co-60, Cr-51, and Mo-99 (<20 Bq/kg for each radioisotope). The activity found in the activation study of the X-ray sterilization for Cr-51, Co-60, and Mo-99 is lower than the activity of natural sources, such as radioactivity in food or the environment itself.13,14 All radiation levels are much lower than the acceptance limit stated in Swiss law 814.501.2 In addition, nonirradiated control samples will be tested for their activity, in order to have a solid basis for comparison. In addition, X-ray–irradiated devices will be included in the biological evaluation.
Biological evaluation. Metal alloys have been used as raw materials in medical devices for decades. Therefore, substantial literature is available regarding several metal alloys, thereby establishing the alloys as acceptable with an appropriate host response upon exposure.15,16 Potential activation must be discussed and evaluated in the context of naturally occurring radiation, which is ubiquitous in nature (e.g., in foods such as coffee and bananas, in the environment).13,14 Although all induced radiation levels are much lower than the acceptance limit stated in the Swiss law 814.501, this law is not particularly relevant to medical devices and no standard document specifying allowed radioactivity levels for implantable permanent medical devices exists thus far.
Potentially, packaging materials made of polymer can leach substances (e.g., monomers, antioxidants, plasticizers), which subsequently could be transferred to the product surface. Leaching can be induced directly or indirectly (i.e., through generation of heat or ozone) by the sterilization process. Although the delivered dose is the same for gamma ray and X-ray, the indirect effect is less expected for X-ray. Because of the higher dose rate, the X-ray treatment is shorter and products are less exposed to ozone.3 In this study, the temperature during X-ray treatment was lower, with a maximum temperature of 45°C compared with 57.5°C for our established gamma sterilization process. A chemical characterization of the product after X-ray radiation, according ISO 10993-18,17 will provide supportive data.
Internal Documentation/Regulatory Requirements
A final part the project will involve the updating of internal documentation. This process will affect all internal procedural steps, including product loading patterns for X-ray pallet, process failure mode and effects analysis, labeling (e.g., instructions for use), the risk management file and design history file, and technical and regulatory documentation (based on discussions with regulatory bodies).
Conclusion
The gamma ray and X-ray sterilization methods are considered closely related and the applicable standards (11137-1 to -45,7,18,19) cover both. However, a specific understanding is still needed regarding a company's product and the respective processes used, in order to determine the steps for changing from gamma ray to X-ray. Our project provides an example of development and validation steps for a metallic product group, which principally are also necessary for an initial gamma sterilization implementation (i.e., supplier qualification, PQ of the sterilization loading configuration, establishing the minimal/maximal sterilization dose, biological evaluation of X-ray–sterilized devices). Specific to X-ray, additional material activation studies might be required. The validation results obtained thus far offer promising evidence of X-ray being a suitable alternative for the sterilization of our CoCrMo heads.
Despite existing scientific data showing comparability of the two processes regarding microbicidal effectiveness20–22 and material compatibility,3,9 data from gamma sterilization validations were not used to establish X-ray as a second sterilization process. This can be considered a very conservative approach—one that exceeds essential requirements—because according to TIR17, material compatibility and packaging studies could be limited to minimal qualification instead of full validation.9
Considerable effort is needed to establish X-ray as a second sterilization process, but we believe that a great benefit will be realized in the near future: increasing the sustainability of our sterilization supply. Regulatory agencies may be less familiar with the use of X-ray sterilization technology. Particularly in Europe, where many notified bodies are busy with implementation of the Medical Device Regulation, the approval timeline for such a project might become longer than usual. Mapping the regulatory strategy, collaborating across manufacturers and sterilizers, and involving regulatory agencies early in the process will be important to accelerating shifts in sterilization methods.
References
- 1.van den Brink S, Kleijn R, Sprecher B, Tukker A. Identifying supply risks by mapping the cobalt supply chain. Resources Conservation & Recycling . 2020;156:104743. [Google Scholar]
- 2.Federal Council Swiss Law 814501 Radiological Protection Ordinance 2017 . Bern, Switzerland: Federal Council; 2017. [Google Scholar]
- 3.McEvoy B, Michel H, Howell D, Roxby P. X-ray: an effective photon. Biomed Instrum Technol . 2020;54(suppl. 1):23–30. doi: 10.2345/0899-8205-54.s3.23. [DOI] [PubMed] [Google Scholar]
- 4.Grégoire O, Cleland MR, Mittendorfer J, et al. Radiological safety of medical devices sterilized with X-rays at 7.5MeV. Radiation Physics and Chemistry . 2003;67(2):149–67. [Google Scholar]
- 5.ANSI/AAMI/ISO 11137-1:2006 (R2015)/A2:2019 Sterilization of health care products—Radiation—Part 1 Requirements for development validation and routine control of a sterilization process for medical devices . Arlington, VA: Association for the Advancement of Medical Instrumentation; [Google Scholar]
- 6.Panel on Gamma and Electron Irradiation Change of Irradiation Modalities in Radiation Sterilization of Medical Devices Normative Requirements and Aspects in EN ISO 111371 . www.irradiationpanel.org/app/download/10382868/Change+of+Irradiation+Modalities+Final.pdf Accessed April 6, 2021.
- 7.ANSI/AAMI/ISO 11137-2:2013/(R)2019 Sterilization of health care products—Radiation—Part 2 Establishing the sterilization dose . Arlington, VA: Association for the Advancement of Medical Instrumentation; [Google Scholar]
- 8.ANSI/AAMI/ISO TIR13004:2013/(R)2016 Sterilization of health care products—Radiation—Substantiation of a selected sterilization dose Method VDmaxSD . Arlington, VA: Association for the Advancement of Medical Instrumentation; [Google Scholar]
- 9.AAMI TIR17:2017 Compatibility of materials subject to sterilization . Arlington, VA: Association for the Advancement of Medical Instrumentation; [Google Scholar]
- 10.Dethier P. Industrial Gamma and Xray ‘Same but Different'. http://iiaglobal.com/uploads/documents/IBA.white_paper_-_xray_vs_gamma.pdf Assessed Oct. 27, 2020.
- 11.ANSI/AAMI/ISO 11607-1:2006/(R)2010 Packaging for terminally sterilized medical devices—Part 1 Requirements for materials sterile barrier systems and packaging systems . Geneva, Switzerland: International Organization for Standardization; [Google Scholar]
- 12.ASTM F1537-20:2020 Standard Specification for Wrought Cobalt28Chromium6Molybdenum Alloys for Surgical Implants . West Conshohocken, PA: ASTM International; [Google Scholar]
- 13.World Nuclear Association Radiation and health. www.world-nuclear.org/information-library/safety-and-security/radiation-and-health/nuclear-radiation-and-health-effects.aspx Accessed Nov. 5, 2020.
- 14.Agency for Toxic Substances and Disease Registry Toxicological Profile for Ionizing Radiation . Atlanta, GA: Agency for Toxic Substances and Disease Registry; 1999. [PubMed] [Google Scholar]
- 15.Finnish Institute of Occupational Health Review on Toxicity of Stainless Steel . Helsinki: Finnish Institute of Occupational Health; 2010. [Google Scholar]
- 16.Klaassen CD. Casarett and Doull's Toxicology The Basic Science of Poisons . Vol. 1236. New York, NY: McGraw-Hill; 2013. [Google Scholar]
- 17.ISO 10993-18:2020 Biological Evaluation of Medical Devices—Part 18 Chemical characterization of medical device within a risk management process . Geneva, Switzerland: International Organization for Standardization; [Google Scholar]
- 18.ANSI/AAMI/ISO 11137-3:2017 Sterilization of health care products—Radiation—Part 3 Guidance on dosimetric aspects of development validation and routine control . Arlington, VA: Association for the Advancement of Medical Instrumentation; [Google Scholar]
- 19.ISO/TS 11137-4:2020 Sterilization of health care products—Radiation—Part 4 Guidance on process control . Geneva, Switzerland: International Organization for Standardization; [Google Scholar]
- 20.Tallentire A, Miller A, Helt-Hansen J. A comparison of the microbicidal effectiveness of gamma rays and high and low energy electron radiations. Radiation Physics and Chemistry . 2010;79(6):701–4. [Google Scholar]
- 21.Tallentire A, Miller A. Microbicidal effectiveness of X-rays used for sterilization purposes. Radiation Physics and Chemistry . 2015;107:128–130. [Google Scholar]
- 22.Hansen JM, Fidopiastis N, Bryans T, et al. Radiation sterilization: dose is dose. Biomed Instrum Technol . 2020;54(suppl. 1):45–52. doi: 10.2345/0899-8205-54.s3.45. [DOI] [PubMed] [Google Scholar]