

Supplemental Digital Content is Available in the Text.
Blue light reduces pain and shows antihyperalgesic effects in a human experimental pain model. Therefore, blue light may be a novel therapeutic approach for pain in multiple conditions.
Keywords: Blue light, Treatment, Therapy, Neuropathic pain, Hyperalgesia
Abstract
Introduction:
Chronic pain is a frequent severe disease and often associated with anxiety, depression, insomnia, disability, and reduced quality of life. This maladaptive condition is further characterized by sensory loss, hyperalgesia, and allodynia. Blue light has been hypothesized to modulate sensory neurons and thereby influence nociception.
Objectives:
Here, we compared the effects of blue light vs red light and thermal control on pain sensation in a human experimental pain model.
Methods:
Pain, hyperalgesia, and allodynia were induced in 30 healthy volunteers through high-density transcutaneous electrical stimulation. Subsequently, blue light, red light, or thermal control treatment was applied in a cross-over design. The nonvisual effects of the respective light treatments were examined using a well-established quantitative sensory testing protocol. Somatosensory parameters as well as pain intensity and quality were scored.
Results:
Blue light substantially reduced spontaneous pain as assessed by numeric rating scale pain scoring. Similarly, pain quality was significantly altered as assessed by the German counterpart of the McGill Pain Questionnaire. Furthermore, blue light showed antihyperalgesic, antiallodynic, and antihypesthesic effects in contrast to red light or thermal control treatment.
Conclusion:
Blue-light phototherapy ameliorates pain intensity and quality in a human experimental pain model and reveals antihyperalgesic, antiallodynic, and antihypesthesic effects. Therefore, blue-light phototherapy may be a novel approach to treat pain in multiple conditions.
1. Introduction
Maladaptive chronic pain is estimated to have a prevalence up to 10% and is often associated with anxiety, depression, insomnia, disability, and reduced quality of life.48,51 Chronic pain is one of the most common reasons why patients seek medical care.20 Generally, a multidisciplinary therapeutic approach is necessary. However, many treatment options are either only mildly analgesic or accompanied by deleterious side effects.7,8,18,44,52
Phototherapy is a nascent approach that has been shown to reduce chronic back, neck, and neuropathic pain without any significant side effects reported so far.9,11,14,19,21,42 In addition to low-level laser therapy, several preclinical and clinical studies have suggested the application of light-emitting diodes (LEDs) for the treatment of various conditions involving acute nociceptive and chronic pain.10,12,16,27,30–32,40,45–47,53 Although most studies have focused on the use of red and infrared light, few preclinical and clinical studies have explored the use of lower wavelength light.22,33 In a rat model of acute nociceptive pain, green and to a lesser extent blue light (BL) exhibited thermal analgesic effects.33 Interestingly, a large behavioral screen in zebrafish has revealed a naturally occurring light-sensitive ligand called optovin, which specifically activates transient receptor potential A1 (TRPA1) cation channels. On BL exposure, optovin transiently binds to TRPA1 through cysteine residues.26 This phenomenon has sparked the idea that BL could be used to modulate pain.15
Therefore, we hypothesized that prolonged exposure to BL may reduce spontaneous and evoked pain by modulating activated peripheral nociceptive fibers in human skin. To test this hypothesis, we used a well-described surrogate pain model in healthy volunteers using high-density transcutaneous electrical stimulation (HD-TES).17,28,36 Blue light, red light (RL), or thermal control (TC) treatment was applied through custom-made (home-built) collars in a cross-over fashion. The reduction of numeric rating scale (NRS) pain scores after 1-hour light treatment was assessed as the primary outcome.
2. Materials and Methods
2.1. Subjects
A total of 30 healthy volunteers were recruited. All participants were required to be at least 18 years old. The exclusion criteria were dermatological diseases and regular use of analgesics. The mean habitual life quality was assessed by 7 questions according to the Marburg questionnaire of general life quality.6 The depression and anxiety stress scale was assessed by 21 questions according to Nilges and Essau.37 Detailed information about the subjects is presented in Table 1.
Table 1.
Characteristics of study participants.
| Factor | Mean | SEM | % |
|---|---|---|---|
| Age | 25.53 | 1.43 | — |
| BMI | 22.60 | 0.45 | — |
| Habitual life quality | 4.78 | 0.10 | — |
| DASS | 0.43 | 0.05 | — |
| Menstrual cycle | 12.46 | 2.55 | — |
| Partnership: single | — | — | 53.33: 46.67 |
| Contentment with relationship status | — | — | 90 |
Assessment of age, body mass index (BMI), habitual quality of life, depression, anxiety stress scale (DASS), menstrual cycle, relationship status, and contentment with relationship status. Means are given ±SEM (n = 30).
The aim of the study and different treatments were explained to the subjects only in a broad sense. Participants were blinded for the light treatments applied. All volunteers signed an informed consent form before the start of the experiment. The study was conducted according to the Declaration of Helsinki on biomedical research involving human subjects (Edinburgh amendment). The proposal of the study was approved by the Local Ethics Committee of the University of Erlangen–Nuremberg.
Subjects were instructed not to take analgesics when the experiments took place. The study was conducted in a cross-over design by dividing the subjects into 3 groups, each consisting of 10 test persons (50% male and 50% female). Randomization was achieved by stratified random allocation according to sex using Excel (Microsoft, Redmond), and each group started with a different treatment condition. Afterwards, the 2 remaining treatment conditions were applied, each with an interval of 4 weeks.
The study was performed in the Department of Neurology, General Hospital Fürth, Germany, in summer 2016.
2.2. Experimental design
The experimental design of the study is illustrated in Figure 1. At the beginning of every experiment, pain scoring was assessed qualitatively and quantitatively on a 100-point NRS, ranging from 0 = no pain to 100 = maximum of tolerable pain. Pain scoring was performed before and after quantitative sensory testing (QST) and every 10 minutes during treatment. At the same time points, skin temperature of the test and control volar forearm was recorded using a thermal camera to assess the temperature profile during the experiment. Pain was induced on the test arm using HD-TES until NRS = 50 was reached. Treatment with BL, RL, or TC was performed for 1 hour. Before electrical stimulation, QST was performed by assessing the mechanical detection threshold (MDT) and mechanical pain threshold (MPT). These parameters were further determined before and after treatment together with measurement of the area of flare, mechanical hyperalgesia, and allodynia.
Figure 1.
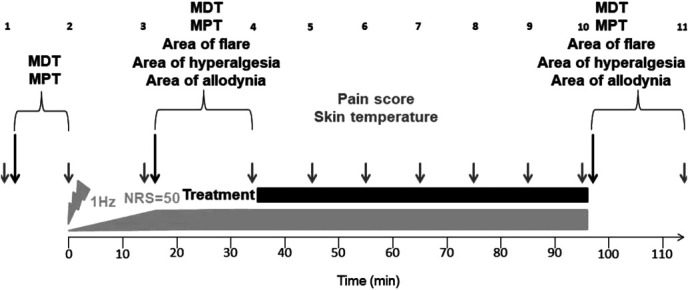
Experimental protocol. Pain was induced on the volar forearm through transcutaneous electrical stimulation (gray bar) using an impulse generator with a frequency of 1 Hz. The current was gradually increased during the first 15 minutes until NRS = 50, and kept constantly until the end of stimulation. Pain status (gray arrows) was assessed qualitatively and quantitatively before and after QST as well as every 10 minutes during treatment. At the same time, skin temperature (gray arrows) of the test and control volar forearm was recorded using a thermal camera. For QST (black arrows), MDT and MPT were assessed before electrical stimulation as well as before and after light treatment (black bar) together with areas of flare, hyperalgesia, and allodynia. MDT, mechanical detection threshold; MPT, mechanical pain threshold; NRS, numeric rating scale; QST, quantitative sensory testing.
2.3. Electrical induction of pain
For HD-TES, 2 self-adhesive electrodes (2 mm × 5 mm) were placed on the skin of the dominant hand volar forearm with a distance of 4 mm between them. Monophasic, rectangular electrical pulses with a frequency of 1 Hz and a voltage of 400 mV were applied using a pulse generator (Digitimer S7; Hertfordshire, UK). The current was gradually increased during the first 15 minutes until NRS = 50 with a predefined maximum of 40 mA and then kept constant until the end of stimulation. To ensure identical baseline conditions before the application of distinct treatments, current profiles were assessed during the adjustment period of electrical stimulation.
2.4. Quantification and qualification of induced pain
For quantification of induced pain, subjects were asked to rate their pain using the NRS, ranging from 0 = no pain to 100 = maximum tolerable pain. To measure pain perception in either direction, HD-TES intensity was adjusted to NRS = 50. To account for individually varying pain adaptation, HD-TES intensity was readjusted after 15 minutes of stimulation to NRS = 50 if it had deviated from NRS = 50. Subsequently, subjects were asked in regular intervals of 10 minutes to rate pain perception on a NRS 0 to 100.
For qualification of induced pain, subjects were asked to describe the quality of pain according to the German counterpart of the McGill Pain Questionnaire.13,34
2.5. Quantitative sensory testing
To determine MDT,41 a standardized set of von Frey hairs (Optihair set; Marstock Nervtest, Heidelberg, Germany) was used, exerting force between 0.25 mN and 256 mN graded by a factor of 2 on a flat contact area of <1 mm2 with a contact time of 1 second on the skin around the electrodes. Test persons were asked whether they felt the force or not.
To determine MPT,41 a standardized set of pinprick punctate probes with 7 custom-made (in-house built)-weighted stimulus intensities between 8 mN and 512 mN graded by a factor of 2 was used. Pinprick punctuate probes were placed on a flat contact area of 0.2 mm diameter with a contact time of 1 second on the skin around the electrodes. Test persons were asked whether they perceived the stimulus as sharp or not. Applying a “modified method of limits,” the geometric mean of MDT and MPT was calculated from 5 lines of ascending and descending stimulus intensities.
To determine the areas of flare, mechanical hyperalgesia, and allodynia,36 8 linear rows separated by angles of 45°, running from the center around the electrodes to the periphery and consisting of points with each 1-cm distance were drawn using a template.
The border of the red flare was determined by counting the points' distances from the center for each row.
Hyperalgesia was measured by using a 256-mN pinprick punctate probe on a flat contact area of 0.2 mm diameter with a contact time of 1 second on the skin, going from point to point from the periphery to the center for each row.
Allodynia was measured using a cotton wool that stroked the skin for a length of 1 cm and with a force of 3 mN, extending from the periphery to the center of each row.
Areas of flare, hyperalgesia, and allodynia were calculated by summing up the calculated areas of all triangles in the template, which delineated the borders of the measured flare, hyperalgesia, and allodynia, respectively.
2.6. Light treatment
Treatment was performed with custom-made (in-house built) opaque collars, emitting either 450 nm BL or RL of 630 nm wavelength. The irradiation unit of the collar consisted of 150 surface mount device LEDs, reaching an optical output power of 0.8 Watt. As TC, an opaque collar was designed producing heat only. The opaque collars were placed around the electrically stimulated forearm before switching them on so that the test person could not see the illumination. For temperature measurements, the light was switched off to ensure subjects' blindness. Light treatment was applied with an initial intensity of 50%. When skin temperature rose above 40°C, the intensity was decreased to 25% to avoid blisters and then reincreased when skin temperature fell again below the 40°C threshold.
2.7. Measurement of skin temperature
Skin temperature was measured on the test and control volar forearm using a thermal camera (FLIR T640; Frankfurt on the Main, Germany).
2.8. Data analysis
Data analysis was performed using Excel (Microsoft), GraphPad Prism 5 (La Jolla), and MATLAB (MathWorks, Natick). Groups were pooled and analyzed in a blinded way. Data are represented as mean with SD or median with interquartile range (25th and 75th percentiles) with extreme data points (boxplot whiskers) and outliers (“+” symbols). Since data did not correspond to a Gaussian distribution, comparisons were evaluated statistically either using nonparametric 1-way analysis of variance for repeated measures (Friedman test) with the Dunn multiple comparison posttest or aligned rank transform analysis of variance for nonparametric factorial analysis with repeated measures. Significance was assumed for P < 0.05.
3. Results
3.1. Current and temperature profiles
For all 3 treatment groups (TC, BL, and RL), the mean current profiles were similar before treatment application (Fig. 2A), indicating the same baseline conditions.
Figure 2.
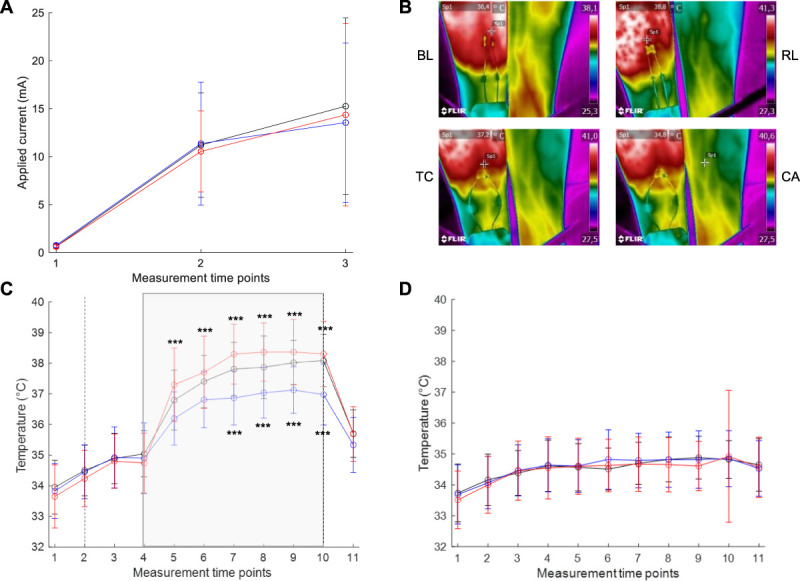
Applied current and temperature profiles. (A) Electrical currents in mA applied to subjects before treatment either with thermal control (TC; dark line), blue light (BL; blue line), or red light (RL; red line) at t = 1 the detection threshold, t = 2 at NRS = 50, and t = 3 after 15 minutes, before currents were kept constantly and treatment was started. Means are given ±SD (n = 30). (B) Representative photographs of the test person's volar right forearm under treatment with TC, BL, and RL as well as of the unstimulated and untreated left control arm (CA) detected by a thermal camera. (C) The mean temperature profiles in °C of subjects' test arm treated with TC, BL, or RL. Intervals between time points from 1 to 10 comprise 10 minutes, and the interval between the time points 10 and 11 comprises 20 minutes. t = 5 represents the time point 10 minutes after treatment, and t = 11 the time point after completion of electrical stimulation and treatment. For statistical analysis, data were aligned rank transformed, and 2-way ANOVA with the Bonferroni posttest was calculated. ***P < 0.001. Means are given ±SD (n = 30). (D) The mean temperature profiles in °C of subjects' control arm. Analysis was the same as for (C). ANOVA, analysis of variance.
Temperature profiles revealed that electrical stimulation alone did not generate a warming effect in contrast to all treatments, which increased temperature by about 2 to 4°C compared to the unstimulated and untreated control arm (Fig. 2B–D). Interestingly, this effect was stronger for RL than for TC and weakest for BL throughout the treatment period with no differences among the 3 groups after treatment termination. The order of treatments across subjects did not have any impact on temperature profiles (Supplemental Table 1, available at http://links.lww.com/PR9/A136).
3.2. Impact of light treatment on pain sensation
From all treatments, only BL reduced NRS pain scores significantly (Fig. 3). This effect was visible as early as 10 minutes after initiation of exposure and continued to increase over the course of treatment, leading to a reduction in NRS pain scores by about half after 60 minutes. Twenty minutes after termination of electrical stimulation and treatment, pain scores returned close to 0 independent of treatment. However, there were 10% nonresponders with no significant decrease in NRS pain scores after BL treatment included in the analysis. NRS pain scores remained negligible in the unstimulated, untreated control arm during the entire course of experiment (Supplemental Figure 1, available at http://links.lww.com/PR9/A136). Moreover, the order of light treatment did not have any significant impact on NRS pain scores reported for the test arm (Supplemental Table 2, available at http://links.lww.com/PR9/A136).
Figure 3.
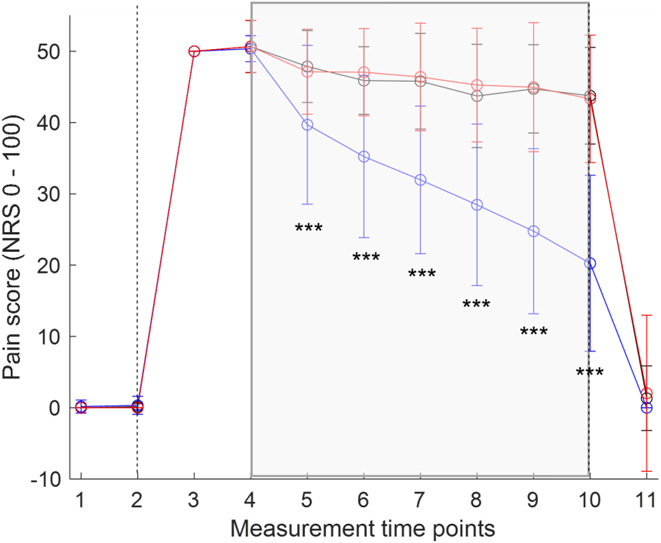
Impact of treatment on pain sensation in the test arm. NRS pain scoring under treatment with TC (black line), BL (blue line), and RL (red line). Intervals between time points from 1 to 10 comprise 10 minutes, and the interval between the time points 10 and 11 comprises 20 minutes. Start (t = 2) and termination (t = 10) of electrical stimulation are indicated by vertical dashed lines. Treatment periods are indicated by a colored gray box. For statistical analysis, data were aligned rank transformed, and 2-way ANOVA with the Bonferroni posttest was calculated. ***P < 0.001. Means are given ±SD (n = 30). ANOVA, analysis of variance; NRS, numeric rating scale.
Qualitative pain sensation showed marked individual variation. However, during distinct treatments, qualitative pain sensation differed depending on the condition applied (Table 2; Supplemental Figure 2, available at http://links.lww.com/PR9/A136). Of note, during BL treatment, participants sensed pain as less hot, tingling, stabbing, and throbbing than during RL and TC treatment.
Table 2.
Statistical comparison of test arm pain quality dependent on treatment.
| Pain quality | TC vs BL Difference |
TC vs RL Difference |
BL vs RL Difference |
|---|---|---|---|
| Itchy | 0.8333* | 1.167* | 0.333* |
| Pressing | −0.6667* | 0.000* | 0.6667* |
| Dull | −2.500* | 3.667† | 6.167§ |
| Burning | −4.167‡ | −1.167* | 3.000* |
| Tingling | −4.833§ | −0.8333* | 4.000‡ |
| Beating | 1.000* | 1.500* | 0.500* |
| Hot | −11.83§ | 8.500§ | 20.33§ |
| Pulling | −8.667§ | −8.333§ | 0.333* |
| Stabbing | −11.00§ | −3.500† | 7.500§ |
| Throbbing | −9.833§ | −6.000§ | 3.833† |
Statistical analysis of pain quality under treatment with TC, BL, and RL. Two-way ANOVA was calculated with the Bonferroni posttest.
P > 0.05.
P < 0.05.
P < 0.01.
P < 0.001.
BL, blue light; RL, red light; TC, thermal control.
3.3. Impact of light treatment on quantitative sensory testing parameters
Independent of treatment group, HD-TES increased MDT and MPT to the same extent in the test arm (Supplemental Figure 3A and B, available at http://links.lww.com/PR9/A136), but not in the control arm (Supplemental Figure 3C and D, available at http://links.lww.com/PR9/A136). This result indicates that HD-TES led to hypesthesia and reduced sensitivity for sharp stimulus discrimination.
Induced hypesthesia decreased under BL and TC treatment, whereas RL did not lead to a significant reduction (Fig. 4A). However, hypesthesia reduction was significantly stronger on BL exposure.
Figure 4.

Impact of treatment on QST parameters in the test arm. (A) Logarithmic MDT in mN (n = 30) before (pretreat) and after (posttreat) treatment with TC (black boxes), BL (blue boxes), and RL (red boxes). All data are represented as median (red line) with interquartile range (box edges represent 25th and 75th percentiles) with extreme data points (boxplot whiskers) and outliers (“+” symbols). Nonparametric 1-way ANOVA for repeated measures (Friedman test) was calculated with the Dunn posttest. nsP > 0.05, **P < 0.01, and ***P < 0.001. (B) Logarithmic MPT in mN (n = 30) before (pretreat) and after (posttreat) treatment with TC, BL, and RL, normalized to the time point before electrical stimulation. One-way ANOVA (Friedman test) with the Dunn posttest. nsP > 0.05, ***P < 0.001. (C) Area of flare in cm2 (n = 30) before (pretreat) and after (posttreat) treatment with TC, BL, and RL. Nonparametric 1-way ANOVA for repeated measures (Friedman test) was calculated with the Dunn posttest. nsP > 0.05, ***P < 0.001. (D) Area of hyperalgesia in cm2 (n = 30) before (pretreat) and after (posttreat) treatment with TC, BL, and RL. Nonparametric 1-way ANOVA for repeated measures (Friedman test) was calculated with the Dunn posttest. nsP > 0.05, **P < 0.01, ***P < 0.001. (E) Area of allodynia in cm2 (n = 30) before (pretreat) and after (posttreat) treatment with TC, BL, and RL. Nonparametric 1-way ANOVA for repeated measures (Friedman test) was calculated with the Dunn posttest. nsP > 0.05, **P < 0.01. ANOVA, analysis of variance; MDT, mechanical detection threshold; MPT, mechanical pain threshold; QST, quantitative sensory testing.
Similar to MDT, MPT decreased under BL treatment and less stronger under TC treatment, whereas RL treatment failed to reduce MPT (Fig. 4B).
For all 3 groups, a red flare was induced by HD-TES. Interestingly, although the area of flare further increased under TC and RL treatment, it decreased under BL treatment (Fig. 4C).
Similarly, the area of mechanical hyperalgesia induced by HD-TES only diminished under blue light treatment (Fig. 4D). This effect was highly significant, although hyperalgesia could not be induced in all subjects.
Similarly, allodynia was observed only in 11 individuals. However, allodynia was significantly reduced only under BL treatment (Fig. 4E).
On the control arm, neither HD-TES nor light treatment affected QST parameters (Supplemental Figure 4, available at http://links.lww.com/PR9/A136). Except for the area of flare between BL and RL treatment, there was no significant difference observed for QST parameters based on the order of applied treatments among subjects, indicating marginal stratification of the data (Supplemental Table 3, available at http://links.lww.com/PR9/A136).
4. Discussion
In this study, we found that BL treatment substantially reduced various parameters of spontaneous and evoked pain in a human experimental pain model in contrast to RL and TC.
4.1. Potential mechanisms of blue-light treatment
Short-wavelength BL has been shown to specifically activate TRPA1 cation channels in zebrafish through transient binding of the light-sensitive ligand optovin.26 Low-intensity light of the same wavelength induces painful sensation, when applied to the skin of healthy volunteers.5 Furthermore, BL up to 460 nm wavelength is sufficient to activate human TRPA1 and already sensitized TRPV1 channels in transfected HEK 293 T cells.4,5 On activation, TRPA1 and TRPV1 channels located at unmyelinated C and small myelinated Aδ fibers induce the release of proinflammatory cytokines.35,38 The neuropeptides substance P and calcitonin gene–related peptide lead to protein extravasation and vasodilatation, which are the key mechanisms in neurogenic inflammation and nociceptor sensitization.5,23 Accordingly, a crucial role of TRPA1 and TRPV1 in neurogenic inflammation and chronic pain has been suggested.3,5,24,50 Interestingly, reactive oxygen species, which also activate TRPA1, lead to photosensitization and augment pain response to BL treatment.5
Brief stimulation with BL has been demonstrated to be nociceptive; however, we have observed an antinociceptive effect for extended periods of illumination in a human surrogate model of chronic pain. On the one hand, this finding might be explained by the excitation status of nociceptive fibers. Owing to electrical stimulation, nociceptive fibers are constantly depolarized, resembling conditions of chronic pain. Additional activation of already sensitized TRPA1 and TRPV1 cation channels by BL illumination may result in the efflux instead of influx of cations, leading to hyperpolarization of excited nociceptive fibers. Alternatively, extended BL illumination may lead to a desensitization of nociceptive fibers as shown for various TRP agonists.1,2,25,43 Finally, BL has been shown to activate antioxidative capacities of human skin fibroblasts, which may mediate further antinociceptive effects.29,39 However, the optimal extent and time scale required for BL to affect nociception, especially in patients with chronic pain, requires further investigation.
4.2. Rescue of hypesthesia and stimulus discrimination under blue-light treatment
In addition to pain induction, HD-TES caused hypesthesia and decreased the potential to discriminate sharp stimuli, thus mimicking sensory loss observed in patients with chronic pain.49 Blue-light treatment significantly improved hypesthesia and sharp stimulus discrimination in contrast to RL treatment. Interestingly, TC resulted in modest improvement, indicating that the warming effect alone may already be beneficial.
4.3. Potential limitations of the study
Although we obtained promising results with BL treatment in our human experimental pain model, some potential limitations need to be considered. First, although the participants were blinded to the treatment applied during each session, they were not explicitly asked to guess to avoid generating expectations in participants. Therefore, we cannot evaluate whether participants attempted to surmise which treatment was being applied during the individual sessions. Unlike participants, the examinator was not blinded for the light treatment.
Moreover, although we expected skin temperature to rise on the test arm under light treatment, there were significant differences between RL and BL. This phenomenon may be due to variable penetration depths and thus different quantities of excited molecules within the tissue. Of note, BL with the lowest penetration depth increased temperature much less than RL with the greatest penetration depth.
Although the area of flare decreased under BL exposure, it intensified under RL and TC treatment. On the one hand, stronger heating by RL and TC may have led to the increased flare. On the other hand, increased flare may be due to neurogenic inflammation induced by HD-TES and not suppressed by TC or RL treatment. Interestingly, although skin temperature rose significantly under BL exposure, the area of flare decreased. This finding suggests that BL attenuates neurogenic inflammation independent of skin temperature.
Finally, although LED-based BL phototherapy effectively reduced spontaneous and evoked pain, 10% of test subjects did not respond to BL treatment. This phenomenon needs to be considered for potential further testing in patients with chronic pain, who represent a much more heterogenous population.
4.4. Clinical relevance of the study
The use of LED-based phototherapy for treating acute nociceptive and chronic pain disorders has increased significantly over the past years because of its low costs, ease of application, and lack of side effects. In particular, red and infrared LEDs have proven to be valuable tools in managing acute and chronic pain in conditions such as knee osteoarthritis,12 back pain,30,31 temporomandibular joint disorder,27,45 orthodontic tooth separation,16 and childbirth.46,47 Moreover, green-light treatment has revealed promising results in treating chronic and episodic migraine.33 However, to date, BL has not been applied for pain treatment in clinical settings.
In our preclinical study, we show that extended exposure to BL leads to significant analgetic, antihyperalgesic, and antiallodynic effects without any evident side effects. These results pave the way to test LED-based BL phototherapy in clinical settings. This novel treatment approach may extend the spectrum of available therapies for acute and chronic pain disorders. Future studies should attempt to elucidate any potential differences in the effects of BL treatment on acute vs chronic pain states as well as the origin of nociceptive, nociplastic, and neuropathic pain.
5. Conclusion
In this study, BL treatment significantly reduced pain intensity and quality in a human experimental pain model. Furthermore, BL showed significant antihyperalgesic, antiallodynic, and antihypesthesic effects. Therefore, BL phototherapy may be a novel approach to treat pain in multiple conditions.
Disclosures
A. M. Reuss, D. Groos, M. Schröter, and R. Scholl declare no competing financial or nonfinancial conflict of interest. In the past 3 years, C. Maihöfner has worked as a consultant and speaker for the following companies: Allergan, Bionorica, Biotest, Grünenthal, GSK, Lilly, Novartis, and Daiichi Sankyo. The present work was performed in fulfillment of the requirements for obtaining the degree “Dr. med.” by Anna Maria Reuss.
Appendix A. Supplemental digital content
Supplemental digital content associated with this article can be found online at http://links.lww.com/PR9/A136.
Supplementary Material
Acknowledgements
The authors thank Conny Hofmann for technical support and Elisabeth Jane Rushing for proofreading the manuscript. The authors are indebted to the subjects who participated in this study for their consent and cooperation. This study was supported by the German Research Network “Non-Visual Effects of Light/NiviL” (German Federal Ministry of Education and Research; BMBF; grant number 13 N 13492).
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal's Web site (www.painrpts.com).
References
- [1].Akopian AN, Ruparel NB, Jeske NA, Hargreaves KM. Transient receptor potential TRPA1 channel desensitization in sensory neurons is agonist dependent and regulated by TRPV1-directed internalization. J Physiol 2007;583:175–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Akopian AN, Ruparel NB, Patwardhan A, Hargreaves KM. Cannabinoids desensitize capsaicin and mustard oil responses in sensory neurons via TRPA1 activation. J Neurosci 2008;28:1064–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Aleixandre-Carrera F, Engelmayer N, Ares-Suarez D, Acosta MDC, Belmonte C, Gallar J, Meseguer V, Binshtok AM. Optical assessment of nociceptive TRP channel function at the peripheral nerve terminal. Int J Mol Sci 2021;22:481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Babes A, Ciotu CI, Hoffmann T, Kichko TI, Selescu T, Neacsu C, Sauer SK, Reeh PW, Fischer MJM. Photosensitization of TRPA1 and TRPV1 by 7-dehydrocholesterol: implications for the Smith-Lemli-Opitz syndrome. PAIN 2017;158:2475–86. [DOI] [PubMed] [Google Scholar]
- [5].Babes A, Sauer SK, Moparthi L, Kichko TI, Neacsu C, Namer B, Filipovic M, Zygmunt PM, Reeh PW, Fischer MJ. Photosensitization in porphyrias and photodynamic therapy involves TRPA1 and TRPV1. J Neurosci 2016;36:5264–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Basler HD. The Marburg questionnaire on habitual health findings--a study on patients with chronic pain. Schmerz 1999;13:385–91. [DOI] [PubMed] [Google Scholar]
- [7].Benyamin R, Trescot AM, Datta S, Buenaventura R, Adlaka R, Sehgal N, Glaser SE, Vallejo R. Opioid complications and side effects. Pain Physician 2008;11(suppl 2):S105–20. [PubMed] [Google Scholar]
- [8].Chiodo LA, Bannon MJ, Grace AA, Roth RH, Bunney BS. Evidence for the absence of impulse-regulating somatodendritic and synthesis-modulating nerve terminal autoreceptors on subpopulations of mesocortical dopamine neurons. Neuroscience 1984;12:1–16. [DOI] [PubMed] [Google Scholar]
- [9].Chow RT, Johnson MI, Lopes-Martins RA, Bjordal JM. Efficacy of low-level laser therapy in the management of neck pain: a systematic review and meta-analysis of randomised placebo or active-treatment controlled trials. Lancet 2009;374:1897–908. [DOI] [PubMed] [Google Scholar]
- [10].Cidral-Filho FJ, Martins DF, More AO, Mazzardo-Martins L, Silva MD, Cargnin-Ferreira E, Santos AR. Light-emitting diode therapy induces analgesia and decreases spinal cord and sciatic nerve tumour necrosis factor-alpha levels after sciatic nerve crush in mice. Eur J Pain 2013;17:1193–204. [DOI] [PubMed] [Google Scholar]
- [11].de Andrade AL, Bossini PS, Parizotto NA. Use of low level laser therapy to control neuropathic pain: a systematic review. J Photochem Photobiol B 2016;164:36–42. [DOI] [PubMed] [Google Scholar]
- [12].de Paula Gomes CAF, Leal-Junior ECP, Dibai-Filho AV, de Oliveira AR, Bley AS, Biasotto-Gonzalez DA, de Tarso Camillo de Carvalho P. Incorporation of photobiomodulation therapy into a therapeutic exercise program for knee osteoarthritis: a placebo-controlled, randomized, clinical trial. Lasers Surg Med 2018;50:819–28. [DOI] [PubMed] [Google Scholar]
- [13].Deutsche Schmerzgesellschaft e.V. Deutscher Schmerz-Fragebogen. Version 20152, 2015. [Google Scholar]
- [14].Enwemeka CS, Parker JC, Dowdy DS, Harkness EE, Sanford LE, Woodruff LD. The efficacy of low-power lasers in tissue repair and pain control: a meta-analysis study. Photomed Laser Surg 2004;22:323–9. [DOI] [PubMed] [Google Scholar]
- [15].Fajardo O, Friedrich RW. Optopharmacology: a light switch for pain. Nat Chem Biol 2013;9:219–20. [DOI] [PubMed] [Google Scholar]
- [16].Figueira IZ, Sousa APC, Machado AW, Habib FAL, Soares LGP, Pinheiro ALB. Clinical study on the efficacy of LED phototherapy for pain control in an orthodontic procedure. Lasers Med Sci 2019;34:479–85. [DOI] [PubMed] [Google Scholar]
- [17].Filitz J, Ihmsen H, Günther W, Tröster A, Schwilden H, Schüttler J, Koppert W. Supra-additive effects of tramadol and acetaminophen in a human pain model. PAIN 2008;136:262–70. [DOI] [PubMed] [Google Scholar]
- [18].Furlan AD, Lui PW, Mailis A. Chemical sympathectomy for neuropathic pain: does it work? Case report and systematic literature review. Clin J Pain 2001;17:327–36. [DOI] [PubMed] [Google Scholar]
- [19].Glazov G, Yelland M, Emery J. Low-level laser therapy for chronic non-specific low back pain: a meta-analysis of randomised controlled trials. Acupunct Med 2016;34:328–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Gupta A, Mehdi A, Duwell M, Sinha A. Evidence-based review of the pharmacoeconomics related to the management of chronic nonmalignant pain. J Pain Palliat Care Pharmacother 2010;24:152–6. [DOI] [PubMed] [Google Scholar]
- [21].Hosokawa T, Kawabata Y. Pain treatment with low reactive level laser therapy (LLLT). Masui 2012;61:718–27. [PubMed] [Google Scholar]
- [22].Ibrahim MM, Patwardhan A, Gilbraith KB, Moutal A, Yang X, Chew LA, Largent-Milnes T, Malan TP, Vanderah TW, Porreca F, Khanna R. Long-lasting antinociceptive effects of green light in acute and chronic pain in rats. PAIN 2017;158:347–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Julius D, Basbaum AI. Molecular mechanisms of nociception. Nature 2001;413:203–10. [DOI] [PubMed] [Google Scholar]
- [24].Karashima Y, Damann N, Prenen J, Talavera K, Segal A, Voets T, Nilius B. Bimodal action of menthol on the transient receptor potential channel TRPA1. J Neurosci 2007;27:9874–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Kistner K, Siklosi N, Babes A, Khalil M, Selescu T, Zimmermann K, Wirtz S, Becker C, Neurath MF, Reeh PW, Engel MA. Systemic desensitization through TRPA1 channels by capsazepine and mustard oil—a novel strategy against inflammation and pain. Sci Rep 2016;6:28621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Kokel D, Cheung CY, Mills R, Coutinho-Budd J, Huang L, Setola V, Sprague J, Jin S, Jin YN, Huang XP, Bruni G, Woolf CJ, Roth BL, Hamblin MR, Zylka MJ, Milan DJ, Peterson RT. Photochemical activation of TRPA1 channels in neurons and animals. Nat Chem Biol 2013;9:257–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Kopacz Ł, Ciosek Ż, Gronwald H, Skomro P, Ardan R, Lietz-Kijak D. Comparative analysis of the influence of selected physical factors on the level of pain in the course of temporomandibular joint disorders. Pain Res Manag 2020;2020:1036306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Koppert W, Dern SK, Sittl R, Albrecht S, Schüttler J, Schmelz M. A new model of electrically evoked pain and hyperalgesia in human skin: the effects of intravenous alfentanil, S(+)-ketamine, and lidocaine. Anesthesiology 2001;95:395–402. [DOI] [PubMed] [Google Scholar]
- [29].Krassovka JM, Suschek CV, Prost M, Grotheer V, Schiefer JL, Demir E, Fuchs PC, Windolf J, Sturmer EK, Oplander C. The impact of non-toxic blue light (453 nm) on cellular antioxidative capacity, TGF-beta1 signaling, and myofibrogenesis of human skin fibroblasts. J Photochem Photobiol B 2020;209:111952. [DOI] [PubMed] [Google Scholar]
- [30].Leichtfried V, Matteucci Gothe R, Kantner-Rumplmair W, Mair-Raggautz M, Bartenbach C, Guggenbichler H, Gehmacher D, Jonas L, Aigner M, Winkler D, Schobersberger W. Short-term effects of bright light therapy in adults with chronic nonspecific back pain: a randomized controlled trial. Pain Med 2014;15:2003–12. [DOI] [PubMed] [Google Scholar]
- [31].Lin YP, Su YH, Chin SF, Chou YC, Chia WT. Light-emitting diode photobiomodulation therapy for non-specific low back pain in working nurses: a single-center, double-blind, prospective, randomized controlled trial. Medicine (Baltimore) 2020;99:e21611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Martin L, Porreca F, Mata EI, Salloum M, Goel V, Gunnala P, Killgore WDS, Jain S, Jones-MacFarland FN, Khanna R, Patwardhan A, Ibrahim MM. Green light exposure improves pain and quality of life in fibromyalgia patients: a preliminary one-way crossover clinical trial. Pain Med 2021;22:118–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Martin LF, Patwardhan AM, Jain SV, Salloum MM, Freeman J, Khanna R, Gannala P, Goel V, Jones-MacFarland FN, Killgore WD, Porreca F, Ibrahim MM. Evaluation of green light exposure on headache frequency and quality of life in migraine patients: a preliminary one-way cross-over clinical trial. Cephalalgia 2021;41:135–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Melzack R. The McGill Pain Questionnaire: major properties and scoring methods. PAIN 1975;1:277–99. [DOI] [PubMed] [Google Scholar]
- [35].Moran MM, Szallasi A. Targeting nociceptive transient receptor potential channels to treat chronic pain: current state of the field. Br J Pharmacol 2018;175:2185–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Nickel FT, DeCol R, Jud S, Fasching PA, Seifert F, Maihöfner C. Inhibition of hyperalgesia by conditioning electrical stimulation in a human pain model. PAIN 2011;152:1298–303. [DOI] [PubMed] [Google Scholar]
- [37].Nilges P, Essau C. Depression, anxiety and stress scales: DASS—A screening procedure not only for pain patients. Schmerz 2015;29:649–57. [DOI] [PubMed] [Google Scholar]
- [38].Nilius B, Appendino G, Owsianik G. The transient receptor potential channel TRPA1: from gene to pathophysiology. Pflugers Arch 2012;464:425–58. [DOI] [PubMed] [Google Scholar]
- [39].Opländer C, Deck A, Volkmar CM, Kirsch M, Liebmann J, Born M, van Abeelen F, van Faassen EE, Kröncke KD, Windolf J, Suschek CV. Mechanism and biological relevance of blue-light (420-453 nm)-induced nonenzymatic nitric oxide generation from photolabile nitric oxide derivates in human skin in vitro and in vivo. Free Radic Biol Med 2013;65:1363–77. [DOI] [PubMed] [Google Scholar]
- [40].Pigatto GR, Silva CS, Parizotto NA. Photobiomodulation therapy reduces acute pain and inflammation in mice. J Photochem Photobiol B 2019;196:111513. [DOI] [PubMed] [Google Scholar]
- [41].Rolke R, Magerl W, Campbell KA, Schalber C, Caspari S, Birklein F, Treede RD. Quantitative sensory testing: a comprehensive protocol for clinical trials. Eur J Pain 2006;10:77–88. [DOI] [PubMed] [Google Scholar]
- [42].Rooney L, Vidal A, D'Souza AM, Devereux N, Masick B, Boissel V, West R, Head V, Stringer R, Lao J, Petrus MJ, Patapoutian A, Nash M, Stoakley N, Panesar M, Verkuyl JM, Schumacher AM, Petrassi HM, Tully DC. Discovery, optimization, and biological evaluation of 5-(2-(trifluoromethyl)phenyl)indazoles as a novel class of transient receptor potential A1 (TRPA1) antagonists. J Med Chem 2014;57:5129–40. [DOI] [PubMed] [Google Scholar]
- [43].Ruparel NB, Patwardhan AM, Akopian AN, Hargreaves KM. Desensitization of transient receptor potential ankyrin 1 (TRPA1) by the TRP vanilloid 1-selective cannabinoid arachidonoyl-2 chloroethanolamine. Mol Pharmacol 2011;80:117–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [44].Schmidt PC, Ruchelli G, Mackey SC, Carroll IR. Perioperative gabapentinoids: choice of agent, dose, timing, and effects on chronic postsurgical pain. Anesthesiology 2013;119:1215–21. [DOI] [PubMed] [Google Scholar]
- [45].Sousa DFM, Gonçalves MLL, Politti F, Lovisetto RDP, Fernandes KPS, Bussadori SK, Mesquita-Ferrari RA. Photobiomodulation with simultaneous use of red and infrared light emitting diodes in the treatment of temporomandibular disorder: study protocol for a randomized, controlled and double-blind clinical trial. Medicine (Baltimore) 2019;98:e14391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Traverzim MADS, Makabe S, Silva DFT, Pavani C, Bussadori SK, Fernandes KSP, Motta LJ. Effect of led photobiomodulation on analgesia during labor: study protocol for a randomized clinical trial. Medicine (Baltimore) 2018;97:e11120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Traverzim MA, Sobral APT, Fernandes KPS, de Fátima Teixeira Silva D, Pavani C, Mesquita-Ferrari RA, Horliana ACRT, Gomes AO, Bussadori SK, Motta LJ. The effect of photobiomodulation on analgesia during childbirth: a controlled and randomized clinical trial. Photobiomodul Photomed Laser Surg 2021;39:265–71. [DOI] [PubMed] [Google Scholar]
- [48].van Hecke O, Austin SK, Khan RA, Smith BH, Torrance N. Neuropathic pain in the general population: a systematic review of epidemiological studies. PAIN 2014;155:654–62. [DOI] [PubMed] [Google Scholar]
- [49].von Hehn CA, Baron R, Woolf CJ. Deconstructing the neuropathic pain phenotype to reveal neural mechanisms. Neuron 2012;73:638–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [50].Wang YY, Chang RB, Waters HN, McKemy DD, Liman ER. The nociceptor ion channel TRPA1 is potentiated and inactivated by permeating calcium ions. J Biol Chem 2008;283:32691–703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [51].Wright ME, Rizzolo D. An update on the pharmacologic management and treatment of neuropathic pain. JAAPA 2017;30:13–17. [DOI] [PubMed] [Google Scholar]
- [52].Yan YY, Li CY, Zhou L, Ao LY, Fang WR, Li YM. Research progress of mechanisms and drug therapy for neuropathic pain. Life Sci 2017;190:68–77. [DOI] [PubMed] [Google Scholar]
- [53].Zhang H, Shi L, Zhang Y, Wang P, Zhang G, Cao Y, Zhou Z, Wang X. Modified photodynamic therapy to minimize pain in the treatment of condylomata acuminata: a prospective, randomized, self-controlled study. Photodiagnosis Photodyn Ther 2020;32:101915. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental digital content associated with this article can be found online at http://links.lww.com/PR9/A136.