

Abstract
Objectives
The Covid‐19 pandemic changed the humanity life. Millions of deaths and infections that spread rapidly around the world made all countries take measures to stop the outbreaks and assume the enormous consequences that the Coronavirus is leaving behind. The challenge has been enormous; governments across the world have implemented a wide span of nonpharmaceutical interventions to mitigate the Coronavirus pandemic (SARS‐CoV‐2) and its consequences in economic terms. The aim of this article is to analyze the effects that different kinds of measures taken by Latin American governments had on the daily new infections. The countries analyzed were Argentina, Bolivia, Chile, Colombia, Costa Rica, El Salvador, Guatemala, Honduras, México, Panamá, Peru, Paraguay, Dominican Republic, Uruguay and Venezuela.
Methods
A time series cross‐section analysis was performed, which allows studying the evolution of the number of daily cases over time and by country. The timeframe of this study was from the day the first case of coronavirus was registered in a country, until September 14, 2020. We used data from Covid‐19 Dashboard database of Johns Hopkins University and the Oxford Covid‐19 Government Response Tracker data set.
Results
The Stringency Index did not have a significant influence at the beginning of the pandemic but turned out to be significant and inversely related to DNI during Phases 2 and 3. On the contrary, the Economic and the Sanitary Containment Index was not statistically significant for any of the phases. Furthermore, the level of wealthfare of a country, measured from its GDP per capita, exerts a substantive conditional influence on the management of the Covid‐19 crisis.
Conclusions
The scenarios have been changing and strategies had to change as well in order to be successful because they lose effectiveness and have increased social costs with time. Therefore, understanding the relative effectiveness of such measures had on the disease spreading during the first wave of the outbreak, could help governments to make more informed decisions about how to control future outbreaks of the Covid‐19 pandemic.
Keywords: comparative politics, coronavirus, Covid‐19, government responses, Latin America, nonpharmaceutical interventions, public policies
Up to September 2020, the new Coronavirus (SARS‐CoV‐2) pandemic has left more than 30 million confirmed cases and 1 million deaths. Moreover, a large part of the globe has been under quarantine (or under some type of movement restriction policies), several national health systems collapsed, and governments struggled to contain or mitigate the crisis. The challenge has been enormous, different governments adopted diverse measures (nonpharmaceutical interventions, NPIs) aimed at reducing the number of new infections and deaths while coping with dire economic consequences. The strategies varied greatly from country to country. While some countries delayed the application of measures, others reacted as soon as the first few cases were registered. Many countries maintained extended quarantines (or stay‐at‐home orders), whereas in others it was less extended in time and some never imposed any human mobility restrictions. Among the measures adopted, the menu of options was likewise extensive. Contact tracing, widespread and massive testing, information campaigns, huge investments on health‐care equipment such as respiratory assist devices, and research for vaccines and treatments have been among the sanitary containment (SC) measures. Other usual measures included human mobility restrictions, social distancing, schools closure, the obligation to wear face masks, and a ban on public events, social gatherings, meetings, etc. Economic measures were also adopted to support people during the crisis, to sustain the restrictions and to allow facing the economic paralysis that the lockdown implied.
Different measures were adopted over time, being usually stricter at the beginning of the pandemic and progressing into different degrees of relaxation after five months. Both the measures and their consequences have varied over time. The scenarios were changing and initially successful strategies had to change because they lost effectiveness or even became obsolete. Moreover, measures that were not successful in reducing infections at the beginning improved over time. In this article, we intend to classify and evaluate the different types of government responses of Latin American countries to the Covid‐19 pandemic, over time. In addition to a review of the policies implemented by 15 Latin American countries to manage daily new infections (DNIs), we intend to study the way in which policies have changed throughout the different phases or stages of the first wave of pandemic in the region. Understanding the relative effectiveness of such policies or NPIs had on Coronavirus transmission during the first wave of the outbreak could help governments to make more informed decisions about how to control the pandemic.
The countries analyzed in this study are Argentina, Bolivia, Chile, Colombia, Costa Rica, El Salvador, Guatemala, Honduras, Mexico, Panama, Peru, Paraguay, Dominican Republic, Uruguay, and Venezuela. We performed a time series cross‐section (TSCS) analysis to study the evolution of the number of daily new cases over time on a country‐by‐country basis. The studied period of time comprises from the day when the first case of the new coronavirus (SARS‐Cov‐2) was diagnosed in a country until September 14, 2020. Furthermore, a multiple linear regression (MLR) model was implemented to understand the effects that different kinds of measures taken by the governments had on the dynamics of the pandemic in each country. For this, we use the data from the Covid‐19 Dashboard database of the Center for Systems Science and Engineering (CSSE) of Johns Hopkins University, which has variables that measure new daily infections, deaths, and various dimensions of the pandemic for each country, and the Oxford Covid‐19 Government Response Tracker (OxCGRT) data set that has different indicators to evaluate the restrictive, economic, and SC measures that governments carried out in the face of the pandemic.
BACKGROUND ON CORONAVIRUS RESEARCH
Due to the contemporary nature of the Covid‐19 pandemic and of its extraordinary characteristics, we do not have previous research to use in the analysis of this global situation. However, since late 2020/early 2021, very interesting works have been published that can help us in the task of studying the effectiveness of NPIs that governments have taken to mitigate the spread of the virus.
It is possible to identify some works that focus on evaluating the effect of a particular measure. For instance, Felson and Adamczyk (2021) studied the effect of the reopening schools in the United States. Moreover, Liang, Tseng, and Ho (2020) studied the effect of the number of tests on the mortality rate through a cross‐country analysis and Hussain (2020) used the same data set analyzed in the present work and found that countries with stricter government responses experienced greater compliance regarding the “social distancing” advice and, therefore, experienced slower Covid‐19 spread rates than countries with fewer restrictions.
Furthermore, other works studied the impact of government measures in a particular country. This is the case of Sebastiani, Massa, and Riboli (2020:345) who analyzed the evolution of the Covid‐19 cumulative incidence for six Italian regions. They provided evidence that the strict measures implemented in Lombardy (Italy) and surrounding areas, and shortly thereafter extended to the whole country, have made a measurable impact in reducing the progression of the epidemic. In addition, Kim et al. (2020:4) indicated that social distancing and public behavior changes were effective at mitigating the Covid‐19 transmission in the Republic of Korea. Gupta et al. (2020:27) used event study regressions to identify the incremental change in mobility that is attributable to specific state and local government actions in United States. Informational or partial closure policies that occurred early in the epidemic have had an important influence on mobility.
Another group of works is specifically related to this article. These articles used comparative databases from several countries and with longitudinal data and evaluated the effect of different NPI used by governments to reduce the spread of the Coronavirus. For example, Brauner et al. (2021) did an interesting work by estimating the effects of NPIs on Covid‐19 transmission in 41 countries around the world during the first wave of the pandemic. They estimated the effectiveness of specific interventions with a Bayesian hierarchical model by linking intervention implementation dates to national number of cases and death counts. They arrived at conclusions that are key insights for our work: closing both schools and universities was highly effective in reducing coronavirus transmission at the advent of the pandemic; banning gatherings was effective in controlling DNI, with a large effect for limiting gatherings to 10 persons or less, a moderate‐to‐large effect for 100 persons or less, and a small‐to‐moderate effect for 1000 persons or less; targeted closures of face‐to‐face businesses with a high risk of infection, such as restaurants, bars, and nightclubs, had a small‐to‐moderate effect; closing most nonessential businesses delivering personal services was only somewhat more effective than previously mentioned measures (moderate effect). They also concluded that when these interventions were already in place, issuing a stay‐at‐home order had only a small additional effect. Thus, using effective interventions, some countries could control the epidemic while avoiding stay‐at‐home orders (Brauner et al., 2021:4–5). The work of Haug et al. (2020) also provides interesting evidence on the effectiveness of government interventions. Using a comprehensive, hierarchically coded data set of 6068 NPIs implemented in March–April 2020 in 79 territories, they analyzed the impact of government interventions on the reproduction factor Rt using harmonized results from three different data sets and four independent methods. Six NPIs obtained full consensus on their significant impact across all the methods used: the largest impacts on the reduction of the reproduction factor are shown by small gathering cancelations (83 percent, ΔRt between −0.22 and –0.35), the closure of educational institutions (73 percent, and estimates for ΔRt ranging from −0.15 to −0.21), and border restrictions (56 percent, ΔRt between −0.057 and –0.23). The consensus measures also include NPIs aiming to increase healthcare and public health capacities (increased availability of personal protective equipment: 51 percent, ΔRt −0.062 to −0.13), individual movement restrictions (42 percent, ΔRt −0.08 to −0.13) and national lockdown (including stay‐at‐home order in US states) (25 percent, ΔRt −0.008 to −0.14). Among the least effective interventions they found are government actions to provide or receive international help, measures to enhance testing capacity or improve case detection strategy (which can be expected to lead to a short‐term rise in cases), tracing and tracking measures as well as land border and airport health checks and environmental cleaning (Haug, 2020:1304). Haug (2020:1309) concluded that a suitable combination (sequence and time of implementation) of a smaller package of such measures can substitute for a full lockdown in terms of effectiveness, while reducing adverse impacts on the society, economy, humanitarian response system, and environment.
Another interesting work is that of Cheng et al. (2020), which produces a statistically valid index that categorizes countries in terms of their responses to the pandemic. This work is of special importance for this article since it showed how relevant is studying the timing of the policy responses during the first wave of the pandemic. Their results showed that relatively easy‐to‐implement policies, such as external border restrictions, the forming of task forces, public awareness campaigns, and efforts to increase health resources, came relatively early in the course of the pandemic, whereas NPIs more difficult to implement, such as curfews, closures of schools, restrictions of nonessential businesses, and restrictions of mass gatherings arrived later (Cheng et al., 2020:758–59). Likewise, the authors built an index that estimates the costs of implementing the measures over time. For instance, at the top of the index, they saw various business closure policies as the most difficult to implement, while school closures were the next most difficult; internal border restrictions were considered more difficult to implement than external border restrictions, while relatively straightforward policies such as public awareness campaigns, health monitoring, and opening new task forces or bureaus were near the bottom of the index. Furthermore, quarantines placing people in external facilities, such as hotels or government quarantine centers, are also estimated as being less costly than quarantine at home (stay‐at‐home orders) (Cheng et al., 2020:762).
In addition, Fang, Nie, and Penny (2020) studied the effectiveness of government interventions on the transmission dynamics of Covid‐19. Through simulations, the authors analyzed four‐phase stringent measures taken by the Chinese government. Here again, the timing of the implementation of the measures played an important role into the analysis. Evidence from the four‐phase stringent measures showed that it was foremost to ensure early detection, early isolation, and early treatment, cutting off the spread from the upstream (Fang, Nie, and Penny, 2020:654). Along the same line of analysis there is the paper by Hale et al. (2021) who, using the OxCGRT, described cross‐national patterns in the timing of containment and health policies, followed by a more detailed presentation of policy sequencing. They found that the sequence of policy adoption is largely similar across countries: most governments moved to a high level of response within a two‐week period around the middle of March, showing remarkable clustering; then economic support policies have tended to be established later than closure or containment and health policies, facial coverings aside, and during the initial two months of policy easing, while closure and containment policies were loosened, economic support and health policies were maintained at countries’ individual maximum strengths (Hale et al., 2021:532). Finally, Jayatilleke et al. (2020) also did a work based on OxCGRT and concluded that the timing with which some measures were adopted and relaxed was as important as the kind of measures being implemented.
Although some of these comparative works include Latin American countries in their analysis, there is little or no work that systematically studies the effectiveness of the NPIs of the governments of Latin American countries. The arrival of the Coronavirus to the different regions of the world had a certain delay1 that allowed the countries where Covid‐19 hit later, to make decisions based on the experience already built, it is important to do a specific assessment of government responses and their effects in Latin America.
Therefore, in this article, we focused on studying the effects of the measures adopted by the different governments of Latin America on the dynamics of DNI. Few papers have studied the impact of NPIs in a selection of Latin American countries, for example, Azerrat, Ratto, and Fantozzi (2021) concluded that the measures implemented by governments had significant impacts in the reductions of mobility and in reductions of infections. In addition, Barberia et al. (2020a) used the same variables from the OxCGRT database to measure the responses of the different states within Brazil2 and found a high heterogeneity on the social distancing measures implemented by them. Later, Barberia et al. (2020b) found that the effectiveness of social distancing in Brazilian states is greater when broader measures were taken and sustained over time including, for example, economic support. This promotes a higher level of observance by citizens (Barberia et al., 2020b:15).
DATA AND MEASUREMENT
This study used the CSSE database of the Johns Hopkins University. It contains Covid‐19 daily information for worldwide countries, useful for evaluating the impact of the different types of measures implemented by Latin American. For this study, 15 Latin American countries were selected: Argentina, Bolivia, Chile, Colombia, Costa Rica, El Salvador, Guatemala, Honduras, Mexico, Panama, Peru, Paraguay, Dominican Republic, Uruguay, and Venezuela. Brazil was excluded for two main reasons. First, the country did not implement any sort of unified response to the emergency. Instead, different policies were implemented by each Brazilian state, in some cases even contradicting National guidelines. Second, because of the difference in the scale and the leverage effect introduced in the MLR by its much larger number of DNI (detected using a principal components analysis). Ecuador and Nicaragua were also excluded because its records suffered from many data loading errors and inconsistencies. Cuba was also excluded because its records had no data for GDP per capita.
In the CSSE database, the number of DNI and deaths is reported daily, by country, as well as the accumulated amounts. The DNI from the 15 LATAM countries will be the dependent variable as it allowed evaluating the daily progression of the pandemic and the changes in the trends over time and between countries. In addition, this database was complemented with data obtained from the OxCGRT database, which has quantitative indicators that estimate the strength or the extent of different measures taken by the governments. In this sense, three indexes were used that ponder restrictive, and economic and fiscal measures. First, the restrictiveness index (Stringency index) of government NPIs includes an assessment of the closure of educational institutions and workspaces, cancelation of public events and public transportation, public information campaigns, restrictions to the internal movement of people, restrictions on international travel, and borders closure. All these variables, daily measured by country, are then integrated into an index that varies between 0 (maximum flexibility) and 100 (maximum restriction). We expect a significant and negative relation between the degree restrictiveness and the number of DNI registered in a given country, thus indicating that more stringent measures should lower the spread of the epidemic. Second, the index of economic and fiscal measures (Economic index) includes evaluations of the policies implemented to stimulate the economy and to contain the pandemic effects, such as fiscal policies, monetary intervention policies, emergency investments in the health system, and massive public vaccination campaigns. All of this is summarized in an index that varies from 0 (without economic stimulus and containment measures) to 100 (maximum economic and fiscal support of the state). For this index, it was expected a negative relation between this index and DNI, indicating the greater the package of economic support, the lower the new daily cases. Third, the SC index measures include public information campaigns; testing policy; contact tracing; emergency investment in healthcare; and investment in vaccines.3 This index ranges between 0 (without SC policies) and 100 (extensive development of sanitary measures). Given that the SC index had very high collinearity with the stringency index, a principal component analysis was carried out using the four original variables to create a new independent index. This variable will be used as a control for the other two indexes.
In addition, other variables were also incorporated as control into the model. These variables were population density and GDP per capita, which had fixed values by country and therefore, are expected to normalize the effects per country, thus correcting for socio‐demographic differences between countries.
There is a great variation of contexts and pandemic dynamics among the 15 Latin American countries considered for this study. For this reason, we decided to incorporate the variable Death regime. This variable indicates the level of severity with which the pandemic stroke each of the countries. Then, the countries were grouped according to their accumulated number of deaths within the timeframe of this study. The use of this variable in the analysis allowed to identify different regimes of evolution of the pandemic and to distinguish among different impact levels regarding the number of deaths. The measures adopted by governments also changed according to the number of deaths. Three groups were identified from the analysis: the first one considered countries that reached up to 100 accumulated deaths throughout the entire period under study, and only includes Uruguay. The second group consisted of countries that accumulated between 101 and 1000 deaths, and was composed of Bolivia, Costa Rica, Dominican Republic, El Salvador, Guatemala, Honduras, Panama, Paraguay, and Venezuela. Finally, the third group has countries with more than 1000 accumulated deceases and comprises Argentina, Chile, Colombia, Mexico, and Peru.
There are certain limitations to the present analysis. The first limitation is related to the quality of the data informed by each country. Every country uses its own set of criteria to register Covid‐19 confirmed cases, suspected cases, and deaths. In addition, many of the characteristics of the Covid‐19 disease are still largely unknown. What is now known is based on the knowledge and information that are currently being gathered. It is important to emphasize that this knowledge constantly evolves due to new findings and research breakthroughs. In addition to the dynamism imposed by this fact, the quality of the records can vary according to the stage of the epidemic that each country is experiencing. As an example, Mexico ran out of death certificates at a point and, for sure, that considerably delayed the official deaths toll. In sum, the conclusions that could be drawn from such a model should be solely considered as indicative of possible relationships.
Another limitation of this article is related to the use of aggregate indexes of government measures by country. Although the indexes may allow us to evaluate the effectiveness of a set of government measures taken together, they do not allow specifying the impact of each of the measures considered in it. In this sense, it could be useful to use single variables that identify the different degrees of implementation of each measure. Unfortunately, this analysis dealing with data from the first wave until September 2020 in the region, and there is very limited variation across and within countries in these variables of individual policies, resulting in collinear relationships thus they were excluded from this analysis of the first wave of the pandemic in Latin America. As argued Hale et al., 2021:533) “this has meant that most analyzes of government responses to date have had to focus on aggregate indexes. However, in later periods, we documented substantially more variation. This variation enables more credible quasi ‐experimental analysis of individual policies, such as school reopening, testing campaigns and income support.”
TIMING OF NPI IMPLEMENTATIONS IN LATIN AMERICA DURING THE FIRST WAVE OF THE OUTBREAK
Some studies have highlighted the importance of taking temporal sequence of NPI into account when studying the effectiveness of government measures. Cheng et al. (2020) mentioned “previous research on pandemics and epidemics suggests that a policy that is effective in one context may be ineffective in another due to a host of potentially conditioning factors.” Thus, erroneous conclusions could be reached if these effects were not analyzed separately for different periods of the first wave of the pandemic. We stated before that a successful measure to control DNI at the beginning might cease to be so as the time passes. On the contrary, a policy that initially had no significant effect on controlling DNI may become relevant over the course of the pandemic. As the previous research indicated, the sequence and timing of NPIs implementation matters (Cheng et al., 2020; Fang, Nie, and Penny, 2020; Hale et al., 2021; Jayatilleke et al., 2020).
In this sense, it is possible to identify different phases of implementation of measures during the first wave of the pandemic in Latin America, which are similar to the phases identified for other regions in the world (Hale et al., 2021). These phases or stages are, in our analysis, initial, intermediate, and late phase within the timeframe of this study that covers until mid‐September of 2020, and allowed us to use a quasi‐natural experiment to test our model, since in the first phase strong stringency and health containment measures and only few economic NPIs were quickly implemented, while in the second stage, economic measures increased and stringency NPIs began to decrease. Finally, in the last phase, restrictive measures lowered significantly and economic NPIs were maintained. In this way, we were able to evaluate the effect that the different types of NPIs had on the DNI under different scenarios (A: High values of Stringency Index, Low values of Economic Measures; B: High values of Stringency Index, High values of Economic Measures; C: Low values of Stringency Index, High values of Economic Measures). In the following lines, we will describe the different types of measures that were adopted and then lifted during the course of the first wave of Covid‐19 in the region.
Figure 1 resumes a reconstruction of the decisions that Latin American governments have implemented based on the OxCGRT database.4 The months of February and March correspond to Phase 1; the months of April to July to Phase 2; and the months of August and September to Phase 3. Each icon corresponds to an NPI implemented by each government. When integrating these responses, we obtained the Stringency index that we explained in the previous section, which in addition, has one of the indicators of the economic measures index from the same database.
FIGURE 1.
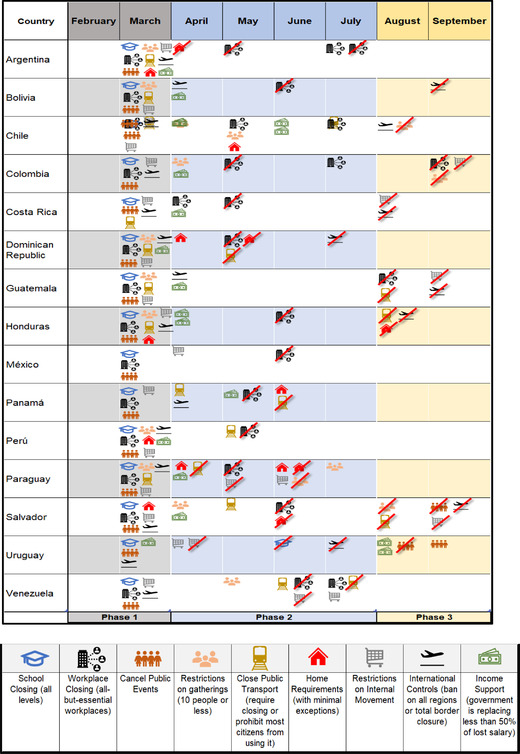
Timing of NPI implementations during the first wave of the pandemic in 15 Latin American countries. Crossed‐out icons signify when an NPI was lifted.
In Phase 1, most of the countries adopted policies to restrict internal and international mobility of its citizens. A common pattern was observed in March 2020 whereby governments implemented quick response policies when the first cases of Covid‐19 were detected. At that time, governments had little information and knowledge about the virus virulence and spreading patterns, thus most of them resolved measures aimed to reduce people mobility. These policies were mainly school and university closing (all levels), workplace closing (all‐but‐essential workplaces), canceling of public events and restrictions to gatherings (10 persons or less), stop public transport (banned for most citizens), home requirements (with minimal exceptions), restrictions on internal movement and international controls (closing of internal and international boarders). In this phase, most countries adopted at least four of seven NPIs, whereas Chile, Mexico, and Uruguay implemented less than four. On the one hand, Argentina adopted all the restriction NPIs, and on the other hand, Panama adopted only four measures. Moreover, the only countries that implemented economic aid NPIs as early as March were Argentina, Dominican Republic, Peru, and Uruguay.
In Phase 2, there are two patterns most of countries followed. On the one hand, the countries that had not adopted any economic aid measures during Phase 1, implemented them in April, with the exceptions of Panama (did it in May) and Mexico (did not adopt any economic NPI). Most of the countries complemented up to 50 percent of the salary to their population, with the exception of Chile (in June), Honduras (in April), which covered more than 50 percent of the salary. During this phase, some of the NPIs implemented in March began more flexible, for instance, between May and June, most countries allowed the return to presence in the workplaces (essentials or not), with the exception of Guatemala that did that in August. Although in the middle of the period, Argentina (in July), Colombia (in May), and Venezuela (in June) once again restricted the presentiality of nonessential workers due to the rise in DNI, whereas Dominican Republic (in May), Paraguay, and El Salvador (in June) lifted Home office requirements measures and Paraguay (May), Uruguay (April), and Venezuela (June) did the same regarding restrictions on internal movement.
In Phase 3, a large part of the countries lifted the restrictive measures. Costa Rica and Honduras (in August), Guatemala, Bolivia, and El Salvador (in September) reestablished international flights and allowed the arrival of foreigners to their countries. In addition, social gatherings of more than 10 persons were allowed in Chile and El Salvador (in August) and Colombia (in September). Likewise, Uruguay (in August) and El Salvador (in September) allowed public events, Uruguay restricted them again in September. Guatemala and Colombia (in September), and Costa Rica (August) lifted all restrictions to internal movement. Finally, Uruguay implemented, in August, economic aid measures that represented 50 percent of the salary or more.
For Phase 1, the pooled mean of the Stringency index is 74 (Figure 2a). The lower values correspond to countries such as Mexico that took very few measures. In comparison, countries that rapidly adopted more restrictive measures, such as Guatemala and El Salvador, had higher mean values for this index. During this phase, economic measures were not so common, which is reflected in relatively low values for the index for each country, with a pooled mean of 32 (Figure 2b). The SC index was relatively high, with a pooled mean of 67 (Figure 2c), indicating that a moderate response related to sanitary measures was put in place by most of the countries under study. In sum, the response was somewhat homogeneous with regard to stringency and SC and very heterogeneous if we focus on the economic support measures. Some countries reacted faster and with a greater number of measures and resources, whereas others did it later and with fewer measures. There is no single pattern because the virus was just beginning to manifest and the governments had a short time to react.
FIGURE 2.
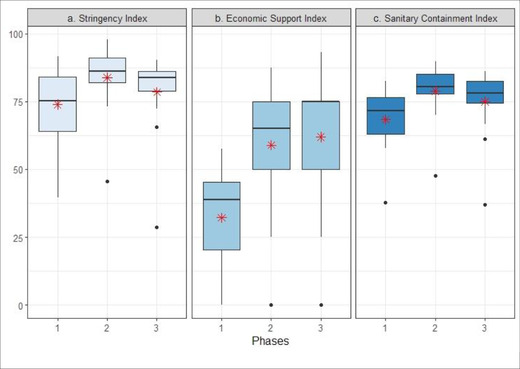
Box‐plot of the values for the three indexes analyzed for the timeframe of each stage: (a) the Stringency index, (b) the Economic Support index and (c) the Sanitary Containment index. The asterisks represent pooled mean values.
At the beginning of Phase 2, the effects of restrictive measures became visible. During this second phase, the most restrictive measures were taken and had a greater compliance from the citizenship. All the countries, except for Uruguay, had an increase in the Stringency index. The pooled mean for this Phase 2 was 84 (Figure 1a), increasing more than 10 units compared to the mean of the former phase. The lower correspond to Uruguay (46), while the highest value corresponds to Honduras (98). In addition, all countries, except Mexico, increased fiscal and economic measures. The Economic index pooled mean for the period was 59 (Figure 1b), roughly doubling the mean of Phase 1, although low when compared with countries from other regions. Mexico was the only country that did not take measures of this kind. Again Honduras had the highest value for economic support (88). With regard to SC measures, the mean value was 80 (Figure 1c), and as it happened with restrictive measures, the dispersion between countries was much lower than for Phase 1.
At the time of Phase 3, five months have passed since the beginning of pandemic and the citizens started to show signs of weariness after experiencing long periods with restrictions. Isolation was sustained for several months and highly restrictive NPIs lost acceptance and adherence. Consequently, several restrictive measures were relaxed, which is reflected on the decrease of the pooled mean for the Stringency index (67; Figure 1a), almost 17 points lower compared to Phase 2. This is also the lowest value for this index since the beginning of the pandemic (Figure 1). The country with the lowest Stringency index value is 28 (Uruguay), while the highest value is 85 (Bolivia and Chile). Although the Economic index values also decreased, they did not do so as much as Stringency (Figure 1b). Thus, the pooled mean of the Economic index for Phase 3 is 50 (9 points below Phase 2). While Mexico continued without taking these types of measures and Bolivia reduced them to less than half, other countries such as Chile and Uruguay display an important increase in this indicator. Finally, SC index lowered a few points (Figure 1c) although the amount of measures taken by all the countries was equal. In conclusion, during Phase 3 most countries began to relax most of the measures considered by the Stringency index, although they kept the economic support and the SC at similar levels to those of Phase 2.
About the regression model used
This work was based on a multivariate regression analysis (MLR) of the TSCS type (Beck and Katz, 1995; Podestá, 2002; Stimson, 1985). TSCS is used in data sets where there are repeated observations (in our case, day of the pandemic) in fixed units by groups (countries). Unlike panel data, the TSCS model is used when there are many observations over time and there are several small‐sized or medium‐sized groups. The simple MLR model becomes problematic with these data as it breaks several assumptions of the regression. The TSCS models, on the other hand, allow temporally and spatially correlated errors and heteroscedasticity corrections using panel‐corrected standard errors (PCSEs) (Beck and Katz, 1995), calculating more accurately the parameters and applying transformations to deal with auto‐correlation of the data (details and model assumptions and diagnostics can be seen in the Supporting Information Appendix).5
TCSC modeling has the advantage of being able to simultaneously evaluate the impact of the different types of government measures on the DNI, allowing to distinguish between countries and to study the temporal sequence of the data. The database was established by country and by day of the epidemic. Day one was set when the first case of Covid‐19 was detected in each country, and it runs until September 14th due to the timeframe of the study. The maximum number of days was 198 and the average between the countries under study was 95 days.
The general approach of the model is as follows:
| (1) |
The TCSC was estimated for the three different phases already described: Phase 1 (days 1–50), Phase 2 (days 51–149), and Phase 3 (days 150–200). The phases are expressed in days because it was the cuantitative continuous variable used in the model, although there is a linear correspondence with the months mentioned above. Here, β0 is a constant and β1–β7 are the coefficients of the different variables. Two control variables of the sociodemographic block were then included: the population density, per capita GDP. These variables allowed normalizing the factor of response of the different countries. The next block of variables comprises the government response to the pandemic: the Stringency, Economic, and SC indexes. The Death Regime variable allowed to distinguish three groups of countries in accordance with their accumulated number of Covid‐19‐related deaths. Finally, e is the additive error term. Each variable has two additional subindexes, namely t and j. The subindex t indicates the time expressed in days from the onset of the pandemic. The subindex j corresponds to each country. The DNIs are incorporated in the model lagged 1 day following Beck and Katz (1995) recommendation to avoid first‐order autocorrelation error (AR‐1). Stringency, Economic, and SC indexes are lagged 14 days to account for the delayed effect of the imposed measures, as their impact became visible two weeks after their implementation (people already incubating Covid‐19 when the measures were put in place, had already been infected).
The pandemic in Latin America
Before we delve deeper into the analysis of the 15 selected Latin American countries, we will briefly review what happened in the region. The first case of coronavirus was registered in Brazil on February 26, 2020. By March 19, it had reached all the countries of the region and by June, Latin America became the epicenter of the pandemic. The countries of the region implemented different political strategies to face the emerging situation. The results obtained during the crisis management were very dissimilar as well. There were countries where the responses were lax, poorly coordinated, or delayed that ended up having an exponential growth of DNI. For example, Peru registered 722,832 accumulated cases and 30,526 deaths by mid‐September, whereas Colombia had 716,319 accumulated cases and 22,924 deaths and Mexico registered 668,381 accumulated cases and 70,821 deaths by the same date. Other countries such as Uruguay responded faster in a more coordinated manner and managed to keep the number of infections contained, with 1780 accumulated cases and 45 deaths as of September 14. Ultimately, countries such as Argentina or Bolivia took immediate measures when the first cases of Covid‐19 were registered and were able to keep the contagions contained for up to four months, after which, and perhaps due to the difficulty of sustaining the mobility restrictive measures, they began to show an increased spread of the disease.
To better understand the trajectory of the different countries of the region throughout the Covid‐19 pandemic, it is important to consider sociodemographic variables such as the population of each country.
In Figure 3, the evolution of DNI per population for each country is shown. It can be seen in the figure that up to the day 110, the growth experienced by most of the studied countries was exponential with the sole exception of Uruguay. After that point, rates began to decline and DNI growth became arithmetic in countries such as El Salvador, Guatemala, and Bolivia, while in others such as Mexico and Panama a plateau was reached. In Argentina and Peru, the growth was still not under control.
FIGURE 3.
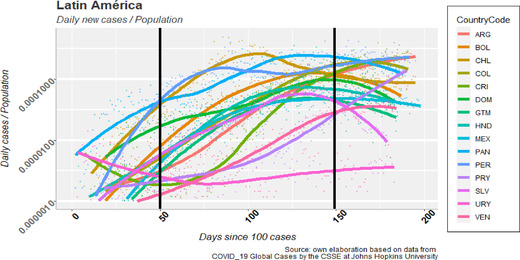
Daily new infections over population for 15 countries of latin america since the day where the 100th case was registered
Toward an explanation
As stated before, the TSCS model was used to evaluate the possible relationships and influences that the different types of measures implemented by the different governments had on the curve of DNI, by country and throughout the three different phases of the pandemic.
The parameters corresponding to the three TSCS multilinear regression models are shown in Table 1. The coefficients were calculated with PCSE for Phases 1–3.6 Each column presents the coefficients corresponding to one of the phases of the pandemic, as described before. The three regressions were statistically significant and reached an acceptable goodness of fit.
TABLE 1.
Parameters of TSCS linear regression models with panel‐corrected standard errors used to explain the new daily infections of Covid‐19 in 15 Latin American countries, throughout the three different phases of the pandemic
| Dependent variables: Number of daily new infections (DNI) | Phase 1 | Phase 2 | Phase 3 |
|---|---|---|---|
| Daily infections 1 day before (β1) | 0.75*** | 0.84*** | 0.75*** |
| (0.10) | (0.03) | (0.05) | |
| Population density (β2) | −0.01 | −0.34 | −1.78** |
| (0.05) | (0.24) | (0.72) | |
| GDP per capita (β3) | 1.76 × 10−6 | −0.00001** | −0.00004* |
| (1.14 × 10−6) | (3.95 × 10−6) | (0.00002) | |
| Stringency index (β4) | 0.39 | −9.55*** | −18.43*** |
| (0.30) | (1.91) | (5.41) | |
| Economic index (β5) | 0.38 | −1.08 | 0.46 |
| (0.20) | (1.04) | (1.48) | |
| Sanitary containment index (β6) | −1.15 | 40.65 | 154.35 |
| (3.65) | (32.61) | (139.82) | |
| Death regime (β7) | 49.90*** | 486.04*** | 1458.44*** |
| (15.28) | (78.14) | (317.79) | |
| Constant (β0) |
−93.95** (38.76) |
700.84*** (172.84) |
863.15 (449.93) |
| General R 2 | 65% | 83% | 85% |
| N observations | 524 | 1500 | 592 |
| Prob. > χ2 | 0.0000 | 0.0000 | 0.0000 |
| Observations per group | 34/35/35 | 100/100/100 | 30/39/49 |
Note: The regression coefficients and standard errors (between parentheses) are expressed for each variable. The asterisks indicate the level of significance (p) of the coefficients: α < 0.001 (***); 0.001< α < 0.01 (**); α < 0.05 (*); no asterisk means that the regression coefficient was not significant. The dependent variable was DNI by country and by day of the pandemic. See the Supporting Information Appendix for a more detailed description of the independent variables. The models were estimated with panel‐corrected standard errors and DNIlag1 of independent variable. Model with PRAIS Watson transformation is reported in the Supporting Information Appendix.
Source: Covid‐19 Dashboard from the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University and Oxford COVID‐19 Government Response Tracker (OxCGRT).
Phases 1 and 3 are characterized by the same β1 coefficient (DNI, lagged 1 day), which has a lower value than for Phase 2. This difference probably reflects that the growth in DNI was arithmetic in the former two phases and exponential in the latter one. The sociodemographic variables show some variability between phases. Population density was significant only at Phase 3 and inversely related to DNI. This counterintuitive result may be related to a better management of the most populous countries in the region during this phase. The GDP per capita was significant for Phases 2 and 3. In Phase 2, the GDP effect is strongly inversely, indicating that countries with more available resources were able to use them to curb the contagion spread. In Phase 3, GDP (β3) had almost no effect meaning that the pandemic has finally affected all countries in the region in a similar manner. Extreme poverty's coefficient (β4) was only significant for Phase 1, which is concordant with the argument that richer countries were the most affected during this phase due the increased mobility associated with international commerce and tourism. Then, the coefficients sign changed for Phase 2 to become positively related to DNI. At this stage, most countries were experiencing an exponential growth of DNI and the poorest countries were the most affected. As people living under extreme poverty conditions were forced move in search of any sort of income they got exposed to contagions. In other words, poverty generated an increased general mobility, disregarding the isolation measures still in place.
The coefficients of Stringency and Economic indexes (β5 and β6) that include relevant government measures, present significant differences across the phases. The Stringency index did not have a significant influence at the beginning of the pandemic but turned out to be significant and inversely related to DNI during Phases 2 and 3. On the contrary, the Economic and the SC indexes were not statistically significant for any of the phases.
The Death regime variable (β7), which classifies countries according to the number of accumulated deaths, was significant throughout the study. The coefficients values increased as the phases proceeded, indicating a stronger relation with DNI. The proposed country grouping in terms of the pandemic impact severity remained unchanged for the three phases. As the coefficient increased over time, the separation into these groups became more important to the analysis.
Testing different scenarios
Insofar, we were able to verify that the effectiveness of the stringency measures adopted by the Latin American governments on the DNI, varied throughout the different phases of the pandemic. In fact, the restrictive measures implemented during Phases 2 and 3 were effective in reducing DNI of Covid‐19. On the other hand, economic support measures that aimed to compensate individuals and businesses for the recession suffered by the local economies provoked by the restrictive NPIs might have had an impact on the overall well‐being of the population, however, no impact was registered on DNI in this work. Based on these, we will focus on evaluating the effect of varying the restrictive NPIs represented by the Stringency index, considering that the economies are already under considerable pressure and probably unable to guarantee further support. In addition, it was taken into consideration that the main debate that governments were facing at the time of the analysis was how to sustain the isolation or mobility restriction measures, or even if these policies made sense after eight months of evolution of the pandemic.
In order to better understand the effectiveness of the Stringency measures on a reduction on DNI and the possible interaction with the economic support NPIs we used the Markov Chain Monte Carlo (MCMC) simulation sampling technique, based on the parameters estimated with the regression analysis, we created different scenarios to check the effect of different values of Stringency measures on DNI when combined with (1) the lowest level of economic NPIs recorded (value = 0) and (2) the highest level of economic measures (96.3) and we contrasted the effects. The results of the simulations correspond to the values of Phase 37 and are presented in Figure 4. Each scenario consisted of 10,000 Monte Carlo simulations8 and allows us to show the conditional effect for a period of 20 days, since then the effect becomes constant.
FIGURE 4.
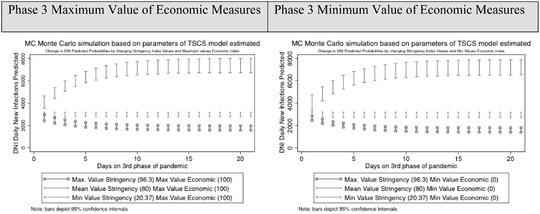
Change in DNI predicted probabilities by changing Stringency index values along maximum and minimum values of Economic index. The change in predicted DNI for any day shows the direct effect of Stringency index on this day and the cumulative lagged effect of DNI on the previous day, for a country that take a restrictive measure in day t. Ten thousand dynamic Markov Chain Monte Carlo simulations were performed for Phase 3. Simulations started with a mean value of DNI( t −1) (2993) and considered three values for Stringency index: minimum (20.37); mean (80); and maximum (96.3). The maximum value of Economic index is 100 and the minimum value is 0. The values of the rest of variables were set in their means as resulted from the model for Phase 3
The results shown in Figure 4 confirm the significance of the coefficients presented in Table 1. Clearly, the effectiveness of the stringency measures are dominant over the effect on DNI. The economic measures do not report any additional significant difference. In both scenarios, with strong economic measures and with no economic measures, the difference between applying strong Stringency measures implies going from about 1600 DNI (below the starting value) to 8000 DNI when they are eased. Therefore, restrictive measures were useful in Latin America in having a significant impact on reducing the number of DNI.
Then, we went further than evaluating the circumstantial influence that a certain package of economic measures could have on the reduction of Covid‐19 cases, thus we analyzed the effect of the structural economic situation of Latin American countries (based on their GDP per capita) can have on DNI when combined with different stringency NPIs. Does the level of wealthfare/poverty of Latin American countries modulate the effect of restrictive measures in reducing DNI? In this sense, again using MCMC simulations, we estimated the effect of Stringency measures in the following scenarios: (1) countries with a higher GDP per capita and (2) countries with the lowest level of GDP per capita.
The results shown in Figure 5 are remarkable. The level of wealthfare of a country, measured from its GDP per capita, exerts a substantive conditional influence on the management of the Covid‐19 crisis. In both Phases 2 and 3, the countries with the highest GDP per capita in the region that apply strong restrictive measures can reduce the DNI to near zero, in both phases. In this type of countries, relaxation of the Stringency measures implied increasing from zero to just over 4000 DNI in Phase 2 and to 6000 DNI in Phase 3.
FIGURE 5.
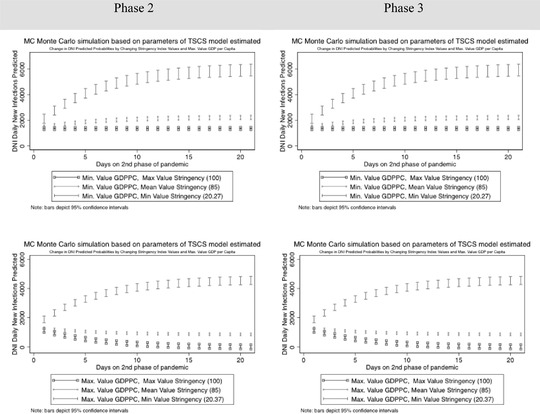
Change in DNI predicted probabilities by changing Stringency index values along maximum and minimum values of GDP per capita. The change in predicted DNI for any day shows the direct effect of Stringency index on this day and the cumulative lagged effect of DNI on the previous day, for a country that take a restrictive measure in day t. Ten thousand dynamic Markov Chain Monte Carlo simulations were performed each scenario of Phases 2 and 3. For Phase 2, simulations started with a mean value of DNI( t −1) (1350) and considered three values for Stringency index: minimum (20.37); mean (85); and maximum (100). The maximum value of GDP per capita is 22,800,000 and the minimum value is 4,541,795. The values of the rest of variables were set in their means as resulted from the model for Phase 2. For Phase 3, simulations started with a mean value of DNI( t −1) (2993) and considered three values for Stringency index: minimum (20.37); mean (85); and maximum (100). The maximum value of GDP per capita is 22,800,000 and the minimum values is 4,541,795. The values of the rest of variables were set in their means as resulted from the model for Phase 2
On the other hand, in the poorest countries, with a lower level of GDP per capita, in Phase 2 having strong restrictive MPIs implied having slightly less than 2000 DNI (way over zero). In those countries, if restrictive measures are relieved, then the number of DNI went to approximately 6000. In Phase 3, the effect is even stronger. If the poorest countries applied strong restrictive measures, they would have lower scenario close to 3000 DNI and if measures are lifted, the number went to 10,000 DNI, whereas relaxing stringency measures in rich countries implied up to 2000 DNI, and for poor countries 7000 DNI. This result likewise reinforce the importance to split the analysis of the first wave of Covid‐19 into phases in order to study in a more adequate way the impacts of the effectiveness of the measures taken by governments.
According to our findings, maintaining some restrictive measures would help to keep DNI stable or even lower them. However, governments should build a base of support for those measures. Otherwise, their effectiveness would be affected.
DISCUSSION
The new Covid‐19 disease emerged just a year ago. In a short period of time, the Coronavirus traveled around the world and drastically transformed our daily lives. Traditional forms of social organization have been transformed and the executive capacity of governments is being challenged in unprecedented ways. Every region of the world was the epicenter of the pandemic at a time, and different countries implemented diverse measures aimed at containing contagions and sustaining their local economies. As a result of these diverse measures, largely different numbers of infections and deaths were obtained. Some governments took time to respond or did it in a lax way, hoping that this kind of action would preserve the level of economic activity. In general, the consequence of this approach was the saturation (or straining) of the national health systems and an inevitable strong economic recession, in addition to a gross increase in the death toll. Other countries adopted early and effective measures, thereby managing to contain the health situation and preventing the depletion of health resources. As the pandemic went on, the measures adopted by governments were put to test and some became increasingly difficult to sustain.
In this article, we set out to evaluate the effectiveness of the different types of NIPs adopted by governments. For the sake of the analysis, we divided them into restrictive, economic and sanitary contained measures, and looked upon them in 15 Latin American countries. We found useful to divide the timeframe going from the first recorded case in each country up to September 14, 2020 into three phases because of changes on the degree of implementation of the different kinds of interventions. Governments had to face those changing dynamics as well.
During Phase 1, neither the restrictive measures nor the economic measures had visible effects on the number of DNI. We understand that during this initial phase, the pandemic barely registered the first cases in the 15 countries under study, and governments were still adapting to this new reality. The effects were not yet clear, also considering the broad incubation window (1–14 days) of the disease.
During Phase 2, the effects became clearer. The greater the restrictive measures, the lower the number of DNI. Going through the third phase of the pandemic, the effect of restrictions became even clearer. Here again, more restrictive measures implied a greater reduction in the number of DNI.
The Monte Carlo simulations allowed us to corroborate that the impact of sustaining restrictive measures was significant and implied an important reduction in the DNI. In the one hand, during the first wave of Covid‐19 in the region, Stringency measures were the main tool that the different governments had to control the number of new infections. These conclusions coincide with other work on other regions of the world (Brauner et al., 2021; Haug et al., 2020; Cheng et al., 2020; Fang, Nie, and Penny, 2020). Although this work has the limitation of not evaluating the single effect of each measure that composed the index, some previous studies have drawn important conclusions in this regard. Thus, for instance, Brauner et al. (2021) found that the most effective measures to reduce the infections were: closure of educational institutions; banning gatherings of 10 people or less; targeted closures of face‐to‐face businesses; closing most nonessential businesses. All these measures contemplated in the Stringency index. On the other hand, the economic measures did not show significant direct or conditional effects on DNI.
The simulations of different scenarios allowed us to evidence two other substantive facts. First, taking into account that this work was focused on studying Latin American countries, where most are developing countries with low average incomes, and with significant parts of their population living in poverty, we were able to highlight how the level of wealthfare of a country affects the effectiveness of stringency measures in reducing DNI, therefore, the effectiveness of a combination of public policies aimed to save lives has greater and more effective impact if the country is rich, reducing infections to zero in our modeled results. In contrast, if poor countries could have applied strong restrictions, the reduction would have been of approximately 2000 DNI in Phase 2 and 3000 DNI in Phase 3, a huge difference when compared to zero. If restrictive measures were eased, and considering Phase 3 for the example, the effect in the richest countries implied going from zero to approximately 5000 DNI, while in contrast, in poor countries the best case scenario was going from 3000 to 10,000 DNI. Such a difference may imply the collapse of the health system, also considering that the number of resources is likewise expected to be greater in richer countries.
Lastly, these results also evidenced another important fact. The conditional effect of the level of GDP per capita was stronger in Phase 2 than in Phase 3, denoting the importance of considering the temporal sequence in which the measures were implemented to study the effectiveness of NPI during the first wave of the pandemic in Latin America (Cheng et al., 2020; Fang, Nie, and Penny, 2020; Hale et al., 2021; Jayatilleke et al., 2020).
CONCLUSION
Among all the combined groups or types of measures implemented by most Latin American governments, the restriction measures (Stringency index) were the most efficient in controlling the number of DNI. The implementation of different degrees of economic support or SC measures, may have had an impact on the overall well‐being of the population but without restrictive measures, and are policies to manage the pandemic to a social degree, although they had no effect on the progression of DNI throughout this first wave of the pandemic.
The modeled effect of the restrictive NPIs was strongly modulated by the welfare of the countries under study (represented by GDP per capita in this study) thus suggesting that the spread of the disease if faster in poor countries at the same level of the Stringency index.
Supporting information
Appendix Material: 1 Codebook
Table I: Stringency and Economic indexes for the countries under study for each pandemic phase.
ACKNOWLEDGEMENT
The authors appreciate the valuable comments of the anonymous reviewers who allowed us to improve the article. They also want to acknowledge the contributions and comments that Lorena Barberia, Alberto Baruj, Leandro DaRold, Anabella Fantozzi and Manuel de Paz made to previous versions of this paper. This paper was made thanks to the contributions of the projects: PIP 0254; PICT 2017/2306; RN 02 COVID FEDERAL EX‐2020‐39070362 of the Ministry of Science, Technology and Innovation of Argentina.
Ratto MC, Cabrera JM , Zacharías D, Azerrat JM. The effectiveness of government measures during the first wave of the outbreak. Social Science Quarterly. 2021;102:2088–2105. 10.1111/ssqu.13043
Footnotes
This began in China, rapidly expanding to Southeast Asia and Asia, and then it arrived to Europe, then moved to the United States and later arrived quite simultaneously to the countries of Latin America.
To see another interesting background at the subnational level, refer to Behrend and Karamaneff (2021). They explore socioeconomic measures adopted by subnational governments in Argentina during the sanitary crisis unleashed by the Covid‐19 pandemic.
To see more details about the Oxford base you can visit the following link https://www.bsg.ox.ac.uk/research/research‐projects/coronavirus‐government‐response‐tracker.
The idea for this figure comes from a similar one from Brauner et al. 2021
For more details on the estimation and the ways to control the model, read Beck and Katz (1995).
Statistics under Durbin–Watson, Wooldridge test, Arellano–Bond test transformation are reported in the Appendix, to deal with autocorrelation of the data. Both results were similar in all aspects (sign and significance) with those reported in Table 1.
In the Appendix, there are those plots corresponding to phase 2, which are very similar to phase 3, with the only difference that in phase 2 the effect is a little lower.
To see another example of this type of dynamic simulations, refer to Poe and Tate (1994).
REFERENCES
- Azerrat, J. M. , Ratto M. C., and Fantozzi A.. 2021. “Gobernar es cuidar? Los estilos de gestión de la Pandemia en América del Sur: Los casos de Argentina, Brasil y Uruguay.” Trabajo y Sociedad 23(36):145–73. [Google Scholar]
- Barberia, L. , Cantarelli L., Claro M. L., de Paula Moreira N., Seelaender Costa Rosa I., Schmalz P., da Silva Pereira F., and Zamundio M.. 2020b. “The Effect of State‐Level Social Distancing Policy Stringency Measures (SDPS) on Willingness to Distance in the States of Brazil.”. Mimeo, June 2020. [Google Scholar]
- Barberia, L. G. , Cantarelli L., Claro M. L., Rosa I. S. C., da Silva Pereira F., and Zamudio M.. 2020a. “Confronting the COVID‐19 Pandemic: Brazilian Federal and Subnational‐Government Responses, Technical Report on Social Distancing Stringency (SDS) 1.0.” Technical report. University of Sao Paulo. [Google Scholar]
- Beck, N. , and Katz J. N.. 1995. “What to Do (and Not to Do) with Time‐Series Cross‐Section Data.” American Political Science Review 89(3):634–47. [Google Scholar]
- Behrend, J. , and Karamaneff L.. 2021. “La variación subnacional en la respuesta socioeconómica a la pandemia en Argentina.” Trabajo y sociedad 21(36):175–202. [Google Scholar]
- Brauner, J. M. , Mindermann S., Sharma M., Johnston D., Salvatier J., Gavenčiak T., and Kulveit J.. 2021. “Inferring the Effectiveness of Government Interventions against COVID‐19.” Science 371(6531). 10.1126/science.abd9338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheng, C. , Barceló J., Hartnett A. S., Kubinec R., and Messerschmidt L.. 2020. “COVID‐19 Government Response Event Dataset (CoronaNet v. 1.0).” Nature Human Behaviour 4(7):756–68. [DOI] [PubMed] [Google Scholar]
- Fang, Y. , Nie Y., and Penny M.. 2020. “Transmission Dynamics of the COVID‐19 Outbreak and Effectiveness of Government Interventions: A Data‐Driven Analysis.” Journal of Medical Virology 92(6):645–59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Felson, J. , and Adamczyk A.. 2021. “Online or in Person? Examining College Decisions to Reopen during the COVID‐19 Pandemic in Fall 2020.” Socius 7:1–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gupta, S. , Nguyen T. D., Rojas F. L., Raman S., Lee B., Bento A., Kosali I. S., and Wing C.. 2020. “Tracking Public and Private Responses to the Covid‐19 Epidemic: Evidence from State and Local Government Actions.” NBER Working paper series . National Bureau of Economic Research. [Google Scholar]
- Hale, T. , Angrist N., Goldszmidt R., Kira B., Petherick A., Phillips T., Webster S., Cameron‐Blake E., Hallas L., Majumdar S., and Tatlow H.. 2021. “A Global Panel Database of Pandemic Policies (Oxford COVID‐19 Government Response Tracker).” Nature Human Behaviour 5(4):529–38 . [DOI] [PubMed] [Google Scholar]
- Haug, N. , Geyrhofer L., Londei A., Dervic E., Desvars‐Larrive A., Loreto V., Pinior B., Thurner S., and Klimek P.. 2020. “Ranking the Effectiveness of Worldwide COVID‐19 Government Interventions.” Nature Human Behaviour 4(12):1303–12. [DOI] [PubMed] [Google Scholar]
- Hussain, A. H. M. B. 2020. Stringency in Policy Responses to Covid‐19 Pandemic and Social Distancing Behavior in Selected Countries . 10.2139/ssrn.3586319. [DOI]
- Jayatilleke, A. U. , Dayarathne S., de Silva P., Siribaddana P., Abeygunawardana R. A., Nieveras O., de Silva N., and de Silva J.. 2020. “COVID‐19 Case Forecasting Model for Sri Lanka Based on Stringency Index.” medRxiv. 10.1101/2020.05.20.20103887. [DOI] [Google Scholar]
- Kim, S. , Ko Y., Kim Y.‐J., and Jung E.. 2020. “The Impact of Social Distancing and Public Behavior Changes on COVID‐19 Transmission Dynamics in the Republic of Korea.” Plos One 15(9):e0238684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liang, L. L. , Tseng C. H., Ho H. J. et al. 2020. . “Covid‐19 Mortality is Negatively Associated with Test Number and Government Effectiveness.” Scientific Reports 10. 10.1038/s41598-020-68862-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Podestà, F. 2002. “Recent Developments in Quantitative Comparative Methodology: The Case of Pooled Time Series Cross‐Section Analysis.” DSS Papers Soc 3‐02, 5–44. Università degli Studi di Brescia. [Google Scholar]
- Poe, S. C. , and Tate C. N.. 1994. “Repression of Human Rights to Personal Integrity in the 1980s: A Global Analysis.” American Political Science Review 88(4):853–72. [Google Scholar]
- Sebastiani, G. , Massa M., and Riboli E.. 2020. “Covid‐19 Epidemic in Italy: Evolution, Projections and Impact of Government Measures.” European Journal of Epidemiology 35:341–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stimson, J. A. 1985. “Regression in Space and Time: A Statistical Essay.” American Journal of Political Sciences 29(4):914–47. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix Material: 1 Codebook
Table I: Stringency and Economic indexes for the countries under study for each pandemic phase.