

Abstract
Centuries of practice and an array of public health literature support social distancing (SD), or self‐quarantine, as a valuable nonpharmaceutical intervention. To convince individuals to engage in behaviors that limit infection, public health professionals communicate risk and hazard based on application of protection motivation theory (PMT). The COVID‐19 pandemic presents an opportunity to explore the efficacy of PMT in the context of a novel coronavirus with unique public health implications. We test an integrative conceptual model of social distancing compliance in U.S. counties and examine the mediating impact of SD on community spread of infection. We find that PMT does impact individual behavior, observing that the proportion of vulnerable populations affects social distancing compliance. However, actions to protect individual health are made within the context of economic concerns and priorities. While results indicate that PMT influences behavior, the expected relationship between that behavior and spread of disease in the community is not found. We do not repudiate SD or the value of PMT, but we suggest that these results may indicate that communication of risk in the context of COVID‐19 may need community, as well as individual, framing.
Keywords: COVID‐19, economic motivation, nonpharmaceutical interventions, protection motivation, social distancing compliance
摘要
几百年的实践和大量公共卫生文献都将保持社交距离或自我隔离作为重要的非药物干预。为说服个体采取限制感染的行为,公共卫生专家在应用保护动机理论(protection motivation theory)的基础上传播风险和灾害信息。新冠肺炎(COVID‐19)大流行提供一个机会,探究保护动机理论在具有独特公共卫生意义的新型冠状病毒情境中的效能。我们在美国多个县中检验一项关于社交距离依从性(social distancing compliance)的综合概念模型,并分析了保持社交距离对社区感染传播产生的中介作用。我们发现,保护动机理论的确会影响个体行为,并发现弱势群体比例会影响社交距离依从性。不过,保护个体健康的行动是在经济关切和经济重点的情境下进行的。尽管研究结果表明,保护动机理论会影响行为,但并未发现行为和社区疾病传播之间的期望关系。我们不否认社交距离或保护动机理论的价值,但我们建议,这些结果可能表明新冠肺炎(COVID‐19)情境下的风险传播可能需要社区和个体的建构。
Resumen
Siglos de práctica y una variedad de literatura sobre salud pública apoyan el distanciamiento social, o la autocuarentena, como una valiosa intervención no farmacéutica. Para convencer a las personas de que adopten comportamientos que limiten la infección, los profesionales de la salud pública comunican el riesgo y el peligro basándose en la aplicación de la teoría de la motivación de protección. La pandemia de COVID‐19 presenta una oportunidad para explorar la eficacia de la teoría de la motivación de protección en el contexto de un nuevo coronavirus con implicaciones únicas para la salud pública. Probamos un modelo conceptual integrador de cumplimiento del distanciamiento social en los condados de EE. UU. Y examinamos el impacto mediador del distanciamiento social en la propagación de la infección en la comunidad. Encontramos que la teoría de la motivación de protección sí impacta el comportamiento individual, observando que la proporción de poblaciones vulnerables afecta el cumplimiento del distanciamiento social. Sin embargo, las acciones para proteger la salud individual se realizan dentro del contexto de preocupaciones y prioridades económicas. Si bien los resultados indican que la teoría de la motivación de protección influye en el comportamiento, no se encuentra la relación esperada entre ese comportamiento y la propagación de la enfermedad en la comunidad. No repudiamos el distanciamiento social o el valor de la teoría de la motivación de protección, pero sugerimos que estos resultados pueden indicar que la comunicación del riesgo en el contexto de COVID‐19 puede necesitar un marco comunitario, así como individual.
INTRODUCTION
A significant role of public health professionals during a national health emergency is to communicate risk and motivate compliance with behaviors that will reduce health hazards. In the COVID‐19 pandemic, public health officials have uniformly advocated for social distancing (SD) as the first line of defense against the novel coronavirus. The practical value of SD as a low‐cost intervention to reduce the spread of infectious disease is clear in literature from public health and epidemiology. Evaluation of public health readiness in the face of the 2009 H1N1 flu (Baum et al., 2009), SARS (Cava et al., 2005), and Ebola (Desclaux et al., 2017) confirmed the efficacy of SD to reduce spread of disease. However, there are limits to the application of the previous research on SD. First, none of these prior pandemic threats was a nationally widespread infectious event in the United States. Second, transmission of COVID‐19 has not followed the same patterns as H1N1 flu, SARS, or Ebola (Gensini et al., 2004). Third, infectious disease research on the efficacy of quarantine generally relates to the biological attributes associated with infection. While a logical extension, SD applied at the community level may be efficacious for reduced spread of infection only within certain parameters. Finally, a unique element of COVID‐19 is that its impact on subpopulations is not uniform. Some subgroups have a low probability of serious harm (WHO, 2020). Thus, the willingness of the community to adopt SD based on the perception of risk may vary significantly by demographic characteristics.
This study examines issues of social distancing compliance at the community level of analysis. We examine the impact of demographic variables on compliance with community SD protocols while also accounting for economic variables that provide countervailing motivation for social distancing compliance. We then look at whether community social distancing compliance acts as the expected mediator in predicting subsequent changes in community spread of infection. Our findings have implications for how the unique characteristics of this novel coronavirus may impact the community's self‐protection behaviors and perception of risk.
The importance of SD in limiting spread of infectious disease
Research in infectious disease control stipulates that nonpharmaceutical interventions can be effective in reducing rates of transmission (Bell et al., 2006; Jefferson et al., 2011). The World Health Organization (WHO, 2020) and the U.S. Centers for Disease Control and Prevention (CDC, 2020a) have recommended a series of nonpharmaceutical interventions, such as hand washing, SD (self‐quarantine), and mask wearing, as strategies for reducing the biological spread of COVID‐19. There is substantial evidence from a variety of research streams to suggest that human behaviors can reduce transmission of disease. Quarantine is a remedy that reduces disease transmission by limiting the opportunity for pathogens to transfer from one host to another (Gensini et al., 2004). Mathematical modeling (Ferguson et al., 2020; Greenstone & Nigam, 2020), where assumptions regarding communicability and dispersion of pathogens contribute to the conclusions, promote the value of SD and self‐quarantine as a powerful nonpharmaceutical intervention. Despite the demonstrable benefit of SD to public health, SD implementation is not uniform (Abouk & Heydari, 2020; Sundwall, 2019). This suggests that SD has elements of both individual and communal response. While individual quarantine may be highly effective as a personal protection strategy, extent of community compliance impacts efficacy of SD as a public health intervention.
Elements that enhance and hinder social distancing compliance
Research on the psychology of health behaviors has long examined what motivates people to adopt changes in behavior in response to perceived threats to health. Rogers (1975) is credited with articulating protection motivation theory (PMT). PMT has been used in a variety of studies to examine and explain individual behavior. Generally, findings have shown that the perceived threat associated with a health condition is associated with vulnerability to the condition, potential severity of the condition, and fear of the condition (Rippetoe & Rogers, 1987). Self‐efficacy and response efficacy, the perception that individuals have the ability to protect themselves and the belief that recommended health actions will work (Maddux & Rogers, 1983), are related to an individual's willingness to adopt recommended health behaviors.
More recently, Williams et al. (2015) looked at the relationship between PMT and SD and found, in a simulated study, that PMT variables (vulnerability, fear, response efficacy, and self‐efficacy) were associated with individual intention to engage in SD. Other research also identified these variables as predicting behavioral responses to respiratory infectious diseases (e.g., Teasdale et al., 2012, 2014). However, both Williams et al. (2015) and Teasdale et al. (2012) found a gap between individual intention to social distance and changed behavior. Both researchers concluded that, regardless of intent, SD or self‐quarantine may be difficult for individuals to implement.
Baum et al. (2009) conducted focus groups with citizens during the H1N1 flu epidemic to characterize public perceptions about SD measures likely to be implemented during a pandemic. They found that, while focus group members generally understood the need to engage in SD, their health concerns were outweighed by concerns regarding the potential economic hazard of such measures. “Immediate economic needs, job security, the need for essential goods and services, and long‐term effects on the economy from extended business or school closure or quarantine were among concerns addressed” (Baum et al., 2009, p. 6). Bhattacharyya and Reluga (2019) modeled social distancing compliance and found that individual compliance was dependent on the perceived costs of the compliance behavior. Greater transmissibility of the disease tended to increase the individual's perceived cost, thus the authors concluded that the more infectious the disease, the greater the cost and the more likely SD would be effective at reducing community spread, particularly early in the pandemic.
Singh et al. (2019) combined demographic and survey data to do extensive modeling of self‐protective behaviors, including SD, in conjunction with influenza. The research examined demographic characteristics in U.S. urban and rural counties. In addition to finding differences based on population size, which was reflective of the urban and rural distinction, the researchers found that both age and income affected the probability of individual compliance with SD and the willingness to accept vaccination. Younger and lower income subjects were less likely to comply with self‐quarantine and engage in self‐protective behaviors. This finding would be consistent with PMT. We could also expect that older populations and higher income populations might perceive greater vulnerability, fear, and costs, as well as have greater response efficacy and self‐efficacy regarding the importance of their personal actions.
An integrative predictive model of community social distancing compliance
This study draws on earlier findings to create and test an integrative model of predictors of community social distancing compliance. From health behavioral psychology, we use PMT and posit that demographic factors related to increased vulnerability to COVID‐19 will tend to predict greater social distancing compliance in the community. Knittel and Ozaltun (2020) report the results of a comprehensive analysis of U.S. demographic data by county and identify age, African American race, share of nonworking people, and household income as significant predictors of vulnerability to death from COVID‐19. We would expect that areas of the country with higher proportions of these characteristics would have higher levels of social distancing compliance. In addition, we identify educational attainment and internet access as proxies for increased self‐efficacy and response efficacy. Areas with a greater share of educated people and people with access to information are more likely to have greater confidence in their ability to implement SD and to better understand SD's impact and potential value.
Drawing on research using mathematical modeling, we suggest that economic costs of SD would also impact social distancing compliance. Areas with higher levels of unemployment, low‐wage workers, and essential employees would be less likely to adopt SD or might be prohibited from it by government order.
Finally, from recent research on SD associated with COVID‐19, we include governmental context as having a potential impact on perception of individual hazard and thus social distancing compliance. Prior research has identified partisanship (Painter & Qiu, 2020) as influential in adopting health‐related behaviors associated with COVID‐19. In addition, the length of time under government‐issued SD orders may both reduce citizen response efficacy and increase economic costs, thus reducing social distancing compliance. We further posit that governments, like individuals, weigh the potential economic costs of mandating social distancing compliance (Béland et al., 2020). States that are heavily reliant on sales tax as a form of revenue would be less likely to encourage citizen compliance with SD.
Consistent with public health literature, our model posits that social distancing compliance reduces the spread of infection (Wilder‐Smith & Freedman, 2020). Although public health literature examining predictors of SD is usually distinct from literature that models a relationship between SD and infectious spread, our integrative model seeks to test the logical link between these two streams. A graphic depiction of our research model can be found in Figure 1.
Figure 1.
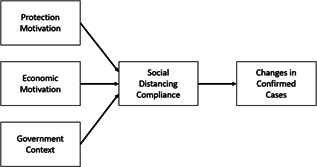
The conceptual path analysis
METHOD
Data and measurements
To test our conceptual model, we integrated data from eight sources: (1) USAFacts (2020) provided data on COVID‐19 cases and deaths; (2) Unacast provided SD data, specifically reduction on average daily distance traveled relative to the previous year; (3) American Community Survey (ACS) provided 5‐year estimates for demographic and socioeconomic attributes; (4) the Bureau of Labor Statistics was the source for the share of workers in essential industries; (5) the Department of Labor provided statewide unemployment rates; (6) NBC News and New York Times (Mervosh et al., 2020) were the sources for the dates that state stay‐at‐home orders were issued and lifted; (7) MIT Election Data and Science Lab (2019) was the source for presidential voting results, and (8) the U.S. Census Bureau supplied each state's dependence on sales tax revenue. Table 1 describes the 11 predictor variables used to represent the three concepts in our integrative model—protection motivation, economic motivation, and government context—and how they were measured. Except where noted, all data are at the county level, which is the most granular level for which data are widely available and relevantly current. Stay‐at‐home orders were largely issued at the state level. State budget reliance on consumer spending was also at that level of aggregation. Unemployment data reflecting the rapidly changing economic environment was only available at the state level at the time of this study.
Table 1.
Variables and sources
| No. | Types | Explanation | Data source | Variables | Headings | |
|---|---|---|---|---|---|---|
| 1 | Dependent | Weekly change in COVID‐19 cases per 1000, May 1–8, 2020 | USAFacts | Change in Cases | CASES1 | |
| Weekly change in COVID‐19 cases per 1000, May 22–29, 2020 | CASES2 | |||||
| 2 | Mediator | Change in daily distance traveled, April 24, 2020 | Unacast | Social Distancing Compliance | SD | |
| 3 | Independent | Protection Motivation | Death count per 1000, April 24, 2020 | USAFacts | Deaths | DEATHS |
| 4 | Nonwhite population (%) | ACS 2018 5‐year estimate | Nonwhite Population | Nonwhite | ||
| 5 | Population over 60 years of age (%) | Older Population | OLD POP | |||
| 6 | Population with a bachelor's degree or higher (%) | High Educational Attainment | HIGH EDU | |||
| 7 | Households subscribing to internet (%) | Internet Subscribers | USE INT | |||
| 8 | Economic Motivation | Employment share in essential industries (%) | Bureau of Labor Statistics | Essential Workers | ESSENTIAL | |
| 9 | Households earning less than $60,000 per year (%) | ACS 2018 5‐year estimate | Lower Income | LESS60K | ||
| 10 | Statewide unemployment rate (%) | U.S. Department of Labor | Unemployment | UEMP | ||
| 11 | Government Context | Ratio of 2016 presidential votes for Republican candidate versus Democratic candidate | MIT Election Data and Science Lab | Republican Dominance | REPUBLICAN | |
| 12 | Days spent under stay‐at‐home order as of April 24, 2020 | NBC News and New York Times | Stay at Home | STAY HOME | ||
| 13 | State budget reliance on sales tax revenues (%) | U.S. Census Bureau | Sales Tax | S TAX | ||
Mediator variable: Measuring social distancing compliance
SD is not a new concept. Restricting the movement of people, or quarantining, has been used throughout history to limit the spread of disease (Wilder‐Smith & Freedman, 2020). However, modern technology is providing novel ways of observing and monitoring how well people adhere to recommendations regarding limiting movement and physical contacts. For this analysis, we chose to use SD data found in ESRI (2020), COVID‐19 GIS Hub, which was provided by the data analytics firm Unacast. Unacast, which maps human mobility through cell phone location tracking to provide insights for retail, hospitality, tourism, and other businesses, developed a COVID‐19 SD Scorecard, allowing government agencies and health‐care organizations to understand how residents were responding to interventions designed to slow the spread of COVID‐19 (Unacast Updates Social Distancing Scoreboard‐Unacast, 2020). Unacast collects location data from a variety of third‐party sources, including software development kits it places in apps (Morrison, 2020). The technology potentially raises troubling questions about personal privacy, but it may provide the most reliable snapshot of the behavior choices of cell phone users in counties throughout the United States.1 For this analysis, we used only one element of Unacast's Scorecard as our variable of interest: Social Distancing Compliance—measured as the change on average distance traveled by aggregated cell phone users in each county, compared to baseline county activity for the same day of the week in the same time period before COVID‐19. The data was scaled such that higher numbers represent greater social distancing compliance.
Dependent variable: Change in cases
USAFacts (2020) provides a daily update of the confirmed COVID‐19 cases and the number of deaths since the detection of the novel coronavirus SARS‐CoV‐2 in the United States. The collection date for much of our data used in this study was April 24, 2020 through May 29, 2020. This period was selected as representative of the time when most of the U.S. was under “stay‐at‐home” restrictions of some kind.2 Public health communication emphasized protection motivation and self‐quarantine. Social distancing compliance data was collected as of April 24, 2020. Given that the incubation period between exposure to the virus and onset of illness is roughly two weeks (Lauer et al., 2020) and due to widespread accounts of testing challenges and delays in reporting results, we used the weekly change in confirmed cases from May 22 to 29 as our dependent variable.3 To account for population differences, our Change in Cases variable was calculated as the change in cases per every 1000 county residents for the identified period.
Predictor variables: Protection motivation
Demographic and socioeconomic characteristics for 3048 U.S. counties were gathered from the 2018 ACS 5‐year estimate, the most recent for which county‐level data are available. As noted earlier, PMT posits that individuals are most likely to alter behaviors to protect themselves from a health threat based on their perceived vulnerability to the disease, the potential severity of the condition, and their fear of contracting the illness (Rippetoe & Rogers, 1987). As such, five variables were used to represent our conceptualized Protection Motivation, three reflecting the potential fear, vulnerability, and severity of disease, and two proxying self‐efficacy and response efficacy. Specifically:
Deaths, measured as the total number of deaths per 1000 county population as of April 24, 2020. Lethality and proximity of the disease are expected to encourage more SD.
Older Population, measured as the ratio of county population that is age 60 or older to the population under 60. Most deaths from COVID‐19 have been among older people so counties with a higher portion of older residents are expected to have more residents motivated to social distance.
Non‐White Population, measured as the share of county population that is Non‐White or Hispanic. Data suggests that African‐Americans and Hispanics contract and die from COVID‐19 in disproportionate numbers so counties that are more diverse are likely to have more residents who are motivated to social distance to protect themselves.
High Educational Attainment, measured as the share of county population age 25 and older that has at least a bachelor's degree. This is one of two proxy measures for efficacy, residents’ knowledge of effective protection measures, such as SD, and belief that they can alter their behaviors.
Internet Subscribers, measured as the share of households that subscribe to the internet. A higher share of residents with access to information regarding effective protection measures such as SD serves as another proxy for the self‐efficacy and response efficacy associated with increased compliance.
Predictor variables: Economic motivation
Mathematical modeling indicates that individuals’ compliance with public health recommendations are also affected by economic conditions and concerns. Therefore, we posit that counties experiencing greater economic motivations and strains will see lower social distancing compliance. For this study, three variables represent our Economic Motivation concept:
Lower Income, measured as the share of county households earning less than $60,000 annually, which was roughly the national average in 2019 (US Census Bureau, 2020). Guided by Singh et al. (2019), counties with a greater share of lower income households are expected to see less social distancing compliance. Lower income workers may be less likely to be able to work from home. However, low‐wage households may be more likely to be headed by workers idled due to retail, personal care, restaurant and hospitality, and other service business closures. Under those circumstances, travel for work purposes would be reduced.
Essential Workers, measured as the percentage of county employment in 23 industries and sectors requiring workers to remain on the job performing important goods‐producing or service activities (see Appendix A for a complete list.) Our cluster of industries and sectors does not encompass all industries allowed to continue operating under states’ varying “essential” designations. Instead, the cluster attempts to capture a comparable share of workers whose jobs providing health services, making protective equipment and materials, or providing food and necessities prevent them from staying at home. A larger share of such employment is expected to reduce SD.
Unemployment, measured as the state‐insured unemployment rates for each state for the week ending April 25, 2020. Available county‐level employment rates significantly lag the economic downturn brought on by the COVID‐19 pandemic. Therefore, we chose to use this more relevant but less granular state‐level measure to represent the varying economic conditions of counties. Unemployed workers certainly would be expected to feel the economic costs of disease mitigation efforts, but, with their need to travel for employment reduced, they may be more likely to comply with SD.
Predictor variables: Government context
Recent research indicates that responses to the pandemic have been shaped by political views. We also can assume that governments, like individuals, may weigh the economic costs of social distancing compliance. We use three variables to represent our conceptualized Government Context:
Stay‐at‐Home Order, measured as the number of days spent under an official state order restricting residents’ movements as of April 24, 2020.4 Abouk and Heydari (2020) found that government mandates, not simply recommendations, increased social distancing compliance. However, we expect that longer durations of such orders may increase economic costs, thus reducing social distancing compliance.
Sales Tax, measured as the share of each county's home state budget for 2019 accounted for by sales taxes. States that rely more heavily on sales taxes and gross receipts for revenue may be less likely to send a strong message of SD (which would reduce local spending) and thus inhibit compliance.
Republican Dominance, measured as the ratio of county votes cast for the Republican candidate to votes cast for the Democratic candidate in the 2016 presidential election. Andersen (2020) and Kushner Gadarian et al. (2020) found partisanship to influence SD decisions. Therefore, we expect lower levels of social distancing compliance the greater the dominance of Republican votes.
Methodology
We examined path analysis models to investigate how protection motivation, economic motivation, and government context indicators affected social distancing compliance and, ultimately, the change in county case counts. Path analysis uses ordinary least squares and maximum likelihood methods to predict path coefficients. Our primary focus in this study was predictors of social distancing compliance and SD's role as mediator between the independent variables and the dependent variable, change in COVID‐19 cases.
Guided by Singh et al. (2019), who found distinct differences between urban and rural county characteristics and responses, we divided our counties into two categories—urbanized and nonurbanized—and conducted separate path analyses. We defined urbanized counties as those where all or any part is included in a metropolitan statistical area; all else were categorized as nonurbanized.
RESULTS
Analysis of means and correlation
Table 2 presents the means, SDs, and correlations of our variables for the two different groupings—urbanized and nonurbanized—of U.S. counties. The table indicates that the two groups vary substantially both in their makeup and their COVID‐19 risk. For example, the weekly change in case counts for the 949 urbanized counties is substantially greater than for the 2099 nonurbanized counties; mean death counts were more than double in the urbanized counties (0.09 per 1000 residents compared to 0.04 in nonurbanized counties). Demographically urbanized counties are younger, more diverse, better educated, more highly paid, less Republican‐leaning, and more digitally connected, suggesting greater self‐efficacy in response to the risk. Additional risk factors were also present in urbanized counties. A higher share of workers in urbanized counties were employed in our bundle of “essential” industries and sectors (14.7% vs. 10.7% in nonurbanized counties). Although three variables were measured at the state level, there was at least a percentage point difference between the urbanized and nonurbanized counties for unemployment (13.8%–12.2%) and for the portion of the state budget funded by sales tax (49.7%–50.7%). Taken together, these variables indicated a potentially reduced response efficacy in urbanized areas. Finally, residents in urbanized counties spent more than four days longer under stay‐at‐home orders, compared to residents in nonurbanized counties (25.2 and 20.9, respectively).
Table 2.
Descriptive statistics and correlations
| Urbanized counties | N:949 | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | Variables | Mean | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 |
| 1 | SD | 39.8370 | 10.9051 | 1 | |||||||||||||
| 2 | CASES1 | 2.7563 | 9.1546 | 0.444** | 1 | ||||||||||||
| 3 | CASES2 | 2.2826 | 7.5480 | 0.406** | 0.819** | 1 | |||||||||||
| 4 | DEATHS | 0.0774 | 0.1523 | 0.304** | 0.495** | 0.394** | 1 | ||||||||||
| 5 | NON‐WHITE | 20.4087 | 14.6201 | 0.201** | 0.423** | 0.477** | 0.266** | 1 | |||||||||
| 6 | OLD POP | 29.2698 | 9.8831 | −0.139** | −0.316** | −0.365** | −0.032 | −0.433** | 1 | ||||||||
| 7 | HIGH EDU | 28.3714 | 10.7274 | 0.682** | 0.396** | 0.399** | 0.188** | 0.164** | −0.272** | 1 | |||||||
| 8 | USE INT | 79.7542 | 6.9041 | 0.511** | 0.334** | 0.325** | 0.113** | 0.011 | −0.302** | 0.745** | 1 | ||||||
| 9 | ESSENTIAL | 14.6982 | 4.1173 | −0.018 | 0.233** | 0.223** | 0.107** | 0.056 | −0.018 | −0.097** | −0.038 | 1 | |||||
| 10 | LESS60K | 61.4421 | 10.6121 | −0.453** | −0.361** | −0.326** | −0.185** | 0.006 | 0.259** | −0.713** | −0.819** | 0.126** | 1 | ||||
| 11 | UEMP | 13.7844 | 5.3456 | 0.045 | 0.063 | 0.041 | 0.175** | 0.047 | 0.036 | −0.035 | 0.033 | 0.100** | −0.069* | 1 | |||
| 12 | REPUBLICAN | 11.4861 | 25.5655 | 0.102** | 0.120** | 0.117** | −0.031 | 0.140** | −0.035 | 0.126** | −0.005 | 0.012 | 0 | −0.119** | 1 | ||
| 13 | STAY HOME | 25.1918 | 8.0783 | 0.187** | 0.195** | 0.125** | 0.259** | −0.032 | 0.051 | 0.085** | 0.194** | 0.113** | −0.224** | 0.471** | −0.043 | 1 | |
| 14 | S TAX | 49.7977 | 16.5882 | −0.137** | −0.074* | −0.059 | −.093** | −.102** | 0.05 | −0.219** | −0.190** | 0.003 | 0.206** | −0.357** | 0.116** | −0.253** | 1 |
| Nonurbanized counties | N: 2099 | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | SD | 31.1384 | 13.9673 | 1 | |||||||||||||
| 2 | CASES1 | 0.1538 | 0.5004 | 0.003 | 1 | ||||||||||||
| 3 | CASES2 | 0.1556 | 0.4820 | −0.005 | 0.651** | 1 | |||||||||||
| 4 | DEATHS | 0.0356 | 0.1236 | −0.003 | 0.345** | 0.285** | 1 | ||||||||||
| 5 | Nonwhite | 15.3461 | 17.1314 | −0.047* | 0.292** | 0.349** | 0.227** | 1 | |||||||||
| 6 | OLD POP | 36.5846 | 10.2348 | 0.041 | −0.291** | −0.315** | −0.139** | −0.326** | 1 | ||||||||
| 7 | HIGH EDU | 18.4413 | 6.8759 | 0.266** | −0.055* | −0.100** | −0.048* | −0.131** | 0.142** | 1 | |||||||
| 8 | USE INT | 70.6710 | 8.5515 | 0.196** | −0.038 | −0.112** | −0.066** | −0.337** | −0.006 | 0.638** | 1 | ||||||
| 9 | ESSENTIAL | 10.7028 | 5.2839 | 0.023 | 0.171** | 0.195** | 0.105** | 0.052* | −0.079** | 0.036 | 0.071** | 1 | |||||
| 10 | LESS60K | 71.3271 | 8.2194 | −0.126** | −0.014 | 0.057** | 0.059** | 0.218** | 0.102** | −0.589** | −0.707** | 0.042 | 1 | ||||
| 11 | UEMP | 12.1808 | 4.4115 | 0.084** | 0.119** | 0.119** | 0.195** | 0.122** | 0.049* | −0.130** | −0.096** | 0.075** | 0.138** | 1 | |||
| 12 | REPUBLICAN | 24.8789 | 24.5963 | −0.032 | 0.102** | 0.108** | 0.026 | 0.230** | −0.032 | −0.018 | −0.067** | 0.002 | 0.001 | 0.067** | 1 | ||
| 13 | STAY HOME | 20.9214 | 11.0409 | 0.082** | 0.055* | 0.015 | 0.094** | −0.109** | 0.042 | −0.026 | 0.133** | 0.053* | −0.037 | 0.472** | 0.027 | 1 | |
| 14 | S TAX | 50.7298 | 16.7435 | −0.145** | 0.060** | 0.047* | −0.004 | 0.013 | −0.122** | −0.248** | −0.194** | −0.017 | 0.155** | −0.194** | 0.261** | −0.002 | 1 |
*p < 0.05.
**p < 0.01.
Differences between the two county groupings can also be seen in the correlations between variables. Social Distancing Compliance is significantly positively correlated with the Change in Cases and Deaths measures in urbanized counties but not in nonurbanized ones. The variables most highly correlated with Social Distancing Compliance—High Educational Attainment and Internet Subscribers—were the same for both groups, but the correlations were substantially stronger in the urbanized counties (r = 0.68 and 0.51, respectively) compared to the nonurbanized counties (r = 0.27 and 0.20). Among the urbanized counties, Non‐White Population (r = 0.20), Stay at Home (r = 0.19), and Republican Dominance (r = 0.10), were also positively and significantly correlated with Social Distancing Compliance, and Older Population (r = −0.14), Lower Income (r = −0.45), and Sales Tax (r = −0.14) were inversely statistically correlated with higher social distancing compliance. Among the nonurbanized counties, Unemployment (r = 0.08) and Stay at Home (r = 0.08), were also positively statistically correlated with Social Distancing Compliance, and Sales Tax (r = −0.15), Non‐White Population (r = −0.05), and Lower Income (r = −0.13) were negatively statistically correlated with improved social distancing compliance.
Among the most highly correlated variables with subsequent Change in Cases is Deaths measured at the end of April, both among urbanized and nonurbanized counties. Change in Cases represents the change in weekly total number of cases per 1000 residents from May 22 to 29. Deaths is the total number of deaths per 1000 residents as of April 24. The correlation here suggests that counties with higher deaths in late April continued to be places of higher risk and higher case counts weeks later. Non‐White Population and Essential Workers were also both positively associated with Change in Cases for both county groups. Older Population was inversely statistically correlated with Change in Cases for both county groups. The inverse correlation may seem surprising, given the considerable reporting on how the elderly are particularly vulnerable to COVID‐19. People age 60 and over make up more than 80% of deaths and a disproportionate share of hospitalizations, but they make up less than half of all cases (CDC, 2020b).
Impact of predictor variables on social distancing compliance mediator
Table 3 provides the standardized regression weights for our path analyses. The regression weights represent the relationships between the predictors and mediator variable (Social Distancing Compliance) and the predictors and dependent variable (Change in Cases), as well as the relationship between mediator and dependent variables. The standardized regression weights are presented for urbanized and nonurbanized counties.
Table 3.
Standardized regression weights
| Parameter | Urbanized counties | Nonurbanized counties | ||||
|---|---|---|---|---|---|---|
| Model 1: May 1–8 | Model 2: May 22–29 | Model 1: May 1–8 | Model 2: May 22–29 | |||
| Social distancing | ← | DEATHS | 0.14** | 0.14** | −0.01 | −0.01 |
| Social distancing | ← | NON‐WHITE | 0.09** | 0.09** | −0.02 | −0.02 |
| Social distancing | ← | OLD POP | 0.08** | 0.08** | −0.03 | −0.03 |
| Social distancing | ← | HIGH EDU | 0.68** | 0.68** | 0.27** | 0.27** |
| Social distancing | ← | USE INT | 0.13** | 0.13** | 0.07 | 0.07 |
| Social distancing | ← | ESSENTIAL | …. | …. | −0.01 | −0.01 |
| Social distancing | ← | LESS60K | 0.16** | 0.16** | 0.09** | 0.09** |
| Social distancing | ← | UEMP | 0.01 | 0.01 | 0.09** | 0.09** |
| Social distancing | ← | REPUBLICAN | 0.01 | 0.01 | −0.01 | −0.01 |
| Social distancing | ← | STAY HOME | 0.11** | 0.11** | 0.04 | 0.04 |
| Social distancing | ← | S TAX | 0.05* | 0.05* | −0.06* | −0.06* |
| Dependent variable | Model 1: May 1–8 | Model 2: May 22–29 | Model 1: May 1–8 | Model 2: May 22–29 | ||
|---|---|---|---|---|---|---|
| Change in cases | ← | DEATHS | 0.31** | 0.20** | 0.26** | 0.18** |
| Change in cases | ← | NON‐WHITE | 0.24** | 0.31** | 0.17** | 0.21** |
| Change in cases | ← | OLD POP | −0.12** | −0.14** | −0.18** | −0.20** |
| Change in cases | ← | HIGH EDU | …. | 0.07 | −0.04 | −0.03 |
| Change in cases | ← | USE INT | −0.02 | 0.01 | −0.01 | −0.05 |
| Change in cases | ← | ESSENTIAL | 0.22** | 0.21** | 0.12** | 0.15** |
| Change in cases | ← | LESS60K | −0.23** | −0.16** | −0.09** | −0.04 |
| Change in cases | ← | UEMP | −0.06* | −0.05 | 0.04 | 0.05* |
| Change in cases | ← | REPUBLICAN | 0.07** | 0.05 | 0.05* | 0.04* |
| Change in cases | ← | STAY HOME | 0.05* | 0.02 | 0.03 | …. |
| Change in cases | ← | SD | 0.18** | 0.14** | 0.01 | 0.02 |
*p < 0.05.
**p < 0.01.
As described above, urbanized counties generally were more likely to be at higher risk to be impacted by COVID‐19 during the time of the study. The standardized regression weights indicate that the predictor variables associated with Protection Motivation were strongly related to Social Distancing Compliance in urbanized counties. All predictor variables were statistically significant in the expected direction: Deaths (0.14**), Non‐White Population (0.09**), Older Population (0.08**), High Educational Attainment (0.68**), and Internet Subscribers (0.13**). The standardized regression weights for nonurbanized counties showed a different pattern. Of the predictors associated with Protection Motivation, only High Educational Attainment (0.27**) was statistically associated with Social Distancing Compliance. This could be interpreted to mean that education increases self‐efficacy, the belief that engaging in the required behavior will result in a good outcome.
In the conceptual model, Economic Motivation was identified as having mixed effects on Social Distancing Compliance. The results of the model for urbanized counties showed that the only predictor that was statistically significantly related to Social Distancing Compliance was the proportion of Lower Income households (0.11**). This predictor was positively related to the mediator. Urbanized counties with a higher proportion of Lower Income households had greater Social Distancing Compliance. This could be because, at the time of data collection (April 24, 2020), many businesses were closed, thereby reducing the daily travel needs of workers, particularly those in low‐wage jobs in the retail, restaurant, and personal care industries.
As with urbanized counties, nonurbanized counties also showed a statistically significant positive relationship between the proportion of Lower Income households (0.09**) and Social Distancing Compliance. In addition, there was a statistically significant positive relationship between the state level of Unemployment (0.09**) and Social Distancing Compliance. This confirms our expectation that higher levels of unemployment are associated with less travel.
In the conceptual model, we expected that Government Context would have an impact on Social Distancing Compliance due to government influence on perceived risk from COVID‐19. For urbanized counties, there was a positive and statistically significant relationship for two of the three predictor variables. Contrary to previous research, political preference had no statistical relationship to Social Distancing Compliance. However, the length of Stay at Home (0.11**) orders was statistically and positively associated with Social Distancing Compliance. In addition, greater reliance on Sales Tax (0.05*) was statistically and positively associated with Social Distancing Compliance in urbanized counties. Both results were inconsistent with expectations based on earlier research findings.
As with urbanized counties, there was no relationship between political preference and the mediator among nonurbanized counties. However, unlike urbanized counties, there was also no statistically significant relationship between the length of the Stay at Home order and the mediator among nonurbanized counties, but there was a statistically significant inverse relationship with Sales Tax (−0.06*). Nonurbanized counties in states with greater reliance on Sales Tax as a revenue source had lower levels of Social Distancing Compliance.
Path analysis: Predictor and mediator impact on subsequent changes in cases
Though research predicting social distancing compliance and research showing the relationship between SD and infection spread represent separate streams, in our study, we join those streams and examine the mediation of Social Distancing Compliance on Change in Cases in a subsequent time period.
Direct effects on change in cases
The test for mediation is a robust test in that it must show significance after the impact of the predictor variables on the dependent variable is accounted for. For both types of counties, there were expected statistically significant relationships between protection motivation variables and the dependent variable, Changes in Cases, suggesting that risk from COVID‐19 was rational and protection motivation was valid. For both urbanized and nonurbanized counties, Deaths, Non‐White Population, and Essential Workers variables were associated with increases in weekly COVID‐19 case counts. For both urbanized and nonurbanized counties, the variable Older Population was negatively associated with increased case count.
For urbanized counties, Lower Income was inversely associated with Change in Cases, but there was no statistically significant relationship in nonurbanized counties. Republican Dominance was statistically related to an increase in cases for nonurbanized counties only. This suggests that political considerations may have influenced the protection motivation messaging and changed the perception of risk for individuals living in Republican‐dominated, nonurban areas.
Unemployment was not related to Change in Cases in the urbanized counties, but in nonurbanized counties, the variable was positively associated with Change in Cases. The length of Stay at Home orders was not statistically associated with Change in Cases.
Test of mediation
Public health research suggests that social distancing compliance would reduce subsequent COVID‐19 case count. We examined this relationship in both urbanized and nonurbanized counties during the period of the study. For nonurbanized counties, there was no statistically significant relationship between Social Distancing Compliance and Change in Cases. For urbanized counties, the results of the study showed Social Distancing Compliance was associated with increases in Change in Cases. This unexpected finding is contrary to existing medical research on the efficacy of isolation in reducing disease spread.
Testing overall model fit
Table 4 shows the results of our path analyses, including the direct, indirect, and total effects of the predictors and mediator on the dependent variable in the urbanized and nonurbanized counties.5 As can be seen in Table 4, our model was robust for both county groups, despite the distinct differences in results. Goodness‐of‐fit measures were well within desirable thresholds of RMSEA of less than 0.08 and CFI, GFI, NNFI, and AGFI of >0.90. Table 4 makes clear that our collection of predictor variables representing our three constructs helps explain differences, in varying degree, in social distancing compliance. The path analyses also show how predictor variables impact changes in COVID‐19 case counts across both urbanized and nonurbanized counties. Yet, the results call into question the mediating effect of SD. The indirect effect shown in Table 4 is the indicator of mediation. Social Distancing Compliance as mediator, evident in the indirect effects of the predictor variables, was small. Only in well‐educated urbanized counties did Social Distancing Compliance substantially mediate the predictor variable's effect on COVID‐19 case counts, but in the opposite direction expected.
Table 4.
Direct, indirect, and total effects
| Urbanized | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Effects | Variables | Protection motivation | Economic motivation | Government context | ||||||||||
| DEATHS | NON‐WHITE | OLD POP | HIGH EDU | USE INT | ESSENTIAL | LESS60K | UEMP | REPUBLICAN | STAY HOME | S TAX | SD | |||
| Model 1: May 1–8 | Total | Social distancing compliance | 0.14** | 0.09** | 0.08** | 0.68** | 0.13** | 0.00 | 0.16** | 0.01 | 0.01 | 0.11** | 0.05* | 0.00 |
| Direct | 0.14** | 0.09** | 0.08** | 0.68** | 0.13** | 0.00 | 0.16** | 0.01 | 0.01 | 0.11** | 0.05* | 0.00 | ||
| Indirect | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Total | Change in cases | 0.34** | 0.25** | −0.10** | 0.12** | 0.01 | 0.22** | −0.20** | −0.06 | 0.07** | 0.07** | 0.01* | 0.18** | |
| Direct | 0.31** | 0.24** | −0.12** | 0.00 | −0.02 | 0.22** | −0.23** | −0.06 | 0.07** | 0.05 | 0.00 | 0.18** | ||
| Indirect | 0.03** | 0.02** | 0.01* | 0.12** | 0.02** | 0.00 | 0.03** | 0.00 | 0.00 | 0.02** | 0.01* | 0.00 | ||
| Model 2: May 22–29 | Total | Social distancing compliance | 0.14** | 0.09** | 0.08** | 0.68** | 0.13** | 0.00 | 0.16** | 0.01 | 0.01 | 0.11** | 0.05* | 0.00 |
| Direct | 0.14** | 0.09** | 0.08** | 0.68** | 0.13** | 0.00 | 0.16** | 0.01 | 0.01 | 0.11** | 0.05* | 0.00 | ||
| Indirect | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Total | Change in cases | 0.22** | 0.32** | −0.12** | 0.16** | 0.03 | 0.21 | −0.14** | −0.04 | 0.05 | 0.03 | 0.01* | 0.14** | |
| Direct | 0.20** | 0.31** | −0.14** | 0.07 | 0.01 | 0.21 | −0.16** | −0.05 | 0.05 | 0.02 | 0.00 | 0.14** | ||
| Indirect | 0.02** | 0.01** | 0.01* | 0.09** | 0.02** | 0.00 | 0.02** | 0.00 | 0.00 | 0.02** | 0.01* | 0.00 | ||
| Model 1 Fit: χ 2 = 3.354/Probability level = 0.067/CFI = 0.999, GFI = 0.999, NFI = 0.999, RFI = 0.942, AGFI = 0.951, RMSEA = 0.050 | ||||||||||||||
| Model 2 Fit: χ 2 = 5.776/Probability level = 0.016/CFI = 0.999, GFI = 0.999, NFI = 0.999, RFI = 0.899, AGFI = 0.915, RMSEA = 0.071 | ||||||||||||||
| Nonurbanized | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Effects | Variables | Protection motivation | Economic motivation | Government context | ||||||||||
| DEATHS | NON‐WHITE | OLD POP | HIGH EDU | USE INT | ESSENTIAL | LESS60K | UEMP | REPUBLICAN | STAY HOME | S TAX | SD | |||
| Model 1: May 1–8 | Total | Social distancing compliance | −0.01 | −0.02 | −0.03 | 0.27** | 0.07 | −0.01 | 0.09** | 0.09 | −0.01 | 0.04 | −0.06 | 0.00 |
| Direct | −0.01 | −0.02 | −0.03 | 0.27** | 0.07 | −0.01 | 0.09** | 0.09 | −0.01 | 0.04 | −0.06 | 0.00 | ||
| Indirect | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Total | Change in cases | 0.26** | 0.17** | −0.18** | −0.04 | −0.01 | 0.12** | −0.09** | 0.04 | 0.05 | 0.03 | 0.00 | 0.01 | |
| Direct | 0.26** | 0.17** | −0.18** | −0.04 | −0.01 | 0.12** | −0.09** | 0.04 | 0.05 | 0.03 | 0.00 | 0.01 | ||
| Indirect | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Model 2: May 22–29 | Total | Social distancing compliance | −0.01 | −0.02 | −0.03 | 0.27** | 0.07 | −0.01 | 0.09 | 0.09 | −0.01 | 0.04 | −0.06 | 0.00 |
| Direct | −0.01 | −0.02 | −0.03 | 0.27** | 0.07 | −0.01 | 0.09 | 0.09 | −0.01 | 0.04 | −0.06 | 0.00 | ||
| Indirect | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Total | Change in cases | 0.18** | 0.21** | −0.20** | −0.03 | −0.05 | 0.15** | −0.04 | 0.05 | 0.04 | 0.00 | 0.00 | 0.02 | |
| Direct | 0.18** | 0.21** | −0.20** | −0.03 | −0.05 | 0.15** | −0.04 | 0.05 | 0.04 | 0.00 | 0.00 | 0.02 | ||
| Indirect | 0.00 | 0.00 | 0.00 | 0.01 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| Model 1 Fit: χ 2 = 4.876/Probability level = 0.027/CFI = 0.999, GFI = 1.000, NFI = 0.999, RFI = 0.936, AGFI = 0.968, RMSEA = 0.043 | ||||||||||||||
| Model 2 Fit: χ 2 = 0.680/Probability level = 0.410/CFI = 1.000, GFI = 1.000, NFI = 1.000, RFI = 0.991, AGFI = 0.995, RMSEA = 0.000 | ||||||||||||||
*p < 0.05.
**p < 0.01.
DISCUSSION AND CONCLUSIONS
To summarize, our study suggests the following important conclusions. First, there were clear differences in social distancing compliance for the two types of counties. There were different patterns of response in terms of protection motivation, economic motivation, and government context. Second, an interesting, yet unexpected, finding was that social distancing csocial distancing compliance was not associated with reduced case count. In urban counties, where more COVID‐19 cases were reported at the time of the study, the relationship was the opposite to what was expected. The results of this test for the mediating impact of social distancing compliance has, we believe, important implications for understanding the community response to the COVID‐19 pandemic.
Medically, the benefit of quarantine to limit the spread of pathogens and reduce cases is well‐supported in research and practice. However, while quarantine limits cases and disease spread from a biological perspective, the term “social distance” implies a collective or collaborative social response that may require a sociological or social‐psychological perspective. This study set out to understand how community characteristics and concerns impact compliance with SD recommendations and orders and then test the logical conclusion that greater compliance with SD reduces subsequent case count.
Our findings showed that each component of the model did influence compliance with SD orders and recommendations to some degree. However, even when data showed an social distancing compliance response consistent with protection motivation, the community social distancing compliance was not related to reduced subsequent case count. As noted above, our SD measure is only significantly associated with case counts among urbanized counties, and the relationship is positive, suggesting greater SD was occurring at the same time as increased case counts. This disconnect found by the model underscores a possible difference between the medical approach to reducing disease and the public health approach to keeping communities safe. Social distance implies a communal response, not just an individual one.
Sundwall (2019) cited U.S. government research reporting that from an epidemiological perspective, 90% compliance with nonpharmaceutical interventions was the level needed to reduce spread of infection. The Unacast Scorecard defined a high level of community compliance as a 70% or better reduction in travel compared to the same period in 2019. Based on the reported data, very few U.S. counties approached that level of compliance. Of the urbanized counties, none met the threshold of a high level of compliance, as defined by Unacast. Among the nonurbanized counties, only 2.6% met that threshold. Across all counties, only 22% achieved an average 55% reduction in distance traveled compared to 2019. Though SD did occur, it was not widespread nor embraced. The possibility exists that stay‐at‐home orders adopted across the United States were not stringent enough nor enforced enough to break “transmission chains” of the disease. Chinese medical experts described lockdown measures in Lombardy, Italy, for example, as not strict enough (Braithwaite & Ruotolo, 2020). In fact, New York Times science and health reporter Donald G. McNeil Jr. described U.S. stay‐at‐home restrictions as a “giant garden party” (McNeil Jr., 2020).
In March and April, COVID‐19 was affecting urbanized and nonurbanized areas quite differently, and this may explain differences in our findings for these two groups. At the time of data collection for this analysis, the virus outbreak in the United States was largely confined to major cities. PMT posits that people will comply with nonpharmaceutical recommendations and mandates that serve to reduce threats to their own health. Evidence from our study suggests that communities with vulnerable populations did respond to public health recommendations to isolate themselves to protect their health. However, fewer local death counts, combined with a comfortable distance from the hard‐hit cities, may have reduced collective perception of risk in nonurbanized counties. Threats to personal health are weighed against other risks to well‐being. In counties where the virus was not impacting death rates or hospitalizations, residents may have weighed the evidence at hand and determined that the economic impact from stay‐at‐home orders designed to slow the spread of the virus provided greater risk to their well‐being than risk of infection. This study demonstrates the public health messaging challenge of failing to account for context at the community level of analysis in this unique health‐care crisis.
In addition to differences in the community presence of COVID‐19, public health messaging may have influenced the results. Generic public health messaging around nonpharmaceutical interventions, whether stay‐at‐home orders or mask mandates, may have influenced local community compliance. Residents were repeatedly told that stay‐at‐home mandates were needed to “flatten the curve” and protect health systems from being overwhelmed. This approach to public health messaging is inconsistent with the traditional public health protection motivation approach. PMT posits that individuals are moved to comply with public health measures based on their own personal health risks. PMT provides little guidance on compliance with public health recommendations and benefits when the risks are not presented at the individual level, but at the system or societal level.
In summary, differences between urban and nonurbanized counties highlight the importance of tailoring community public health messaging to align with the realities of place. Public health messaging built on health risks to the individual is insufficient to motivate substantial numbers of the community to act for the benefit of systems and society, especially when personal risks seem at odds. Reason (2000) observed that traditional medicine assumes that people are free agents capable of choosing between safe and unsafe modes of behavior. However, Reason's “Swiss Cheese Model” argues that in complex systems there is a place for both individual and societal action. Reason (2000) believed that putting the greatest emphasis on individual response to a crisis in a complex system was doomed to fail. Public health response to COVID‐19 has relied on PMT to offset inadequate systemic responses to the pandemic. Pandemic response has exposed deficiencies in the U.S. health care system in the areas of testing, contact tracing, protections for health‐care workers, hospital capacity, and crisis staffing. (Blumenthal et al., 2020; Sha et al., 2020; Slavitt, 2020). The pandemic has also underscored structural issues of health care access, racial inequities, and rural deprivation (Blumenthal et al., 2020; Sha et al., 2020; Slavitt, 2020). As Reason posited, individual community members’ compliance with SD recommendations was inadequate to overcome such broad systemic deficiencies, as evidenced by the observed lack of reduction in case counts.
Kyne and Aldrich (2020) make a case for community as the unit in which personal connections, government trust, and social capital are most likely to facilitate resilience in the face of disaster. Adequate and equitable public health systems and social safety nets, as described by Reason (2000), contribute to the government trust critical for individual compliance in the face of public health crisis. The authors’ concrete method for measuring the social capital influencing disaster recovery could be useful in crafting policies that encourage better compliance and outcomes by broadening and personalizing individual protection motivation to include the communities where people live and work.
LIMITATIONS OF THE STUDY
As noted earlier, our SD measure, change on average daily distance traveled, may not adequately capture SD.6 The data being collected by technology firms and shared purportedly for the good of public health may be less useful than expected in helping government agencies and health organizations anticipate and craft initiatives to stop the spread of disease. Our findings are also limited by the challenge of accessing relevant data at the speed and level necessary for understanding a rapidly unfolding pandemic. There is frequently a significant delay in availability of county‐level data from government sources; subcounty data, which presumably is even more helpful in mapping disease outbreaks and responses, is reported even later, if at all. Timing may be another reason for caution in interpreting findings. The date we used as a baseline for SD, death counts, and stay‐at‐home durations (April 24) was dependent on data available at the time we commenced this study; the time frame used for change in case counts sought to capture the time between onset of disease and desire to seek treatment and testing. However, these dates may not have aligned well with the actual transmission timeline of the virus. During, and subsequent to, the case count time period in May, stay‐at‐home orders were lifted, thus closing the window on additional evaluation of such SD mandates and providing residents less reason to continue to comply.
Finally, the fragmented nature of the U.S. public health system means that there is frequently a delay in reporting deaths and positive test results. It is not uncommon for counties and states to report deaths and positive test results days or even weeks after the fact. At the time of this study, states were also increasing the availability of testing, which could have the effect of increasing case counts by capturing mild cases of the disease that previously went unreported.
POLICY IMPLICATIONS
Despite these limitations, the research does offer useful insights for public health officials and policymakers across all levels of government:
-
1.
Protection motivation is potentially a powerful tool to influence individual behavior in the face of a health hazard. In urban areas, there was support for the idea that fear of infection is associated with acceptance of nonpharmaceutical interventions. This insight may be useful to motivate citizens to adopt other nonpharmaceutical interventions to reduce risk beyond self‐isolation, such as masks. If people believe that they are at risk, they do seem willing to cooperate with nonpharmaceutical interventions.
-
2.
Though PMT is supported, there is also evidence to suggest that clearer communication of the nature of the threat is warranted. Unlike other pandemics, there is substantial variance regarding the seriousness of the infection. COVID‐19 has been shown to be a disease with wide differences in severity depending on age, ethnicity, and comorbidity. Thus, for subgroups with low probability of having a severe impact, individual protection motivation is lower.
-
3.
Public health messaging at the time of this study greatly emphasized individual protection. Protection motivation beyond the individual, more clearly articulating the relationship between community threat and personal interest, is warranted. Linkages between community impact and second‐order impact (i.e., jobs, economic welfare, hospital capacity) on “nonthreatened” individuals is a more complex but necessary public health message.
-
4.
In addition to public health reliance on individual choice and behavior, greater emphasis on building institutional capabilities and capacities for responding to a pandemic crisis is needed. While the United States has been subject to threat of pandemic from SARS, H1N1 flu, and Ebola, none of those events prompted investment in scaling up response capacity, particularly at the state and local levels.
-
5.
Government bodies at all levels have an important role in providing consistent information and messaging regarding facts about recognizing, avoiding, and treating COVID‐19. Clear, reliable information is key to developing the appropriate protection motivation. Confidence in nonpharmaceutical interventions will increase the self‐efficacy and response efficacy needed for compliance with public health initiatives. Boin et al. (2020) underscore the particular challenge a “creeping crisis” like COVID‐19 presents to trust in public institutions and, thus, compliance with their mandates and recommendations. A further compliance complication of COVID‐19 is that, unlike other recent pandemics, subpopulations appear to have very different risk profiles. This adds to confusion regarding threat assessment and reduces across‐the‐board compliance with nonpharmaceutical interventions.
-
6.
Health agencies at all levels of government must find effective paths to communicate information about dangers and protection measures to vulnerable populations with the objective of increasing protection motivation. This may require creativity. The elderly and non‐White communities are both likely to suffer disproportionately from COVID‐19, but they are populations that may also have less access to informational websites or even online grocery ordering. These populations may have been much more likely to rely on community institutions, such as churches, local libraries, and senior centers, to gain vital information. However, many of these institutions were closed under stay‐at‐home orders, cutting off an important avenue of information. Research on social compliance (Duck et al., 2000) suggests that the persuasive impact of messaging is enhanced when using icons and organizations with whom the target audience is highly identified. Cuomo et al. (2020) and Odiase et al. (2020) suggest the importance of harnessing the power of local religious institutions and racial, ethnic, and cultural bonds in crisis response.
Public health officials and elected political leaders, in the United States and countries around the world, have struggled to contain the spread and havoc of the novel coronavirus. With no cure or widely available vaccine and few treatments offering demonstrable effect, governments have relied heavily on nonpharmaceutical interventions. Our research provides empirical support for PMT's value in motivating individual responses to pandemic disease. Individuals will react to protect themselves and those they care about. However, COVID‐19 shows the limitations of that approach. Policymakers must be mindful that a crisis of the magnitude of COVID‐19 may require response and message framing at more than one level of analysis. In addition, policy initiatives to provide systemic response and reinforcement of health‐care infrastructure will be necessary to bring the current crisis to a close and build capacity for effective response to future threats.
Biographies
Minkyu Yeom, PhD., is a research scholar in Maxine Goodman Levin College of Urban Affairs at the Cleveland State University, Ohio. He teaches Geographical information system certificate courses for undergraduate and graduate students.
Fran Stewart, is Senior Research Associate at The Ohio State University s John Glenn College of Public Affairs and the Ohio Manufacturing Institute. Stewart is the author of The STEM Dilemma: Skills that Matter to Regions (W.E. Upjohn Institute for Employment Research, 2017).
Alice Stewart, Strategic Management, Haslam College of Business, University of Tennessee, Knoxville, TN 37996.
INDUSTRIES AND SECTORS MAKING UP “ESSENTIAL WORKERS” VARIABLE*
| NAICS code | Industry or sector |
|---|---|
| 11 | Agriculture, forestry, fishing and hunting |
| 221 | Utilities |
| 311 | Food manufacturing |
| 3222 | Converted paper product manufacturing |
| 3252 | Resin, rubber, and artificial fibers manufacturing |
| 3254 | Pharmaceutical and medicine manufacturing |
| 3256 | Soap, cleaning compound, and toiletry manufacturing |
| 3261 | Plastics product manufacturing |
| 33324 | Industrial machinery manufacturing |
| 3391 | Medical equipment and supplies manufacturing |
| 4241 | Paper and paper product merchant wholesalers |
| 4242 | Druggists' goods merchant wholesalers |
| 4244 | Grocery and related product wholesalers |
| 42345 | Medical equipment merchant wholesalers |
| 4245 | Farm product raw material merchant wholesalers |
| 4451 | Grocery stores |
| 44611 | Pharmacies and drug stores |
| 4471 | Gasoline stations |
| 452 | General merchandise stores |
| 4541 | Electronic shopping and mail‐order houses |
| 48‐49 | Transportation and warehousing |
| 562 | Waste management and remediation services |
| 62 | Health care and social assistance |
| 722513 | Limited‐service restaurants |
*Data was unavailable for NAICS 9221, Justice, Public Order and Safety.
Source: U.S. Bureau of Labor Statistics, Quarterly Census of Employment and Wages.
Yeom, Minkyu , Stewart Fran, and Stewart Alice. “The Impact of Social Distancing on Community Case Count in The United States: Testing The Efficacy of Protection Motivation Theory During Early Stages of The Covid‐19 Pandemic.” Risks Hazards Crisis Public Policy. 2021;12:303–327. 10.1002/rhc3.12232
ENDNOTES
Unacast, which was founded in Norway, purports to adhere to General Data Protection Regulation and California Consumer Privacy Act guidelines for its Scorecard research for the entirety of the United States. It describes its process as capturing data from millions of anonymized cell phones and their interactions with others each day and extrapolating to the larger population level.
We chose the time frame for our study purposefully. We gave careful consideration to the length of time between exposure and onset of disease, as well as challenges regarding testing availability, accuracy, and reporting. However, we were also loath to extend the study period beyond the end of May. By late May, nearly all states had allowed stay‐at‐home orders to expire. There also was the added consideration of the effects of summer's warm weather and outdoor activities on spread of the disease. This continues to be a topic of debate, as colder weather across much of the United States during the winter months has been considered a factor in increases in cases, hospitalizations, and deaths.
In a prior version of this study, we explored using a study time frame closer to the generally accepted two‐week incubation period. Specifically, we examined the change in confirmed COVID‐19 case counts from May 1 to 8, as well as from May 22 to 29. The findings were relatively similar in terms of the statistical significance of the variables and in their direction. Therefore, for this final version of the article, we opted to include findings from only one time period, May 22 to 29, to avoid redundancy and unnecessary complication of the discussion, as well as for space considerations.
For two states without official statewide mandates, we included locally enacted orders.
The total effect was calculated multiplying the path coefficient of independent variable “A” to mediator “B” by the path coefficient of mediator “B” to dependent variable “C,” and then adding the path coefficient from “A” to “C.” The total effect is indirect effect plus direct effect. The direct effect value is the path coefficient from “A” to “B,” from “A” to “C,” or from “B” to “C.” The direct effect is a single measurement between an independent, a mediator, and a dependent variable. The indirect effect value is calculated by multiplying the path coefficients from “A” to “B” and from “B” to “C.” The indirect effect factors path coefficients from an independent to a dependent variable via a mediator.
At the time of our study, social distancing, along with good hand hygiene, were the primary nonpharmaceutical interventions encouraged by public health officials. In a working paper, we use a model similar to the one presented here in our test of PMT to explore the effects of mask wearing and mask mandates on disease spread later in the summer.
REFERENCES
- Abouk, Rahi , and Heydari Babak. 2020. “The Immediate Effect of COVID‐19 Policies on Social Distancing Behavior in the United States.” SSRN Scholarly Paper ID 3571421. Social Science Research Network. 10.2139/ssrn.3571421 [DOI] [PMC free article] [PubMed]
- Andersen, Martin . 2020. “Early Evidence on Social Distancing in Response to COVID‐19 in the United States.” SSRN Scholarly Paper ID 3569368. Social Science Research Network. 10.2139/ssrn.3569368 [DOI]
- Baum, Nancy M. , Jacobson Peter D., and Goold Susan D.. 2009. “‘Listen to the People’: Public Deliberation about Social Distancing Measures in a Pandemic.” The American Journal of Bioethics 9(11): 4–14. 10.1080/15265160903197531 [DOI] [PubMed] [Google Scholar]
- Béland, Louis‐Philippe , Brodeur Abel, and Wright Taylor. 2020. “The Short‐Term Economic Consequences of COVID‐19: Exposure to Disease, Remote Work and Government Response.” “SSRN Scholarly Paper ID 3584922.” Social Science Research Network. https://papers.ssrn.com/abstract=3584922 [DOI] [PMC free article] [PubMed]
- Bell, David , Fukuda Keiji, Horby Peter, Monto Arnold, Hayden Frederick, Wylks Clare, Sanders Lance, and Van Tam Jonathan. 2006. “Non‐Pharmaceutical Interventions for Pandemic Influenza, International Measures.” Emerging Infectious Diseases 12(1): 81–87. 10.3201/eid1201.051370 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bhattacharyya, Samit , and Reluga Timothy. 2019. “Game Dynamic Model of Social Distancing While Cost of Infection Varies with Epidemic Burden.” IMA Journal of Applied Mathematics 84(1): 23–43. 10.1093/imamat/hxy047 [DOI] [Google Scholar]
- Blumenthal, David , Fowler Elizabeth J., Abrams Melinda, and Collins Sara R.. 2020. “COVID‐19—Implications for the Health Care System.” The New England Journal of Medicine 383(17): 1698. https://www.nejm.org/doi/full/10.1056/nejmsb2021088 [DOI] [PubMed] [Google Scholar]
- Boin, Arjen , Ekengren Magnus, and Rhinard Mark. 2020. “Hiding in Plain Sight: Conceptualizing the Creeping Crisis.” Risks, Hazards & Crisis in Public Policy 11(2): 116–138. 10.1002/rhc3.12193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Braithwaite, S. , and Ruotolo N.. 2020. “March 19 Coronavirus News.” CNN, March 19, 2020. https://www.cnn.com/world/liver--news/coronavirus-outbreak-03-19-20-intl-hnk/index.html
- Cava, Maureen A. , Krissa E Fay., Heather J Beanlands., Elizabeth A McCay., and Rouleen Wignall. 2005. “Risk Perception and Compliance with Quarantine During the SARS Outbreak.” Journal of Nursing Scholarship 37(4): 343–347. 10.1111/j.1547-5069.2005.00059.x [DOI] [PubMed] [Google Scholar]
- CDC . 2020a. “Coronavirus Disease 2019 (COVID‐19).” Centers for Disease Control and Prevention. April 20, 2020. https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/index.html
- CDC . 2020b. “Demographic Trends of COVID‐19 Cases and Deaths in the US Reported to CDC.” June 29, 2020. https://www.cdc.gov/covid-data-tracker/#demographics
- Cuomo, Raphael E. , Davis Daniel B., Goetz Stephan J., Shapiro Josh D., and Walshok Mary L.. 2020. “Religiosity and Regional Resilience to Recession.” Risks, Hazards & Crisis in Public Policy 11(2): 166–187. 10.1002/rhc3.12189 [DOI] [Google Scholar]
- Desclaux, Alice , Badji Dioumel, Ndione Albert Gautier, and Sow Khoudia. 2017. “Accepted Monitoring or Endured Quarantine? Ebola Contacts' Perceptions in Senegal.” Social Science & Medicine (1982) 178: 38–45. 10.1016/j.socscimed.2017.02.009 [DOI] [PubMed] [Google Scholar]
- Duck, Julie M. , Hogg Michael A., and Terry Deborah J.. 2000. “The Perceived Impact of Persuasive Messages on ‘Us’ and ‘Them’.” In Attitudes, Behavior, and Social Context: The Role of Norms and Group Membership, edited by Terry Deborah J. and Hogg Michael A., 265–291. New York: Lawrence Erlbaum Associates Publishers. [Google Scholar]
- ESRI . 2020. “COVID‐19 Resources.” https://coronavirus-disasterresponse.hub.arcgis.com/
- Ferguson, Neil M. , Laydon Daniel, Nedjati Gilani Gemma, Imai Natsuko, Ainslie Kylie, Baguelin Marc, and Bhatia Sangeeta, et al. 2020. “Report 9: Impact of Non‐Pharmaceutical Interventions (NPIs) to Reduce COVID19 Mortality and Healthcare Demand.” Imperial College London. 10.25561/77482 [DOI]
- Gensini, Gian Franco , Yacoub Magdi H., and Conti Andrea A.. 2004. “The Concept of Quarantine in History: From Plague to SARS.” The Journal of Infection 49(4): 257–261. 10.1016/j.jinf.2004.03.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenstone, Michael , and Nigam Vishan. 2020. “Does Social Distancing Matter?“ SSRN Scholarly Paper ID 3561244. Social Science Research Network. 10.2139/ssrn.3561244 [DOI]
- Jefferson, Tom , Del Mar Chris B., Dooley Liz, Ferroni Eliana, Al‐Ansary Lubna A., Bawazeer Ghada A., van Driel Mieke L., et al. 2011. “Physical Interventions to Interrupt or Reduce the Spread of Respiratory Viruses.” The Cochrane Database of Systematic Reviews 2011(7), CD006207. 10.1002/14651858.CD006207.pub4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knittel, Christopher R. , and Ozaltun Bora. 2020. “What Does and Does not Correlate with COVID‐19 Death Rates.” Working Paper No. 27391; Working Paper Series. National Bureau of Economic Research. 10.3386/w27391 [DOI]
- Kushner Gadarian, Shana , Goodman Sara Wallace, and Pepinsky Thomas B.. 2020. “Partisanship, Health Behavior, and Policy Attitudes in the Early Stages of the COVID‐19 Pandemic.” SSRN Scholarly Paper ID 3562796. Social Science Research Network. 10.2139/ssrn.3562796 [DOI] [PMC free article] [PubMed]
- Kyne, Dean , and Aldrich Daniel P.. 2020. “Capturing Bonding, Bridging, and Linking Social Capital Through Publicly Available Data.” Risk, Hazards & Crisis in Public Policy 11(2): 61–86. 10.1002/rhc3.12183 [DOI] [Google Scholar]
- Lauer, Stephen A. , Grantz Kyra H., Bi Qifang, Jones Forrest K., Zheng Qulu, Meredith Hannah R., Azman Andrew S., Reich Nicholas G., and Lessler Justin. 2020. “The Incubation Period of Coronavirus Disease 2019 (COVID‐19) from Publicly Reported Confirmed Cases: Estimation and Application.” Annals of Internal Medicine 172: 577–582. 10.7326/M20-0504 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maddux, James E. , and Rogers Ronald W.. 1983. “Protection Motivation and Self‐efficacy: A Revised Theory of Fear Appeals and Attitude Change.” Journal of Experimental Social Psychology 19(5): 469–479. 10.1016/0022-1031(83)90023-9 [DOI] [Google Scholar]
- McNeil Jr., Donald G. 2020. “Compared with China, U.S. Stay‐at‐Home Has Been ‘Giant Garden Party,’ journalist says.” NPR.Org, April 29, 2020. https://www.npr.org/sections/health-shots/2020/04/29/847755751/compared-to-china-u-s-stay-at-home-has-been-a-giant-garden-party-journalist-says
- Mervosh, Sarah , Lu Denise, and Swales Vanessa. 2020. “See Which States and Cities have Told Residents to Stay at Home.” The New York Times. https://www.nytimes.com/interactive/2020/us/coronavirus-stay-at-home-order.html
- MIT Election Data and Science Lab . 2019. “County Presidential Election Returns 2000‐2016 [Data set].” Harvard Dataverse. 10.7910/DVN/VOQCHQ [DOI]
- Morrison, Sara . 2020. “Like it or Not, Tech Companies Can Use Your Phone Location Data to Map Social Distancing.” Vox, March 26, 2020. https://www.vox.com/recode/2020/3/26/21192653/coronavirus-privacy-social-distancing-data-collection-unacast
- Odiase, Osamuede , Wilkinson Suzanne, and Neef Andreas. 2020. “Disaster Risk and the Prospect of Enhancing the Resilience of the African Community in Auckland.” Risks, Hazards & Crisis in Public Policy 11(2): 188–203. 10.1002/rhc3.12190 [DOI] [Google Scholar]
- Painter, Marcus O. , and Qiu Tian. 2020. “Political Beliefs Affect Compliance with COVID‐19 Social Distancing Orders.” SSRN Scholarly Paper ID 3569098. Social Science Research Network. 10.2139/ssrn.3569098 [DOI]
- Reason, James . 2000. “Human error: models and management.” BMJ 320(7237): 768–770. 10.1136/bmj.320.7237.768 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rippetoe, Patricia A. , and Rogers Ronald W.. 1987. “Effects of Components of Protection‐Motivation Theory on Adaptive and Maladaptive Coping with a Health Threat.” Journal of Personality and Social Psychology 52(3): 596–604. 10.1037//0022-3514.52.3.596 [DOI] [PubMed] [Google Scholar]
- Rogers, Ronald W. 1975. “A Protection Motivation Theory of Fear Appeals and Attitude Change.” The Journal of Psychology 91(1): 93–114. 10.1080/00223980.1975.9915803 [DOI] [PubMed] [Google Scholar]
- Sha, Dexuan , Miao Xin, Lan Hai, Stewart Kathleen, Ruan Shiyang, Tian Yifei, Tian Yuyang, and Yang Chaowei. 2020. “Spatiotemporal Analysis of Medical Resource Deficiencies in the U.S. Under COVID‐19 Pandemic.” PLOS ONE 15(10): e0240348. 10.1371/journal.pone.0240348 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Singh, Meghendra , Sarkhel Prasenjit, Gloria J. Kang , Marathe Achla, Boyle Kevin, Murray‐Tuite Pamela, Abbas Kaja M., and Swarup Samarth. 2019. “Impact of Demographic Disparities in Social Distancing and Vaccination on Influenza Epidemics in Urban and Rural Regions of the United States.” BMC Infectious Diseases 19(1): 221. 10.1186/s12879-019-3703-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Slavitt, Andy . July 2, 2020. “The COVID‐19 Pandemic Underscores the Need to Address Structural Challenges of the US Health Care System.” JAMA Health Forum. Published online 141: 428. 10.1001/jamahealthforum.2020.0839 [DOI] [PubMed] [Google Scholar]
- Sundwall, David N . 2019. “Quarantine in the 21st Century: To be Effective, Public Health Policies must be Inclusive.” American Journal of Public Health 109(9): 1184–1185. 10.2105/AJPH.2019.305224 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teasdale, Emma , Santer Miriam, Geraghty Adam W. A., Little Paul, and Yardley Lucy. 2014. “Public Perceptions of Non‐Pharmaceutical Interventions for Reducing Transmission of Respiratory Infection: Systematic Review and Synthesis of Qualitative Studies.” BMC Public Health 14: 589. 10.1186/1471-2458-14-589 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teasdale, Emma , Yardley Lucy, Schlotz Wolff, and Michie Susan. 2012. “The Importance of Coping Appraisal in Behavioural Responses to Pandemic Flu.” British Journal of Health Psychology 17(1): 44–59. 10.1111/j.2044-8287.2011.02017.x [DOI] [PubMed] [Google Scholar]
- Unacast Updates Social Distancing Scoreboard-Unacast . 2020. RSS. https://www.unacast.com/post/unacast-updates-social-distancing-scoreboard
- US Census Bureau Census Bureau . 2020. “U.S. Median Household Income was $63,179 in 2018, Not Significantly Different from 2017.” The United States Census Bureau. https://www.census.gov/library/stories/2019/09/us-median-household-income-not-significantly-different-from-2017.html
- USAFacts . 2020. “Coronavirus Live Map—US Coronavirus Cases by County.” USAFacts. https://usafacts.org/visualizations/coronavirus-covid-19-spread-map/
- WHO . 2020. “Advice for the Public on COVID‐19—World Health Organization. April 19, 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public
- Wilder‐Smith, Annelies , and Freedman David O.. 2020. “Isolation, Quarantine, Social Distancing and Community Containment: Pivotal Role for Old‐style Public Health Measures in the Novel Coronavirus (2019‐nCoV) Outbreak.” Journal of Travel Medicine 27(2): taaa020. 10.1093/jtm/taaa020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams, Lynn , Rasmussen Susan, Kleczkowski Adam, Maharaj Savi, and Cairns Nicole. 2015. “Protection Motivation Theory and Social Distancing Behaviour in Response to a Simulated Infectious Disease Epidemic.” Psychology, Health & Medicine 20(7): 832–837. 10.1080/13548506.2015.1028946 [DOI] [PubMed] [Google Scholar]