

Abstract
Objectives
Guided by the Health Belief Model (HBM), this study explored factors associated with accessing COVID‐19 health information.
Design/sample
A cross‐sectional study design was used.
Sample
Migrants (n = 259) employed in Israel prior to the onset of the COVID‐19 pandemic were recruited.
Measurements
The on‐line questionnaire included: The Satisfaction with Life Scale, the Brief Resilience Coping Scale and Immigrants' Language Ability scale.
Results
Migrants obtaining COVID‐19 information when issued were more likely to have decreased employment or unemployment after COVID‐19 government restrictions (OR = 1.98; CI = 1.03, 3.89; p < .05) and more likely to have a better language ability (OR = 1.20; CI = 1.10, 1.32, p < .0001), but they were less likely to use family and/or friends as their COVID‐19 health resource (OR = 0.54, CI = 0.30, 0.96; p < .05). Migrants encountering the most employment difficulties were: female (p < .05), older age (p < .05), unmarried (p < .01), with unstable finances (p < .0001), and in Israel less than 5 years (p < .01).
Conclusions
Migrants with more precarious employment had more societal disadvantage (i.e., women, older age, unmarried, poorer socioeconomic status, and newer migrants) and relied on informal and potentially inaccurate, health sources. Public health officials aiming to decrease COVID‐19 infection must improve health information access to all members of society, particularly at‐risk groups such as migrants.
Keywords: community health, COVID‐19, health literacy, migrants
1. INTRODUCTION
With almost 200 million confirmed cases worldwide (World Health Organization, 2021), COVID‐19 has changed the daily routine of many working adults. Migrants (the World Health Organization's (WHO) term for individuals who relocated to another country (United Nations Department of Economic & Social Affairs‐Population Division, 2017)) comprise a more vulnerable population than the native‐born population for at least two major reasons: (1) many migrants, even those with advanced education, are at higher risk for being un‐ or under‐employed, both of which threaten their ability to maintain a stable living situation (Brynin et al., 2019; Munoz‐Comet & Steinmetz, 2020); and (2) migrants whose native‐language and culture are different than the host country's may have difficulty obtaining needed health‐related information (Jung et al., 2018; Lee et al., 2014). This study's objective is to assess whether English‐speaking migrants who were working prior to the COVID‐19 pandemic in Israel were able to obtain needed health information during the COVID‐19 pandemic.
2. BACKGROUND
Migrants who are employed may have an advantage over those who are unemployed because they can increase their knowledge on culture, healthcare resources, and language proficiency through their workplace exposure to native‐born individuals (Valenzuela et al., 2020). Although there is a strong association between employment and integration into the host society and its culture, the community where migrants live also exerts strong influences on the migrants' knowledge of the host country's culture and resources (Vinokurov et al., 2017). Migrants, therefore, who primarily communicate with their family or immigrant friends and dwell in predominantly migrant communities are at a disadvantage compared to those who live in native‐born communities and are continually exposed to the native‐born population. Workplaces that allow for informal socialization are helpful for integration, but not all workplaces or types of work allow for informal socialization (Vinokurov et al., 2017).
Many migrants become self‐employed when they are unable to find full‐time employment (Tapia & Alberti, 2018). Self‐employment for migrants results in more hours of work, less stability, and lower income (Brynin et al., 2019). Additionally, self‐employment, compared to full‐ or part‐time employment is more likely to lead to unemployment (Munoz‐Comet & Steinmetz, 2020). Self‐employment also does not facilitate socialization and contact with the native‐born population. As noted above, reduced exposure with the native‐born population may have negative influences on language proficiency, acculturation, and knowledge about health resources.
During the COVID‐19 pandemic, many countries instituted mandatory closures of non‐essential businesses where social distancing was not possible and transmission of the virus was more likely; these businesses included tourist sites, restaurants, and hair and nail salons (Huang et al., 2020). Many adults, including migrants, lost their jobs (Guest et al., 2020; Huang et al., 2020). Unemployment may reduce access to healthcare if employment is linked to healthcare benefits. Unemployment also may reduce access to health information among migrants who depend on their work colleagues for this information. Initiated at the onset of the COVID‐19 pandemic, this study explores the factors associated with the timely receipt of COVID‐19 health information for English‐speaking migrants who were living in Israel and employed prior to the onset of the COVID‐19 pandemic.
2.1. Health belief model
The Health Belief Model (HBM), a well‐established theoretical model, suggests that a health‐related action, such as obtaining information to prevent disease, is based on four constructs: perceived susceptibility (i.e., belief that there is a chance of contracting the disease), perceived severity (i.e., belief that the disease causes physical, social/economic, and/or emotional sequelae), perceived benefits (i.e., belief that effective actions reduce the chance of contracting the disease), and perceived barriers (i.e., belief that there are obstacles to taking actions that reduce the chance of disease) (Rosenstock, 1974; Rosenstock et al., 1988).
Previous systematic and meta‐analytic reviews show that of the four HBM constructs, perceived benefits and perceived barriers were the strongest predictors of health‐related actions (Borthwick et al., 2020; Carpenter, 2010). The positive relationship of perceived benefits to the health‐related action was later contested when some researchers found a positive association between obtaining health information and the perceived benefit only if it referred to using official sources and not informal sources such as friends and family (Borthwick et al., 2020). Another study also noted a negative association between using social media platforms as the main source of COVID‐19 information and engaging in health‐related protective actions (Allington et al., 2020). However, it should be noted that social media platforms were not examined in this study.
These recent study findings question whether there is a difference between obtaining information from informal and formal sources. Informal sources may be perceived as a benefit, but if it provides misinformation, the informal source of information may reduce the chances of the health‐related action. As a result, this study will examine both formal and informal information sources separately to determine the association between each information source and the health‐related action.
2.2. The outcome: Preventive health actions
The objective of the HBM model was to depict the constructs leading to preventive health‐related actions (Rosenstock, 1974). Health literacy is comprised of four consecutive, health‐related actions: accessing, understanding, appraising, and using health‐related information (Yuen et al., 2018). Each of the four steps must be taken sequentially to achieve health literacy; consequently, accessing health information is a necessary precursor to the three latter steps of health literacy. Unfortunately, accessing health‐related information is much more difficult for migrants, compared to native‐born adults, particularly if the host country's health system is different from the health system in the migrants’ country of origin (Guo et al., 2019). Although many countries have established websites, hotlines, clinics, and other outlets providing written or verbal materials, finding the locations of these sources of information may be challenging for migrants; and when migrants are unable to access sources of information, they have a reduced chance of obtaining needed health services (Yang et al., 2015).
2.3. Psychological variables and demographic characteristics
Psychological variables and demographic characteristics contribute to the HBM's ability to predict health‐related actions. The psychological variables have included self‐efficacy and expectations (Rosenstock et al., 1988), emotional control, resilience and psychological flexibility (Borthwick et al., 2020; Gillibrand & Stevenson, 2006), and well‐being, quality of life and the life situation (Gillibrand & Stevenson, 2006; Zhang et al., 2020). These psychological variables have contributed to the prediction of health‐related actions as adults’ feelings of helplessness (or hopefulness) were associated with the consideration of using health‐related preventive and protective actions during the COVID‐19 pandemic (Mukhtar, 2020).
Researchers using the HBM often controlled for demographic characteristics such as gender, age, income level, and employment status (Mukhtar, 2020; Zhang et al., 2020). These demographic characteristics not only have strong associations with health actions but also represent layers of societal advantage (i.e., intersectionality) prevalent in migrants (Ressia et al., 2017). For example, studies conducted during the COVID‐19 pandemic found that income levels influenced compliance with self‐quarantine (i.e., individuals with lower compared to higher income reported poorer self‐quarantine compliance) (Bodas & Peleg, 2020), and that younger versus older individuals were the more likely to be users of cellphone apps containing COVID‐19 information (Walrave et al., 2020 (forthcoming)).
Migrant status, a demographic characteristic, often is measured as a confounding, mediating or moderating variable in models assessing the relationship between the four HBM factors and the health‐related action (Chen et al., 2013). Migrants, compared to native‐born adults, exhibited fewer health‐related actions and lower health literacy due to cultural differences, poor language ability (Jung et al., 2018), and less years in the host country (Lee et al., 2014).
2.4. Study model and hypotheses
Accordingly, guided by the HBM and targeting migrants who were employed prior to the COVID‐19 pandemic, this study examined the association between the four HBM constructs and the health‐related action of obtaining COVID‐19 information on the same day it was issued (dependent variable), controlling for demographic characteristics, and psychological variables (see Figure 1).
FIGURE 1.
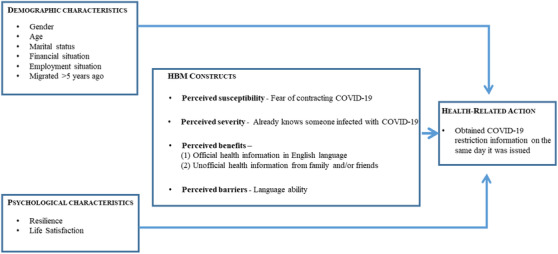
Adaptation of the Health Belief Model (HBM): To predict who obtained covid‐19 information on the same day it was issued in a sample of English‐speaking migrants [Colour figure can be viewed at wileyonlinelibrary.com]
We hypothesized that among migrants,
All HBM constructs (i.e., perceived susceptibility, perceived severity, perceived benefits, perceived barriers) will be associated with the likelihood of obtaining COVID‐19 information on the same day it was issued.
A. The HBM construct of perceived barriers, when defined as obtaining COVID‐19 information using official English‐language health resources, will be positively associated with the likelihood of obtaining COVID‐19 information on the same day it was issued.
B. The HBM construct of perceived benefits, when defined as obtaining COVID‐19 information using informal health resources of family/and or friends, will be negatively associated with the likelihood of obtaining COVID‐19 information on the same day it was issued.
C. Both formal and informal health resources will have significant associations with the likelihood of obtaining COVID‐19 information on the same day it was issued.
Those who had no change in their employment, versus migrants who did, will be more likely to obtain COVID‐19 information on the same day it was issued.
3. METHODS
For this cross‐sectional study, English‐speaking migrants living in Israel were recruited. Of the approximately 30,000 migrants coming to Israel annually (The Israeli Central Bureau of Statistics, 2020), almost 3000 migrants arrive annually from English‐speaking countries such as the USA, UK, Canada, South Africa (The Israeli Central Bureau of Statistics, 2020). English‐speaking migrants living in Israel are reported to be a “privileged” group, often arriving with funds, income and education (Zlotnick et al., 2020). Moreover, since many materials are translated into English and often native‐born individuals can speak in English, English‐speaking migrants have an easier time communicating than other migrants (Raijman et al., 2015). Yet, many English‐speaking migrants do not speak Israel's primary language Hebrew resulting in difficulties with everyday living (Zlotnick et al., 2020). Lacking the ability in the native‐language also results in the need to accept work in a different field or becoming un‐ or under‐employed (Zlotnick & Dryjanska, 2020).
Recruitment was conducted between April and mid‐May 2020, and online social media sites that specifically targeted English‐speaking migrants were used. On each social media site, the online announcements provided a link describing the study aims, the voluntary nature of participation, the target population of English‐speaking migrant adults aged 18 or older, the researchers' names and contact information, and that the individual was providing implied consent for study participation by continuing and completing the questionnaire. Of the 517 questionnaires opened on the online sites, only 411 questionnaires were completed (79.5% response rate). However, since this study focused on working migrants, only respondents who reported being employed prior to the COVID‐19 pandemic were included in this sample (n = 259). This study received the university's ethics committee approval (#197/20).
3.1. Instruments
The 70‐question online survey included: demographic characteristics (i.e., gender; age; socioeconomic status; past, current, and expected employment status in 2 months); psychological characteristics (i.e., resilience, life satisfaction); perceived susceptibility (i.e., fear of contracting COVID‐19); perceived severity (i.e., already knowing someone infected with COVID‐19); perceived benefits (i.e., official health information source is in English‐language and informal health information source consists of family and friends); perceived barriers (i.e., language ability); and the health‐related action (i.e., obtained health information on COVID‐10 on the same day it was issued).
Among these variables, three scales were used. The Brief Resilience Coping Scale with four items and a five‐level Likert scale has scores ranging from four to 20 (Sinclair & Wallston, 2004). Internal consistency (Cronbach alpha) for this sample was 81.5%.
Life satisfaction was measured by the Satisfaction with Life Scale (SWLS) containing five statements and a seven‐level Likert‐scale with scores ranging from five to 35 (Diener et al., 1985). In this study, internal consistency (Cronbach's alpha) was 89.4%
Language ability was measured by the Immigrants’ Language Ability scale (ILA) containing three questions and a five‐level rating and scores ranging from zero to twelve (Zlotnick et al., 2020). The ILA measured the English‐speaking migrants’ ability to speak and communicate in Hebrew. This scale attained a Cronbach alpha of 90.0%.
3.2. Analyses
Comparisons between groups (very confident of obtaining COVID‐19 information on the same day it was issued versus not) used chi‐square tests for categorical variables and Student t‐Tests for continuous variables. Pearson's Correlation Coefficient was used to examine associations among continuous variables. Logistic models were used to examine the relationship between the dependent dichotomous variable of very confident of obtaining COVID‐19 information on the same day it was issued versus not and the model components (i.e., demographic characteristics, psychological characteristics, and HBM constructs of perceived susceptibility, perceived severity, perceived benefits and perceived barriers). Odds ratios (OR) and 95% confidence intervals (CI) were obtained. Significance was declared at p < .05. All analyses were conducted using SAS Version 9.3.
4. RESULTS
The total sample (n = 259) was divided into two groups by the dependent variable: migrants who obtained COVID‐19 information when on the same day it was issued versus those who did not. Approximately 66% (n = 171) reported that they obtained COVID‐19 information when it was issued and 37% did not (n = 88) (See Table 1). The total sample of migrants was comprised of 69.9% women. Ages varied: 20.9% were 18–35 years, 62.6% were 36–64 years, and 16.6% were 65 or older. Approximately 58.3% were married; 71.4% migrated more than 5 years ago; and 37.5% reported decreased employment or unemployment after COVID‐19 restrictions. The two groups were compared on the demographic characteristics (i.e., gender, age, marital status, migrated more than 5 years ago, the financial status is worse now than 2 months ago and will deteriorate further in another 2 months, and decreased employment or unemployment after COVID‐19 government restrictions), but no significant differences by groups were found.
TABLE 1.
Comparison of Health Belief Model (HBM) components based on action of obtained COVID‐19 information when issued among English‐speaking migrants (n = 259)
| Total sample | Obtained COVID‐19 information when issued | ||
|---|---|---|---|
| HBM components | (n = 259) Percent (n) | Yes (n = 171) Percent (n) | No (n = 88) Percent (n) |
| Psychological characteristics | |||
| Resilience (Mean, SD) | 14.7 (3.04) | 14.7 (3.20) | 14. 7 (2.73) |
| Life satisfaction (Mean, SD) | 16.1 (6.90) | 15.5 (6.78) | 17.3 (7.03) |
| Perceived susceptibility | |||
| Fear of COVID‐19 infection | 62.6 (162) | 63.7 (109) | 60.2 (53) |
| Perceived severity | |||
| Knows someone with COVID‐19 | 29.3 (76) | 31.6 (54) | 25.0 (22) |
| Perceived benefits | |||
| COVID‐19 health resource of English‐language website | 78.4 (203) | 77.2 (132) | 80.7 (71) |
| COVID‐19 health resource of family and/or friends* | 40.2 (104) | 35.7 (61) | 48.9 (43) |
| Perceived barriers | |||
| Language ability (Mean, SD)**** | 7.51 (3.59) | 8.2 (3.68) | 6.2 (3.01) |
p < .05.
p < .01.
p < .001.
p < .0001.
Comparisons between the two groups were conducted on the psychological characteristics (i.e., resilience and life satisfaction), perceived susceptibility (i.e., fear of COVID‐19 infection) and perceived severity (i.e., knows someone with COVID‐19), but no significant differences by groups were found (see Table 1). However, differences were found in the perceived benefit variable of COVID‐19 health resource of family and/or friends the perceived barrier variable of language ability. More migrants in the group that did not obtain COVID‐19 information on the same day it was issued, compared to the group that did, relied on the COVID‐19 health resource of family/or friends (p < .05), and had a good language ability (p < .0001).
Logistic regression models were used to examine whether the health‐related action (i.e., the migrant obtained COVID‐19 information on the same day it was issued) was related to model components of demographic characteristics, psychological characteristics, perceived susceptibility, perceived severity, perceived benefits, and perceived barriers. As perceived benefits contained two variables representing formal and informal sources of information, separate models were used to examine the influence first of formal and then of informal sources of information.
In the first model (see Table 2), perceived benefits was measured by a variable representing formal sources of information. Although this model was significant (p < .05), obtaining COVID‐19 information on the same day it was issued was not associated with the perceived benefits' variable; however, the dependent variable was associated with decreased employment or unemployment after COVID‐19 government restrictions (OR = 1.91; CI = 1.01, 3.73; p < .05) and having a better language ability (OR = 1.22; CI = 1.12, 1.32, p < .0001).
TABLE 2.
Logistic regression models with odds ratios and 95% confidence intervals (CI) predicting obtained COVID‐19 information on the same day when disseminated pandemic in English‐speaking migrants (n = 259)
| OR (CI) | OR (CI) | OR (CI) | |
|---|---|---|---|
| Demographic characteristics | |||
| Gender (Referent‐male) | 0.83 (0.45, 1.53) | 0.76 (0.41, 1.42) | 0.74 (0.40, 1.39) |
| Age (Referent‐18–35 years) | |||
| 36–64 years | 1.14 (0.52, 2.60) | 1.21 (0.51, 2.42) | 1.15 (0.52, 2.51) |
| 65+ years | 1.58 (0.56, 4.56) | 1.62 (0.57, 4.79) | 1.67 (0.58, 4.96) |
| Marital status ‐ married | 1.73 (0.94, 3.23) | 1.64 (0.88, 3.08) | 1.66 (0.89, 3.12) |
| Financial situation is worse now than 2 months ago and will deteriorate further in another 2 months | 1.71 (0.93, 3.22) | 1.82 (0.98, 3.46) | 1.81 (0.97, 3.44) |
| Decreased employment or unemployment after COVID‐19 government restrictions | 1.91 (1.01, 3.73)* | 1.94 (1.01, 3.80)* | 1.98 (1.03, 3.89) * |
| Migrated > 5 years ago | 0.75 (0.37, 1.50) | 0.73 (0.36, 1.47) | 0.73 (0.36, 1.46) |
| Psychological characteristics | |||
| Resilience | 0.98 (0.88, 1.09) | 0.98 (0.88, 1.08) | 0.97 (0.87, 1.08) |
| Life satisfaction | 0.98 (0.94, 1.02) | 0.98 (0.94, 1.02) | 0.98 (0.94, 1.02) |
| Perceived susceptibility | |||
| Fears contracting COVID‐19 infection | 0.94 (0.52, 1.68) | 1.00 (0.55, 1.78) | 1.44 (0.77, 2.76) |
| Perceived severity | |||
| Knows someone with COVID‐19 | 1.43 (0.77, 2.72) | 1.44 (0.77, 2.76) | 0.98 (0.54, 1.76) |
| Perceived benefits | |||
| COVID‐19 health resource of English‐language website | 1.26 (0.60, 2.62) | 1.28 (0.61, 2.69) | |
| COVID‐19 health resource of family and/or friends | 0.54 (0.30, 0.96)* | 0.54 (0.30, 0.96) * | |
| Perceived barriers | |||
| Language ability | 1.21 (1.11, 1.33)**** | 1.20 (1.10, 1.32)**** | 1.20 (1.10, 1.32)**** |
| Wald chi‐square (df) | 26.22 (13)* | 29.07 (13)** | 29.46 (14)** |
p < .05.
p < .01.
p < .001.
p < .0001.
In the second model (see Table 2), perceived benefits was measured by a variable representing informal sources of information. This model was significant (p < .01). Perceived benefits when measured by informal sources of information (OR = 0.54; CI = 0.30, 0.96; p < .05) was negatively associated with obtaining COVID‐19 information on the same day it was issued. Additionally, the dependent variable was associated with decreased employment or unemployment after COVID‐19 government restrictions (OR = 1.94; CI = 1.01, 3.80; p < .05) and having a better language ability (OR = 1.20; CI = 1.10, 1.32, p < .0001).
The third model includes both variables representing perceived benefits (see Table 2). The model was significant (p < .01). Migrants who obtained COVID‐19 information on the same day it was issued were more likely to have had decreased employment or unemployment after COVID‐19 government restrictions (OR = 1.98; CI = 1.03, 3.89; p < .05), were less likely to use the COVID‐19 health resource of family and/or friends (OR = 0.54, CI = 0.30, 0.96; p < .05), and were more likely to have a better language ability (OR = 1.20; CI = 1.10, 1.32, p < .0001).
Post‐hoc examinations of the demographic characteristics were conducted to examine migrants who had decreased employment or unemployment after COVID‐19 government restrictions versus those who did not (see Figure 2). Findings revealed that among migrants, those who did not experience decreased employment or unemployment after COVID‐19 government restrictions were more likely to be: male (p < .05), aged 36–64 (p < .05), married (p < .01), with stable finances (p < .0001), more than 5 years post migration (p < .01).
FIGURE 2.
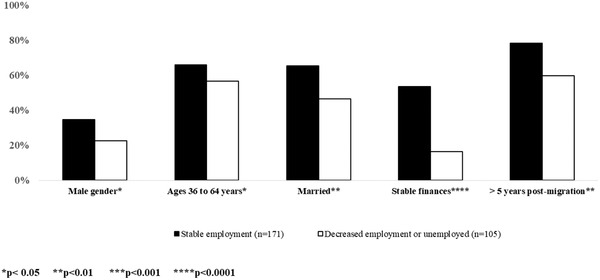
Demographic characteristics by employment status among English‐speaking migrants (n = 259)
5. DISCUSSION
Among migrants who were working 2 months prior to the COVID‐19 pandemic, the dependent variable (i.e., obtaining COVID‐19 information on the same day it was issued) was associated with the HBM constructs of perceived benefits (i.e., health resource of family/friends) and perceived barriers (i.e., language ability), but not with perceived susceptibility or perceived severity (Hypothesis 1). Although no association was found between receiving information from official English‐language sources and obtaining COVID‐19 information on the same day it was issued (Hypothesis 2A), consistent with the literature (Borthwick et al., 2020), reliance on health information from family and friends was negatively associated with obtaining COVID‐19 information on the same day it was issued (Hypothesis 2B). Additionally, findings showed that migrants who obtained COVID‐19 information on the same day it was issued were more likely to be those who had decreased employment or unemployment after COVID‐19 government restrictions, contrary to the hypothesis (Hypothesis 3).
5.1. Migrants, COVID‐19 information and the HBM
This study found that among migrants, obtaining COVID‐19 information on the same day it was issued was associated with the two HBM constructs of perceived benefits and perceived barriers, which were the two HBM constructs most often associated with preventive health‐related action (Borthwick et al., 2020). In this study, the construct of perceived barriers, operationalized as language ability, was positively associated with obtaining COVID‐19 information on the same day it was issued for the migrants. COVID‐19 information was disseminated through written and verbal media; however, it was most often delivered in Israel's native languages (Hebrew or Arabic). Thus, consistent with other studies on migrants (Jung et al., 2018), our study found that migrants who reported having better language abilities in the host country's mother tongue, were more likely to access COVID‐19 information on the same day it was issued.
The construct of perceived benefits was operationalized in this study as using formal health resources in English‐language and informal health resources of family and friends. Only using the informal health resource of family and friends exhibited a significant relationship with the dependent variable indicating that migrants using the informal health resource of family and friends were less likely to obtain COVID‐19 information on the same day it was issued. A similar finding was obtained by other researchers targeting the general population who noted that while using a variety of formal resources to obtain COVID‐19 information was positively associated with health‐related actions, using friends and family was negatively associated with the health‐related action (Allington et al., 2020). A plausible explanation for this negative association could be that migrants, due to lack of education or understanding of other sources of information, relied on friends and family as their health resource; and reliance on friends and family as their sole health information source resulted in obtaining health information in a less timely or accurate manner.
Despite the vast literature relating psychological variables, we found that resilience and life satisfaction had no associations with the dependent variable (i.e., obtained COVID‐19 health information on the same day it was issued). According to the scale, migrants in our sample attained scores indicating moderate resilience (Sinclair & Wallston, 2004). A US‐based study found that adult migrants during the COVID‐19 pandemic had low levels of resilience; these researchers attributed this lower level of resilience to the high levels of stress that resulted from their struggles with the native language (Ferreira et al., 2020).
5.2. Working migrants in the COVID‐19 pandemic
Among the demographic variables, decreased employment or unemployment was associated with being more likely to obtain COVID‐19 health information on the same day it was issued. This finding was surprising given that existing literature highlighted the benefits of workplace socialization as a source of information (Valenzuela et al., 2020) and that those with the most precarious employment is typically less likely to access health information (Guo et al., 2019). We had anticipated that employed individuals would need to be attentive to new restrictions and engage in protective actions such as using face coverings during work interactions (Fisher et al., 2020). Our findings indicating that migrants with decreased employment or unemployment obtained COVID‐19 in a timely fashion may suggest these migrants were more attuned to health information with the hope that COVID‐19 restrictions would be removed. In this situation, our finding is not really a positive finding, but a reaction to a negative situation. Another possible explanation is that those who did not work or worked less, had more time to search for health information.
Consistent with our findings, employment status is a focal point where many demographic characteristics (i.e., gender, age, marital status, finances, and year of migration) indicating societal advantage and disadvantage (i.e., intersectionality) overlap (Ressia et al., 2017; Tapia & Alberti, 2018). Societal advantage is more common among men (McCall, 2005), individuals in the mid‐age range (Choroszewicz, 2019), those with higher socioeconomic status (Walby et al., 2012), and non‐migrants (Brynin et al., 2019; Tapia & Alberti, 2018). These same layers of societal disadvantage were found by other researchers focusing on migrants (Siebers & van Gastel, 2015).
5.3. Limitations
This study has the limitation of using a cross‐sectional study design with self‐reported responses and a convenience sample. Thus, associations are presented and causality cannot be inferred. The convenience sample was recruited via social media targeting English‐language speakers; migrants who do not use social media or use native language resources may not be represented. Accordingly, results may not be generalizable to all migrants. Lastly, the operationalization of the HBM constructs may vary, particularly, since the HBM originally was based on studies with US populations and no efforts were made to represent other cultures (Rosenstock, 1974).
5.4. Relevance for clinical practice
Despite limitations, this study provides a unique insight on the use of COVID‐19 information among migrants who were working prior to the pandemic. It is important to note that health literacy views the obligation of individuals to determine and obtain their healthcare needs. Nevertheless, health systems and their healthcare professional also have the obligation to consider their populations' needs. The COVID‐19 pandemic has revealed that even high‐income countries failed to invest in community‐based public health infrastructures. The vast network of community‐based, public health nurses worked to decrease spread of infection, disseminate health advice, and promote wellness have dwindled substantially in recent decades; however, the inconsistent public response to the pandemic suggests the need for its return (Madjar et al., 2019). But country‐wide efforts are not enough in a global pandemic. We also need global nursing leadership (Rosser et al., 2020).
CONFLICT OF INTEREST
The authors have no competing or conflicting interests.
ETHICAL STATEMENT
University's ethics committee approval (#197/20).
AUTHOR CONTRIBUTIONS
Study design: Cheryl Zlotnick, Laura Dryjanska, Suzanne Suckerman. Data collection: Suzanne Suckerman. Data analysis: Cheryl Zlotnick. First draft: Cheryl Zlotnick. Manuscript writing: Cheryl Zlotnick, Laura Dryjanska. Final manuscript approval: Cheryl Zlotnick, Laura Dryjanska, Suzanne Suckerman
ACKNOWLEDGMENTS
None.
Zlotnick, C. , Dryjanska, L. , & Suckerman, S. (2022). Factors linked to accessing COVID‐19 recommendations among working migrants. Public Health Nursing, 39, 24–32. 10.1111/phn.12982
DATA AVAILABILITY STATEMENT
Research data are not shared.
REFERENCES
- Allington, D. , Duffy, B. , Wessely, S. , Dhavan, N. , & Rubin, J. (2020). Health‐protective behaviour, social media usage and conspiracy belief during the COVID‐19 public health emergency. Psychological Medicine, 51, 1763–1769. 10.1017/S003329172000224X ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bodas, M. , & Peleg, K. (2020). Self‐isolation compliance in the Covid‐19 era influenced by compensation: Findings from a recent survey in Israel. Health Affairs, 39(6), 936–941. 10.1377/hlthaff.2020.00382 [DOI] [PubMed] [Google Scholar]
- Borthwick, C. , O'Connor, R. , & Kennedy, L. (2020). Psychological predictors of seasonal influenza vaccination uptake among adults with a high‐risk physical health condition: A systematic review. Psychology & Health, 36(2), 214–235. 10.1080/08870446.2020.1772971 [DOI] [PubMed] [Google Scholar]
- Brynin, M. , Shamsul Karim, M. , & Zwysen, W. (2019). The value of self‐employment to ethnic minorities. Work, Employment and Society, 33(5), 846–864. 10.1177/0950017019855232 [DOI] [Google Scholar]
- Carpenter, C. J. (2010). A meta‐analysis of the effectiveness of health belief model variables in predicting behavior. Health Communication, 25(8), 661–669. 10.1080/10410236.2010.521906 [DOI] [PubMed] [Google Scholar]
- Chen, S. C. , Tsai, Y. T. , Hu, S. C. , Lin, C. L. , Chen, K. L. , Chen, K. H. , & Chen, K. T. (2013). Factors affecting the use of anti‐amoebiasis protective measures among Taiwan immigrants returning to amoebiasis‐endemic regions. Public Health, 127(12), 1126–1132. 10.1016/j.puhe.2013.09.004 [DOI] [PubMed] [Google Scholar]
- Choroszewicz, M. (2019). Gender and age in the professions: Intersectionality, metawork, and social change. Professions & Professionalism, 9(2), e3432. 10.7577/pp.3432 [DOI] [Google Scholar]
- Diener, E.d , Emmons, R. A. , Larsen, R. J. , & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49(1), 71–75. 10.1207/s15327752jpa4901_13 [DOI] [PubMed] [Google Scholar]
- Ferreira, R. J. , Buttell, F. , & Cannon, C. (2020). COVID‐19: Immediate predictors of individual resilience. Sustainability, 12(16), 1–11. 10.3390/su12166495 35136666 [DOI] [Google Scholar]
- Fisher, K. A. , Barile, J. P. , Guerin, R. J. , Esschert, K. L. V. , Jeffers, A. , Tian, L. H. , Garcia‐Williams, A. , Gurbaxani, B. , Thompson, W. W. , & Prue, C. E. (2020). Factors associated with cloth face covering use among adults during the COVID‐19 pandemic—United States, April and May 2020. MMWR: Morbidity and Mortality Weekly Report, 69(28), 933–937. [DOI] [PubMed] [Google Scholar]
- Gillibrand, R. , & Stevenson, J. (2006). The extended health belief model applied to the experience of diabetes in young people. British Journal of Health Psychology, 11(Pt 1), 155–169. 10.1348/135910705X39485 [DOI] [PubMed] [Google Scholar]
- Guest, D. , Knox, A. , & Warhurst, C. (2020). Human relations virtual special issue: The quality of working life revisited. Human Relations, 74(1), 153–156. 10.1177/0018726720973156 [DOI] [Google Scholar]
- Guo, M. , Steinberg, S. , Nadia Dong, X. , & Tiwari, A. (2019). Is family relations related to health service utilisation among older immigrants: Evidence from Chinese elderly in the United States. Health & Social Care in the Community, 27(1), 215–225. 10.1111/hsc.13054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huang, A. , Makridis, C. , Baker, M. , Medeiros, M. , & Guo, Z. (2020). Understanding the impact of COVID‐19 intervention policies on the hospitality labor market. International Journal of Hospitality Management, 91, 102660. 10.1016/j.ijhm.2020.102660 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jung, M. Y. , Ng, D. , Sim, H. J. , Xiaoxiao, L.u , Sunmin, L. , Holt, C. L. , Juon, H. ‐S. , Li, J. , & Jun, L.i (2018). The Chinese and Korean American immigrant experience: A mixed‐methods examination of facilitators and barriers of colorectal cancer screening. Ethnicity & Health, 23(8), 847–866. 10.1080/13557858.2017.1296559 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, H. Y. , Stange, M. J.u , & Ahluwalia, J. S. (2014). Breast cancer screening behaviors among Korean American immigrant women: Findings from the Health Belief Model. Journal of Transcultural Nursing, 26(5), 450–457. 10.1177/1043659614526457 [DOI] [PubMed] [Google Scholar]
- Madjar, B. , Shachaf, S. , & Zlotnick, C. (2019). Changing the current health system's vision for disease prevention and health promotion. International Nursing Review, 66(4), 490–497. 10.1111/inr.12535 [DOI] [PubMed] [Google Scholar]
- McCall, L. (2005). The complexity of intersectionality. Signs: Journal of Women in Culture and Society, 30(3), 1771–1800. 10.1086/426800 [DOI] [Google Scholar]
- Mukhtar, S. (2020). Mental health and emotional impact of COVID‐19: Applying health belief model for medical staff to general public of Pakistan. Brain, Behavior, and Immunity, 87, 28–29. 10.1016/j.bbi.2020.04.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Munoz‐Comet, J. , & Steinmetz, S. (2020). Trapped in precariousness? Risks and opportunities of female immigrants and natives transitioning from part‐time jobs in Spain. Work, Employment and Society, 34, 749–768. 10.1177/0950017020902974 [DOI] [Google Scholar]
- Raijman, R. , Semyonov, M. , & Geffen, R. (2015). Language proficiency among post‐1990 immigrants in Israel. Journal of Ethnic and Migration Studies, 41(8), 1347–1371. 10.1080/1369183X.2014.982523 [DOI] [Google Scholar]
- Ressia, S. , Strachan, G. , & Bailey, J. (2017). Operationalizing intersectionality: An approach to uncovering the complexity of the migrant job search in Australia. Gender, Work & Organization, 24(4), 376–397. 10.1111/gwao.12172 [DOI] [Google Scholar]
- Rosenstock, I. M. (1974). Historical origins of the health belief model. Health Education Quarterly, 2(4), 328–335. 10.1177/109019817400200403 [DOI] [PubMed] [Google Scholar]
- Rosenstock, I. M. , Strecher, V. J. , & Becker, M. H. (1988). Social learning theory and the health belief model. Health Education Quarterly, 15(2), 175–183. 10.1177/109019818801500203 [DOI] [PubMed] [Google Scholar]
- Rosser, E. , Westcott, L. , Ali, P. A. , Bosanquet, J. , Castro‐Sanchez, E. , Dewing, J. , McCormack, B. , Merrell, J. , & Witham, G. (2020). The need for visible nursing leadership during COVID‐19. Journal of Nursing Scholarship, 52(5), 459–461. 10.1111/jnu.12587 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Siebers, H. , & van Gastel, J. (2015). Why migrants earn less: In search of the factors producing the ethno‐migrant pay gap in a Dutch public organization. Work, Employment and Society, 29(3), 371–391. 10.1177/0950017014568138 [DOI] [Google Scholar]
- Sinclair, V. G. , & Wallston, K. A. (2004). The development and psychometric evaluation of the brief resilient coping scale. Assessment, 11(1), 94–101. 10.1177/1073191103258144 [DOI] [PubMed] [Google Scholar]
- Tapia, M. , & Alberti, G. (2018). Unpacking the category of migrant workers in trade union research: A multi‐level approach to migrant intersectionalities. Work, Employment and Society, 33(2), 314–325. 10.1177/0950017018780589 [DOI] [Google Scholar]
- The Israeli Central Bureau of Statistics (Producer) .(2020). Table 2–Immigrants, By Continent and Selected Last Country of Residence. Retrieved from: https://www.cbs.gov.il/en/subjects/Pages/Immigration‐and‐International‐Migration.aspx
- United Nations Department of Economic and Social Affairs‐Population Division . (2017). International Migration Report. ST/ESA/SER.A/404. https://www.un.org/en/development/desa/population/migration/publications/migrationreport/docs/MigrationReport2017_Highlights.pdf
- Valenzuela, M. A. , Flinchbaugh, C. , & Rogers, S. E. (2020). Can organizations help adjust?: The effect of perceived organizational climate on immigrants' acculturation and consequent effect on perceived fit. Journal of International Management, 26(3), 100775. 10.1016/j.intman.2020.100775 [DOI] [Google Scholar]
- Vinokurov, A. , Trickett, E. J. , & Birman, D. (2017). Community context matters: Acculturation and underemployment of Russian‐speaking refugees. International Journal of Intercultural Relations, 57, 42–56. 10.1016/j.ijintrel.2017.02.002 [DOI] [Google Scholar]
- Walby, S. , Armstrong, J.o , & Strid, S. (2012). Intersectionality: Multiple inequalities in social theory. Sociology, 46(2), 224–240. 10.1177/0038038511416164 [DOI] [Google Scholar]
- Walrave, M. , Waeterloos, C. , & Ponnet, K. (.(forthcoming)). (2020) Tracing the COVID‐19 Virus: A health belief model approach to the adoption of a contact tracing App. JMIR Public Health and Surveillance, 6, e20572. 10.2196/20572 [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization . (2021). Coronavirus disease (COVID‐19) pandemic, Numbers at a glance (28 July 2021). Home/Diseases/Coronavirus disease (COVID‐19). Retrieved from: https://www.who.int/emergencies/diseases/novel‐coronavirus‐2019
- Yang, Y. ‐M. , Wang, H. ‐H. , Lee, F. ‐H. , Lin, M. ‐L. , & Lin, P. ‐C. (2015). Health empowerment among immigrant women in transnational marriages in Taiwan. Journal of Nursing Scholarship, 47(2), 135–142. 10.1111/jnu.12110 [DOI] [PubMed] [Google Scholar]
- Yuen, E. Y. N. , Knight, T. , Ricciardelli, L. A. , & Burney, S. (2018). Health literacy of caregivers of adult care recipients: A systematic scoping review. Health & Social Care in the Community, 26(2), e191–e206. 10.1111/hsc.12368 [DOI] [PubMed] [Google Scholar]
- Zhang, L. , Jung, E. H. , & Chen, Z. (2020). Modeling the pathway linking health information seeking to psychological well‐being on WeChat. Health Communication, 35(9), 1101–1112. 10.1080/10410236.2019.1613479 [DOI] [PubMed] [Google Scholar]
- Zlotnick, C. , & Dryjanska, L. (2020). Immigrants’ health, acculturation, and the work‐retirement continuum. Health & Social Work, 45(1), 13–22. 10.1093/hsw/hlz039 [DOI] [PubMed] [Google Scholar]
- Zlotnick, C. , Dryjanska, L. , & Suckerman, S. (2020). The association between acculturation variables and life satisfaction among Israeli immigrants from four English‐speaking countries. Journal of Happiness Studies, 21, 1427–1444. 10.1007/s10902-019-00137-3 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Research data are not shared.