

To the Editor,
The decision on whether or not to vaccinate young children against coronavirus disease 2019 (COVID‐19) is causing significant controversy in the UK. Ladhani 1 outlines the pros and cons of vaccinating school children, and we agree that it is not an easy decision. However, with a potentially difficult winter ahead, including the backlog of non‐COVID‐19 medical cases to care for and the return of seasonal respiratory viruses in the absence of COVID‐19 restrictions, 2 expanding vaccine coverage for both influenza and COVID‐19, would seem prudent. Another aspect that needs to be considered is the impact that increased numbers of sick children (even if not requiring hospitalization) will have on working parents, who will need to take time off work to care for them.
Although the COVID‐19 vaccine rollout in the UK has been a remarkable success, the last phase of the severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) versus vaccine race is being hampered by a reduced vaccine uptake in the younger population (18–30 years old). This is likely due to individual risk‐benefit self‐assessment, based on some widely publicized data, 3 which estimates much lower risks of COVID‐19 complications in the young. Yet, the inadvertent impact of this data sharing has been to reduce the urgency of COVID‐19 vaccination in these younger populations.
Unfortunately, what these low vaccine update figures do not show is the potential impact on the older adult contacts of these potentially delta variant‐infected younger populations (e.g., parents, grandparents, teachers), where the delta variant has effectively broken through fully vaccinated individuals, some of whom need hospitalization. 4 , 5
The increasing numbers of hospitalized cases infected with the delta variant are likely partly due to some degree of the waning of vaccine immunity over time. 6 , 7 Not only this, a recent US study has suggested that delta variant SARS‐COV‐2 viral loads are similar between newly diagnosed COVID‐19 cases that have been vaccinated (mainly with the messenger RNA vaccines) and the unvaccinated, 8 indicating that even fully vaccinated adults can potentially still transmit the virus to unvaccinated children.
Local data (Table and Figure 1), during May–July 2021, confirm this UK trend of a higher incidence of hospitalized COVID‐19 cases in the younger population, in whom vaccine coverage is generally lower.
Figure 1.
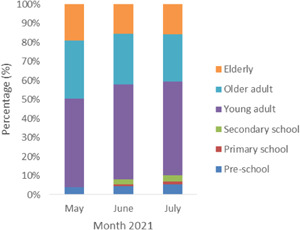
Proportions by age of severe acute respiratory syndrome coronavirus 2 polymerase chain reaction‐positive patients presenting or admitted to University Hospitals of Leicester May–July 2021. Preschool: 4 years old and under; primary school 5–11 years; secondary school 12–18 years; young adult 19–50 years; older adult 51–75 years; and elderly 76 years and older
Table 1 shows increasing numbers of COVID‐19 cases presenting to hospital—now mostly due to the delta variant 9 —in the younger groups, but also in the more vulnerable older adult and elderly populations. Yet, although the absolute numbers of COVID‐19 cases are rising in these populations, COVID‐19 cases are rising at similar rates across all the age groups, so the overall proportion of COVID‐19 cases across these different age groups remains more or less constant during this period (Figure 1). So despite the UK COVID‐19 vaccination success, the young adults (19–50 years) still constitute the highest proportion (45%–50%) of all COVID‐19 cases in this hospitalized patient population.
Table 1.
SARS‐CoV‐2 PCR‐positive patients presenting or admitted to UHL during May–July 2021
| Month | Preschool (%) | Primary school (%) | Secondary school (%) | Young adult (%) | Older adult (%) | Elderly (%) | Total |
|---|---|---|---|---|---|---|---|
| May | 4 (3.8) | 0 (0) | 0 (0) | 49 (46.7) | 32 (30.5) | 20 (19) | 105 |
| June | 9 (4.5) | 2 (1) | 5 (2.5) | 100 (50) | 53 (26.5) | 31 (15.5) | 200 |
| July | 24 (5.4) | 6 (1.3) | 15 (3.4) | 220 (49.3) | 111 (24.9) | 70 (15.7) | 446 |
Note: Preschool: 4 years old and under; primary school 5–11 years; secondary school 12–18 years; young adults 19–50; older adults 51–75; and elderly 76 years and older.
Abbreviations: PCR, polymerase chain reaction; SARS‐CoV‐2, severe acute respiratory syndrome coronavirus 2; UHL, University Hospitals of Leicester.
These ongoing infection rates will allow the delta variant to seed itself across more of the UK population, leading to the more widespread viral transmission when schools reopen in September. If breakthrough infections with the delta variant produce similar viral loads in both the vaccinated and the unvaccinated, 8 an increase in COVID‐19 cases and hospitalizations is inevitable, in the UK population, going into the autumn and winter months.
The recent decision by the UK's Joint Committee on Vaccination and Immunisation (JCVI) to allow the COVID‐19 vaccination (with the Pfizer vaccine) only in 16–17 years old will help to reduce the overall pool of susceptible hosts to the virus. 10 Yet, this still leaves a large number of school children (aged 15 years and younger) that can still be infected with the virus and transmit it onwards—as was seen earlier, in another large UK city (Bristol). 11
The UK JCVI's reluctance to approve COVID‐19 vaccinations for younger children is in notable contrast to other developed countries, such as the USA, Canada, France, Italy, Spain, Switzerland, and The Netherlands, which have already been offering COVID‐19 vaccines to 12–15 year old for several months ahead of the school year—with some, like The Netherlands, not even requiring parental consent. 12
This hesitation is somewhat surprising, given the UK's previous “pioneering” decisions to offer just one vaccine dose initially, with variable intervals between first and second vaccine doses—as well as the ongoing school influenza immunization program in the UK (https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1011774/Withdrawn_Annual_national_childhood_flu_programme_2020_21_v2.pdf).
It will be interesting to compare and contrast the spread of the virus in the UK with these other countries, when schools reopen in September.
CONFLICT OF INTERESTS
The authors declare that there are no conflict of interests.
AUTHOR CONTRIBUTIONS
Julian W. Tang conceived the presented idea. Data were collected by Roger Riff and Andrew Folwell. Data were analyzed by Paul W. Bird, Christopher W. Holmes, and Julian W. Tang. Julian W. Tang and Paul W. Bird drafted the manuscript. All authors reviewed the manuscript and made amendments before submission.
DATA AVAILABILITY STATEMENT
Data are available from the corresponding author upon reasonable request.
REFERENCES
- 1. Ladhani SN. Crossing the Rubicon: a fine line between waiting and vaccinating adolescents against COVID‐19. J Infect. 2021;83:294‐297. 10.1016/j.jinf.2021.07.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Weekly national influenza and COVID‐19 surveillance report week 29 report (up to week 28 data). Public Health England. July 22, 2021. Accessed August 12, 2021. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1005056/Weekly_Flu_and_COVID-19_report_w29.pdf
- 3.News—communicating the potential benefits and harms of the Astra‐Zeneca COVID‐19 vaccine. Winton Centre for Risk and Evidence Communication. 2021. Accessed August 15, 2021. https://wintoncentre.maths.cam.ac.uk/news/communicating-potential-benefits-and-harms-astra-zeneca-covid-19-vaccine/
- 4. Sheikh A, McMenamin J, Taylor B, Robertson C, Public Health Scotland and the EAVE II Collaborators . SARS‐CoV‐2 delta VOC in Scotland: demographics, risk of hospital admission, and vaccine effectiveness. Lancet. 2021;397(10293):2461‐2462. 10.1016/S0140-6736(21)01358-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. SARS‐CoV‐2 variants of concern and variants under investigation in England . Technical briefing 20. Public Health England. August 6, 2021. Accessed August 12, 2021. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1009243/Technical_Briefing_20.pdf
- 6. Mizrahi B, Lotan R, Kalkstein N, et al. Correlation of SARS‐CoV‐2 breakthrough infections to time‐from‐vaccine. medRxiv. 2021. https://www.medrxiv.org/content/10.1101/2021.07.29.21261317v1.full [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Thomas SJ, Moreira ED Jr., Kitchin N, et al. Six month safety and efficacy of the BNT162b2 mRNA COVID‐19 vaccine. medRxiv. 2021. https://www.medrxiv.org/content/10.1101/2021.07.28.21261159v1.full [Google Scholar]
- 8. Riemersma KK, Grogan BE, Kita‐Yarbro A, et al. Shedding of Infectious SARS‐CoV‐2 Despite Vaccination when the Delta Variant is Prevalent ‐ Wisconsin, July 2021. medRxiv. 2021. https://www.medrxiv.org/content/10.1101/2021.07.31.21261387v3 [Google Scholar]
- 9.COVID‐19 genomic surveillance. Wellcome Sanger Institute. September 2020–August 2021. Accessed September 6, 2021. https://covid19.sanger.ac.uk/lineages/raw?date=2020-09-12%26latitude=54.539588%26longitude=-3.458979%26zoom=4.74%26show=A%2CAY.4%2CAY.5%2CAY.6%2CAY.9%2CB%2CB.1.1.7%2CB.1.177%2CB.1.351%2CB.1.617.2
- 10.Written statement: COVID‐19 vaccination—JCVI announcement on vaccinating children & young people. Welsh Government. 2021. Accessed August 12, 2021. https://gov.wales/written-statement-covid-19-vaccination-jcvi-announcement-vaccinating-children-young-people-0
- 11. Hall R, Geddes L. Expert expresses fears over Covid outbreaks at Bristol schools. The Guardian. June 2, 2021. Accessed August 15, 2021. https://www.theguardian.com/world/2021/jun/02/expert-expresses-fears-over-covid-outbreaks-at-bristol-schools
- 12.Factbox: countries vaccinating children against COVID‐19. Reuters. June 29, 2021. Accessed August 15, 2021. https://www.reuters.com/business/healthcare-pharmaceuticals/countries-vaccinating-children-against-covid-19-2021-06-29/
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data are available from the corresponding author upon reasonable request.