

Abstract
Aim and objective
Fogging of eyeglasses while wearing N95 respirators is common. It is commonly held that the N95 respirator has a poor fit if there is fogging of eyeglasses. We conducted this prospective, pilot study to determine if fogging of eyeglasses predicts poor fit of N95 respirator.
Materials and methods
Seventy volunteer healthcare workers from a tertiary intensive care unit in Sydney, Australia participated. The participants donned one of the following N95 respirators: three-panel flat-fold respirator (3M 1870), cup-shaped respirator (3M 1860), or a duckbill respirator. After a satisfactory “user seal check” as recommended by the manufacturer, the participants donned eyeglasses and checked for fogging. A quantitative fit test (QnFT) of the respirator was then performed (using PortaCount Respirator Fit Tester 8048, TSI Inc., Minnesota, USA). A fit factor of <100 on quantitative fit testing indicates poor fit. The sensitivity and specificity for fogging of eyeglasses (index test) to predict the poor fit of N95 respirator was determined, compared to QnFT (gold standard test).
Results
Fogging of eyeglasses as a predictor of poor respirator fit (i.e., fit factor <100 on QnFT) had sensitivity of 71% (95% CI, 54–85%) and specificity 46% (95% CI, 29–63%). The odds ratio of fogging as a predictor for poor fit was 2.10 (95% CI, 0.78–5.67), with a two-tailed p-value of 0.22 (not significant). The receiver operating characteristic curve for fogging of eyeglasses as a diagnostic test had the area under the curve of 0.59.
Conclusion
Fogging of eyeglasses is neither a sensitive nor a specific predictor for poor fit of N95 respirators.
How to cite this article
Kyaw S, Johns M, Lim R, Stewart WC, Rojas N, Thambiraj SR, et al. Prediction of N95 Respirator Fit from Fogging of Eyeglasses: A Pilot Study. Indian J Crit Care Med 2021;25(9):976–980.
Keywords: Eyeglasses, Healthcare workers, Infectious disease, Intensive care, N95 respirators, Occupational health
Introduction
During the COVID-19 pandemic, N95 respirators are commonly used as part of personal protective equipment (PPE) for healthcare workers (HCWs).1–3 The N95 respirators block at least 95% of the particles >0.3 µm in size.4 The respirator efficiency is dependent on an adequate seal, and there is no guarantee of its efficiency unless it is fit-tested for each user. Quantitative fit test (QnFT), as defined in the Australia/New Zealand Standard 1715: 2009, is a validated method for fit testing of N95 respirator.5,6
However, passing the QnFT does not always guarantee a good fit. At point-of-care, the manufacturers recommend performing a “user seal check,” also known as “fit checking” which is done by inhaling and exhaling sharply and observing for air leak around the nose and respirator edges. The user seal check has poor sensitivity in detecting leaks around the respirator and there is no other widely available point-of-care test for determining adequate fit of the N95 respirator.7,8
Most N95 respirators have a mouldable metallic strip near the upper margin, where it covers the nose and the cheekbone. Exhaled aerosols get directed through the gap between the skin and the top margin of the respirator.9 Exhaled humidified gases also result in fogging of the eyeglasses, which is a frequent observation of those who wear eyeglasses.9,10 In a recently reported prospective cohort study from India, all users complained of fogging when using PPE and caring for patients with COVID-19.11 It is a commonly held notion that fogging of eyeglasses indicates poor seal of the N95 respirator and vice versa. Indeed, if fogging is present, the HCW frequently makes efforts to improve the respirator fit. The absence of fogging, on the other hand, may lure the user to a false sense of security of adequate seal.
There is currently no literature available that provides information on the relationship between fogging of eyeglasses and the adequacy of an N95 respirator seal. We hypothesize that fogging of eyeglasses while wearing an N95 respirator indicates poor fit. If that is proven, fogging of eyeglasses may be used as a point-of-care test in addition to the USC for determining the adequacy of the N95 respirator seal. To study this, we checked for fogging of eyeglasses followed by QnFT on healthy volunteers.
Materials and Methods
The study protocol was approved by the South Eastern Sydney Local Health District Human Research and Ethics Committee. All HCWs who had training in the use of PPE were eligible to participate in the study. Men with a beard or HCW with hypersensitivity to isopropyl alcohol were excluded. Male participants were required to be clean-shaven on the day of their participation.
The participants were recruited from August to October 2020. The participants were volunteer HCW from the Prince of Wales Hospital in Sydney, Australia. Most of the participants were nurses and junior medical officers working in the intensive care unit. The participants, therefore, were recruited using a convenience sample approach. All participants received a copy of the participant information sheet and consent form. Informed consent for participation was obtained from all participants.
The participants donned one of the three N95 respirators types commonly used in healthcare settings: a cup-shaped respirator (3M 1860), a three-panel flat-fold respirator (3M AURA™ 1870), or a duckbill respirator (Fig. 1). Due to limited availability and uncertainty in the supply of each N95 respirator during the pandemic, the allocation of respirators was not randomized. The study method is outlined in Flowchart 1.
Figs 1A to C.

Types of N95 respirators used in the study: (A) Cup-shaped (3M 1860); (B) Three-panel flat-fold (3M AURA 1870); (C) Duckbill respirator
Flowchart 1.
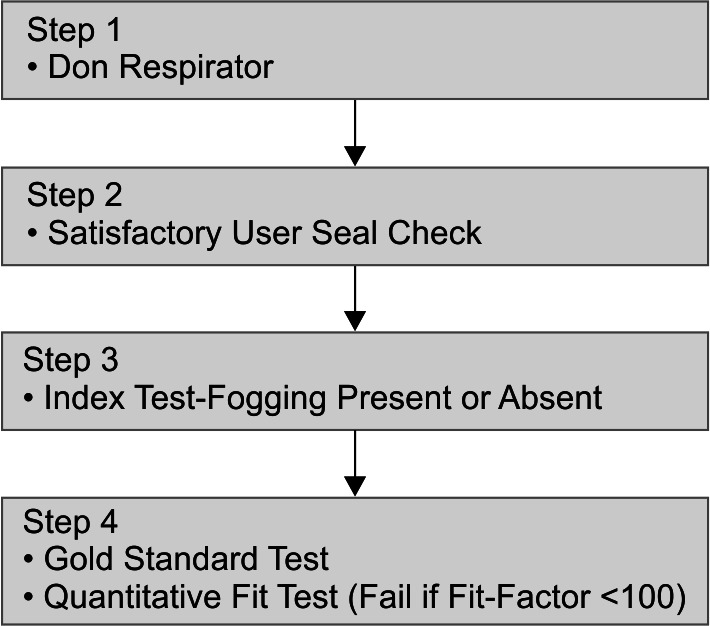
Study pathway
The study investigators ensured that each participant was conducting appropriate donning of the respirator and the “user seal check” as per the manufacturers’ recommendation. Those who failed the user seal check with all three respirators were excluded from the study.
The participants then wore plain eyeglasses, supplied by the investigators. The participants performed the following: took two deep breaths and the following activities while breathing normally—two times side to side head movement, two times up and down head movement, talking (reading two lines of a written passage), and bending forward two times. The participants self-reported if they noticed fogging of the eyeglasses (Fig. 2). As the fogging of glasses is proposed to be a point-of-care test for respirator fit, self-reporting of fogging was considered appropriate.
Fig. 2.

Fogging on the eyeglasses while wearing an N95 respirator
After testing for fogging, regardless of its presence or absence, QnFT was performed using TSI PortaCount Pro 8048 (TSI Inc. Minnesota, 55126, USA), with condensation nuclei counter method to determine a quantitative estimate of the respirator fit.12,13 A particle generator (TSI 8026, TSI Inc. Minnesota, 55126, USA) was utilized as per manufacturers’ instruction to achieve adequate ambient particle concentration. OSHA 29 CFR 1910.13414,15 protocol was used for fit testing.
According to the protocol, the participants performed a series of activities for 60 seconds each, as outlined in Box 1. These modules comprise of normal breathing with a series of activities like head movement, body movement and speaking, and also 60 seconds of deep breathing. Dividing the number of particles measured outside the respirator by the number of particles measured inside the respirator yielded the fit factor for each activity. Once all the activities were complete, an overall fit factor (FF) was calculated for the respirator using the equation shown in Equation 1.16 Higher FF indicates low concentration of particles inside the respirator and, therefore, a better seal. An overall FF ≥100 is considered to be indicative of an adequate seal for N95 respirator.17 Where the participants scored an overall FF ≥100, it was categorized as “pass” result on QnFT. An overall FF <100 was categorized as “fail”. Where the FF was greater than 200, the PortaCount assigned an FF of >200, i.e., higher values were truncated.
Box 1: OHSA 29 CFR 1910.134 quantitative fit-test protocol
ff1: Normal breathing 60 seconds
ff2: Deep breathing 60 seconds
ff3: Move head from side-to-side 60 seconds
ff4: Move head up and down 60 seconds
ff5: Read the “rainbow passage” 60 seconds
ff6: Bend forward 60 seconds
ff7: Normal breathing 60 seconds
Equation 1.

Overall fit factor (FF) calculation using quantitative fit test. ff1, fit factor normal breathing; ff2, deep breathing; ff3, head side to side; ff4, head up and down; ff5, reading aloud, ff6, bending over and ff7, normal breathing again.
Statistical Plan
Our null hypothesis is that fogging of eyeglasses does not predict “fail” result on QnFT. The descriptive statistics on the demographic data was done using Microsoft Excel and the inferential statistics was done using GraphPad Prism (San Diego, California, USA).
QnFT is the gold standard test. It determines if there is a leak around the respirator. Fogging is the index text. We tested how the index test (fogging) compared to the gold standard test (QnFT).
True positives are indicated by presence of fogging and “leak present” (fail) result on QnFT. True negatives are indicated by absence of fogging and “leak absent” (pass) on QnFT. The 2×2 contingency table was constructed. Sensitivity, specificity, and positive likelihood ratio are reported.
A receiver operating characteristic (ROC) curve was then constructed to graphically demonstrate the utility of fogging as a diagnostic test for poor respirator fit, when compared to QnFT.
Results
Seventy healthy volunteers participated in the study from August to October 2020. The demographic characteristics of the participants is listed in Table 1. The following three categories of N95 respirators were used—duckbill (n = 29, 41%), cup-shaped (3M 1860, n = 22, 31%), and three-panel flat-fold (3M Aura 1870, n = 19, 27%) respirators.
Table 1.
Participant characteristics and the respirators used
| Participant Characteristic | Number (%) |
|---|---|
| Number of participants | 70 |
| Number male (%) | 22 (31%) |
| BMI (SD) | 25.0 (4.31) |
| Age in years n (%) | |
| <30 | 26 (37%) |
| 30–50 | 34 (49%) |
| >50 | 10 (14%) |
| Ethnicity n (%) | |
| Asian | 19 (27%) |
| Caucasians | 49 (70%) |
| Other | 2 (3%) |
| N95 respirator used | |
| Duckbilled (ProShield$ medium or Halyards# Fluidshield) | 29 (41%) |
| Cup-shaped (3M 1860*) | 22 (31%) |
| 3 panel flat-fold (3M 1870*) | 19 (27%) |
The mean particle count in the room where research was carried out was 324/cm3 (SD 143). All participants had a satisfactory fit on user seal check. Forty-four (63%) participants experienced fogging of eyeglasses. Thirty-five (50%) participants had leak detected on QnFT, meaning that the overall FF was <100.
The 2 × 2 contingency table to evaluate the diagnostic value of fogging of eyeglasses (index test) to predict leak of the respirator on QnFT (gold standard test) was constructed as shown in Table 2 and Figure 3.
Table 2.
2 × 2 contingency table for all participants
| Leak (determined by quantitative fit test) | ||||||||
|---|---|---|---|---|---|---|---|---|
| QnFT fail (leak present) | n | QnFT pass (leak absent) | n | Row total | ||||
| Bedside screening test (fogging) | Positive (fogging present) | True-positive | a = | 25 | False-positive (Type I error) | c = | 19 | a + c = 44 |
| Negative (fogging absent) | False-negative (Type II error) | b = | 10 | True-negative | d = | 16 | b + d = 26 | |
| Column total | a + b = | 35 | c + d = | 35 | ||||
Formulas: Sensitivity = a/(a + c), specificity = d/(c + d), positive likelihood ratio = sensitivity/(1 − specificity), negative likelihood ratio = (1 − sensitivity)/specificity
Fig. 3.
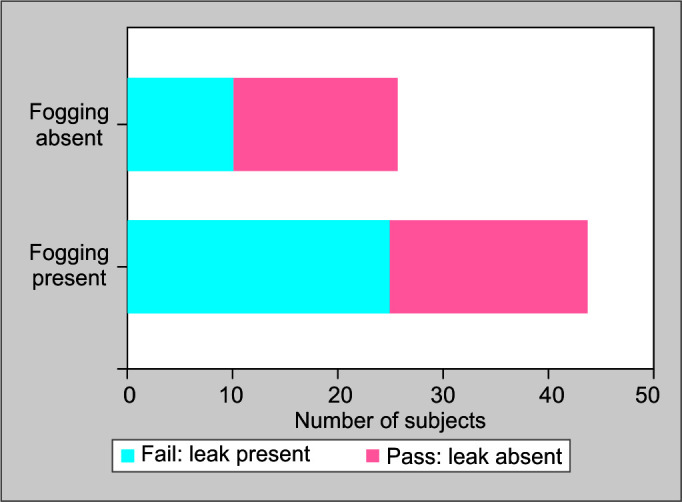
Relationship between fogging and QnFT
The presence of fogging had a sensitivity of 71% (95% CI 54–85%) and a specificity of 46% (95% CI 29–63%) to detect “fail” result on QnFT (Table 3). The odds ratio of fogging as a predictor for “fail” result on QnFT was 2.10 (95% CI 0.78–5.67), with two-tailed p-value of 0.22 (not significant).
Table 3.
Analysis of the 2 × 2 contingency table for the utility of fogging as an index test for all participants
| Statistic | Value | 95% CI |
|---|---|---|
| Sensitivity | 71% | 54–85% |
| Specificity | 46% | 29–63% |
| Positive likelihood ratio | 1.32 | 0.91–1.9 |
| Odds ratio | 2.10 | 0.78–5.67 |
| p-value (2-tailed) | 0.22 | Not significant |
The ROC curve for fogging as a diagnostic test for “fail” result on QnFT is shown in Figure 4. The area under the curve is 0.586, indicating that presence of fogging is neither a sensitive nor a specific test for fail result on QnFT.
Fig. 4.
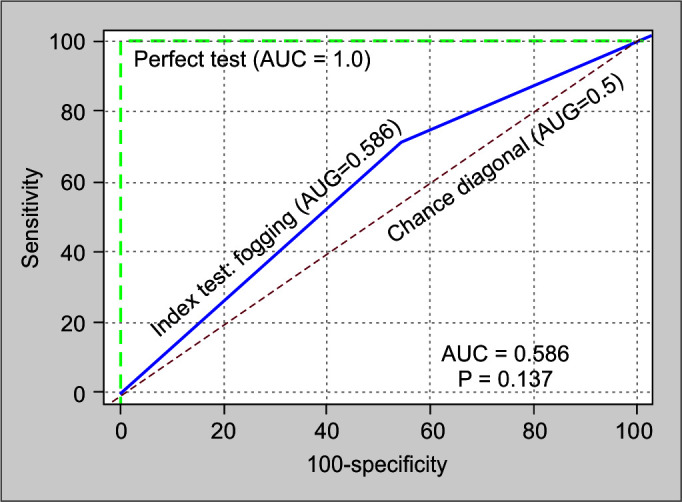
ROC curve for fogging as a diagnostic test for leak of a N95 respirator
Contingency table was constructed for all three types of respirators (duckbill, cup-shaped and three-panel flat-fold respirator). Since this is a pilot study, the number of participants was small. Fogging did not predict leak from N95 respirator for any of the categories of the respirators used.
Discussion
Fogging of the eyeglasses is commonly encountered occurrence when wearing N95 respirators.11 In our study, 62% of the participants experienced fogging. We hypothesized that the presence of fogging of eyeglasses when worn with an N95 respirator should predict poor respirator fit. Our pilot study showed that not to be the case.
Our results show that in a person wearing the N95 respirator, presence of fogging of the eyeglasses has low sensitivity (71%) for presence of leak. As a result, a significant number of users will not have fogging of the eyeglasses despite poor N95 respirator fit. It is possible that this was related other sites commonly implicated to have a leak, including both cheeks and the chin.18
In addition, the presence of fogging has low specificity (46%). As a result, a significant proportion of users will have fogging despite a good respirator fit. This is in keeping with observations using infrared camera, which shows that exhalation leak around the nasal and malar regions is commonly observed even when the participant passes the QnFT.19
This is a pilot study; therefore, the results need to be replicated in larger studies. There are a variety of respirators in clinical use around the world at the time of the COVID-19 pandemic. The diagnostic value of fogging may be different among the respirators and among people of different body habitus, facial structure, and racial background.
In this time of COVID-19 pandemic, the importance of safety of the HCW cannot be overstated.20 It is important that the respirator used is a good fit for the user. There is no reliable point-of-care test to confirm absence of leak around a respirator.21,22 It is a commonly held belief among HCW that if there is fogging of the eyeglasses, the respirator fit is not adequate. Based on our pilot study, this assumption cannot be made. Even more dangerous is the sense of security from the belief that if there is no fogging of the eyeglasses, then the respirator fit is satisfactory. Reliance on this indicator for good respirator fit may result in an increase in the risk of transmission of airborne infections like COVID-19 to HCW.
For the health safety policymakers, it is important that their HCW workforce undergoes the recommended fit testing to identify the respirator that fits their face. However, due to lack of availability of resources, very few centers are doing it currently.3,22 A reliable point-of-care diagnostic test for leak around the respirators, however, is urgently needed.
Our study has several strengths. First, this is the first study to have systematically evaluated the diagnostic value of presence of fogging over the eyeglasses as a diagnostic test for poor respirator fit.
Second, we used a QnFT which is the gold standard method, to compare the diagnostic utility. The qualitative fit tests, which are more widely used, are reliant on the participant's ability to taste a sweet or bitter aerosol and do not give a FF.23 Third, the testing was done in a designated room, and the particle count in the room was maintained within the range required for satisfactory fit testing using a particle generator. Finally, heterogeneity in the size of eyeglasses that participants used was eliminated by providing them with plain eyeglasses of the same dimension. We used the same maneuvers with the eyeglasses as those used in the QnFT.
Our study is a pilot study and suffers from several limitations. It has all the limitations of a convenience sample, which had a higher proportion of females, had lower BMI25 as compared to general population, and were mostly Caucasians or Asians.24,25 It is known that the respirator fit pass rate vary with ethnicity.26,27 Similarly, we only tested for three respirators. Therefore, the results may be different among other N95 respirators. We did not assess or ensure if the elastic headband of the respirator was adequately tight. Due to limited availability and uncertainty in the supply of each N95 respirator during the pandemic, the allocation of respirators was not randomized.
Conclusion
Fogging of eyeglasses is neither a sensitive nor a specific predictor for poor fit of N95 respirators. There is an urgent need to find a good point-of-care test for a proper fit that the HCW can use after donning an N95 respirator. We hoped that fogging of eyeglasses may be a quick, easy, and inexpensive screening test, but this pilot study failed to confirm our hypothesis.
Acknowledgments
The authors acknowledge the help and advice of Mr. Ricardo Maldonado of Power Stats (West Ryde, New South Wales, Australia. www.powerstats.com.au) in doing the statistics for this study.
Footnotes
Source of support: Nil
Conflict of interest: Dr. Arora is the Director of Quiz Time in Critical Care PTY Ltd, Sydney, Australia; which runs the website www.gotheextramile.com - MCQ in Critical Care. Dr. Arora is not paid any salary for his work with Go the Extra Mile.
Orcid
Sandy Kyaw https://orcid.org/0000-0003-4750-652X
Moira Johns https://orcid.org/0000-0001-5532-1723
Rimen Lim https://orcid.org/0000-0002-3552-1856
Warren C Stewart https://orcid.org/0000-0003-3048-9516
Natalia Rojas https://orcid.org/0000-0002-7725-8988
Solomon R Thambiraj https://orcid.org/0000-0001-5107-9060
Yahya Shehabi https://orcid.org/0000-0003-4707-7462
Sumesh Arora https://orcid.org/0000-0002-2065-3522
References
- 1.Sozkes S. COVID-19 and respiratory protection for healthcare providers. Int J Occup Med Environ Health. 2021;34(2):307–318. doi: 10.13075/ijomeh.1896.01666. DOI: [DOI] [PubMed] [Google Scholar]
- 2.Tirupathi R, Bharathidasan K, Palabindala V, Salim SA, Al-Tawfiq JA. Comprehensive review of mask utility and challenges during the COVID-19 pandemic. Infez Med. 2020;28(Suppl. 1):57–63. Pubmed ID: [PubMed] [Google Scholar]
- 3.Haji JY, Subramaniam A, Kumar P, Ramanathan K, Rajamani A. State of personal protective equipment practice in Indian Intensive Care Units amidst COVID-19 pandemic: a nationwide survey. Indian J Crit Care Med. 2020;24(9):809–816. doi: 10.5005/jp-journals-10071-23550. DOI: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Qian Y, Willeke K, Grinshpun SA, Donnelly J, Coffey CC. Performance of N95 respirators: filtration efficiency for airborne microbial and inert particles. Am Ind Hyg Assoc J. 1998;59(2):128–132. doi: 10.1080/15428119891010389. DOI: [DOI] [PubMed] [Google Scholar]
- 5.Australian Guidelines for the Prevention and Control of Infection in Healthcare. Canberra: Commonwealth of Australia, National Health and Medical Research Council (2019); 2019. Available from: https://www.safetyandquality.gov.au/sites/default/files/2020-06/infections_control_guidelines_update1_4.pdf .
- 6.Regli A, Sommerfield A, von Ungern-Sternberg BS. The role of fit testing N95/FFP2/FFP3 masks: a narrative review. Anaesthesia. 2021;76(1):91–100. doi: 10.1111/anae.15261. DOI: [DOI] [PubMed] [Google Scholar]
- 7.Lam SC, Lee JK, Yau SY, Charm CY. Sensitivity and specificity of the user-seal-check in determining the fit of N95 respirators. J Hosp Infect. 2011;77(3):252–256. doi: 10.1016/j.jhin.2010.09.034. DOI: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Derrick JL, Chan YF, Gomersall CD, Lui SF. Predictive value of the user seal check in determining half-face respirator fit. J Hosp Infect. 2005;59(2):152–155. doi: 10.1016/j.jhin.2004.09.009. DOI: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kolewe EL, Stillman Z, Woodward IR, Fromen CA. Check the gap: facemask performance and exhaled aerosol distributions around the wearer. PLoS One. 2020;15(12):e0243885. doi: 10.1371/journal.pone.0243885. DOI: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chawla G, Abrol N, Kakkar K. Personal protective equipment: a Pandora's Box. Indian J Crit Care Med. 2020;24(5):371–372. doi: 10.5005/jp-journals-10071-23443. DOI: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Choudhury A, Singh M, Khurana DK, Mustafi SM, Ganapathy U, Kumar A, et al. Physiological effects of N95 FFP and PPE in healthcare workers in COVID intensive care unit: a prospective cohort study. Indian J Crit Care Med. 2020;24(12):1169–1173. doi: 10.5005/jp-journals-10071-23671. DOI: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.PORTACOUNT RESPIRATOR FIT TESTER 8048 2021. Available from: https://www.tsi.com/products/respirator-fit-testers/portacount-respirator-fit-tester-8048/
- 13.Noti JD, Lindsley WG, Blachere FM, Cao G, Kashon ML, Thewlis RE, et al. Detection of infectious influenza virus in cough aerosols generated in a simulated patient examination room. Clin Infect Dis. 2012;54(11):1569–1577. doi: 10.1093/cid/cis237. DOI: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.OSHA. Fit testing procedures (Mandatory). Personal protective equipment. Occupational safety and health standards 2004
- 15.Respiratory protection–OSHA. Final rule; request for comment on paperwork requirements. https://www.osha.gov/laws-regs/federalregister/1998-01-08. Fed Regist. 1998;63(5):1152–1300. [PubMed] [Google Scholar]
- 16.Incorporated T. TSI Incorporated / 500 Cardigan Road / Shoreview, MN 55126 / USA2015. Revision P ed. PORTACOUNT® PRO 8030 AND PORTACOUNT® PRO+ 8038 RESPIRATOR FIT TESTERS; pp. 87–9. p. [Google Scholar]
- 17.Clayton M, Vaughan N. Fit for purpose? The role of fit testing in respiratory protection. Ann Occup Hyg. 2005;49(7):545–548. doi: 10.1093/annhyg/mei046. DOI: [DOI] [PubMed] [Google Scholar]
- 18.Lei Z, Yang J, Zhuang Z, Roberge R. Simulation and evaluation of respirator faceseal leaks using computational fluid dynamics and infrared imaging. Ann Occup Hyg. 2012;57(4):493–506. doi: 10.1093/annhyg/mes085. DOI: [DOI] [PubMed] [Google Scholar]
- 19.Roberge RJ, Monaghan WD, Palmiero AJ, Shaffer R, Bergman MS. Infrared imaging for leak detection of N95 filtering facepiece respirators: a pilot study. Am J Ind Med. 2011;54(8):628–636. doi: 10.1002/ajim.20970. DOI: [DOI] [PubMed] [Google Scholar]
- 20.Peres D, Boleo-Tome JP, Santos G. Respiratory and facial protection: current perspectives in the context of the COVID-19 pandemic. Acta Med Port. 2020;33(9):583–592. doi: 10.20344/amp.14108. DOI: [DOI] [PubMed] [Google Scholar]
- 21.Williams DL, Kave B, Lee K, Segal R, Krieser RB, Mezzavia PM, et al. A randomised crossover study to compare the user seal check and quantitative fit test between two types of duckbill N95 particulate respirator masks: The Halyard Fluidshield® N95 and the BSN Medical ProShield® N-95 particulate respirator masks. Anaesth Intensive Care. 2021;49(2):112–118. doi: 10.1177/0310057X20974022. DOI: [DOI] [PubMed] [Google Scholar]
- 22.Kapoor A, Baronia AK, Azim A, Agarwal G, Prasad N, Mishra R, et al. Breathability and safety testing of personal protective equipment: “Human-comfort” factor remains undefined. Indian J Crit Care Med. 2021;25(1):12–15. doi: 10.5005/jp-journals-10071-23598. DOI: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lee K, Slavcev A, Nicas M. Respiratory protection against Mycobacterium tuberculosis: quantitative fit test outcomes for five type N95 filtering-facepiece respirators. J Occup Environ Hyg. 2004;1(1):22–28. doi: 10.1080/15459620490250026. DOI: [DOI] [PubMed] [Google Scholar]
- 24.Mainous AG, Hougland JG. Survey sampling issues in primary care research. Fam Med. 1991;23(7):539–543. Pubmed ID: [PubMed] [Google Scholar]
- 25.Summers S. Selecting the sample for a research study. J Post Anesth Nurs. 1991;6(5):355–358. Pubmed ID: [PubMed] [Google Scholar]
- 26.Wilkinson IJ, Pisaniello D, Ahmad J, Edwards S. Evaluation of a large-scale quantitative respirator-fit testing program for healthcare workers: survey results. Infect Control Hosp Epidemiol. 2010;31(9):918–925. doi: 10.1086/655460. DOI: [DOI] [PubMed] [Google Scholar]
- 27.Green S, Gani A, Bailey M, Brown O, Hing CB. An analysis on fit-testing of Respiratory Protective equipment in the UK during the initial response to the Covid-19 pandemic. J Hosp Infect. 2021;113:180–186. doi: 10.1016/j.jhin.2021.04.024. DOI: [DOI] [PMC free article] [PubMed] [Google Scholar]