

Abstract
Background.
Roughly one in ten American adults have used hallucinogens, and emerging evidence suggests that the prevalence of use is increasing. However, our understanding of the degree to which individuals “specialize” in the use of a particular hallucinogen or are poly-hallucinogen users remains incomplete.
Methods.
This study examined data from 6,381 individuals reporting past-year hallucinogen use in the 2016–2018 National Survey on Drug Use and Health. Logistic regression examined the association between the number of distinct hallucinogens used and psychosocial/behavioral risks, and latent class analysis (LCA) characterized subgroups of hallucinogen users.
Results.
The vast majority of hallucinogen users, roughly 70%, are not “specialists” who use only one hallucinogen type; rather, lifetime poly-hallucinogen use is the norm. Critically, however, we also see that important differences exist within the population of hallucinogen users—half (51%) could be classified as LSD-Mushroom-Ecstasy users only (this group was disproportionally comprised of youth), nearly one third (30%) were Poly-Hallucinogen users (this group was disproportionately male and non-Hispanic White), and smaller proportions were limited primarily to use of LSD-Mushrooms (6%; these individuals were almost exclusively ages 35 and older) or Ecstasy Only (12%; these individuals were mostly younger adults ages 18–34).
Conclusions.
Findings provide a fresh contribution to our understanding of poly-hallucinogen use in a time in which local and state governmental leaders, and people across the country, weigh the benefits and drawbacks of legalizing specific hallucinogenic drugs.
Keywords: hallucinogens, poly-hallucinogen use, risk behavior, drugs
Introduction
The use of hallucinogens in the United States (US) is surprisingly common. Indeed, it is estimated that roughly one in ten adults—more than thirty million Americans—report lifetime hallucinogen use (Krebs & Johansen, 2013; Shalit et al., 2019; Yockey et al., 2019). And, critically, a growing body of evidence suggests that hallucinogen use is on the rise. Evidence from the National Survey on Drug Use and Health (NSDUH) indicates that the past-year prevalence of Lysergic acid diethylamide (LSD) use in the US increased by more than 200% between 2002 and 2018 (from 0.2% in 2002–2005 to 0.7% in 2015–2018) (Killion et al., 2021; Yockey et al., 2020).
In general terms, it has been widely observed that individuals who misuse one psychoactive substance are more likely to misuse other substances as well (Salas-Wright et al., 2016; Vaughn et al., 2014). For hallucinogens in particular, prior research indicates that individuals who use hallucinogens are more likely than non-users to use cannabis and other illicit substances (Ford et al., 2011; Shalit et al., 2019; Wu et al., 2006). Additionally, there is evidence that some hallucinogen users partake in poly-hallucinogen use—or the use of more than one type of hallucinogen (Wish et al., 2006). For instance, Wu and colleagues (2011) found that Salvia divinorum use is particularly elevated among LSD, ecstasy, and phencyclidine users. Similarly, Palamar and colleagues (2017) found that, among ecstasy users, past-year use of LSD, ketamine, and DMT is elevated and increasing.
Prior research has made valuable contributions to our understanding of hallucinogen use, and studies have begun to explore the prevalence and correlates of poly-hallucinogen use. However, important research shortcomings persist. For instance, most studies looking at poly-hallucinogen use have been restricted to only a handful of hallucinogen types. Yet, given the broad array of substances that exist across the spectrum of hallucinogens (Bogenschutz & Johnson, 2016; Vollenweider, 2001), such a narrow frame does not provide a sufficiently comprehensive picture of how hallucinogens are used. Similarly, prior work has relied mostly on variable-centered approaches rather than person-centered methodologies, thereby limiting our understanding of how poly-hallucinogen use manifests among individuals. Third, working from a framework of self-medication (Khantzian, 1997; Markou et al., 1998) and self-regulation/control (Delisi & Vaughn, 2014; Salas-Wright et al., 2016), there is a need to systematically examine how patterns of hallucinogen use relate to key psychological and behavioral outcomes. The basic theoretical position here is that some individuals who misuse drugs (such as hallucinogens) do so, in part, to alleviate psychological distress (i.e., the self-medication hypothesis) and/or may be involved in other risky/antisocial behaviors due to overall challenges related to emotion regulation and decision making (i.e., self-control/regulation hypothesis).
In sum, a number of important questions remain largely unanswered such as: Are hallucinogen users generalists or specialists in their use? And, are the demographic, psychological, and behavioral characteristics of different “types” of hallucinogen users distinct? In the present study, we address these questions in several ways. We begin by providing new evidence on the prevalence of use of the eight most commonly-used hallucinogens—and examine their association with key demographic, psychological, and behavioral factors—among hallucinogen users in a large nationally representative sample in the US. Additionally, we use a person-centered approach, latent class analysis (LCA), which allows us to model a typology of hallucinogen users and, in turn, examine the relationship between particular hallucinogen user subtypes and key mental health, substance use, and criminal justice system outcomes.
Method
2.1. Sample and Procedures
This study drew from public-use data collected between 2016 and 2018 as part of the NSDUH (SAMHSA, 2019). The NSDUH provides population estimates for an array of substance use and health-related behaviors in the US general population using multistage area probability sampling methods. Each independent, cross-sectional NSDUH sample is considered representative of the non-institutionalized population ages 12 and older. To improve the precision of subgroup estimates, adolescents (ages 12–17) and young adults (ages 18–25) were oversampled.
The present study’s analytic sample was limited to participants reporting past-year hallucinogen use (N = 6381). Data from 2016, 2017, and 2018 were pooled to improve estimates and model stability. Recent documentation from SAMHSA indicates that the NSDUH’s screening response rate in recent years was >70% and interview response rate >60%, yielding an overall response rate of ~50%. All estimates were adjusted to account for the NSDUH’s complex probability sampling design. The design and methods are summarized briefly here, but a fuller description of NSDUH procedures is available elsewhere (see Substance Abuse and Mental Health Services Administration, 2019 and https://nsduhweb.rti.org/).
2.2. Measures
2.2.1. Hallucinogen use.
Hallucinogen use was measured by asking participants if they ever used “hallucinogens,” which are described in the NSDUH survey as drugs that “often cause people to see or experience things that are not real.” As part of this question, participants were provided with a list of hallucinogenic substances (i.e., LSD/acid, psilocybin/mushrooms, mescaline/peyote, DMT/foxy, ecstasy/molly, PCP/ozone, ketamine, salvia divinorum) and asked to report any instances of the use of these specific substances in their lifetime. In turn, individuals who reported lifetime use of one or more hallucinogens were asked about any past-year hallucinogen use in general—those reporting past-year use were classified as hallucinogen users and were included in the sample. It should be noted that the battery of questions in the NSDUH survey includes a broad array of substances (e.g., ecstasy/molly) beyond the narrow list of “classical” hallucinogens (Johnson et al., 2006); we view this as advantageous as it allows us to model a broad array of substances with hallucinogenic properties.
2.2.2. Psychological and behavioral factors.
Self-reported dichotomous (no, yes) psychosocial/behavioral correlates were examined.
Depression was measured in terms of past-year major depressive episodes based on criteria from the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association, 2000).
Other drug use refers to past-year use of any illicit drug other than hallucinogens (i.e., cannabis, stimulants, opiates) and/or the misuse of prescription pain relievers.
Criminal justice involvement was measured in terms of past-year being “arrested and booked” for breaking the law excluding minor traffic violations.
2.2.3. Sociodemographic variables.
Commonly used sociodemographic variables were also examined and included as indicator covariates in the latent modeling: age, gender, race/ethnicity, and household income (e.g., Killion et al., 2021; Salas-Wright et al., 2021).
2.3. Statistical Analysis
All statistical analyses were weighted to abide by the Substance Abuse and Mental Health Data Archive’s (SAMHDA) guidelines, accounting for the NSDUH’s stratified cluster sampling design (SAMHDA, 2014). All analyses were conducted using Stata 16MP (StataCorp, 2019) or Latent Gold (Vermunt & Magidson, 2016).
First, among the sample of past-year hallucinogen users, we present the survey adjusted prevalence estimates with 95% confidence intervals (CIs)—using Stata 16’s svyset command and svy prefix—for lifetime use of specific hallucinogens overall and by demographic and psychological/behavioral subgroup (see Table 1). Additionally, we examined the proportion of past-year hallucinogen users reporting lifetime use of 1–8 distinct hallucinogen types (see Figure 1). In turn, using logistic regression and controlling for demographic confounds, we examined the association between the number of distinct hallucinogens used and the risk of depression, other drug use, and criminal justice system involvement.
Table 1.
Prevalence of lifetime hallucinogen type use among hallucinogen users.
|
|
||||||||||||||||
| LSD | Mushrooms | Peyote | DMT | Ecstasy | PCP | Ketamine | Salvia | |||||||||
|
| ||||||||||||||||
| % | CI | % | CI | % | CI | % | CI | % | CI | % | CI | % | CI | % | CI | |
| Full Sample | 64.3 | 62.5–66.0 | 62.3 | 60.5–64.1 | 12.8 | 11.6–14.1 | 18.2 | 17.1–19.4 | 71.8 | 70.0–73.5 | 7.8 | 6.6–9.0 | 17.9 | 16.6–19.4 | 24.1 | 22.5–25.8 |
|
Demographic Factors | ||||||||||||||||
| Age | ||||||||||||||||
| 12–17 (ref) | 52.9 | 48.8–57.0 | 39.1 | 33.8–44.6 | 4.5 | 3.2–6.1 | 10.0 | 7.7–.9 | 43.4 | 39.6–47.3 | 7.3 | 5.2–10.3 | 7.2 | 5.4–9.6 | 6.8 | 5.2–9.0 |
| 18–25 | 65.5 | 63.4–67.5 | 58.7 | 56.5–60.9 | 6.5 | 5.5–7.6 | 17.2 | 15.6–19.0 | 70.5 | 68.3–72.6 | 3.3 | 2.7–4.1 | 11.7 | 10.6–13.0 | 20.4 | 18.6–22.2 |
| 26–34 | 58.9 | 54.9–62.7 | 69.6 | 65.9–73.2 | 15.0 | 12.7–17.6 | 19.9 | 17.4–22.7 | 86.4 | 83.3–89.0 | 8.6 | 6.5–11.3 | 26.6 | 23.0–30.4 | 39.5 | 35.7–43.5 |
| 35–49 | 77.5 | 72.4–81.9 | 77.4 | 71.5–82.4 | 26.9 | 21.8–32.7 | 22.8 | 18.7–27.5 | 80.0 | 74.2–84.8 | 14.5 | 11.0–18.7 | 32.5 | 26.4–39.4 | 22.0 | 17.2–27.7 |
| 50 and older | 73.8 | 60.1–84.1 | 64.2 | 52.4–74.5 | 44.5 | 32.7–56.9 | 22.9 | 14.2–34.8 | 36.5 | 24.5–50.4 | 30.5 | 19.7–44.1 | 15.2 | 7.4–28.6 | 10.6 | 4.6–22.6 |
| Sex | ||||||||||||||||
| Female (ref) | 57.7 | 55.4–60.0 | 53.0 | 50.2–55.8 | 10.3 | 8.3–12.6 | 14.5 | 12.4–16.9 | 72.3 | 69.7–74.8 | 7.2 | 5.6–9.2 | 15.0 | 13.0–17.3 | 15.8 | 13.7–18.3 |
| Male | 68.1 | 66.2–69.9 | 67.7 | 65.3–70.0 | 14.3 | 12.6–16.1 | 20.4 | 18.9–21.9 | 71.4 | 68.9–73.9 | 8.1 | 6.6–9.8 | 19.6 | 17.5–21.9 | 28.9 | 26.7–31.1 |
| Race/Ethnicity | ||||||||||||||||
| White (ref) | 70.8 | 69.0–72.5 | 70.1 | 68.2–71.9 | 14.0 | 12.5–15.7 | 20.7 | 19.0–22.5 | 71.3 | 68.9–73.5 | 7.5 | 6.1–9.1 | 19.6 | 17.5–21.8 | 27.8 | 25.9–29.7 |
| Black | 32.9 | 28.2–38.1 | 25.1 | 20.6–30.2 | 6.0 | 3.9–9.2 | 7.2 | 4.7–10.8 | 76.1 | 70.2–81.1 | 10.4 | 6.5–16.2 | 7.7 | 4.8–12.1 | 7.4 | 4.5–12.1 |
| Asian | 47.5 | 39.5–55.6 | 48.4 | 37.1–59.9 | 8.9 | 3.1–23.1 | 8.0 | 4.6–13.6 | 74.3 | 65.0–81.8 | 3.4 | 1.4–7.7 | 13.5 | 7.1–24.3 | 13.2 | 7.4–22.5 |
| Hispanic | 60.5 | 55.5–65.3 | 53.5 | 48.4–58.6 | 11.3 | 8.8–14.4 | 16.5 | 13.4–20.2 | 71.5 | 67.6–75.1 | 9.0 | 6.8–11.9 | 17.1 | 13.6–21.2 | 20.7 | 16.2–26.0 |
| Other | 60.1 | 53.6–66.2 | 63.8 | 56.5–70.5 | 17.2 | 12.5–23.3 | 19.2 | 14.5–25.0 | 69.1 | 61.0–76.1 | 7.1 | 4.3–11.6 | 21.0 | 15.9–27.2 | 25.4 | 19.9–31.8 |
| Household Income | ||||||||||||||||
| <$20,000 (ref) | 64.1 | 60.1–68.0 | 56.9 | 52.9–60.7 | 12.5 | 10.1–15.5 | 19.4 | 16.7–22.4 | 67.1 | 62.7–71.1 | 10.0 | 7.3–13.5 | 15.7 | 13.4–18.3 | 20.2 | 17.3–23.6 |
| $20,000–39,999 | 63.4 | 60.0–66.8 | 62.1 | 58.6–65.5 | 13.6 | 11.2–16.4 | 19.9 | 17.5–22.5 | 73.5 | 70.0–76.7 | 8.9 | 6.7–11.9 | 19.1 | 16.5–21.9 | 28.4 | 25.2–31.9 |
| $40,000–74,999 | 68.9 | 64.9–72.6 | 66.2 | 61.9–70.2 | 10.7 | 7.6–15.0 | 17.7 | 14.4–21.7 | 72.4 | 67.9–76.6 | 7.6 | 5.2–11.1 | 19.0 | 15.1–23.6 | 25.6 | 21.7–30.0 |
| $75,000+ | 63.2 | 60.1–66.1 | 64.9 | 61.8–67.9 | 13.2 | 10.8–15.9 | 15.7 | 13.4–18.3 | 73.3 | 69.9–76.4 | 4.8 | 3.4–6.7 | 18.0 | 14.9–21.4 | 21.9 | 19.4–24.6 |
| Psychological and Behavioral Factors | ||||||||||||||||
|
| ||||||||||||||||
| Depressive Episode | ||||||||||||||||
| No | 64.4 | 62.3–66.5 | 63.9 | 61.7–66.1 | 13.6 | 12.1–15.3 | 18.1 | 16.8–19.6 | 75.0 | 72.9–76.9 | 7.6 | 6.4–9.1 | 17.7 | 16.1–19.4 | 24.9 | 22.8–27.1 |
| Yes | 69.3 | 64.5–73.8 | 68.0 | 64.7–71.1 | 12.9 | 10.2–16.1 | 22.5 | 19.6–22.6 | 73.1 | 68.5–77.3 | 8.4 | 6.4–11.0 | 23.2 | 19.6–27.4 | 28.8 | 24.9–33.1 |
| Other Drug Use | ||||||||||||||||
| No | 59.7 | 57.1–62.3 | 58.1 | 54.4–59.7 | 11.5 | 9.9–13.4 | 14.6 | 13.2–16.1 | 62.1 | 59.7–64.5 | 6.4 | 5.2–7.7 | 11.4 | 9.7–13.2 | 19.2 | 17.4–-21 |
| Yes | 71.2 | 69.0-73.2 | 70.2 | 68.1-72.2 | 14.8 | 12.9-16.9 | 23.7 | 21.4-26.2 | 86.3 | 84.1-88.3 | 9.9 | 8.0–12.1 | 27.9 | 25.5-30.4 | 31.6 | 28.8-34.5 |
| Criminal Justice | ||||||||||||||||
| No | 64.3 | 62.5–65.9 | 62.9 | 60.9–64.8 | 12.8 | 11.5–14.2 | 17.5 | 16.1–18.9 | 70.9 | 69.0–72.6 | 6.6 | 5.5–7.9 | 17.8 | 16.4–19.4 | 23.6 | 21.9–25.4 |
| Yes | 63.1 | 57.3–68.6 | 57.5 | 53.0–61.9 | 12.6 | 9.4–16.6 | 24.1 | 19.8–29.0 | 81.0 | 77.4–84.2 | 17.8 | 13.7–22.8 | 18.8 | 14.7–23.7 | 28.6 | 25.3–32.2 |
Notes. Data from 2016–2018 are pooled. % = Percent reporting use of the corresponding hallucinogen. % in bold signifies significant difference controlling for demographic factors.
CI = 95% confidence interval. Estimates weighted for complex sampling design.
Figure 1.
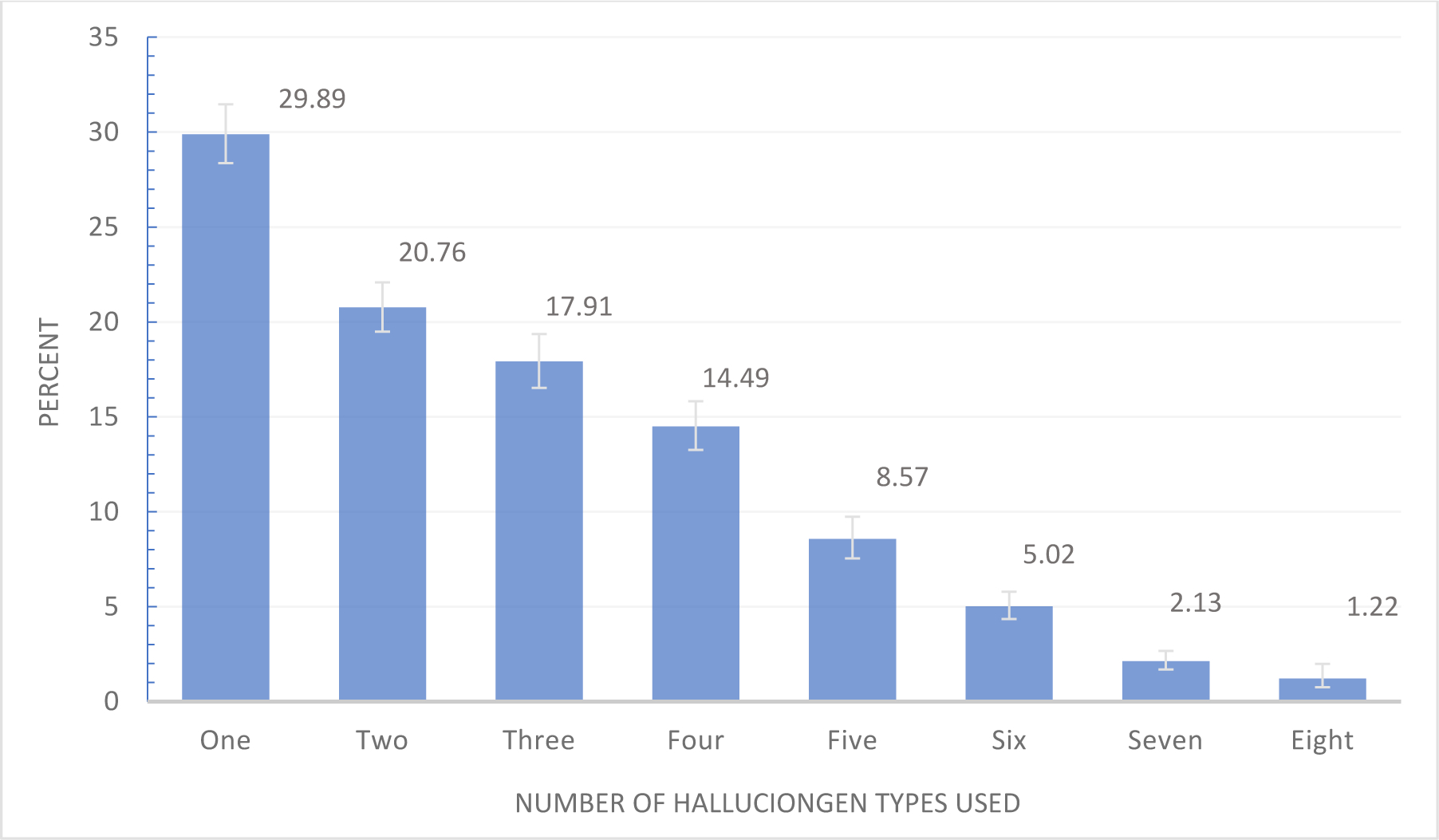
Number of distinct hallucinogens used in lifetime among hallucinogen users
Next, we conducted LCA to identify latent subgroups of hallucinogen users on the basis of the specific types of hallucinogens used. LCA is a statistical procedure that assigns individual cases to their most likely latent subgroups on the basis of observed data (McLachlan and Peel, 2004). We began by identifying a sequence of latent profile models ranging from one to six classes by using Latent GOLD® 5.1 software (Vermunt & Magidson, 2016). Five statistical criteria were used to identify the best fitting model: Bayesian Information Criterion (BIC), Akaike’s Information Criterion (AIC), Consistent Akaike’s Information Criterion (CAIC), log likelihood (LL), and entropy. Higher entropy values indicate clearer class delineation (Celeux and Soromenho, 1996). In addition to quantitative criteria, the parsimony and substantive interpretability of the latent class solutions also function as model selection criteria. We present a visual of the latent classes (see Figure 2) in which the conditional item-response probabilities are displayed as dots or points for each class/item. After modeling the latent classes, we examined the demographic characteristics of the latent classes using Stata 16 (StataCorp, 2019).
Figure 2.
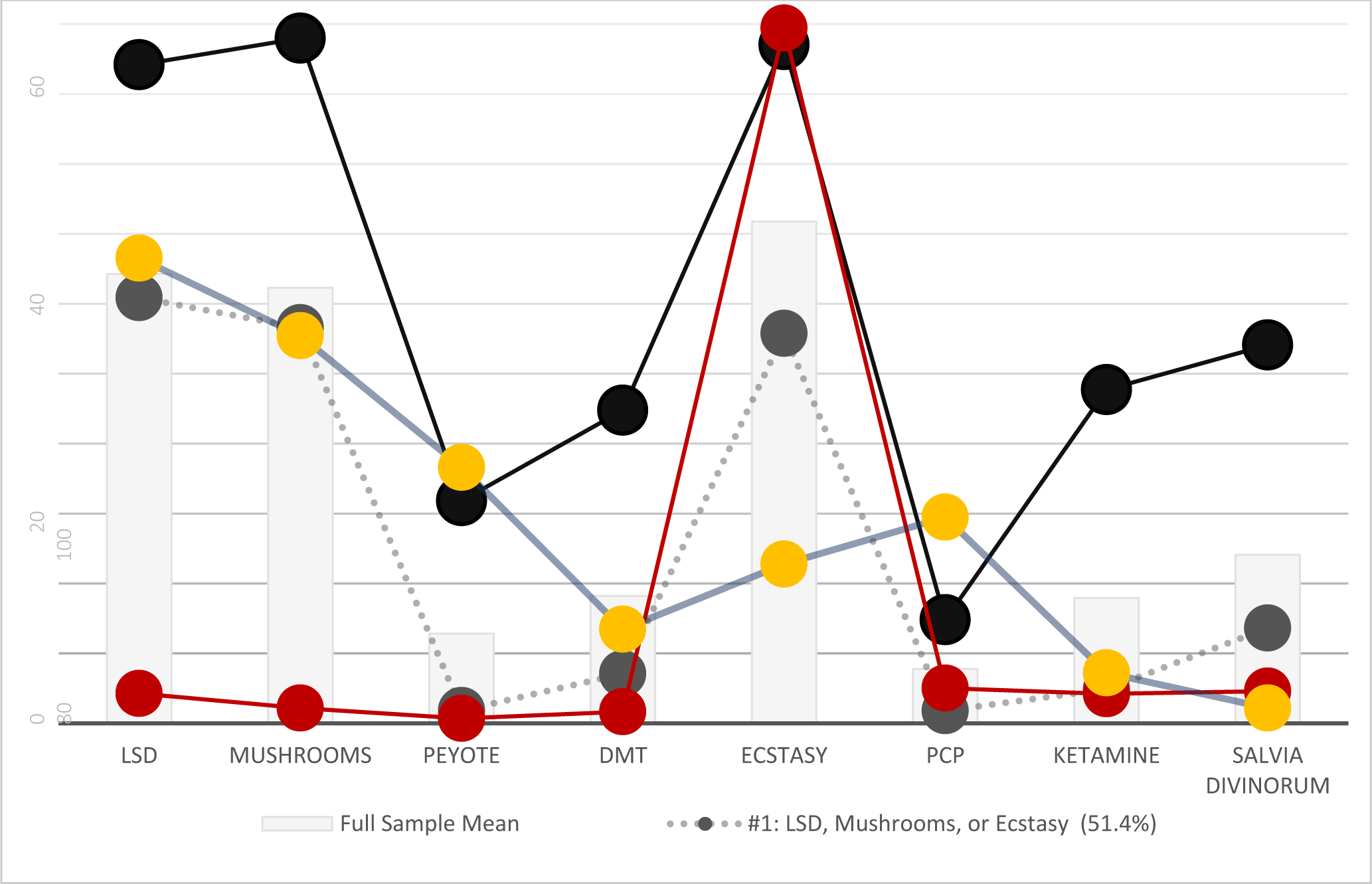
Predicted probability of hallucinogen use, by latent class
Results
3.1. Lifetime Rates of Use of Hallucinogen Types
Table 1 displays the lifetime prevalence of hallucinogen use, by hallucinogen type and by demographic and psychological/behavioral subgroup. The lifetime prevalence of specific hallucinogens use among past-year hallucinogen users was, in order: ecstasy (71.8, 95% CI = 70.0–73.5), LSD (64.3, 95% CI = 62.5–66.0), mushrooms (62.3, 95% CI = 60.5–64.1), Salvia divinorum (24.1, 95% CI = 22.5–25.8), DMT (18.2, 95% CI = 17.1–19.4), ketamine (17.9, 95% CI = 16.6–19.4), peyote (12.8, 95% CI = 11.6–14.1), and PCP (7.8, 95% CI = 6.6–9.0).
3.2. Lifetime Rates by Demographic and Psychological/Behavioral Subgroup
In terms of demographic factors, we see that—among current hallucinogen users—lifetime ecstasy users were more likely to be between the ages of 18 and 49 (compared to adolescents, ages 12–17) but no other demographic differences were observed for gender, race/ethnicity, or household income. Lifetime LSD users were likely to be older (compared to adolescents, ages 12–17), male, and non-Hispanic White. A similar pattern was identified for mushroom users with the exception that there was no significant difference identified between non-Hispanic White and participants of “other” race/ethnicity. Lifetime Salvia divinorum users tended to be adults (ages 18–49, in contrast to adolescents) and more likely to be male and reside in households earning between $20,000 and $39,999 per year. Lifetime DMT users were more likely to be 18 or older and male, and less likely to be non-Hispanic Black or Asian. Lifetime ketamine users were more likely to be ages 18 and older and male, and less likely to be non-Hispanic Black. With respect to peyote, lifetime users were more likely to be age 26 or older, male, and less likely to be non-Hispanic Black (compared to non-Hispanic White). Finally, lifetime PCP users were less likely to reside in households earning more than $75,000 per year and to be ages 18–25 and more likely to be 35 or older.
We see several distinct patterns in terms of psychological and behavioral factors. Among current hallucinogen users, we see that individuals reporting a past-year depressive episode and other illicit drug use were more likely to endorse lifetime LSD, mushroom, and ketamine use. We also see that those reporting only other illicit drug use were more likely to report lifetime use of peyote. Those reporting other illicit drug use and criminal justice system involvement were more likely to report higher rates of lifetime ecstasy and PCP use. And those reporting a depressive episode, other illicit drug use, and criminal justice system involvement were more likely to report DMT and Salvia divinorum use.
3.3. The Number of Distinct Hallucinogen Types Used
Figure 1 displays the proportion of current hallucinogen users reporting the lifetime use of one to eight distinct hallucinogen types—for example, someone reporting lifetime use of LSD, mushrooms, and ecstasy would have a score of three and someone only using peyote would have a score of one. The highest single category was one distinct hallucinogen used in a lifetime (29.89% of current hallucinogen users). However, notably, a majority reported using at least two distinct hallucinogens in their lifetime (70.11%) and half (49.35%) reported using three+ hallucinogens in their lifetime.
Among hallucinogen users, the distinct number of hallucinogens used was associated with the likelihood of past-year depression (AOR = 1.10, 95% CI = 1.03–1.18), other illicit drug use (AOR=1.38, 95% CI = 1.32–1.45), and arrest (AOR=1.16, 95% CI = 1.06–1.27). Examining predicted probability of each of these behavioral outcomes as a function of the number of hallucinogens used is helpful in interpreting this association. For instance, among users reporting only one hallucinogen use, the predicted probability of depression was 14.1%, but increased to 20.4% among those using two types and reached a pinnacle of 24.5% among those using six or more distinct types. A similar, albeit more robust, pattern was observed for other illegal drug use. Among those reporting using only one type of hallucinogens, the predicted probability of other illicit drug use was 22.9%, but this increased markedly among those using four (52.5%), five (55.8%), or six or more (60.4%) distinct types of hallucinogens. With respect to past year arrest, the predicted probability of arrest for hallucinogen users reporting using one or two types of hallucinogens was 7.4% and 7.5%, respectively; however, among those using five or six types, the predicted probability of other arrest increased to 11.3% and 16.1%, respectively.
3.4. Modeling the Heterogeneity of Hallucinogen Use among Current Users
Analyzing the modeling of latent class solutions suggested a four-class solution as the best-fitting model of the data (Table 2). It should be noted that the entropy values suggest that a three-class solution may be the most clearly delineated modeling of the data; however, other goodness of fit statistics suggest that a four or five class modeling may be superior and, more importantly, the three-class modeling excluded the Ecstasy Only class described below (which we determined merited inclusion in terms of substantive interpretability). Similarly, while the BIC/AIC values suggest that a five-class solution may be a slightly better fit, this included a class that was not clearly distinguishable and therefore did not satisfy the requirement of parsimony. As shown in Figure 2, the four-class modeling revealed a conceptually coherent modeling of the data.
Table 2.
Fit Indices for Latent Classes
| # Class Solution | Log Likelihood | LL | Bayesian Information Criterion | BIC | Akaike’s Information Criterion | AIC | Consistent Akaike’s Information Criterion | CAIC | Entropy R2 |
|---|---|---|---|---|---|
| 1-Class | −25921.2687 | 51912.6260 | 51858.5374 | 51920.6260 | n/a |
| 2-Class | −23398.6630 | 47007.5919 | 46845.3260 | 47031.5919 | 0.7153 |
| 3-Class | −22917.3898 | 46185.2227 | 45914.7795 | 46225.2227 | 0.7622 |
| 4-Class | −22454.7656 | 45400.1516 | 45021.5312 | 45456.1516 | 0.7321 |
| 5-Class | −22181.9615 | 44994.7208 | 44507.9230 | 45066.7208 | 0.6748 |
| 6-Class | −22051.2500 | 44873.4750 | 44278.4999 | 44961.4750 | 0.6858 |
Class #1, the LSD, Mushrooms, or Ecstasy class comprised 51.4% of the total sample of current hallucinogen users. This class was characterized by relatively elevated predicted probabilities of LSD (61%), mushroom (57%), and ecstasy use (56%) and low predicted probabilities for all other substances. As shown in Table 3, this class had the highest proportion of adolescents (ages 12–17) and young adult (18–25) respondents. Class #2, the Poly-Hallucinogen class, comprised 30.3% of the total sample of hallucinogen users and was characterized by predicted probabilities of hallucinogen use that are far above the mean observed among the full sample. Notably, the rates of LSD, mushrooms, DMT, ketamine, and Salvia divinorum for this class stood out as uniquely high among all of the classes. It should be noted that this second class had the highest proportion of male and non-Hispanic White respondents. Class #3, the Ecstasy Only class, comprised 13.3% of the sample and was characterized by a low predicted probability of lifetime use of all of the classic and dissociative hallucinogens except ecstasy. This class had the highest proportion of female, Hispanic, Asian, and non-Hispanic Black respondents and the lowest proportion of non-Hispanic white respondents. Class #4, the LSD or Mushrooms class, comprised 5.9% of the sample and was characterized by relatively elevated levels of lifetime LSD (67%) and mushroom (55%) using a combination with relatively moderate to low rates of the other hallucinogens. This class was comprised almost entirely of participants between the ages of 35 and 49 (26.6%) and 50 and older (70.7%).
Table 3:
Demographic characteristics of latent classes
| #1: LSD, Mushrooms, or Ecstasy (50.39%) | #2: Poly-Hallucinogen (30.39%) | #3: Ecstasy Only (13.28%) | #4: LSD or Mushrooms (5.94%) | ||||||
|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||
| % | CI | % | CI | % | CI | % | CI | χ2 | |
| Age | |||||||||
| 12–17 | 16.35 | (15.1–17.7) | 1.15 | (0.08–1.17) | 5.52 | (4.2–7.2) | -- | -- | |
| 18–25 | 60.24 | (58.0–62.5) | 33.56 | (30.7–36.6) | 47.13 | (42.7–51.6) | -- | -- | |
| 26–34 | 20.00 | (17.9–22.2) | 40.09 | (37.1–43.2) | 39.30 | (34.6–44.2) | 2.68 | (0.8–8.7) | 160.6*** |
| 35–49 | 3.40 | (2.5–6) | 22.78 | (20.2–25.5) | 8.06 | (5.1–12.4) | 26.60 | (19.4–35.4) | |
| 50 and older | -- | -- | 2.42 | (1.3–4.5) | -- | -- | 70.72 | (60.8–79.0) | |
| Sex | |||||||||
| Female | 37.41 | (35.1–39.7) | 24.91 | (22.0–28.0) | 55.73 | (50.3–60.9) | 47.97 | (38.2–57.9) | 31 2*** |
| Male | 62.59 | (60.2–64.9) | 75.09 | (71.9–78.0) | 44.27 | (39.0–49.6) | 52.03 | (42.1–61.8 | |
| Race/Ethnicity | |||||||||
| White | 69.53 | (67.1–71.8) | 78.50 | (74.9–81.7) | 29.65 | (25.9–33.6) | 58.88 | (47.6–63.3) | |
| Black | 5.13 | (4.3–6.1) | 2.25 | (1.4–3.5) | 34.64 | (30.1–39.5) | 14.66 | (9.0–23.0) | |
| Asian | 4.67 | (3.7–5.8) | 2.28 | (1.2–4.2) | 10.31 | (7.7–13.6) | 7.47 | (2.8–18.4) | 35.1*** |
| Hispanic | 15.55 | (13.6–17.7) | 12.07 | (9.7–14.9) | 20.86 | (17.3–24.9) | 14.69 | (9.0–23.0) | |
| Other | 5.10 | (4.4–5.9 | 4.90 | (3.7–6.4 | 4.54 | (3.2–6.4) | 4.30 | (2.1–8.4) | |
| Household Income | |||||||||
| <$20,000 | 23.65 | (21.6–25.8) | 19.77 | (17.0–22.9) | 28.60 | (24.3–33.3) | 33.39 | (25.1–42.8) | |
| $20,000–39,999 | 29.86 | (27.6–32.2) | 34.48 | (31.6–37.5) | 34.06 | (29.6–38.8) | 36.29 | (25.4–48.8) | 3.1** |
| $40,000–74,999 | 14.50 | (12.9–16.2) | 15.27 | (12.8–18.1) | 10.43 | (8.2–13.2) | 8.11 | (3.9–16.2) | |
| $75,000+ | 31.99 | (29.8–34.3) | 30.48 | (27.3–33.9) | 26.90 | (22.6–31.7 | 22.20 | (14.2–33.0) | |
Notes. Data from 2016–2018 are pooled. % = Proportion of latent class. Estimates weighted to account for complex sampling design. χ2 = Chi-square (and accompanying test of significance via p-values [*p < .05, **p< .01, *** p< .001]) to test for differences in the distribution of demographic variables between latent classes.
3.5. Psychological and Behavioral Characteristics of Latent Classes
We also examined the rates of psychological and behavioral outcomes by latent class. With regards to depression, the lowest rates were observed for Class #3 (Ecstasy Only) with only 13.45% (95% CI = 10.4–17.2) reporting a past-year depressive episode compared to significantly higher rates among those categorized into Class #1 (LSD, Mushrooms, or Ecstasy; 19.82, 95% CI = 18.1–21.6) and Class #2 (Poly-Hallucinogen; 22.48, 95% CI = 20.2–25.0). No significant differences were observed for depression between Class #1 and Class #4 (LSD or Mushrooms; 18.60, 95% CI = 10.1–31.7).
In terms of other illicit drug use, the lowest rates were observed for Class #4 (LSD or Mushrooms) with 23.85% (15.4–35.0) reporting the use of an illegal drug besides hallucinogens. No differences were observed between Class #4 and Classes #1 (LSD, Mushrooms, or Ecstasy; 34.58, 95% CI = 32.2–37.0) and #3 (Ecstasy Only; 30.85, 95% CI = 26.3–35.8). We also see that rates of other illicit drug use were markedly higher among members of Class #2 (Poly-Hallucinogen; 55.23, 51.5–58.9) than among any of the other classes.
Finally, with respect to criminal justice system involvement, the lowest rates of past year arrest were observed among members of Class #1 (LSD, Mushrooms, or Ecstasy; 8.51, 95% CI = 7.3–9.8). Members of this class were significantly less likely to report arrest than members of Class #2 (Poly-Hallucinogen; 10.69, 95% CI = 9.1–12.5) or Class #3 (Ecstasy Only; 14.11, 95% CI = 11.3–17.4). No differences were observed between Class #1 and Class #4 (LSD or Mushrooms; 9.25, 95% CI = 4.2–19.1).
Discussion
Prior research on poly-hallucinogen use has been hampered by the inclusion of a limited number of hallucinogens and sole reliance on variable centered methods. We sought to surmount these limitations in the extant literature by examining a wide array of hallucinogens, and uncovering profiles of use. Several key findings stand out.
First, we see compelling evidence that most hallucinogen users are lifetime poly-users. Indeed, fewer than one in three hallucinogen users reported having used only one hallucinogen in their lifetime—more than half of all hallucinogen users reported having used two to four distinct types of hallucinogens and one in six users reported having used five or more distinct types of hallucinogens. Notably, we also see evidence that hallucinogen users reporting the use of a greater number of distinct types of hallucinogens were characterized by a greater risk of past-year depression, other illicit drug use, and criminal justice system contact. The link between poly-hallucinogen use and depression is consistent with self-medication theorizing (Khantzian, 1997; Markou et al., 1998), which suggests that substance use may be influenced by a desire to relieve psychological distress. Additionally, the link between poly-hallucinogen use and substance misuse and criminal justice system contact is consistent with research on externalizing behavior in general—namely, that behaviors related to underlying self-regulation and self-control mechanisms (such as drug experimentation and risky/antisocial behaviors that can lead to criminal justice system involvement) tend to cluster among individuals and be informed by overlapping etiologic processes (Bresin, 2020; DeLisi & Vaughn, 2014; Salas-Wright et al., 2016). To be sure, it should be noted that this finding may be confounded by the fact that hallucinogen and other drug use is criminalized, which could be primary driver of arrest for a proportion of hallucinogen users.
Second, results from the finite mixture modeling reveal the existence of meaningfully distinct subgroups of hallucinogen users. For instance, we see that half of all hallucinogen users could be classified into an LSD, Mushrooms, or Ecstasy class. Notably, participants categorized into this class were by far the youngest of all classes and were overwhelmingly between the ages of 12 and 25. Although we can only speculate, it is plausible that this class—characterized by experimentation with higher-prevalence hallucinogens—is comprised primarily of young people who are likely to experiment with a variety of drugs, and have access to these more “mainstream” hallucinogens. Another possibility is that young people in this group may be especially attuned to discussion of the potential psychological treatment effects of hallucinogens for depression (see Carhart-Harris et al., 2021; Davis et al., 2021; Mitchell et al., 2021), and are therefore inclined to experiment with these substances to alleviate psychological distress.
We also observed that the Ecstasy Only class (characterized by near exclusive ecstasy use) was disproportionately comprised of young adults and the LSD or Mushrooms class included no participants under the age of 26 and was almost entirely comprised of adults ages 35–49 or 50 and older. Again, we can only speculate based on study findings, but this classification does seem to point to interesting generational or subcultural differences (Golub et al., 2005; Pearson & Shiner, 2002) in which “Gen Y” individuals may be more likely to use ecstasy (which became a popular street drug in the 1980s [National Institute on Drug Abuse, 2017]) and “Baby Boomers” and “Gen X” individuals may be more drawn to the hallucinogens that became especially prominent in the mid-1960s as part of the “counterculture” in the U.S.: namely, LSD and mushrooms (Dyck, 2015).
The final subgroup, the Poly-Hallucinogen class was characterized by across-the-board predicted probabilities that greatly exceeded the full sample mean of all hallucinogenic drugs examined. Notably, this class was disproportionately male and non-Hispanic White, and stood out as categorically distinct from the other classes in terms of other illicit drug use. The identification of this subgroup is in keeping with research indicating a profound “asymmetry” in drug use in which a small subset of individuals—small in the general population—account for a lopsided proportion of overall risk behavior, including illicit drug use (Vaughn et al., 2016).
4.1. Implications
Findings from the present study have a number of potential practice implications. First, findings indicating that the vast majority of current hallucinogen users tend to be lifetime poly-users suggests that youth prevention efforts that include a focus on hallucinogen use should focus not only on one particular high-prevalence hallucinogen (such as ecstasy or LSD), but should also discuss risks related to the full array of classic and dissociative hallucinogens. Second, the identification of a Poly-Hallucinogen class, which was characterized not only by the use of multiple hallucinogenic substances but also by involvement in other polydrug use, suggests that particular attention be paid to this high-risk subgroup. In light of the tremendous social cost associated with such behavior, scholars have argued that this “severe subset” involved in high rates of drug misuse and, frequently, other illegal behaviors, should be targeted in terms of early detection/prevention and treatment efforts (Salas-Wright et al., 2016; Vaughn et al., 2018).
4.2. Limitations
Findings from the present study should be interpreted in light of several limitations. First, although we pooled several years of data to increase our sample size and generate stable prevalence estimates, data from the NSDUH are fundamentally cross-sectional and therefore we cannot make any causal interpretations. Second, we were only able to look at the lifetime use of most hallucinogens. As such, while our study sheds light on lifetime poly-hallucinogen use, we were unable to make a specific contribution to more circumscribed or recent assessments of co-occurring use. Third, all data in the NSDUH are respondent self-report and, therefore, are potentially vulnerable to social desirability biases which can result in under/overreporting of high-risk behaviors. Finally, although the NSDUH is well respected as a source of US drug use surveillance, findings from general population surveys should be interpreted with caution and, ideally, coupled with other sources of surveillance to create more robust estimates (Reuter et al., 2021).
Conclusion
Findings from the present study shed new light on our understanding of the characteristics and behaviors of hallucinogen users in the US. We see compelling evidence that the overwhelming majority of current hallucinogen users, roughly 70%, are not “specialists” who use only one hallucinogen type, but rather that lifetime poly-hallucinogen use is the norm. Critically, however, we also see that important differences exist within the population of hallucinogen users—indeed, half could be classified as LSD-Mushroom-Ecstasy users only (this group was disproportionally comprised of youth), one third were Poly-Hallucinogen users (this group was disproportionately male and non-Hispanic White), and smaller proportions were limited primarily to use of LSD-Mushrooms (these individuals were almost exclusively ages 35 and older) or Ecstasy Only (these individuals were mostly younger adults ages 18–34). Our hope is that these findings provide a fresh contribution to our understanding of poly-hallucinogen use in a time in which local and state governmental leaders, and people across the country, weigh the benefits and drawbacks of legalizing specific hallucinogenic drugs.
Highlights.
The sample included 6,381 past-year hallucinogen users.
Only a minority of hallucinogen users report use of just one hallucinogen type.
70% of users report having used multiple hallucinogens, and 50% three or more.
Four distinct subtypes of hallucinogen users were identified.
Lifetime poly-hallucinogen use is associated with myriad behavior health problems.
Acknowledgments
Author Disclosures
Research reported in this publication was supported in part by the National Institute on Alcohol Abuse and Alcoholism (NIAAA) of the National Institutes of Health (NIH) under award number K01 AA026645. The content is solely the responsibility of the authors and does not necessarily represent the official views of NIAAA or the NIH.
Footnotes
Conflicts of Interest
Authors have no competing interests to declare.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- American Psychiatric Association (2000) Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: Amer Psychiatric Pub Inc. [Google Scholar]
- Bogenschutz MP, & Johnson MW (2016). Classic hallucinogens in the treatment of addictions. Prog Neuropsychopharmacol Biol Psychiatry, 64, 250–258. 10.1016/j.pnpbp.2015.03.002 [DOI] [PubMed] [Google Scholar]
- Bresin K (2020). Toward a unifying theory of dysregulated behaviors. Clin Psychol Rev, 101885. 10.1016/j.cpr.2020.101885 [DOI] [PubMed] [Google Scholar]
- Carhart-Harris R, Giribaldi B, Watts R, Baker-Jones M, Murphy-Beiner A, Murphy R, ... & Nutt DJ. (2021). Trial of psilocybin versus escitalopram for depression. N Engl J Med, 384(15), 1402–1411. 10.1056/NEJMoa2032994 [DOI] [PubMed] [Google Scholar]
- Celeux G, & Soromenho G (1996). An entropy criterion for assessing the number of clusters in a mixture model. Journal of Classification, 13(2), 195–212. 10.1007/BF01246098 [DOI] [Google Scholar]
- Davis AK, Barrett FS, May DG, Cosimano MP, Sepeda ND, Johnson MW, ... & Griffiths RR. (2021). Effects of psilocybin-assisted therapy on major depressive disorder: a randomized clinical trial. JAMA Psychiatry, 78(5), 481–489. 10.1001/jamapsychiatry.2020.3285 [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeLisi M, & Vaughn MG (2014). Foundation for a temperament-based theory of antisocial behavior and criminal justice system involvement. Journal of Criminal Justice, 42(1), 10–25. 10.1016/j.jcrimjus.2013.11.001 [DOI] [Google Scholar]
- Dyck E (2015). LSD: A new treatment emerging from the past. CMAJ, 187(14), 1079–1080. 10.1503/cmaj.141358 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ford JA, Watkins WC, & Blumenstein L (2011). Correlates of Salvia divinorum use in a national sample: Findings from the 2009 National Survey on Drug Use and Health. Addict Behav, 36(11), 1032–1037. 10.1016/j.addbeh.2011.06.004 [DOI] [PubMed] [Google Scholar]
- Golub A, Johnson BD, & Dunlap E (2005). Subcultural evolution and illicit drug use. Addiction Research & Theory, 13(3), 217–229. 10.1080/16066350500053497 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson MW, Richards WA, & Griffiths RR (2008). Human hallucinogenic research: Guidelines for safety. J Psychopharmacol, 22, 603–620. 10.1177/0269881108093587 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khantzian EJ (1997). The self-medication hypothesis of substance use disorders: A reconsideration and recent applications. Harv Rev Psychiatry, 4(5), 231–244. 10.3109/10673229709030550 [DOI] [PubMed] [Google Scholar]
- Killion B, Hai AH, Vaughn MG, Oh S, Oh S, Alsoami A, & Salas-Wright CP (2021). LSD use and in the United States: Trends, correlates, and a typology of use. Drug Alcohol Depend, 223. 108715. 10.1016/j.drugalcdep.2021.108715 [DOI] [PubMed] [Google Scholar]
- Krebs TS, & Johansen PØ (2013). Over 30 million psychedelic users in the United States. F1000 Research, 2(98). 10.12688/f1000research.2-98.v1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Markou A, Kosten TR, & Koob GF (1998). Neurobiological similarities in depression and drug dependence: A self-medication hypothesis. Neuropsychopharmacol, 18(3), 135–174. 10.1016/S0893-133X(97)00113-9 [DOI] [PubMed] [Google Scholar]
- McLachlan G, & Peel D (2000). Finite mixture models. New York, NY: John Wiley. [Google Scholar]
- Mitchell JM, Bogenschutz M, Lilienstein A, Harrison C, Kleiman S, Parker-Guilbert K, & Doblin R (2021). MDMA-assisted therapy for severe PTSD: a randomized, double-blind, placebo-controlled phase 3 study. Nat Med, 27(6), 1025–1033. 10.1038/s41591-021-01336-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Institute on Drug Abuse (2017, September). What is the history of MDMA? Retrieved on October 5, 2021 from: https://www.drugabuse.gov/publications/research-reports/mdma-ecstasy-abuse/what-is-the-history-of-mdma
- Palamar JJ, Mauro PM, Han BH, & Martins SS (2017). Shifting characteristics of ecstasy users ages 12–34 in the United States, 2007–2014. Drug Alcohol Depend, 181, 20–24. 10.1016/j.drugalcdep.2017.09.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pearson G, & Shiner M (2002). Rethinking the generation gap: attitudes to illicit drugs among young people and adults. Criminal Justice, 2(1), 71–86. 10.1177/17488958020020010401 [DOI] [Google Scholar]
- Reuter P, Caulkins JP, & Midgette G (2021). Heroin use cannot be measured adequately with a general population survey. Addiction. Advance online publication. 10.1111/add.15458 [DOI] [PubMed] [Google Scholar]
- Salas-Wright CP, Cano M, Hai AH, Oh S, & Vaughn MG (2021). Prevalence and correlates of driving under the influence of cannabis in the United States. Am J Prev Med. Advance online publication. 10.1016/j.amepre.2021.01.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salas-Wright CP, Vaughn MG, & Reingle Gonzalez JM (2016). Drug abuse and antisocial behavior: A biosocial life course approach. New York, NY: Palgrave Macmillan. [Google Scholar]
- Shalit N, Rehm J, & Lev-Ran S (2019). Epidemiology of hallucinogen use in the US results from the National epidemiologic survey on alcohol and related conditions III. Addict Behav, 89, 35–43. 10.1016/j.addbeh.2018.09.020 [DOI] [PubMed] [Google Scholar]
- StataCorp. (2019). Stata statistical software: Release 16. College Station, TX: Author. [Google Scholar]
- Substance Abuse and Mental Health Services Administration (SAMHSA). (2019). Results from the 2018 National Survey on Drug Use and Health: Summary of national findings. Rockville, MD: Substance Abuse and Mental Health Services Administration [Google Scholar]
- Vaughn MG, Salas-Wright CP, DeLisi M, & Maynard BR (2014). Violence and externalizing behavior among youth in the United States: Is there a Severe 5%? Youth Violence and Juvenile Justice, 12(1), 3–21. 10.1177/1541204013478973 [DOI] [Google Scholar]
- Vaughn MG, Salas-Wright CP, & Reingle-Gonzalez JM (2016). Addiction and crime: The importance of asymmetry in offending and the life-course. J Addict Dis, 35(4), 213–217. 10.1080/10550887.2016.1189658 [DOI] [PubMed] [Google Scholar]
- Vermunt JK, Magidson J, 2016. Upgrade manual for Latent GOLD 5.1. Statistical Innovations, Belmont, MA. [Google Scholar]
- Vollenweider FX (2001). Brain mechanisms of hallucinogens and entactogens. Dialogues Clin Neurosci, 3(4), 265–279. 10.31887/DCNS.2001.3.4/fxvollenweider [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wish ED, Fitzelle DB, O’Grady KE, Hsu MH, & Arria AM (2006). Evidence for significant polydrug use among ecstasy-using college students. J Am Coll Health, 55(2), 99–104. 10.3200/JACH.55.2.99-104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu LT, Woody GE, Yang C, Li JH, & Blazer DG (2011). Recent national trends in Salvia divinorum use and substance-use disorders among recent and former Salvia divinorum users compared with nonusers. Substance Abuse and Rehabilitation, 2, 53. 10.2147/SAR.S17192 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yockey RA, King KA, & Vidourek RA (2019). “Go ask Alice, when she’s 10-feet tall”: Psychosocial correlates to lifetime LSD use among a national sample of US adults. Journal of Psychedelic Studies, 3(3), 308–314. 10.1556/2054.2019.014 [DOI] [Google Scholar]
- Yockey RA, Vidourek RA, & King KA (2020). Trends in LSD use among US adults: 2015–2018. Drug Alcohol Depend, 108071. 10.1016/j.drugalcdep.2020.108071 [DOI] [PubMed] [Google Scholar]
- Zhang J, & Yu K (1998). What’s the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA, 280, 1690–1691. 10.1001/jama.280.19.1690 [DOI] [PubMed] [Google Scholar]