

Abstract
Background
Microvascular anastomosis is the key for successful free flap transplantation. Ideally, the anastomosis should maintain the flow with minimal turbulence, disruption of endothelium, and minimizing the furrow to prevent thrombosis and failure of the flap. One of the main pitfalls of micro‐anastomosis is vessels size mismatch.
Method and Result
There are many ways to overcome this issue, which includes forced mechanical dilation of the smaller vessel, oblique cuts, fish mouth cuts, interposition grafts, end‐to‐side anastomosis, coupling device, and others. Here, we report a simple technique with single customizable longitudinal arteriotomy of the smaller vessel to achieve an adequate size match to the larger vessel. It has been used for more than 10 years at our institution that allow us to achieve an end‐to‐end patent anastomosis.
Conclusion
Vertical arteriotomy is a simple technique that in our experience achieved end‐to‐end anastomosis high patency rate.
Keywords: arteriotomy, microsurgery, microsurgical anastomosis, vessels mismatch

Simple and effective technique to overcome the vessel mismatch predicament during microvascular anastomosis.
1. INTRODUCTION
Microvascular anastomosis is the key for successful free flap transplantation. Ideally, the anastomosis should maintain the flow with minimal turbulence, disruption of endothelium, and minimizing the furrow to prevent thrombosis and failure of the flap. One of the main pitfalls of micro‐anastomosis is vessels size mismatch. There are many ways to overcome this issue which includes forced mechanical dilation of the smaller vessel, oblique cuts, fish mouth cuts, interposition grafts (usually veins), end‐to‐side anastomosis, coupling device, and others. Here, we report a simple technique with single customizable longitudinal arteriotomy of the smaller vessel to achieve an adequate size match to the larger vessel. It has been used by the senior author (TG) for more than 10 years at our institution, which allow us to achieve an end‐to‐end patent anastomosis with high success rate. To our knowledge, this technique was only described in 2014 in a correspondence and communication to the journal editors by Ridha et al and they called their technique spatulated end‐to‐end microvascular anastomosis. 1
2. TECHNIQUE
After cleaning the adventitia of the vessels, the smaller artery is manually dilated with jeweler's micro‐forceps confirming the size discrepancy of >1:1.5. A pot's micro‐scissors then used to perform a clean longitudinal incision in that vessel. The cut can be customized in length till the desirable size achieved to overcome the size mismatch (Figures 1 and 2). The cut will result in an apex at the end of the cut, which will be called (heel). The microvascular anastomosis then begins with a suture passing through the heel of the smaller vessel to the larger vessel, another suture placed at 180° to allow the proper alignment of the two vessels. As a result of this longitudinal incision and after the placement of the two stay sutures, there are two arterial flaps on each side of that incision on the smaller vessel, these can be trimmed or just incorporated in the anastomosis. This technique can work with the interrupted suture method or the running method as we demonstrate in Figure 3 and the Video S1.
FIGURE 1.
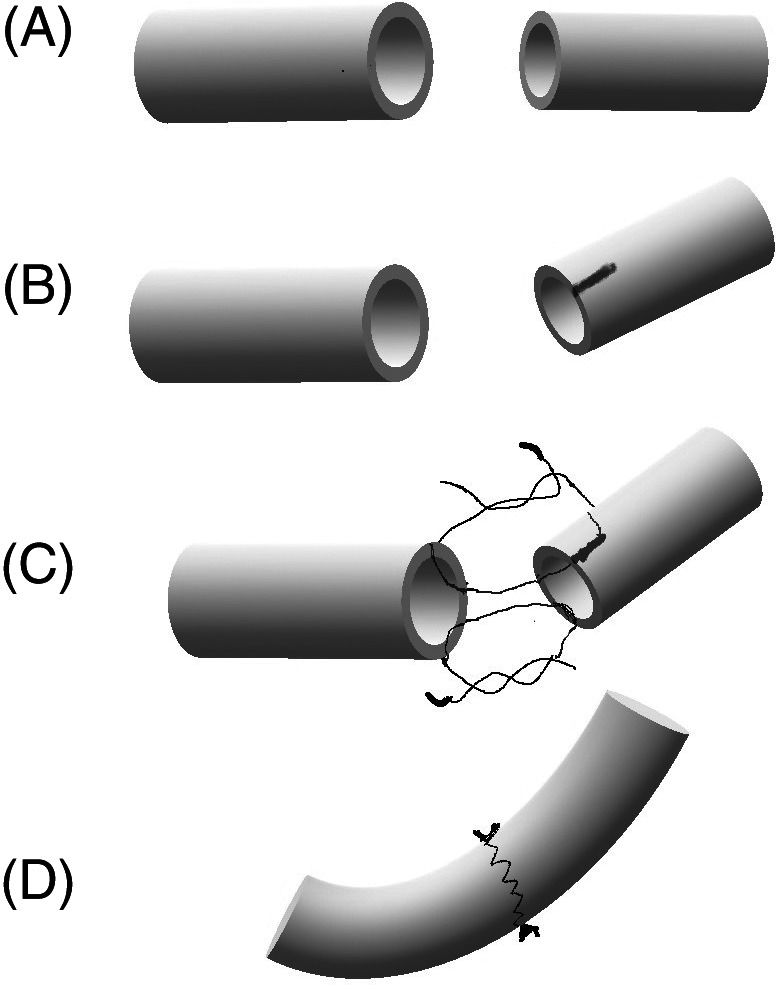
A, Vessels mismatch. B, Vertical arteriotomy in the small vessel. C, Suturing technique. D, Result of the closure
FIGURE 2.
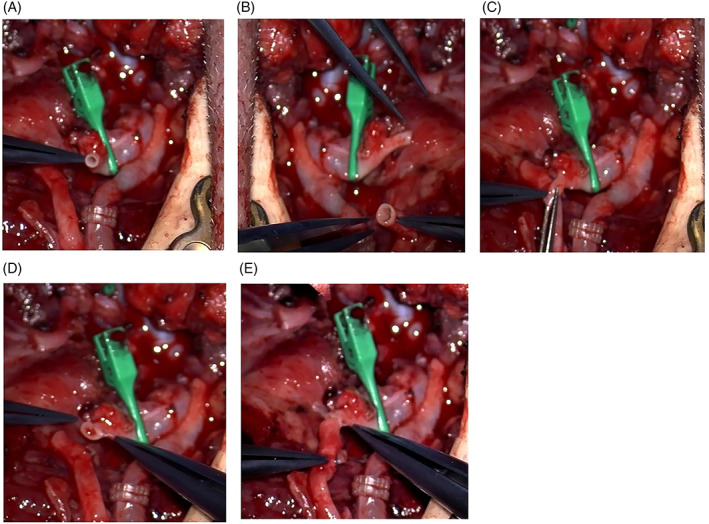
View of the vessels under the surgical microscope. A, The facial artery; B, peroneal artery; C, a longitudinal cut been performed to the facial artery, D, increase in the diameter after the cut; and E, improvement of size mismatch
FIGURE 3.
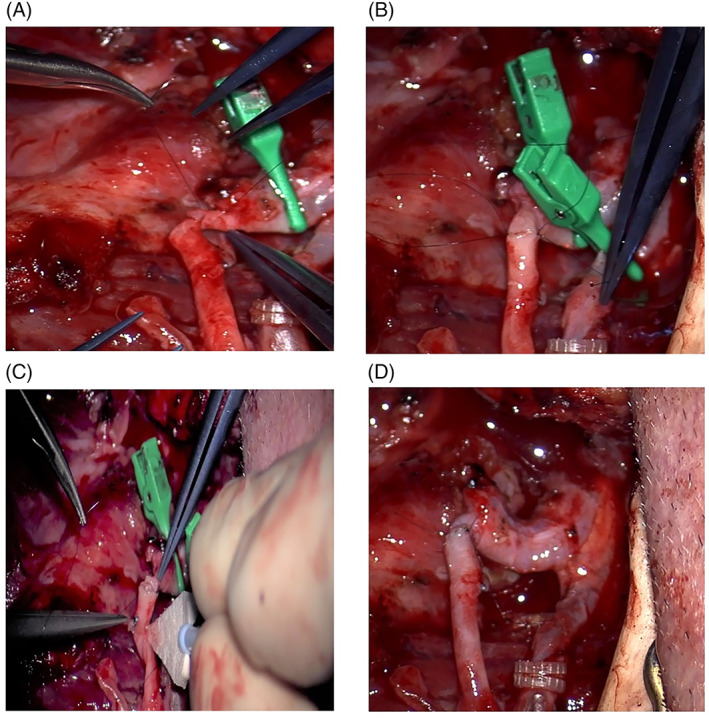
Suturing technique. A, First stay suture passed through the heel at the apex of the longitudinal incision to the larger vessel. B, Two stay sutures 180° apart. C, Look inside the lumen after running one wall. D, At the end of the anastomosis with arterial flow established
3. DISCUSSION
Microvascular flap reconstruction is widely used in head and neck reconstruction, with extremely high reliability 97% to 99% success rates. These results are achievable due to successful vascular anastomosis patency due to meticulous surgical technique rather than pharmacological agents to maintain a streamline flow. 2 This is particular in anastomosing vessels of different sizes. Various techniques exist to manage the vessels mismatch during microsurgery. Mechanical dilation can be applied only when the mismatch is about 1:1.5 or less. Forced dilation of a vessel more than 1.5 times will result in an endothelial damage, which might predispose to thrombosis. 3 Another relatively easy techniques include oblique cut, which can be used in limited discrepancy as it might predispose to turbulent flow. Fish mouth technique requires excessive vessel handling and it is used in a limited size mismatch vessel. 4 Sleeve technique is a fast, easy technique, and proven reliable to use in 1:2 discrepancy ratio. The smaller vessel is telescoped into the larger vessel. Disadvantages of this technique, turbulence of the flow and risk of thrombosis if not done correctly and risk of aneurysmal dilatation. 5 For larger discrepancy up to 1:3, a wedge resection technique can be utilized. Rickard et al demonstrate that wedge resection of the large vessel twice the vessel diameter had superior flow compared to the previous techniques. 6 A more involved technique is to use a V‐plasty, which can be used in a discrepancy ratio up to 1:5. It involves a “V” flap in the larger vessel and a longitudinal cut in the smaller vessel. 7 An open Y‐plasty technique was used by Chen et al in head and neck reconstruction with reported success rate of 98.6% in a series of more than 70 cases. The main disadvantage besides being a challenging technique, is that a bifurcation at the site of the anastomosis is required for this technique. 8
Spatulation end‐to‐end anastomosis is technically demanding and involves excessive manipulation of the vessels but can be used for large vessels discrepancies. It involved spatulation of both vessels with subsequent four corner sutures. If increased circumference is required, a two equal triangular sidewall flaps can be raised. 9 Other alternative techniques include interposition artery, interposition vein grafts, and coupler devices. End to side anastomosis is one of the reliable techniques to overcome any size discrepancy. 10
In comparison to previous techniques, in spatulated technique, only single vertical arteriotomy is required which translates to less vessel handling and minimizes the intimal injury. Moreover, an intermediate to large size discrepancy can be handled in this technique sustaining nonturbulent flow. This technique been exercised on irradiated vessels, atherosclerotic vessels, and even on interposition vein grafts with size mismatch with recipient arteries with adequate results. The main advantage of this technique is that it is reproducible and easy to perform when compared to other more challenging techniques described above.
4. CONCLUSION
Many techniques exist for the management of vessels size discrepancy in microvascular anastomosis. We re‐present the spatulated technique as a reliable, easy way to overcome this issue. It requires no experience and show less vessel handling and appropriate for a discrepancy ratio larger than 1:3.
CONFLICT OF INTEREST
Nothing to disclose.
ETHICS STATEMENT
Statement of institutional review board (IRB) approval: Not needed, as this is a surgical technique that can be used at the surgeon discretion.
Supporting information
Video S1 Microsurgical anastomosis between facial artery and peroneal artery depicting the vertical arteriotomy. This was performed by Dr Tamer Ghanem, MD, PhD, FACS
Alamoudi U, Ghanem T. Solution to vessels mismatch in microsurgery: Vertical arteriotomy technique. Laryngoscope Investigative Otolaryngology. 2021;6(6):1321‐1324. doi: 10.1002/lio2.650
BIBLIOGRAPHY
- 1. Ridha H, Morritt AN, Wood SH. Spatulated end‐to‐end microvascular anastomosis: a useful technique for overcoming vessel size discrepancy. J Plast Reconstr Aesthet Surg. 2014;67(10):e254‐e255. 10.1016/j.bjps.2014.07.008 [DOI] [PubMed] [Google Scholar]
- 2. Hayhurst JW, O'Brien BM. An experimental study of microvascular technique, patency rates and related factors. Br J Plast Surg. 1975;28(2):128‐132. 10.1016/s0007-1226(75)90175-7 [DOI] [PubMed] [Google Scholar]
- 3. Turker T, Tsai TM, Thirkannad S. Size discrepancy in vessels during microvascular anastomosis: two techniques to overcome this problem. Hand Surg. 2012;17(3):413‐417. 10.1142/S0218810412970052 [DOI] [PubMed] [Google Scholar]
- 4. Harashina T, Irigaray A. Expansion of smaller vessel diameter by fish‐mouth incision in microvascular anastomosis with marked size discrepancy. Plast Reconstr Surg. 1980;65(4):502‐503. 10.1097/00006534-198004000-00019 [DOI] [PubMed] [Google Scholar]
- 5. de la Peña‐Salcedo JA, Cuesy C, López‐Monjardin H. Experimental microvascular sleeve anastomosis in size discrepancy vessels. Microsurgery. 2000;20(4):173‐175. [DOI] [PubMed] [Google Scholar]
- 6. Rickard RF, McPhaden AR, Hudson DA. Healing of two microarterial anastomoses with diameter mismatch. J Surg Res. 2014. Sep;191(1):239‐49. e3. 10.1016/j.jss.2014.03.011 [DOI] [PubMed] [Google Scholar]
- 7. Bakhach J, Dibo S, Zgheib ER, Papazian N. The V‐Plasty: a novel microsurgical technique for anastomosis of vessels with marked size discrepancy. J Reconstr Microsurg. 2016;32(2):128‐136. 10.1055/s-0035-1563394 [DOI] [PubMed] [Google Scholar]
- 8. Chen YC, Scaglioni MF, Huang EY, Kuo YR. Utility of “open‐Y” anastomosis technique in the use of superior thyroid artery as recipient vessel for head and neck reconstruction with free flap. Microsurgery. 2016;36(5):391‐396. 10.1002/micr.22384 [DOI] [PubMed] [Google Scholar]
- 9. Kruse AL, Luebbers HT, Grätz KW, Obwegeser JA. Factors influencing survival of free flap in reconstruction for cancer of the head and neck: a literature review. Microsurgery. 2010;30(3):242‐248. 10.1002/micr.20758 [DOI] [PubMed] [Google Scholar]
- 10. Okazaki M, Asato H, Sarukawa S, Takushima A, Nakatsuka T, Harii K. Availability of end‐to‐side arterial anastomosis to the external carotid artery using short‐thread double‐needle microsuture in free‐flap transfer for head and neck reconstruction. Ann Plast Surg. 2006. Feb;56(2):171‐175. 10.1097/01.sap.0000197620.03306.2f [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Video S1 Microsurgical anastomosis between facial artery and peroneal artery depicting the vertical arteriotomy. This was performed by Dr Tamer Ghanem, MD, PhD, FACS