

Abstract
Objective:
To assess the reproducibility of cephalometric measurements performed with software for a tablet, with a program for personal computers (PCs), and manually.
Materials and Methods:
The pretreatment lateral cephalograms of 20 patients that were acquired using the same digital cephalometer were collected. Tracings were performed with NemoCeph for Windows (Nemotec), with SmileCeph for iPad (Glace Software), and by hand. Landmark identification was carried out with a mouse-driven cursor using NemoCeph and with a stylus pen on the iPad screen using SmileCeph. Hand tracings were performed on printouts of the cephalograms, using a 0.3-mm 2H pencil and a protractor. Cephalometric landmarks and linear and angular measurements were recorded. All the tracings were done by the same investigator. To evaluate reproducibility, for each cephalometric measurement the agreement between the value derived from NemoCeph, that given by SmileCeph and that measured manually was assessed with the intraclass correlation coefficient (ICC). Agreement was rated as low for an ICC ≤0.75, and an ICC > 0.75 was considered indicative of good agreement. Also, differences in measurements between each software and manual tracing were statistically evaluated (P < .05).
Results:
All the measurements had ICC >0.8, indicative of a high agreement among the tracing methods. Relatively lower ICCs occurred for linear measurements related to the occlusal plane and to N perpendicular to the Frankfurt plane. Differences in measurements between both software programs and hand tracing were not statistically significant for any of the cephalometric parameters.
Conclusion:
Tablet-assisted, PC-aided, and manual cephalometric tracings showed good agreement.
Keywords: Computer-aided cephalometric analysis, Manual cephalometric analysis
INTRODUCTION
Currently, cephalometric analyses for orthodontic diagnosis, treatment planning, and research are often performed on digital images by means of computer softwares. Digital technology has introduced several benefits in cephalometric radiology, as it enables instantaneous image acquisition, requires a lower radiation dose,1 avoids the developing process, and simplifies image storing and sharing.2 Moreover, the quality of digital cephalograms can be improved using digital tools for image enhancement.3–6
Additionally, the use of cephalometric tracing softwares on screen-displayed digital images has been considered advantageous in many regards. In computerized cephalometric analysis, once the requested landmarks have been entered, the software automatically calculates distances and angles, thus eliminating errors that may occur in hand tracing when drawing lines with a ruler and measuring angles with a protractor.5,7,8 Furthermore, collecting computer-assisted cephalometrics is less time-consuming than manual tracing,3,9 and it allows the user to obtain several analyses at a time.6 In addition, digital archiving overcomes the problem of film deterioration.6,9 Earlier studies have assessed the reproducibility of measurements in manual versus computer-aided cephalometric analysis.3–6,8–20
However, as new programs for computerized cephalometry are continuously launched, their accuracy needs to be validated against that of previously marketed softwares and against traditional hand tracing. Lately, a software for digital tracing has been made available as an application for iPad. A distinctive feature of this software is that landmark identification is carried out by touching the tablet screen with a finger or by using a stylus pen. Conversely, with all the other marketed softwares points are digitized by means of a mouse-driven cursor. As landmark identification has been reported to be the main source of error in cephalometric analysis,9,21 it seemed worth verifying whether digitizing the points directly on the tablet touch screen is a reliable method. With this objective, the reproducibility of cephalometric measurements provided by the tablet, by marketed software for personal computers (PCs), and by hand-tracing was assessed. The tested null hypothesis was that linear and angular measurements derived from tablet-assisted, PC-aided, and manual cephalometrics did not disagree to a statistically significant level.
MATERIALS AND METHODS
Pretreatment lateral cephalometric radiographs of 20 patients acquired using the same digital cephalometer (Gendex Orthoralix 9200 DDE, Gendex Dental Systems, Des Plaines, Ill; magnification ×1.1) were collected. The subjects had been positioned in the cephalostat with the sagittal plane at a right angle to the path of the X-rays, the Frankfurt plane parallel to the floor, the teeth in centric occlusion, and the lips pressed lightly together. No differentiation was made for gender, type of occlusion, or skeletal pattern.
The following sample exclusion criteria were established: no unerupted or partially erupted teeth that could hinder incisor apex identification and no poor-quality images or artifacts that could interfere with anatomic point identification. Digital tracings were performed using NemoCeph NX 2009 for Windows (Nemotec, Madrid, Spain)8 and SmileCeph for iPad (Glace Software, Imola, Italy). Before entering the landmarks, cephalograms were calibrated by digitizing two points on the length-measuring gauge within the digital cassette. Landmark identification was carried out with a mouse-controlled cursor using NemoCeph and with a stylus pen on the iPad screen using SmileCeph.
In hand tracing, for the purpose of standardization, no change in resolution, contrast, or brightness was made to digital cephalograms before printing. After resizing to 1∶1 scale with Adobe Photoshop (Adobe Systems, San Jose, Calif), digital images were printed on semigloss paper for high-quality photographic images (Hewlett-Packard, Palo Alto, Calif)3 using a 2400 dpi color laser printer (Canon Laser I-sensys Lbp-6020, Tokyo, Japan). Manual tracings were performed on a clear acetate sheet placed over the printed image and using a 0.3-mm 2H lead pencil and a protractor (3M Unitek, Monrovia, Calif). Bilateral structures were averaged to make a single landmark. All the tracings were performed by the same investigator, an orthodontist who had long experience with cephalometrics. No more than 10 radiographs per day were traced to avoid examiner fatigue.8 Commonly used dental and skeletal landmarks were selected and produced the linear and angular measurements listed in Table 1 and shown in Figure 1. To assess reliability, all the cephalograms were retraced by the same investigator with each method. A time interval longer than 6 weeks elapsed between first and second analyses.
Table 1.
Description of Landmarks, Planes, and Measurements Used in the Study

Figure 1.
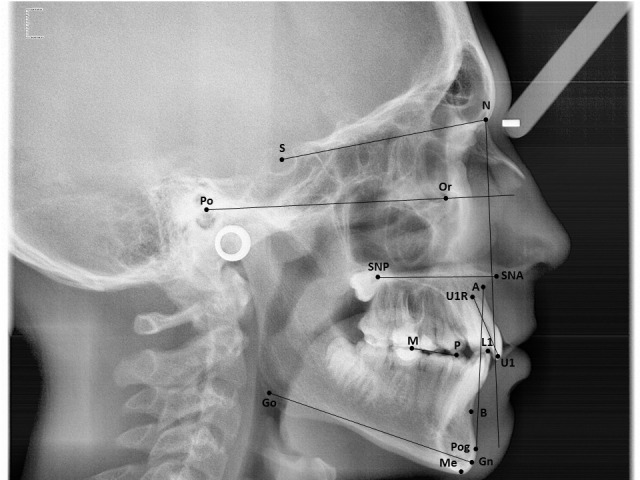
Location of landmarks, planes, and measurements used in the study. S indicates Sella; N, Nasion; A, point A; B, point B; Po, Porion; Or, Orbitale; Pog, Pogonion; Me, Menton; Go, Gonion; Gn, Gnathion; ANS, anterior nasal spine; PNS, posterior nasal spine; M, lower first molar; P, lower first premolar; U1, upper incisor tip; U1R, upper incisor apex; L1, lower incisor tip.
Statistical Analysis
To determine intrarater reliability for each tracing technique, the intraclass correlation coefficient (ICC) of repeated measurements was calculated for every cephalometric variable.9,20 To evaluate reproducibility for each cephalometric parameter, the agreement between the value derived from NemoCeph, that given by SmileCeph, and that measured manually was assessed with the ICC.4,5,9,20 Agreement was rated as low for an ICC ≤lower than 0.75. Conversely, an ICC > 0.75 was considered indicative of good agreement.5,22 Also, differences in measurements between each software and manual tracing were evaluated using the t-test for independent samples after preliminarily checking that data distribution was normal in each group.3,8 For the same purpose, the Mann-Whitney U test was used in case the data distribution was not found to be normal (variables Pog to N perpendicular to the Frankfurt plane and U1∧SNA-SNP). The level of statistical significance was set at P < .05. The statistical analyses were handled by the software Statistical Package for Social Sciences version 11.0 (SPSS Inc, Chicago, IL).
RESULTS
The ICC values calculated for repeated measurements with each tracing technique are reported in Table 2. All ICCs exceeded 0.85, and most values were above 0.9, thus providing an indication of very high intrarater reliability.9
Table 2.
Intraclass Correlation Coefficients (ICCs) of Repeated Cephalometric Measurements in Tablet-Assisted, PC-Aided, and Hand Tracing for Assessing Intrarater Reliability

The ICC values of cephalometric measurements recorded with the three tracing techniques are reported in Table 3. All the cephalometric parameters had ICC >0.8, indicative of a high agreement among the tracing methods. Most of the ICCs actually exceeded 0.9. The highest values of correlation were noticed for the SNA, SNB, ANB angles, and for the linear distances of incisor tip to A-Pog. The lowest ICCs occurred for linear measurements related to the occlusal plane and to N perpendicular to Frankfurt plane. Table 4 reports means and standard deviations of the differences in measurements between either software and manual tracing as well as between the two softwares. The t-test revealed that for all the assessed cephalometric parameters, statistically similar amounts of difference from manual tracing occurred using either software (P > .05).
Table 3.
Intraclass Correlation Coefficients (ICCs) of the Cephalometric Measurements Derived from Tablet-assisted, PC-Aided, and Manual Tracing for Assessing Reproducibility

Table 4.
Differences in Cephalometric Measurements Between Either Software and Hand Tracing (Columns 2 and 3) and Between the Two Softwares (Column 5)*

DISCUSSION
Based on the outcome of the statistical analyses, the formulated null hypothesis fails to be rejected. The finding of ICC values >0.8 for all the assessed variables points out that the reproducibility of cephalometric tracings recorded manually, with NemoCeph, and with SmileCeph was satisfactory. The lack of statistical significance of the differences in measurements between both computerized methods and hand tracing reinforces the evidence that the tested softwares can be reliably used in orthodontic diagnosis.
Among several advantages of digital cephalometry, time saving and ease of use are much appreciated by clinicians. Increased user-friendliness was a specific objective in the development of SmileCeph, the cephalometric software for iPad that provides greater portability than a PC. However, the peculiar method of landmark digitization by touching the tablet screen needed to be tested in an independent study. The observation that the measurements obtained in the tablet-assisted analysis agreed well with those derived from the other tracing methods validates the use of the iPad application for gathering cephalometrics.
Both NemoCeph and SmileCeph allow for image enhancement through adjustments of magnification, contrast, and brightness. Moreover, both software programs feature a digital tool to correct landmark position after the initial digitization. Any procedure helpful to refine landmark identification is indeed beneficial, as point location remains the main source of error in cephalometry.21
The finding of relatively lower correlation coefficients for distances to Nasion perpendicular to Frankfurt plane has also been reported in previous studies.3,9,20 The explanation for this occurrence was that the Frankfurt plane is defined by Porion and Orbitale, landmarks sometimes not clearly identifiable in a cephalogram.3,9,12,20,23 Similar difficulties may be encountered in the definition of the occlusal plane12 and this may account for the relatively lower intermethod agreement observed for Wits measurements. In contrast to the finding of Santoro et al.,18 who reported a significant difference between digital and manual measurements of L1 to A-Pog, in the present study this cephalometric parameter showed very high reproducibility with an ICC value of 0.986.
Because standardization is crucial in comparative studies and interexaminer error has been reported to be greater than intraexaminer error,9 only one operator should be involved with all the cephalometric measurements.3,6 This indication was strictly followed in the present study. The intention to minimize errors also guided the choice of the landmarks used in this investigation. Following the indications of previous studies,3,4 the most easily locatable points in analyses featured by both softwares were selected. As the lower incisor apex has often been reported to be affected by the superimposition of other anatomic structures and to have poor reproducibility,4,24 the measurement of the lower incisor angulation was omitted in the present study. Based on similar considerations, measurements involving the point Condylion were not included in the analysis.4
CONCLUSION
Tablet-assisted cephalometry showed good agreement with PC-aided cephalometry and with manual tracing and might be preferred when user-friendliness and portability are prioritized.
REFERENCES
- 1.Visser H, Rödig T, Hermann KP. Dose reduction by direct-digital cephalometric radiography. Angle Orthod. 2001;71:159–163. doi: 10.1043/0003-3219(2001)071<0159:DRBDDC>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 2.Tan SS, Ahmad S, Moles DR, Cunningham SJ. Picture archiving and communications systems: a study of reliability of orthodontic cephalometric analysis. Eur J Orthod. 2011;33:537–543. doi: 10.1093/ejo/cjq116. [DOI] [PubMed] [Google Scholar]
- 3.Celik E, Polat-Ozsoy O, Toygar Memikoglu TU. Comparison of cephalometric measurements with digital versus conventional cephalometric analysis. Eur J Orthod. 2009;31:241–246. doi: 10.1093/ejo/cjn105. [DOI] [PubMed] [Google Scholar]
- 4.Polat-Ozsoy O, Gokcelik A, Toygar Memikoglu TU. Differences in cephalometric measurements: a comparison of digital versus hand-tracing methods. Eur J Orthod. 2009;31:254–259. doi: 10.1093/ejo/cjn121. [DOI] [PubMed] [Google Scholar]
- 5.Tsorovas G, Karsten AL. A comparison of hand-tracing and cephalometric analysis computer programs with and without advanced features—accuracy and time demands. Eur J Orthod. 2010;32:721–728. doi: 10.1093/ejo/cjq009. [DOI] [PubMed] [Google Scholar]
- 6.AlBarakati SF, Kula KS, Ghoneima AA. The reliability and reproducibility of cephalometric measurements: a comparison of conventional and digital methods. Dentomaxillofac Radiol. 2012;41:11–17. doi: 10.1259/dmfr/37010910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Liu JK, Cheng KS. Accuracy of computerized automatic identification of cephalometric landmarks. Am J Orthod Dentofacial Orthop. 2000;118:535–540. doi: 10.1067/mod.2000.110168. [DOI] [PubMed] [Google Scholar]
- 8.Erkan M, Gurel HG, Nur M, Demirel B. Reliability of four different computerized cephalometric analysis programs. Eur J Orthod. 2012;34:318–321. doi: 10.1093/ejo/cjr008. [DOI] [PubMed] [Google Scholar]
- 9.Sayinsu K, Isik F, Trakyali G, Arun T. An evaluation of the errors in cephalometric measurements on scanned cephalometric images and conventional tracings. Eur J Orthod. 2007;29:105–108. doi: 10.1093/ejo/cjl065. [DOI] [PubMed] [Google Scholar]
- 10.Macrì V, Wenzel A. Reliability of landmark recording on film and digital lateral cephalograms. Eur J Orthod. 1993;15:137–148. doi: 10.1093/ejo/15.2.137. [DOI] [PubMed] [Google Scholar]
- 11.Geelen W, Wenzel A, Gotfredsen E, Kruger M, Hansson L-G. Reproducibility of cephalometric landmarks in conventional film, hardcopy and monitor-displayed images obtained by the storage phosphor technique. Eur J Orthod. 1998;20:331–340. doi: 10.1093/ejo/20.3.331. [DOI] [PubMed] [Google Scholar]
- 12.Chen YI, Chen SK, Chan HF, Chen KC. Comparison of landmark identification in traditional versus computer-aided digital cephalometry. Angle Orthod. 2000;70:387–392. doi: 10.1043/0003-3219(2000)070<0387:COLIIT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.Ongkosuwito EM, Katsaros C, van't Hof MA, Bodegom JC, Kuijpers-Jagtman AM. The reproducibility of cephalometric measurements: a comparison of analogue and digital methods. Eur J Orthod. 2002;24:655–665. doi: 10.1093/ejo/24.6.655. [DOI] [PubMed] [Google Scholar]
- 14.Chen YI, Chen SK, Yao JC, Chang HF. The effects of differences in landmark identification on cephalometric measurements in traditional versus digitized cephalometry. Angle Orthod. 2004;74:155–161. doi: 10.1043/0003-3219(2004)074<0155:TEODIL>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 15.Gregston MD, Kula T, Hardman P, Glaros A, Kula K. Comparison of conventional and digital radiographic methods and cephalometric analysis software: I. Hard tissue. Semin Orthod. 2004;10:204–211. [Google Scholar]
- 16.Kublashvili T, Kula K, Glaros A, Hardman P, Kula T. A comparison of conventional and digital radiographic methods and cephalometric analysis software: II. Soft tissue. Semin Orthod. 2004;10:212–219. [Google Scholar]
- 17.Power G, Breckon J, Sherriff M, McDonald F. Dolphin Imaging Software: an analysis of the accuracy of cephalometric digitization and orthognathic prediction. Int J Oral Maxillofac Surg. 2005;34:619–626. doi: 10.1016/j.ijom.2005.04.003. [DOI] [PubMed] [Google Scholar]
- 18.Santoro M, Jarjoura K, Cangialosi TJ. Accuracy of digital and analogue cephalometric measurements assessed with the sandwich technique. Am J Orthod Dentofacial Orthop. 2006;129:345–351. doi: 10.1016/j.ajodo.2005.12.010. [DOI] [PubMed] [Google Scholar]
- 19.Naoumova J, Lindman R. A comparison of manual traced images and corresponding scanned radiographs digitally traced. Eur J Orthod. 2009;31:247–253. doi: 10.1093/ejo/cjn110. [DOI] [PubMed] [Google Scholar]
- 20.Uysal T, Baysal A, Yagci A. Evaluation of speed, repeatability, and reproducibility of digital radiography with manual versus computer-assisted cephalometric analyses. Eur J Orthod. 2009;31:523–528. doi: 10.1093/ejo/cjp022. [DOI] [PubMed] [Google Scholar]
- 21.Forsyth DB, Shaw WC, Richmond S, Roberts CT. Digital imaging of cephalometric radiographs. Part 2: image quality. Angle Orthod. 1996;66:43–60. doi: 10.1043/0003-3219(1996)066<0043:DIOCRP>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 22.Fayers P, Hays R. Assessing Quality of Life in Clinical Trials Methods and Practice. Oxford, UK: Oxford University Press; 2005. [Google Scholar]
- 23.Bruntz LQ, Palomo JM, Baden S, Hans MG. A comparison of scanned lateral cephalograms with corresponding original radiographs. Am J Orthod Dentofacial Orthop. 2006;130:340–348. doi: 10.1016/j.ajodo.2004.12.029. [DOI] [PubMed] [Google Scholar]
- 24.Houston WJB, Maher RE, McElroy D, Sheriff M. Sources of error in measurements from cephalometric radiographs. Eur J Orthod. 1986;8:149–151. doi: 10.1093/ejo/8.3.149. [DOI] [PubMed] [Google Scholar]