

Abstract
The maintenance of balanced oral homeostasis depends on saliva. A readily available and molecularly rich source of biological fluid, saliva fulfills many functions in the oral cavity, including lubrication, pH buffering, and tooth mineralization. Saliva composition and flow can be modulated by different factors, including circadian rhythm, diet, age, drugs, and disease. Recent events have revealed that saliva plays a central role in the dissemination and detection of the SARS-CoV-2 coronavirus. A working knowledge of saliva function and physiology is essential for dental health professionals.
Saliva is essential for the maintenance of oral health.1 Human salivary glands produce from 0.5 to 1.5 liters of total saliva in a 24-hour period. A complex fluid, containing electrolytes, salivary and serum proteins, and small organic molecules, as well as metabolites and debris from microorganisms that colonize the mouth, saliva functions to moisten and protect oral tissues, clean the gingiva and teeth, and aids speaking and swallowing. Additional essential roles include buffering of the oral cavity, protective pellicle formation, tooth mineralization, antimicrobial activity, tissue repair, and taste and digestion. Radiation therapy for head and neck cancers, autoimmune diseases such as Sjögren’s syndrome, as well as other systemic diseases and many medications can decrease saliva production; this condition is known as xerostomia and has multiple often debilitating consequences. Given the central role of saliva in oral health and disease, an up-to-date understanding of its physiology and functions is essential for dentists and health professionals.
HUMAN SALIVARY GLANDS: STRUCTURE AND COMPOSITION
Three pairs of major salivary glands collectively produce approximately 90% of total saliva. The remainder is produced by hundreds of minor salivary glands located in submucosal tissues lining the oral cavity.2 The major salivary glands consist of clustered secretory cells known as acini, which produce the primary saliva and secrete most salivary proteins.3 Serous acinar cells secrete a watery saliva containing proteins such as alpha-amylase, while mucous acinar cells secrete a stickier saliva containing mucins, highly glycosylated proteins that function to increase viscosity. Acini secrete saliva into small intercalated ducts linked to a ductal tree of larger striated ducts which coalesce and ultimately terminate in the excretory ducts that empty into the oral cavity. As the isotonic fluid secreted by the acini passes through this system, duct cells actively modify the ionic composition through resorption.3 The ducts are lined by the epithelial cells of heterogeneous cell types,4,5 some of which also secrete salivary proteins.6
The parotid glands (PGs), the largest of the major salivary glands, are made up of serous acini.7 PG excretory ducts, known as Stensen ducts, open on both surfaces of the buccal mucosa near the second maxillary molar (Fig. 1).8 The submandibular glands (SMGs), located inferiorly to the mandible, include both serous and mucous acini, which secrete saliva of moderate viscosity7 into the oral cavity by way of the Wharton excretory ducts, located at the sublingual caruncle below the tongue. Together, the PGs and SMGs produce the major volume of saliva. The smallest sublingual glands (SLGs) are located between the muscles of the lower oral cavity floor. The SLGs secrete a small volume of highly viscous saliva produced by mucous acini, mixed with a few serous acinar cells, which passes through the Bartholin and Rivinus ducts into the oral cavity at the sublingual caruncle and the sublingual fold, respectively. Hundreds of minor salivary glands, approximately 1 to 2 mm in size, drain into short excretory ducts which are widely distributed throughout the oral submucosa.9 With the exception of von Ebner glands, which are serous, the minor salivary glands are made up of mucous acini.
Figure 1.
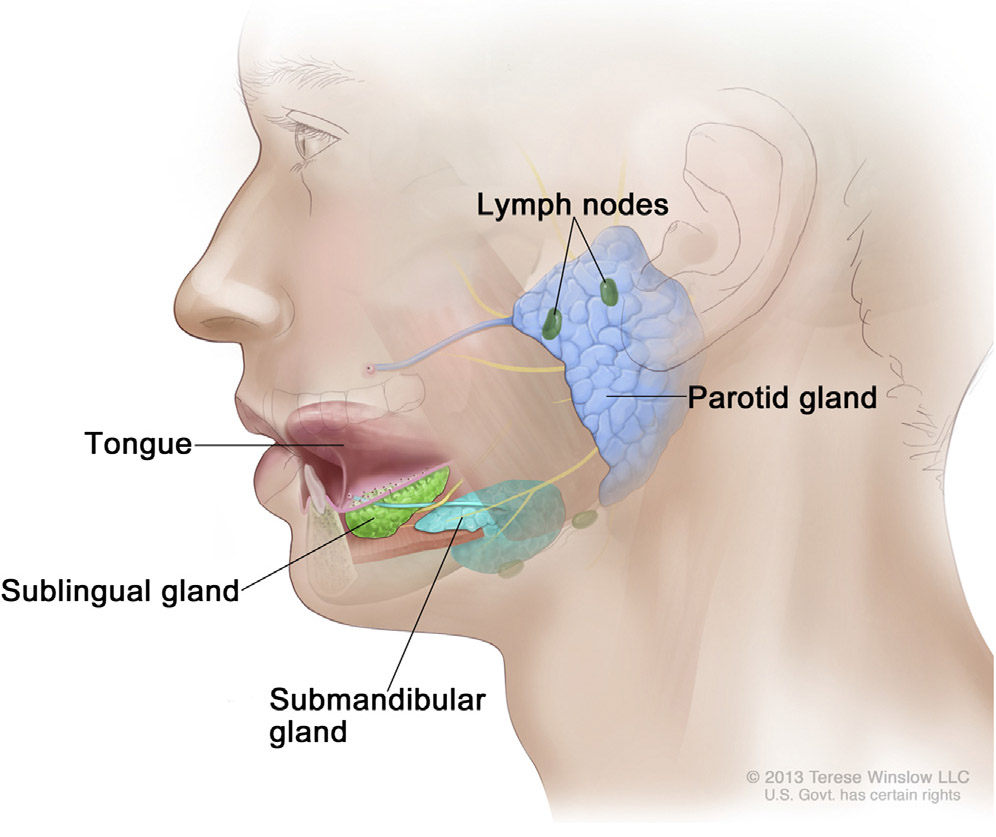
Location of parotid, submandibular, and sublingual major salivary glands in relation to tongue, mandible, and oral cavity. Points of entry of excretory ducts from each gland into oral cavity indicated. Nerves shown in yellow. Reprinted with permission. © 2013 Terese Winslow LLC, U.S. Govt. has certain rights.
SALIVA SECRETION
The mechanism of saliva secretion is the same in all salivary glands, although the composition and volume of saliva produced vary widely.10,11 Multiple ion and water channels, exchangers, and transporter proteins act in a coordinated manner to produce and secrete saliva.12 The secretion process is controlled by parasympathetic nerves which release acetylcholine that binds to muscarinic receptors on the acinar cell membrane.3,13 Stimulation of the receptors results in increased intracellular Ca2+, which drives electrolytes into intercalated ducts, followed by water.11 Salivary glands are also innervated by sympathetic nerves, which release noradrenaline that binds to adrenergic receptors and promotes secretion of salivary proteins. Minor salivary glands are innervated by parasympathetic nerve fibers.14
Under unstimulated conditions, the SMG make the highest contribution to whole saliva volume (SMG: 60%, PG: 25% to 30%, SLG: 8%). However, under stimulated conditions, the PG contribution is highest (SMG: 35%, PG: 50%, SLG: 8%).1 Minor salivary glands secrete 10% of total resting saliva.2 In healthy adults, the mean flow rate of unstimulated whole saliva is 0.3 to 0.4 mL/min, and a flow rate of less than 0.1 mL/min is classified as hyposalivation.15 In contrast, the mean stimulated saliva flow rate is reported to range from 1.5 to 2.0 mL/min.15 There are significant differences in the composition of stimulated and unstimulated saliva (Table 1).16,17 The concentration of inorganic and organic components changes with stimulation, as does the hypotonicity. The bicarbonate concentration of stimulated saliva is also many times higher than that of unstimulated saliva. However, the total protein content is decreased in stimulated saliva.
Table 1.
Concentration and composition of unstimulated and mastication-stimulated whole human saliva
| Salivary Components | Concentration in Unstimulated Saliva |
Concentration in Stimulated Saliva |
|---|---|---|
| H2O | 99.55% | 99.53% |
| Solids | 0.45% | 0.47% |
| – | Mean ±S.D. | Mean ±S.D. |
| Flow rate (mL/min) | 0.32 ±0.23 | 2.08 ±0.84 |
| pH | 7.04 ±0.28 | 7.61 ±0.17 |
| Inorganic constituents | – | – |
| Sodium (mmol/L) | 5.76 ±3.43 | 20.67 ±11.74 |
| Potassium (mmol/L) | 19.47 ±2.18 | 13.62 ±2.70 |
| Calcium (mmol/L) | 1.32 ±0.24 | 1.47 ±0.35 |
| Magnesium (mmol/L) | 0.20 ±0.08 | 0.15 ±0.05 |
| Chloride (mmol/L) | 16.40 ±2.08 | 18.09 ±7.38 |
| Bicarbonate (mmol/L) | 5.47 ±2.46 | 16.03 ±5.06 |
| Phosphate (mmol/L) | 5.69 ±1.91 | 2.70 ±0.55 |
| Thiocyanate (mmol/L) | 0.70 ±0.42 | 0.34 ±0.20 |
| Iodide (μmol/L) | NA | 13.8 ±8.5 |
| Fluoride (μmol/L) | 1.37 ±0.76 | 1.16 ±0.64 |
| Organic constituents | – | – |
| Total protein (mg/L) | 1630 ±720 | 1350 ±290 |
| Secretory IgA (mg/L) | 76.1 ±40.2 | 37.8 ±22.5 |
| MUC5B (mg/L) | 830 ±480 | 460 ±200 |
| MUC7 (mg/L) | 440 ±520 | 320 ±330 |
| Amylase (U=mg maltose/mL/min) | 317 ±290 | 453 ±390 |
| Lysozyme (mg/L) | 28.9 ±12.6 | 23.2 ±10.7 |
| Lactoferrin (mg/L) | 8.4 ±10.3 | 5.5 ±4.7 |
| Statherin (μmol/L) | 4.93 ±0.61 | NA |
| Albumin (mg/L) | 51.2 ±49.0 | 60.9 ±53.0 |
| Glucose (μmol/L) | 79.4 ±33.3 | 32.4 ±27.1 |
| Lactate (mmol/L) | 0.20 ±0.24 | 0.22 ±0.17 |
| Total lipids (mg/L) | 12.1 ±6.3 | 13.6 |
| Amino acids (μmol/L) | 780 | 567 |
| Urea (mmol/L) | 3.57 ±1.26 | 2.65 ±0.92 |
| Ammonia (mmol/L) | 6.86 | 2.57 ±1.64 |
Data show concentrations of salivary components in unstimulated and in mastication-stimulated saliva. Concentrations shown as mean ±standard deviation. Reproduced with permission from Saliva and Oral Health: An essential overview for the health professional, fourth edition16 and with grateful acknowledgment to C. Dawes. NA, not available.
The rate of saliva secretion can be modulated by different factors.18 Secretion of both unstimulated and stimulated saliva fluctuates in circadian rhythms, with peak flow in the late afternoon and the lowest flow rate during sleep.19 Taste, smell, and mastication all stimulate salivary secretion. Moreover, environmental conditions such as lower temperatures influence saliva flow rates.20,21
Given the variability in saliva flow rate and composition, proper collection requires standardization of time of day, type of stimulation, environmental conditions, and type of collection device. In addition, the sampling method, sample storage conditions, duration of time before analysis, and methods of analysis must be controlled.22-24
SALIVA COMPOSITION: MORE THAN JUST WATER
Human saliva is approximately 99% water, but the remaining 1% includes electrolytes, enzymes, hormones, nucleic acids, cytokines, antibodies, and sugars, yielding a far more complex biofluid.1 Many ions such as K+, Ca2+, HCO3−, Na+, Cl−, and PO43− fulfill important roles in saliva function. Saliva contains carbohydrates, blood-group substances, lipids, and vitamins, as well as many proteins, including alpha-amylase, mucins, lysozyme, immunoglobulin A (IgA), lactoferrin, proline-rich proteins, histatins, peroxidase, defensins, glycoproteins, lipoproteins, statherin, and matrix metalloproteases.1 However, the early estimates of nearly 3000 proteins present in whole saliva25-30 have been revised, as a large number are derived from sources other than the salivary glands.29,31 Importantly, microorganisms, desquamated epithelial cells, gingival crevicular fluid (GCF), serum, and food debris present in the oral cavity also contribute to the salivary proteome.1
Saliva composition varies between individuals and depends on a multitude of factors, including sex, age, health status, and time of day. Saliva pH, protein content, and lysozyme activity differ between men and women,32 and saliva composition and flow rate can vary with age.33 Salivary flow rates and saliva composition are altered by anticholinergic, sympathomimetic, and antihypertensive medications.34 Salivary disorders associated with decreased saliva flow include Sjögren’s syndrome, diabetes, depression, and Down syndrome.1 Alterations in salivary components vary with diseases such as cancer or diabetes and conditions such as obesity.35 Reports that the molecular profile of saliva reflects the physiological status of the individual36 have been widely embraced to promote saliva as a diagnostic fluid.
SALIVA: A COMPLEX BIOLOGICAL FLUID WITH MULTIPLE FUNCTIONS
Saliva fulfills a broad array of functions, which have been comprehensively described elsewhere.1,16,37 This review will focus on newly uncovered roles for saliva, particularly in wound healing, taste perception, and as a diagnostic fluid.1,37
INTERACTIONS BETWEEN SALIVA AND ORAL SURFACES
Saliva coats the oral soft tissues in what is known as the mucosal pellicle, a hydrogel-like layer made up of heavily glycosylated mucin proteins that trap and retain water to form a thick viscoelastic layer.37,38 The mucosal pellicle maintains lubrication in the oral cavity, the pharynx, and the esophagus, creating a barrier that protects oral tissues from dryness and mechanical stress.38 Notably, saliva from PG and from SMG and SLG has the same lubricating properties, but different viscosities, indicating that lubrication is not entirely dependent on mucins.39 Artificial saliva substitutes produced for patients with xerostomia often fail to replicate the sustained lubricating qualities of the mucosal pellicle in the oral cavity.40,41
The metabolism of ingested carbohydrates in the oral cavity results in a drop in pH,2 and below pH 5.5, tooth enamel erosion occurs.42 Saliva plays a central role in maintaining the oral pH in a range of 6.8 to 7.8 through the buffering capacities of bicarbonate (HCO3−)43 and phosphate.44 Bicarbonate and phosphate are important in the cyclic processes of demineralization and remineralization, which act to protect against dental caries. Salivary proteins such as statherin bind calcium or phosphate to maintain the supersaturation of these electrolytes in the saliva and to prevent excess deposition of calcium phosphate on tooth surfaces.45
When exposed to saliva, a thin organic film known as the acquired enamel pellicle (AEP) rapidly forms on the surface of tooth enamel. The AEP consists predominantly of salivary proteins complexed with glycoproteins, carbohydrates, and lipids,46,47 and oral bacteria contribute as well.48 The AEP forms a diffusion barrier that reduces calcium release from tooth enamel and protects against abrasion, erosion, demineralization, and dental caries.49 As an attachment site for initial colonizers of the dental biofilm, the AEP influences the composition of the oral microbiome.46
SALIVA AND ORAL INFECTION
The oral cavity is a major entry portal for pathogens and can be colonized by more than 700 different microbial species.50 Dozens of antimicrobial proteins and peptides involved in both innate and acquired immunity51 are secreted by the salivary glands, oral epithelial cells, and resident immune cells.52 The low frequency of infections arising after injuries in the oral cavity highlights the effectiveness of host defense mechanisms. However, as the antimicrobial proteins are present at minimal inhibitory concentrations, they do not completely eliminate the oral microbiome.37,52
The protective activity of these proteins varies. Defensins are cationic proteins which bind to bacteria; lysozyme hydrolyzes bacterial cell walls, resulting in lysis; cathelicidin binds bacterial toxins such as LPS; cystatins inactivate bacterial proteases; and lactoferrin, a Fe3+ chelator, inhibits microbial metabolic activity.52 The terminal sialic acids of mucins promote bacterial aggregation and the clearance of bacteria from the oral cavity53 and are implicated in the inhibition of HIV in the oral cavity.54 Histatins, salivary peptides produced only in humans and higher primates, are fungicidal55 and show potent antibacterial activity against common multidrug-resistant bacterial species.56 Human salivary glands also secrete immunoglobulins.7,29 IgA knockout mice showed an increased level of alveolar bone loss compared with wild-type control mice, which may suggest that salivary IgA plays a role in preventing periodontal disease.57 Some antimicrobial proteins are differentially regulated in the presence of periodontal disease, supporting their use as diagnostic biomarkers.52,58
In contrast with skin, soft tissues in the oral cavity heal rapidly with no scarring.59 Cells in the buccal mucosa turnover 2 times faster than those in skin epithelium.60 Saliva continuously lubricates the wound, reducing tissue dehydration and cell death, and provides various cytokines, chemokines, and growth factors to promote wound healing.61,62 Histatins are potent activators of wound healing63,64 and show therapeutic potential for promoting tissue repair.
SALIVA AND FOOD
Humans can detect 5 basic tastes: sour, salt, sweet, bitter, and umami,65 and recent work suggests that a sixth type of taste receptor detects free fatty acids.66 It is the interaction of saliva with food during bolus formation that informs the perception of taste. Saliva plays a central role by dissolving and diffusing food substances within the oral cavity.67 In humans, significant variations in flavor perception are related to differences in salivary protein composition.68 Hormones present in saliva, such as leptin, ghrelin, insulin, and glucagon, have been shown in animal models to modulate taste perception.67 Repeated exposure of mice to bitter compounds upregulates specific salivary proteins that alter taste, reducing sensitivity to such compounds.69 In humans, proline-rich proteins bind food substances such as tannins to modulate astringency.70 Numerous enzymes in saliva contribute to taste perception through the proteolysis of dietary proteins, and alterations in enzyme expression levels may underlie certain taste disorders. Taste receptors can be damaged by dryness or microbial infections, which affects taste perception in patients with hyposalivation.67
Saliva functions in the clearance of food debris from the oral cavity. The most abundant salivary protein, alpha-amylase, plays only a limited role in starch digestion71 and is likely more important in the dissolution and removal of food particles from the teeth.72 The use of sugar-free gum, which is positively linked to reduced dental caries,73 depends on mastication to stimulate saliva secretion.74 The increased incidence of dental caries in patients with salivary hypofunction is directly linked to reduced salivary clearance rates.37
SALIVA AS A DIAGNOSTIC TOOL
As a diagnostic fluid, saliva offers clear advantages over blood. Saliva collection is straightforward, noninvasive, and generally painless; does not require trained personnel or sterile equipment; and can be done by the participants themselves. Saliva presents significantly lower risks of inadvertent pathogenic infection than blood collection22 and is a noninvasive alternative for infants75 or individuals with mental illness.76 Saliva collection is widely used for drug and medical testing and for the analysis of genetic molecules and proteins.77 Desquamated epithelial cells and blood cells in the oral cavity are a ready source of human deoxyribonucleic acid (DNA), and microbial flora provide a unique set of bacterial species per individual, making saliva critical in forensic investigations.78,79
Major technical advances in salivary proteomics have enabled comparative profiling analyses and the identification of potential biomarkers. Salivary proteins are currently under investigation as diagnostic biomarkers for a wide variety of oral,80 as well as systemic, diseases.81 The current challenge is to unambiguously link disease biomarkers with specific physiological conditions.23
SALIVA AS A PREDICTOR OF ORAL DISEASE
The potential for exploiting specific salivary protein components as biomarkers in the diagnosis of oral diseases has long been recognized.82 Of particular interest is whether salivary biomarkers may be predictive of dental caries. To date, only weak evidence has linked caries with specific salivary components 83 or shown that saliva pH, buffering capacity, proteins, or electrolyte composition serve as effective indicators of the risk factors causing dental caries.
Periodontitis develops as a result of change in the host environment.84 Whether there is a link between saliva flow rates and periodontitis has been the subject of conflicting reports.85 Saliva functions in periodontitis both to promote bacterial adherence and AEP formation and to protect, through the activities of antimicrobial proteins, secreted antibodies and rapid clearance. Responses to periodontitis include increased inflammatory cytokines.86,87 In particular, interleukin-1β (IL-1β) and matrix metalloproteinase-8 (MMP-8) are significantly elevated in the whole saliva of patients with periodontitis and have been suggested as promising salivary biomarkers.88-91 However, because GCF passes through inflamed periodontal tissues before entering the sulcus, the current focus of most saliva-based tests for periodontal disease is the detection of biomarkers present at higher concentrations in the GCF (Fig. 2).92,93 A recently revised classification system to define the clinical stages of periodontitis94 is compatible with the inclusion of specific salivary biomarkers to distinguish progressive stages of the disease by severity.
Figure 2.

Illustration of how gingival crevicular fluid (GCF) passes through epithelial cells in periodontal tissues before entering periodontal pocket (black arrows). For patients with periodontal disease, GCF passing through inflamed tissues may accumulate higher concentrations of disease-specific biomarkers than present in whole saliva. Reprinted with permission from Barros et al. Periodontology 2000 (2015),92 ©John Wiley &Sons A/S. Published by John Wiley & Sons Ltd.
Saliva metabolome analysis has been used to detect metabolites associated with tissue breakdown, beta-oxidation, proinflammatory mediator production, pH regulation, reactive oxygen species generation, and subsequent antioxidative defense.95-97 However, while many promising disease-specific metabolites have been detected, an incomplete understanding of specific metabolic pathways associated with oral diseases remains a limitation. Human immunodeficiency virus (HIV) infection and antiretroviral therapies are associated with oral diseases, including periodontitis, necrotizing ulcerative gingivitis, oral candidiasis, hairy leukoplakia, and aphthous ulcers.98,99 More than 100 salivary biomarkers have been proposed for oral cancers.100,101 However, a majority of these, including interleukin 6 (IL-6), interleukin 10 (IL-10), tumor necrosis factor alpha (TNF-alpha), and interferon gamma (IFN-gamma), are inflammatory markers that are elevated in patients with various diseases, making them relatively nonspecific markers for cancer.102,103 The validation of biomarkers must first rule out compounding factors such as periodontitis, Sjögren’s syndrome, or stress, which also increase cytokine levels.
SALIVA AS A PREDICTOR OF SYSTEMIC DISEASES
The analysis of human saliva has been applied to the diagnosis of many systemic diseases. Extensive efforts are underway to validate novel salivary biomarkers for Sjögren’s syndrome,104 neurological diseases,105,106 early diagnosis of Alzheimer disease,107 diabetes,108 cardiovascular disease, and autoimmune disorders. A strong correlation between levels of salivary and blood glucose suggests that saliva can be used for monitoring blood glucose concentration.109,110 The link between periodontitis and type I diabetes suggests that further characterization of salivary biomarkers for both conditions may prove useful for screening the progression and control of diabetes.105,111
The quantity and enzymatic activity of salivary amylase vary widely among individuals. A recent study noted a positive correlation between the amylase gene copy number and high-starch or low-starch diets in various human populations,112 suggesting that expression levels of amylase may be linked to obesity, but extensive genomic analysis revealed no association between the 2.113
Childhood obesity is associated with a reduction in salivary gland flow,114 which has been attributed to an increase in proinflammatory cytokines secreted by adipocytes and macrophages that impair salivary gland function.115 Salivary redox biomarkers (uric acid, sulfhydryl groups) are altered in obese individuals,116 although studies relating salivary biomarkers of oxidative stress to obesity-related conditions such a hyperlipidemia, insulin resistance, or type 2 diabetes are so far inconclusive.117 Insulin, adiponectin, or resistin in saliva has been correlated with serum levels in patients with diabetes.118 Levels of antioxidants are similarly elevated in saliva and serum of patients with diabetes and chronic kidney disease.119
Because of the ease of collection, saliva analysis is a practical approach to evaluating mental stress in adults, most often by assaying for cortisol.120,121 Salivary cortisol is used as a biomarker for psychiatric disorders, including anxiety and depression, and for patients with high risk of schizophrenia.122 Salivary cortisol is also used to monitor stress in neonates under intensive care.123
Secretory protein release from the salivary glands is stimulated by sympathetic neural activity. For this reason, salivary alpha-amylase (sAA) has been proposed as a diagnostic marker for systemic stress.124 In the past 10 years, dozens of studies have been conducted to measure cortisol and sAA as markers of cardiovascular stress,125 although the reliability of sAA as a marker of stress has been challenged. sAA levels are linked to saliva flow rate, which is modulated both by sympathetic and parasympathetic signals.126 Notably, cortisol levels are under circadian control,127 and both markers can be influenced by various confounders, including age, sex, medication, health conditions, smoking, drinking, and sleep habits.
Saliva is a critical diagnostic fluid for the detection of viruses, including congenital cytomegalovirus,128 Epstein-Barr, hepatitis B,129 HIV,130-132 and human papilloma virus.133 Saliva is the focus of diagnostic tests for dengue,134 herpes simplex, and Zika viruses.135
SALIVA AND THE COVID-19 PANDEMIC
The recent COVID-19 pandemic clearly illustrates how central saliva can be in disease. The primary source of SARS-CoV-2 transmission is saliva, which is disseminated through aerosols produced by sneezing, coughing, speaking, singing, or contact with the mucous membranes of affected individuals.136,137 SARS-CoV-2 is present at high viral load in saliva and can be used for the rapid detection of virus ribonucleic acid (RNA) and antigens, as well as for antibodies produced against it.138,139 Saliva samples have proven as effective as mucosal samples collected from nasopharyngeal swabs in detecting SARS-CoV-2, and the ease of collection reduces the inadvertent exposure of health-care workers.140,141 Development of rapid test kits has simplified saliva-based testing for RNA or viral antigens.138-140,142-147 In addition, a highly sensitive test based on CRISPR-Cas13-RNA detection has recently been developed, which dramatically shortens the time to results.148
SARS-CoV-2 can be transmitted by asymptomatic, presymptomatic, and symptomatic individuals.141 Importantly, it has been demonstrated that saliva from asymptomatic individuals can be highly infectious.149 Furthermore, the virus may persist in saliva, after it is no longer detectable in nasopharyngeal swabs.149 These findings suggest that sites in the oral cavity may act as reservoirs of SARS-CoV-2 virus. The cellular viral targets required for infection by SARS-CoV-2, angiotensin-converting enzyme 2 (ACE2) and transmembrane serine protease 2 (TMPRSS) receptors, are broadly expressed in serous acinar and ductal epithelial cells of human PG and SMG.150,151 In addition, SARS-CoV-2 has been found in both major and minor SG.149 The detection of ACE2 expression in taste bud cells and throughout the oral cavity152,153 indicates that many epithelial cells can be targeted by the virus and may explain the loss of taste, a frequently reported symptom in COVID-19 patients.154
Given these challenges, it is imperative to understand the infection risks and follow guidelines for effective preventive measures in dental practice.136 Importantly, diagnostic markers for the detection of SARS-CoV-2 vary in a time-dependent manner.155
Owing to the delay between infection and onset of symptoms, infectivity should not be ruled out on the basis of RT-PCR tests alone.143,155-157 Mask wearing reduces salivary droplet spread more than 10-fold.149 The use of appropriate personal protective equipment combined with effective safety protocols significantly reduces the infection risk for dental health personnel.158
CONCLUSIONS
Advances in proteomics have expanded the understanding of the roles played by salivary proteins in taste, wound healing, and immune responses.
Technologies using saliva as a diagnostic fluid are rapidly being developed. Until recently, most commercially available detection platforms were enzyme-linked immunosorbent assay (ELISA)-based, but numerous devices for potential point-of-care screening and diagnostic systems159-161 now enable detection of multiple targets within a saliva sample.
Given the central role that saliva plays in maintaining oral health and the advantages of using saliva as a diagnostic tool, a general knowledge of basic saliva physiology is important in clinical practice.
Acknowledgments
Supported by the Training Program in Oral Sciences, R90DE022529 (HU), and R21DE026861 (CEO) from National Institute of Dental and Craniofacial Research (NIDCR/NIH).
REFERENCES
- 1.Pedersen AML, Sørensen CE, Proctor GB, Carpenter GH, Ekström J. Salivary secretion in health and disease. J Oral Rehabil 2018;45:730–46. [DOI] [PubMed] [Google Scholar]
- 2.Proctor GB, Carpenter GH. Salivary secretion: Mechanism and neural regulation. Monogr Oral Sci 2014;24:14–29. [DOI] [PubMed] [Google Scholar]
- 3.Melvin JE, Yule D, Shuttleworth T, Begenisich T. Regulation of fluid and electrolyte secretion in salivary gland acinar cells. Annu Rev Physiol 2005;67:445–69. [DOI] [PubMed] [Google Scholar]
- 4.Bullard T, Koek L, Roztocil E, Kingsley PD, Mirels L, Ovitt CE. Ascl3 expression marks a progenitor population of both acinar and ductal cells in mouse salivary glands. Dev Biol 2008;320:72–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kwak M, Alston N, Ghazizadeh S. Identification of stem cells in the secretory complex of salivary glands. J Dent Res 2016;95:776–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tandler B, Gresik EW, Nagato T, Phillips CJ. Secretion by striated ducts of mammalian major salivary glands: Review from an ultrastructural, functional, and evolutionary perspective. Anat Rec 2001;264:121–45. [DOI] [PubMed] [Google Scholar]
- 7.Redman RS. On approaches to the functional restoration of salivary glands damaged by radiation therapy for head and neck cancer, with a review of related aspects of salivary gland morphology and development. Biotech Histochem 2008;83:103–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Holmberg KV, Hoffman MP. Anatomy, biogenesis and regeneration of salivary glands. Monogr Oral Sci 2014;24:1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nanci A, TenCate AR. Ten Cate’s oral histology: Development, structure, and function. 9th ed. St. Louis: Missouri Elsevier; 2018. p. 236–59. [Google Scholar]
- 10.Kondo Y, Nakamoto T, Jaramillo Y, Choi S, Catalan MA, Melvin JE. Functional differences in the acinar cells of the murine major salivary glands. J Dent Res 2015;94:715–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Catalán MA, Nakamoto T, Melvin JE. The salivary gland fluid secretion mechanism. J Med Invest 2009;56(Suppl):192–6. [DOI] [PubMed] [Google Scholar]
- 12.Roussa E. Channels and transporters in salivary glands. Cell Tissue Res 2011;343:263–87. [DOI] [PubMed] [Google Scholar]
- 13.Proctor GB, Carpenter GH. Regulation of salivary gland function by autonomic nerves. Auton Neurosci 2007;133:3–18. [DOI] [PubMed] [Google Scholar]
- 14.Proctor GB. The physiology of salivary secretion. Periodontol 2000 2016;70:11–25. [DOI] [PubMed] [Google Scholar]
- 15.Sreebny LM, Vissink A. Dry mouth-The malevolent symptom: A clinical guide. Ames, Iowa: Wiley-Blackwell; 2010. p. 33–76. [Google Scholar]
- 16.Edgar M, Dawes C, O’Mullane D. Saliva and oral health an essential overview for the health professional fourth edition. Duns Tew: Stephen Hancocks Limited; 2012. p. 1–55. [Google Scholar]
- 17.Belstrøm D. The salivary microbiota in health and disease. J Oral Microbiol 2020;12:1723975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wolff A, Zuk-Paz L, Kaplan I. Major salivary gland output differs between users and non-users of specific medication categories. Gerodontology 2008;25:210–6. [DOI] [PubMed] [Google Scholar]
- 19.Dawes C. Circadian rhythms in human salivary flow rate and composition. J Physiol 1972;220:529–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ligtenberg AJM, Meuffels M, Veerman ECI. Effects of environmental temperature on saliva flow rate and secretion of protein, amylase and mucin 5B. Arch Oral Biol 2020;109:104593. [DOI] [PubMed] [Google Scholar]
- 21.Elishoov H, Wolff A, Kravel LS, Shiperman A, Gorsky M. Association between season and temperature and unstimulated parotid and submandibular/sublingual secretion rates. Arch Oral Biol 2008;53:75–8. [DOI] [PubMed] [Google Scholar]
- 22.Martí-Álamo S, Mancheño-Franch A, Marzal-Gamarra C, Carlos-Fabuel L. Saliva as a diagnostic fluid. Literature review. J Clin Exp Dent 2012;4:e237–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wang J, Schipper HM, Velly AM, Mohit S, Gornitsky M. Salivary biomarkers of oxidative stress: A critical review. Free Radic Biol Med 2015;85:95–104. [DOI] [PubMed] [Google Scholar]
- 24.Khurshid Z, Zohaib S, Najeeb S, Zafar MS, Slowey PD, Almas K. Human saliva collection devices for proteomics: An update. Int J Mol Sci 2016;17:846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Walz A, Stühler K, Wattenberg A, Hawranke E, Meyer HE, Schmalz G, et al. Proteome analysis of glandular parotid and submandibular-sublingual saliva in comparison to whole human saliva by two-dimensional gel electrophoresis. Proteomics 2006;6:1631–9. [DOI] [PubMed] [Google Scholar]
- 26.Denny P, Hagen FK, Hardt M, Liao L, Yan W, Arellanno M, et al. The proteomes of human parotid and submandibular/sublingual gland salivas collected as the ductal secretions. J Proteome Res 2008;7:1994–2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Gonzalez-Begne M, Lu B, Liao L, Xu T, Bedi G, Melvin JE, et al. Characterization of the human submandibular/sublingual saliva glycoproteome using lectin affinity chromatography coupled to multidimensional protein identification technology. J Proteome Res 2011;10:5031–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Grassl N, Kulak NA, Pichler G, Geyer PE, Jung J, Schubert S, et al. Ultra-deep and quantitative saliva proteome reveals dynamics of the oral microbiome. Genome Med 2016;8:44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Saitou M, Gaylord EA, Xu E, May AJ, Neznanova L, Nathan S, et al. Functional specialization of human salivary glands and origins of proteins intrinsic to human saliva. Cell Rep 2020;33:108402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Loo JA, Yan W, Ramachandran P, Wong DT. Comparative human salivary and plasma proteomes. J Dent Res 2010;89:1016–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ruhl S. The scientific exploration of saliva in the post-proteomic era: From database back to basic function. Expert Rev Proteomics 2012;9:85–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Prodan A, Brand HS, Ligtenberg AJ, Imangaliyev S, Tsivtsivadze E, van der Weijden F, et al. Interindividual variation, correlations, and sex-related differences in the salivary biochemistry of young healthy adults. Eur J Oral Sci 2015;123:149–57. [DOI] [PubMed] [Google Scholar]
- 33.Srivastava A, Wang J, Zhou H, Melvin JE, Wong DT. Age and gender related differences in human parotid gland gene expression. Arch Oral Biol 2008;53:1058–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Scully C. Drug effects on salivary glands: Dry mouth. Oral Dis 2003;9:165–76. [DOI] [PubMed] [Google Scholar]
- 35.Muñoz-González C, Feron G, Canon F. Main effects of human saliva on flavour perception and the potential contribution to food consumption. Proc Nutr Soc 2018;77:423–31. [DOI] [PubMed] [Google Scholar]
- 36.Wang A, Wang CP, Tu M, Wong DT. Oral biofluid biomarker research: Current status and emerging frontiers. Diagnostics (Basel) 2016;6:45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Dawes C, Pedersen AM, Villa A, Ekström J, Proctor GB, Vissink A, et al. The functions of human saliva: A review sponsored by the World Workshop on Oral Medicine VI. Arch Oral Biol 2015;60:863–74. [DOI] [PubMed] [Google Scholar]
- 38.Hannig C, Hannig M, Kensche A, Carpenter G. The mucosal pellicle - An underestimated factor in oral physiology. Arch Oral Biol 2017;80:144–52. [DOI] [PubMed] [Google Scholar]
- 39.Schipper RG, Silletti E, Vingerhoeds MH. Saliva as research material: Biochemical, physicochemical and practical aspects. Arch Oral Biol 2007;52:1114–35. [DOI] [PubMed] [Google Scholar]
- 40.See L, Mohammadi M, Han PP, Mulligan R, Enciso R. Efficacy of saliva substitutes and stimulants in the treatment of dry mouth. Spec Care Dentist 2019;39:287–97. [DOI] [PubMed] [Google Scholar]
- 41.Vinke J, Kaper HJ, Vissink A, Sharma PK. Dry mouth: Saliva substitutes which adsorb and modify existing salivary condition films improve oral lubrication. Clin Oral Investig 2020;24:4019–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Dawes C, Wong DTW. Role of saliva and salivary diagnostics in the advancement of oral health. J Dent Res 2019;98:133–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Lee MG, Ohana E, Park HW, Yang D, Muallem S. Molecular mechanism of pancreatic and salivary gland fluid and HCO3 secretion. Physiol Rev 2012;92:39–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Loke C, Lee J, Sander S, Mei L, Farella M. Factors affecting intra-oral pH - a review. J Oral Rehabil 2016;43:778–85. [DOI] [PubMed] [Google Scholar]
- 45.Siqueira WL, Oppenheim FG. Small molecular weight proteins/peptides present in the in vivo formed human acquired enamel pellicle. Arch Oral Biol 2009;54:437–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Siqueira WL, Custodio W, McDonald EE. New insights into the composition and functions of the acquired enamel pellicle. J Dent Res 2012;91:1110–8. [DOI] [PubMed] [Google Scholar]
- 47.Gibbins HL, Proctor GB, Yakubov GE, Wilson S, Carpenter GH. Concentration of salivary protective proteins within the bound oral mucosal pellicle. Oral Dis 2014;20:707–13. [DOI] [PubMed] [Google Scholar]
- 48.Lindh L, Aroonsang W, Sotres J, Arnebrant T. Salivary pellicles. Monogr Oral Sci 2014;24:30–9. [DOI] [PubMed] [Google Scholar]
- 49.Hannig M, Hannig C. The pellicle and erosion. Monogr Oral Sci 2014;25:206–14. [DOI] [PubMed] [Google Scholar]
- 50.Aas JA, Paster BJ, Stokes LN, Olsen I, Dewhirst FE. Defining the normal bacterial flora of the oral cavity. J Clin Microbiol 2005;43:5721–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Fábián TK, Hermann P, Beck A, Fejérdy P, Fábián G. Salivary defense proteins: Their network and role in innate and acquired oral immunity. Int J Mol Sci 2012;13:4295–320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Gorr SU. Antimicrobial peptides in periodontal innate defense. Front Oral Biol 2012;15:84–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Frenkel ES, Ribbeck K. Salivary mucins in host defense and disease prevention. J Oral Microbiol 2015;7:29759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Habte HH, Mall AS, de Beer C, Lotz ZE, Kahn D. The role of crude human saliva and purified salivary MUC5B and MUC7 mucins in the inhibition of Human Immunodeficiency Virus type 1 in an inhibition assay. Virol J 2006;3:99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Helmerhorst EJ, Alagl AS, Siqueira WL, Oppenheim FG. Oral fluid proteolytic effects on histatin 5 structure and function. Arch Oral Biol 2006;51:1061–70. [DOI] [PubMed] [Google Scholar]
- 56.Du H, Puri S, McCall A, Norris HL, Russo T, Edgerton M. Human salivary protein histatin 5 has potent bactericidal activity against ESKAPE pathogens. Front Cell Infect Microbiol 2017;7:41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Chang E, Kobayashi R, Fujihashi K, Komiya M, Kurita-Ochiai T. Impaired salivary SIgA antibodies elicit oral dysbiosis and subsequent induction of alveolar bone loss. Inflamm Res 2021;70:151–8. [DOI] [PubMed] [Google Scholar]
- 58.Khan SA, Fidel PL Jr, Thunayyan AA, Varlotta S, Meiller TF, Jabra-Rizk MA. Impaired histatin-5 levels and salivary antimicrobial activity against C. albicans in HIV infected individuals. J AIDS Clin Res 2013;4:1000193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Nikoloudaki G, Creber K, Hamilton DW. Wound healing and fibrosis: A contrasting role for periostin in skin and the oral mucosa. Am J Physiol Cell Physiol 2020;318:C1065–c77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Squier CA, Kremer MJ. Biology of oral mucosa and esophagus. J Natl Cancer Inst Monogr 2001:7–15. [DOI] [PubMed] [Google Scholar]
- 61.Behm B, Babilas P, Landthaler M, Schreml S. Cytokines, chemokines and growth factors in wound healing. J Eur Acad Dermatol Venereol 2012;26:812–20. [DOI] [PubMed] [Google Scholar]
- 62.Schenck K, Schreurs O, Hayashi K, Helgeland K. The role of nerve growth factor (NGF) and its precursor forms in oral wound healing. Int J Mol Sci 2017;18:386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Oudhoff MJ, Kroeze KL, Nazmi K, van den Keijbus PA, van ’t Hof W, Fernandez-Borja M, et al. Structure-activity analysis of histatin, a potent wound healing peptide from human saliva: Cyclization of histatin potentiates molar activity 1,000-fold. FASEB J 2009;23:3928–35. [DOI] [PubMed] [Google Scholar]
- 64.Shah D, Son KN, Kalmodia S, Lee BS, Ali M, Balasubramaniam A, et al. Wound healing properties of histatin-5 and identification of a functional domain required for histatin-5-induced cell migration. Mol Ther Methods Clin Dev 2020;17:709–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Niki M, Yoshida R, Takai S, Ninomiya Y. Gustatory signaling in the periphery: Detection, transmission, and modulation of taste information. Biol Pharm Bull 2010;33:1772–7. [DOI] [PubMed] [Google Scholar]
- 66.Mattes RD. Accumulating evidence supports a taste component for free fatty acids in humans. Physiol Behav 2011;104:624–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Neyraud E. Role of saliva in oral food perception. Monogr Oral Sci 2014;24:61–70. [DOI] [PubMed] [Google Scholar]
- 68.Canon F, Neiers F, Guichard E. Saliva and flavor perception: Perspectives. J Agric Food Chem 2018;66:7873–9. [DOI] [PubMed] [Google Scholar]
- 69.Martin LE, Kay KE, James KF, Torregrossa AM. Altering salivary protein profile can decrease aversive oromotor responding to quinine in rats. Physiol Behav 2020;223:113005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Canon F, Ballivian R, Chirot F, Antoine R, Sarni-Manchado P, Lemoine J, et al. Folding of a salivary intrinsically disordered protein upon binding to tannins. J Am Chem Soc 2011;133:7847–52. [DOI] [PubMed] [Google Scholar]
- 71.Fernández CI, Wiley AS. Rethinking the starch digestion hypothesis for AMY1 copy number variation in humans. Am J Phys Anthropol 2017;163:645–57. [DOI] [PubMed] [Google Scholar]
- 72.Carpenter GH. The secretion, components, and properties of saliva. Annu Rev Food Sci Technol 2013;4:267–76. [DOI] [PubMed] [Google Scholar]
- 73.Newton JT, Awojobi O, Nasseripour M, Warburton F, Di Giorgio S, Gallagher JE, et al. A systematic review and meta-analysis of the role of sugar-free chewing gum in dental caries. JDR Clin Trans Res 2020;5:214–23. [DOI] [PubMed] [Google Scholar]
- 74.Wessel SW, van der Mei HC, Maitra A, Dodds MW, Busscher HJ. Potential benefits of chewing gum for the delivery of oral therapeutics and its possible role in oral healthcare. Expert Opin Drug Deliv 2016;13:1421–31. [DOI] [PubMed] [Google Scholar]
- 75.Peña-Bautista C, Durand T, Vigor C, Oger C, Galano JM, Cháfer-Pericás C. Non-invasive assessment of oxidative stress in preterm infants. Free Radic Biol Med 2019;142:73–81. [DOI] [PubMed] [Google Scholar]
- 76.Kułak-Bejda A, Waszkiewicz N. Diagnostic value of salivary markers in neuropsychiatric disorders. Dis Markers 2019;2019:4360612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Khan RS, Khurshid Z, Yahya Ibrahim Asiri F. Advancing point-of-care (PoC) testing using human saliva as liquid biopsy. Diagnostics (Basel) 2017;7:39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.van Oorschot RAH, Szkuta B, Meakin GE, Kokshoorn B, Goray M. DNA transfer in forensic science: A review. Forensic Sci Int Genet 2019;38:140–66. [DOI] [PubMed] [Google Scholar]
- 79.Fábián TK, Fejérdy P, Csermely P. Salivary genomics, transcriptomics and proteomics: The emerging concept of the oral ecosystem and their use in the early diagnosis of cancer and other diseases. Curr Genomics 2008;9:11–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Melguizo-Rodríguez L, Costela-Ruiz VJ, Manzano-Moreno FJ, Ruiz C, Illescas-Montes R. Salivary biomarkers and their application in the diagnosis and monitoring of the most common oral pathologies. Int J Mol Sci 2020;21:5173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Qin R, Steel A, Fazel N. Oral mucosa biology and salivary biomarkers. Clin Dermatol 2017;35:477–83. [DOI] [PubMed] [Google Scholar]
- 82.Podzimek S, Vondrackova L, Duskova J, Janatova T, Broukal Z. Salivary markers for periodontal and general diseases. Dis Markers 2016;2016:9179632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Gao X, Jiang S, Koh D, Hsu CY. Salivary biomarkers for dental caries. Periodontol 2000 2016;70:128–41. [DOI] [PubMed] [Google Scholar]
- 84.Kinane DF, Attström R. Advances in the pathogenesis of periodontitis. Group B consensus report of the fifth European Workshop in Periodontology. J Clin Periodontol 2005;32(Suppl 6):130–1. [DOI] [PubMed] [Google Scholar]
- 85.Vallabhan CG, Sivarajan S, Shivkumar AD, Narayanan V, Vijayakumar S, Indhuja RS. Assessment of salivary flow rate in patients with chronic periodontitis. J Pharm Bioallied Sci 2020;12:S308–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Bassim CW, Redman RS, DeNucci DJ, Becker KL, Nylen ES. Salivary procalcitonin and periodontitis in diabetes. J Dent Res 2008;87:630–4. [DOI] [PubMed] [Google Scholar]
- 87.Ramseier CA, Kinney JS, Herr AE, Braun T, Sugai JV, Shelburne CA, et al. Identification of pathogen and host-response markers correlated with periodontal disease. J Periodontol 2009;80:436–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Gursoy UK, Könönen E, Uitto VJ, Pussinen PJ, Hyvärinen K, Suominen-Taipale L, et al. Salivary interleukin-1beta concentration and the presence of multiple pathogens in periodontitis. J Clin Periodontol 2009;36:922–7. [DOI] [PubMed] [Google Scholar]
- 89.Salminen A, Gursoy UK, Paju S, Hyvärinen K, Mäntylä P, Buhlin K, et al. Salivary biomarkers of bacterial burden, inflammatory response, and tissue destruction in periodontitis. J Clin Periodontol 2014;41:442–50. [DOI] [PubMed] [Google Scholar]
- 90.Sorsa T, Gursoy UK, Nwhator S, Hernandez M, Tervahartiala T, Leppilahti J, et al. Analysis of matrix metalloproteinases, especially MMP-8, in gingival creviclular fluid, mouthrinse and saliva for monitoring periodontal diseases. Periodontol 2000 2016;70:142–63. [DOI] [PubMed] [Google Scholar]
- 91.de Morais EF, Pinheiro JC, Leite RB, Santos PPA, Barboza CAG. Matrix metalloproteinase-8 levels in periodontal disease patients: A systematic review. J Periodontal Res 2018;53:156–63. [DOI] [PubMed] [Google Scholar]
- 92.Barros SP, Williams R, Offenbacher S, Morelli T. Gingival crevicular fluid as a source of biomarkers for periodontitis. Periodontol 2000 2016;70:53–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Ozeki M, Nozaki T, Aoki J, Bamba T, Jensen KR, Murakami S, et al. Metabolomic analysis of gingival crevicular fluid using gas chromatography/mass spectrometry. Mass Spectrom (Tokyo) 2016;5:A0047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J Periodontol 2018;89(Suppl 1):S159–72. [DOI] [PubMed] [Google Scholar]
- 95.Barnes VM, Ciancio SG, Shibly O, Xu T, Devizio W, Trivedi HM, et al. Metabolomics reveals elevated macromolecular degradation in periodontal disease. J Dent Res 2011;90:1293–7. [DOI] [PubMed] [Google Scholar]
- 96.Kuboniwa M, Sakanaka A, Hashino E, Bamba T, Fukusaki E, Amano A. Prediction of periodontal inflammation via metabolic profiling of saliva. J Dent Res 2016;95:1381–6. [DOI] [PubMed] [Google Scholar]
- 97.Mikkonen JJ, Singh SP, Herrala M, Lappalainen R, Myllymaa S, Kullaa AM. Salivary metabolomics in the diagnosis of oral cancer and periodontal diseases. J Periodontal Res 2016;51:431–7. [DOI] [PubMed] [Google Scholar]
- 98.Heron SE, Elahi S. HIV Infection and compromised mucosal immunity: Oral manifestations and systemic inflammation. Front Immunol 2017;8:241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Ryder MI, Shiboski C, Yao TJ, Moscicki AB. Current trends and new developments in HIV research and periodontal diseases. Periodontol 2000 2020;82:65–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Cheng YS, Rees T, Wright J. A review of research on salivary biomarkers for oral cancer detection. Clin Transl Med 2014;3:3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Roi A, Roi C, Negruţiu ML, Riviş M, Sinescu C, Rusu LC. The challenges of OSCC diagnosis: Salivary cytokines as potential biomarkers. J Clin Med 2020;9:2866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Rathnayake N, Akerman S, Klinge B, Lundegren N, Jansson H, Tryselius Y, et al. Salivary biomarkers for detection of systemic diseases. PLoS One 2013;8:e61356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Szabo YZ, Slavish DC, Graham-Engeland JE. The effect of acute stress on salivary markers of inflammation: A systematic review and meta-analysis. Brain Behav Immun 2020;88:887–900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Aqrawi LA, Galtung HK, Vestad B, Øvstebø R, Thiede B, Rusthen S, et al. Identification of potential saliva and tear biomarkers in primary Sjögren’s syndrome, utilising the extraction of extracellular vesicles and proteomics analysis. Arthritis Res Ther 2017;19:14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Aitken JP, Ortiz C, Morales-Bozo I, Rojas-Alcayaga G, Baeza M, Beltran C, et al. α-2-macroglobulin in saliva is associated with glycemic control in patients with type 2 diabetes mellitus. Dis Markers 2015;2015:128653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Farah R, Haraty H, Salame Z, Fares Y, Ojcius DM, Said Sadier N. Salivary biomarkers for the diagnosis and monitoring of neurological diseases. Biomed J 2018;41:63–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Klimiuk A, Maciejczyk M, Choromańska M, Fejfer K, Waszkiewicz N, Zalewska A. Salivary redox biomarkers in different stages of dementia severity. J Clin Med 2019;8:840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Tiongco RE, Bituin A, Arceo E, Rivera N, Singian E. Salivary glucose as a non-invasive biomarker of type 2 diabetes mellitus. J Clin Exp Dent 2018;10:e902–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Mussavira S, Dharmalingam M, Omana Sukumaran B. Salivary glucose and antioxidant defense markers in type II diabetes mellitus. Turk J Med Sci 2015;45:141–7. [DOI] [PubMed] [Google Scholar]
- 110.Naseri R, Mozaffari HR, Ramezani M, Sadeghi M. Effect of diabetes mellitus type 2 on salivary glucose, immunoglobulin A, total protein, and amylase levels in adults: A systematic review and meta-analysis of case-control studies. J Res Med Sci 2018;23:89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Kuehl MN, Rodriguez H, Burkhardt BR, Alman AC. Tumor necrosis factor-α, matrix-metalloproteinases 8 and 9 levels in the saliva are associated with increased hemoglobin A1c in type 1 diabetes subjects. PLoS One 2015;10:e0125320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Perry GH, Dominy NJ, Claw KG, Lee AS, Fiegler H, Redon R, et al. Diet and the evolution of human amylase gene copy number variation. Nat Genet 2007;39:1256–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Usher CL, Handsaker RE, Esko T, Tuke MA, Weedon MN, Hastie AR, et al. Structural forms of the human amylase locus and their relationships to SNPs, haplotypes and obesity. Nat Genet 2015;47:921–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Modéer T, Blomberg CC, Wondimu B, Julihn A, Marcus C. Association between obesity, flow rate of whole saliva, and dental caries in adolescents. Obesity (Silver Spring) 2010;18:2367–73. [DOI] [PubMed] [Google Scholar]
- 115.Lundin M, Yucel-Lindberg T, Dahllöf G, Marcus C, Modéer T. Correlation between TNFalpha in gingival crevicular fluid and body mass index in obese subjects. Acta Odontol Scand 2004;62:273–7. [DOI] [PubMed] [Google Scholar]
- 116.Chielle EO, Casarin JN. Evaluation of salivary oxidative parameters in overweight and obese young adults. Arch Endocrinol Metab 2017;61:152–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Zalewska A, Kossakowska A, Taranta-Janusz K, Zięba S, Fejfer K, Salamonowicz M, et al. Dysfunction of salivary glands, disturbances in salivary antioxidants and increased oxidative damage in saliva of overweight and obese adolescents. J Clin Med 2020;9:548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Desai GS, Mathews ST. Saliva as a non-invasive diagnostic tool for inflammation and insulin-resistance. World J Diabetes 2014;5:730–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Ben-Zvi I, Green Y, Nakhoul F, Kanter Y, Nagler RM. Effects of diabetes mellitus, chronic renal failure and hemodialysis on serum and salivary antioxidant status. Nephron Clin Pract 2007;105:c114–20. [DOI] [PubMed] [Google Scholar]
- 120.Obayashi K. Salivary mental stress proteins. Clin Chim Acta 2013;425:196–201. [DOI] [PubMed] [Google Scholar]
- 121.Giacomello G, Scholten A, Parr MK. Current methods for stress marker detection in saliva. J Pharm Biomed Anal 2020;191:113604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Coulon N, Brailly-Tabard S, Walter M, Tordjman S. Altered circadian patterns of salivary cortisol in individuals with schizophrenia: A critical literature review. J Physiol Paris 2016;110:439–47. [DOI] [PubMed] [Google Scholar]
- 123.Peña-Bautista C, Escrig R, Lara I, García-Blanco A, Cháfer-Pericás C, Vento M. Non-invasive monitoring of stress biomarkers in the newborn period. Semin Fetal Neonatal Med 2019;24:101002. [DOI] [PubMed] [Google Scholar]
- 124.Nater UM, Rohleder N. Salivary alpha-amylase as a non-invasive biomarker for the sympathetic nervous system: Current state of research. Psychoneuroendocrinology 2009;34:486–96. [DOI] [PubMed] [Google Scholar]
- 125.Cozma S, Dima-Cozma LC, Ghiciuc CM, Pasquali V, Saponaro A, Patacchioli FR. Salivary cortisol and α-amylase: Subclinical indicators of stress as cardiometabolic risk. Braz J Med Biol Res 2017;50:e5577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Nagy T, van Lien R, Willemsen G, Proctor G, Efting M, Fülöp M, et al. A fluid response: Alpha-amylase reactions to acute laboratory stress are related to sample timing and saliva flow rate. Biol Psychol 2015;109:111–9. [DOI] [PubMed] [Google Scholar]
- 127.Harrison RF, Debono M, Whitaker MJ, Keevil BG, Newell-Price J, Ross RJ. Salivary cortisone to estimate cortisol exposure and sampling frequency required based on serum cortisol measurements. J Clin Endocrinol Metab 2019;104:765–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Ross SA, Ahmed A, Palmer AL, Michaels MG, Sánchez PJ, Bernstein DI, et al. Detection of congenital cytomegalovirus infection by real-time polymerase chain reaction analysis of saliva or urine specimens. J Infect Dis 2014;210:1415–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Cruz HM, da Silva EF, Villela-Nogueira CA, Nabuco LC, do Ó KM, Lewis-Ximenez LL, et al. Evaluation of saliva specimens as an alternative sampling method to detect hepatitis B surface antigen. J Clin Lab Anal 2011;25:134–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Fransen K, Vermoesen T, Beelaert G, Menten J, Hutse V, Wouters K, et al. Using conventional HIV tests on oral fluid. J Virol Methods 2013;194:46–51. [DOI] [PubMed] [Google Scholar]
- 131.Bohórquez SP, Díaz J, Rincón CM, Estupiñán M, Chaparro M, Low-Calle AM, et al. Shedding of HSV-1, HSV-2, CMV, and EBV in the saliva of hematopoietic stem cell transplant recipients at Fundación HOMI - Hospital de la Misericordia, Bogotá, D.C. Biomedica 2016;36:201–10. [DOI] [PubMed] [Google Scholar]
- 132.Corstjens PL, Abrams WR, Malamud D. Saliva and viral infections. Periodontol 2000 2016;70:93–110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Qureishi A, Ali M, Fraser L, Shah KA, Møller H, Winter S. Saliva testing for human papilloma virus in oropharyngeal squamous cell carcinoma: A diagnostic accuracy study. Clin Otolaryngol 2018;43:151–7. [DOI] [PubMed] [Google Scholar]
- 134.Andries AC, Duong V, Ly S, Cappelle J, Kim KS, Lorn Try P, et al. Value of routine Dengue diagnostic tests in urine and saliva specimens. PLoS Negl Trop Dis 2015;9:e0004100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Khurshid Z, Zafar M, Khan E, Mali M, Latif M. Human saliva can be a diagnostic tool for Zika virus detection. J Infect Public Health 2019;12:601–4. [DOI] [PubMed] [Google Scholar]
- 136.Meng L, Hua F. Coronavirus disease 2019 (COVID-19): Emerging and future challenges for dental and oral medicine. J Dent Res 2020;99:481–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 137.Zhang R, Li Y. Identifying airborne transmission as the dominant route for the spread of COVID-19. Proc Natl Acad Sci USA 2020;117:14857–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Azzi L, Carcano G, Gianfagna F, Grossi P, Gasperina DD, Genoni A, et al. Saliva is a reliable tool to detect SARS-CoV-2. J Infect 2020;81:e45–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.To KK, Tsang OT, Yip CC, Chan KH, Wu TC, Chan JM, et al. Consistent detection of 2019 novel coronavirus in saliva. Clin Infect Dis 2020;71:841–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Fernandes LL, Pacheco VB, Borges L, Athwal HK, de Paula Eduardo F, Bezinelli L, et al. Saliva in the diagnosis of COVID-19: A review and new research directions. J Dent Res 2020;99:1435–43. [DOI] [PubMed] [Google Scholar]
- 141.Wyllie AL, Fournier J, Casanovas-Massana A. Saliva or Nasopharyngeal Swab Specimens for Detection of SARS-CoV-2. N Engl J Med 2020;383:1283–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Vogels CBF, Watkins AE, Harden CA, Brackney DE, Shafer J, Wang J, et al. SalivaDirect: A simplified and flexible platform to enhance SARS-CoV-2 testing capacity. Med (N Y) 2021;2:263–80.e6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Nagura-Ikeda M, Imai K. Clinical Evaluation of Self-Collected Saliva by Quantitative Reverse Transcription-PCR (RT-qPCR), Direct RT-qPCR, Reverse Transcription-Loop-Mediated Isothermal Amplification, and a Rapid Antigen Test To Diagnose COVID-19. J Clin Microbiol 2020;58:e01438. 20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Pisanic N, Randad PR, Kruczynski K, Manabe YC, Thomas DL, Pekosz A. COVID-19 Serology at Population Scale: SARS-CoV-2-Specific Antibody Responses in Saliva. J Clin Microbiol 2020;59:e02204–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Azzi L, Maurino V, Baj A, Dani M, d’Aiuto A, Fasano M, et al. Diagnostic Salivary Tests for SARS-CoV-2. J Dent Res 2021;100:115–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Asai N, Sakanashi D, Ohashi W, Nakamura A, Kawamoto Y, Miyazaki N, et al. Efficacy and validity of automated quantitative chemiluminescent enzyme immunoassay for SARS-CoV-2 antigen test from saliva specimen in the diagnosis of COVID-19. J Infect Chemother 2021;27:1039–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.MacMullan MA, Chellamuthu P, Mades A, Das S, Turner F, Slepnev VI, et al. Detection of SARS-CoV-2 Antibodies in Oral Fluid Obtained Using a Rapid Collection Device. J Clin Microbiol 2021;59:e02510–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 148.Shinoda H, Taguchi Y, Nakagawa R, Makino A, Okazaki S, Nakano M, et al. Amplification-free RNA detection with CRISPR–Cas13. Commun Biol 2021;4:476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Huang N, Pérez P, Kato T. SARS-CoV-2 infection of the oral cavity and saliva. Nat Med 2021;27:892–903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Matuck BF, Dolhnikoff M, Duarte-Neto A, Maia G, Gomes S, Sendyk D, et al. Salivary glands are a target for SARS-CoV-2: A source for saliva contamination. J Pathol 2021;254:239–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Hoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020;181:271–80.e8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 152.Sakaguchi W, Kubota N, Shimizu T, Saruta J. Existence of SARS-CoV-2 entry molecules in the oral cavity. Int J Mol Sci 2020;21:6000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Xu H, Zhong L, Deng J, Peng J, Dan H, Zeng X, et al. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int J Oral Sci 2020;12:8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Amorim Dos Santos J, Normando AGC, Carvalho da Silva RL, Acevedo AC, De Luca Canto G, Sugaya N, et al. Oral Manifestations in Patients with COVID-19: A Living Systematic Review. J Dent Res 2021;100:141–54. [DOI] [PubMed] [Google Scholar]
- 155.Sethuraman N, Jeremiah SS, Ryo A. Interpreting diagnostic tests for SARS-CoV-2. JAMA 2020;323:2249–51. [DOI] [PubMed] [Google Scholar]
- 156.Kucirka LM, Lauer SA, Laeyendecker O, Boon D, Lessler J. Variation in false-negative rate of reverse transcriptase polymerase chain reaction-based SARS-CoV-2 tests by time since exposure. Ann Intern Med 2020;173:262–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157.Ishii T, Sasaki M, Yamada K, Kato D, Osuka H, Aoki K, et al. Immunochromatography and chemiluminescent enzyme immunoassay for COVID-19 diagnosis. J Infect Chemother 2021;27:915–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 158.Ren Y, Feng C, Rasubala L, Malmstrom H, Eliav E. Risk for dental healthcare professionals during the COVID-19 global pandemic: An evidence-based assessment. J Dent 2020;101:103434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 159.Priye A, Bird SW, Light YK, Ball CS, Negrete OA, Meagher RJ. A smartphone-based diagnostic platform for rapid detection of Zika, Chikungunya, and Dengue viruses. Sci Rep 2017;7:44778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160.Garg N, Boyle D, Randall A, Teng A, Pablo J, Liang X, et al. Rapid immunodiagnostics of multiple viral infections in an acoustic microstreaming device with serum and saliva samples. Lab Chip 2019;19:1524–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161.Li X, Pomares C, Peyron F, Press CJ, Ramirez R, Geraldine G, et al. Plasmonic gold chips for the diagnosis of Toxoplasma gondii, CMV, and rubella infections using saliva with serum detection precision. Eur J Clin Microbiol Infect Dis 2019;38:883–90. [DOI] [PubMed] [Google Scholar]