

Abstract
Background
Previous research showed that computerized cognitive behavioral therapy can effectively reduce depressive symptoms. Some mental health apps incorporate gamification into their app design, yet it is unclear whether features differ in their effectiveness to reduce depressive symptoms over and above mental health apps without gamification.
Objective
The aim of this study was to determine whether mental health apps with gamification elements differ in their effectiveness to reduce depressive symptoms when compared to those that lack these elements.
Methods
A meta-analysis of studies that examined the effect of app-based therapy, including cognitive behavioral therapy, acceptance and commitment therapy, and mindfulness, on depressive symptoms was performed. A total of 5597 articles were identified via five databases. After screening, 38 studies (n=8110 participants) remained for data extraction. From these studies, 50 total comparisons between postintervention mental health app intervention groups and control groups were included in the meta-analysis.
Results
A random effects model was performed to examine the effect of mental health apps on depressive symptoms compared to controls. The number of gamification elements within the apps was included as a moderator. Results indicated a small to moderate effect size across all mental health apps in which the mental health app intervention effectively reduced depressive symptoms compared to controls (Hedges g=–0.27, 95% CI –0.36 to –0.17; P<.001). The gamification moderator was not a significant predictor of depressive symptoms (β=–0.03, SE=0.03; P=.38), demonstrating no significant difference in effectiveness between mental health apps with and without gamification features. A separate meta-regression also did not show an effect of gamification elements on intervention adherence (β=–1.93, SE=2.28; P=.40).
Conclusions
The results show that both mental health apps with and without gamification elements were effective in reducing depressive symptoms. There was no significant difference in the effectiveness of mental health apps with gamification elements on depressive symptoms or adherence. This research has important clinical implications for understanding how gamification elements influence the effectiveness of mental health apps on depressive symptoms.
Keywords: depression, reward, gamification, mental health apps, apps
Introduction
Depression is a highly prevalent mental disorder in the United States that affects 17.3 million people [1]. Effective treatments are available to treat depression, including pharmacotherapy and psychological treatment [2,3]. However, widespread barriers to treatment exist, such as problems of consistent adherence, access to mental health care resources, and cost [4-7]. The United States alone spends approximately US $71 billion annually on depression treatment [8], which underscores the substantial financial burden that depression can incur. Furthermore, of all adult Americans who experienced a major depressive episode in 2017, 35% did not receive treatment [1].
To mitigate these challenges, companies have created technology-based mental health apps, with the goal of alleviating symptoms of various mental disorders [8,9]. As of 2019, 81% of all Americans owned a smartphone, which highlights the potential impact of technology-based mental health apps: providing a platform, consuming less time, requiring less commitment, and allowing users to move at their own pace [10]. This ubiquity suggests that app technology could make treatment more accessible by providing individuals with cost-efficient tools and apps to aid them between sessions. However, development of these apps is recent and additional attention is needed to identify what is most effective and rewarding about these digital tool kits.
People with depression frequently experience anhedonia, which may result in blunted sensitivity to reward [11-15]. Depressed individuals view rewards, like money or social encouragement, as less motivating than individuals without depressive symptoms [16-18]. Effective therapeutic approaches may benefit from improving this reward-processing deficit, potentially through the use of gamification elements. Gamification is defined as the use of game-design elements and incentives combined with desired behaviors in order to positively influence user motivation, behavior of users, and adherence [19-22]. Previous research suggests that different gamification elements represent motivational affordances that can influence psychological outcomes [23]. These elements include leaderboards, achievements, badges, levels, challenges, and points [23]. The Unified Gamification and Motivation (UGM) model lends a framework for understanding how including gamification elements in therapeutic intervention can enhance treatment engagement [24]. Based on this model, the inclusion of game-like elements would make the intervention more salient, which could increase motivation to use the intervention, thereby resulting in greater treatment usage.
Much of the work demonstrating the effects of gamification elements on reward motivation stems from video game research. For example, in a recent study, young adults were randomized to either a video game training or a control task [25]. After 2 months playing the video game, participants randomized to the video game intervention exhibited higher activation in the ventral striatum (ie, increase in reward activation) during a nongamified task than those assigned to the control task at 2 months posttest. This finding suggests that (1) the effect of video games on reward motivation can transfer to other tasks and (2) video games can enhance individuals’ general reward responsiveness to positive stimuli [25]. However, very little research has centered on how individuals suffering from depression are motivated to pursue reward and engage in video games. The capability of video games to enhance reward processing, motivation, and engagement could play a critical role in the development of app technology specifically grappling with anhedonia.
Mental health apps provide a potential way to reduce symptoms and increase adherence by dispensing psychoeducation and other therapeutic skills through an electronic, easily accessible format [26-34]. Some apps include reward-based features, in the form of money, games, or hearts (eg, SPARX-R) [35], while other apps do not mention any type of reward (eg, AI Tess) [36]. Yet, these apps appear effective overall; in an initial meta-analysis collecting data from nine randomized controlled trials (RCTs) with depression as a secondary concern (mean age 36.1 years; male, 34.8%), results indicated that mental health apps led to a large reduction in depressive symptoms [30]. A second meta-analysis (19 RCTs; mean age 30.7 years; female, 63.17%) examined the effect of smartphone mental health apps on a variety of disorders (eg, anxiety, substance use, and sleep problems) including depression, and results showed significant differences between groups in reducing depressive symptoms with a small to moderate effect size [37]. Another meta-analysis, which predominately recruited adults over the age of 16 years (93.3%), examined 45 RCTs with various technological interventions for depressive patients, like symptom tracking, online diaries, and email and phone reminders. Depressive symptoms showed significant reductions in comparison to either wait-list or treatment-as-usual controls [38]. Taken together, there is evidence that mental health apps are effective, but the variability in effect size between meta-analyses suggest there could be another mechanism. Given the UGM model, gamification is a logical next step to replicate prior meta-analyses and add further context. Mental health apps offer a novel, easily accessible way to combine therapy techniques and motivational reward elements, like a video game, yet it is unclear whether reward or gamification features uniquely offer additional advantages in reducing depressive symptoms. Pairing this novel app approach with traditional techniques that are effective for depression may be able to mitigate anhedonia symptoms.
The purpose of this systematic review and meta-analysis is to (1) provide a comprehensive and updated meta-analytical evaluation of the effectiveness of mental health apps in reducing depressive symptoms and (2) to assess whether mental health apps with gamification elements are more effective than those without. Prior research on video games, like apps, indicates high levels of reward motivation and pleasure [25,39]. Additionally, previous systematic reviews and meta-analyses have shown significant reductions in symptoms for depression and other mental disorders while using mental health apps, some of which included cognitive behavioral therapy (CBT) or gamification elements [26,36,37,40,41]. However, no study to date has explored the effectiveness of mental health apps with gamification components in mitigating depressive symptoms.
Previous research shows that gamification can increase motivation to engage with mental health apps [42-44], improve mood [45], and activate the ventral striatum, which can enhance individuals’ general reward responsiveness to positive stimuli [21]. Building on this research, we propose that gamification may enhance the efficacy of therapeutic-based apps (eg, CBT) and reduce depressive symptoms through the following mechanism: (1) it might increase engagement with and adherence to mental health apps and (2) it may activate reward-mediated neural pathways, eliciting positive feelings, which might counteract some negative feelings from depression. We hypothesize that mental health apps that include gamification elements will be more effective in reducing depressive symptoms and increasing adherence than those without such elements.
Methods
Overview
The systematic review and meta-analysis were conducted following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [46]. A protocol was designed and registered through the Open Science Framework after data collection and before data extraction and analysis began [47]. The quality of the studies included was assessed through the Cochrane Collaboration’s risk of bias assessment tool [48].
Eligibility and Inclusion Criteria
Studies were included if they met the following criteria: (1) studies involving human participants; (2) mental health apps targeting depression as a primary, secondary, or tertiary outcome; (3) RCTs or experimental or quasi-experimental designs with an active, wait-list, or treatment-as-usual control group; (4) published between January 1, 2005, and December 31, 2020; (5) mental health app intervention groups contain elements of CBT, acceptance and commitment therapy (ACT), behavioral activation (BA), or mindfulness; and (6) provide a measure of depressive symptoms pre- and posttreatment. Studies were excluded if they (1) were books chapters, meta-analyses, reviews, case studies, or opinion pieces; (2) were not written in English; (3) included participants younger than 18 years of age; (4) included participants with a terminal or life-threatening illness (eg, patients with cancer who had depression) to avoid potential confounds of disentangling which condition (ie, life-threatening illness or depression) influenced outcomes; and (5) included a therapist or other mental health specialist’s guidance for the mental health apps, as this could create a confound. No specific measure of depression was required, in order to allow the focus to remain on the mental health apps.
Literature Search Strategy
Studies were identified through a comprehensive literature search in PubMed, PsycInfo, Cochrane Clinical Trials Registry, Web of Science, and PsyArXiv (for publication bias) with no publication date restriction. The search was conducted in February 2021. Additionally, the authors conducted a manual search to locate studies that were not identified through databases. Search terms used three different concepts critical to the extant literature: app-based, mental health, and reward or gamification. Within each concept (eg, app-based), we identified multiple tags that reflected this concept (eg, “mental health app” and “MHapp”). The specific combination of operators can be found in Multimedia Appendix 1. This resulted in 129 unique combinations of search terms (eg, “MHapp-Money” and “Depression-Points”).
Study Selection Procedure
During the identification phase, articles were identified and collected based on the search term combinations from the five databases. After duplicate removal, two researchers (SGS and KAB) independently conducted initial screening for eligible articles by assessing titles and abstracts for inclusion or exclusion criteria (Multimedia Appendix 2). After the initial screening, both researchers independently assessed the remaining full-text articles against the inclusion and exclusion criteria. Disagreements were resolved through re-examination of the articles in question and discussion among the screeners.
Data Extraction
Two independent reviewers independently coded the studies in a Microsoft Excel spreadsheet. The following data were extracted from each article: first author, year of publication, participants’ characteristics (ie, gender and age), population, and study length (Multimedia Appendix 3), as well as app name, app classification (ie, mobile or internet), presence of gamification elements, type of gamification element (eg, digital rewards, challenge or game, and competition or challenges), app adherence, the instrument used to measure depression, and type of therapy (eg, CBT and ACT) offered (Table 1) [31,49-85].
Table 1.
Study app classification, therapy, and gamification information.
| First author, publication year, and app | App classification | Depression measure | Therapy intervention | Game elements, n | Adherence rate, % | |
| Bakker, 2018 [54] | ||||||
|
|
MoodMission | Mobile | PHQ-9a | CBTb | 2 | 69.6 |
|
|
MoodPrism | Mobile | PHQ-9 | CBT | 2 | 46.4 |
|
|
MoodKit | Mobile | PHQ-9 | CBT | 0 | 46.0 |
| Berger, 2011 [85] | ||||||
|
|
Deprexis | Mobile | BDI-IIc | BAd, PSTe, and mindfulness | 1 | N/Af |
| Birney, 2016 [80] | ||||||
|
|
Moodhacker | Internet | PHQ-9 | Mindfulness | 0 | N/A |
| Bosso, 2020 [67] | ||||||
|
|
Headspace | Mobile | DASS-21g | Mindfulness | 3 | 58.0 |
| Bostock, 2019 [68] | ||||||
|
|
Headspace | Mobile | HADSh | Mindfulness | 3 | 2.0 |
| Botella, 2016 [57] | ||||||
|
|
Smiling is Fun | Internet | BDI-II | CBT | 1 | 86.4 |
| Choi, 2012 [81] | ||||||
|
|
Brighten Your Mood | Internet | CBDIi | CBT | 0 | 68.0 |
| Collins, 2018 [51] | ||||||
|
|
MindWise | Internet | PHQ-9 | CBT | 0 | 41.7 |
| Dahne, 2019 [66] | ||||||
|
|
Aptivate | Mobile | BDI-II | CBT | 2 | 36.4 |
|
|
iCouch CBT | Mobile | BDI-II | CBT | 0 | N/A |
| Dahne, 2019 [77] | ||||||
|
|
Moodivate | Mobile | BDI-II | CBT | 2 | 42.9 |
|
|
Moodkit | Mobile | BDI-II | BA | 0 | N/A |
| Deady, 2020 [78] | ||||||
|
|
HeadGear | Internet | PHQ-9 | BA and mindfulness | 2 | 10.1 |
| de Graaf, 2009 [62] | ||||||
|
|
Colour Your Life | Internet | BDI-II | CBT | 0 | 36.0 |
| Fish, 2019 [53] | ||||||
|
|
Headspace | Mobile | PHQ-9 | Mindfulness | 3 | N/A |
| Flett, 2018 [69] | ||||||
|
|
Headspace | Mobile | CES-Dj | Mindfulness | 3 | 16.4 |
|
|
Smiling Mind | Mobile | CES-D | Mindfulness | 1 | 15.4 |
|
|
Evernote | Mobile | CES-D | N/A | 0 | N/A |
| Fuller-Tyszkiewicz, 2020 [73] | ||||||
|
|
StressLess | Mobile | DASS-21 | Mindfulness-based CBT | 1 | 19.0 |
|
|
Stress Monitor | Mobile | DASS-21 | N/A | 1 | N/A |
| Gilbody, 2015 [63] | ||||||
|
|
Beating the Blues | Internet | PHQ-9 | CBT | 0 | 79.0 |
|
|
MoodGYM | Internet | PHQ-9 | CBT | 2 | 75.0 |
| Ha, 2020 [49] | ||||||
|
|
Spring | Mobile | BDI-II | CBT | 1 | N/A |
| Howells, 2016 [56] | ||||||
|
|
Headspace | Mobile | CES-D | Mindfulness | 3 | 29.8 |
|
|
Catch Notes | Mobile | CES-D | N/A | 0 | N/A |
| Hur, 2018 [72] | ||||||
|
|
Todac Todac | Mobile | BDI-II | CBT | 3 | N/A |
| Kladnitski, 2020 [71] | ||||||
|
|
iCBTk program | Mobile | PHQ-9 | CBT and mindfulness | 2 | 69.4 |
|
|
MEiCBTl program | Mobile | PHQ-9 | CBT and mindfulness | 2 | 69.7 |
|
|
iMTm program | Mobile | PHQ-9 | CBT and mindfulness | 2 | 67.6 |
| Krafft, 2019 [58] | ||||||
|
|
Simple Matrix | Internet | DASS-21 | ACTn | 1 | 42.9 |
|
|
Complex Matrix | Internet | DASS-21 | ACT | 2 | 40.0 |
| Levin, 2020 [75] | ||||||
|
|
Stop, Breathe, & Think | Internet | CCAPS-34o | Mindfulness | 0 | 63.0 |
| Lintvedt, 2013 [79] | ||||||
|
|
MoodGYM | Mobile | CES-D | CBT | 2 | N/A |
|
|
Blue Pages | Mobile | CES-D | N/A | 0 | N/A |
| Löbner, 2018 [64] | ||||||
|
|
MoodGYM | Internet | PHQ-9 | CBT | 2 | 13.0 |
| Lokman, 2017 [60] | ||||||
|
|
CDMIsp: Sleep Better, Worry Less, and Stress Less | Mobile | IDS-SRq | CBT | 1 | N/A |
| Lüdtke, 2018 [59] | ||||||
|
|
Be Good to Yourself | Internet | PHQ-9 | CBT | 3 | 79.6 |
| Mantani, 2017 [52] | ||||||
|
|
Kokoro | Mobile | BDI-II | CBT | 6 | 40.7 |
| McCloud, 2020 [70] | ||||||
|
|
Feel Stress Free | Internet | HADS | CBT and mindfulness | 2 | 7.0 |
| Moberg, 2019 [61] | ||||||
|
|
Pacifica | Internet | DASS-21 | CBT and mindfulness | 3 | N/A |
| Montero-Marín, 2016 [82] | ||||||
|
|
Smiling is Fun | Internet | BDI-II | CBT | 1 | 84.3 |
| Richards, 2020 [55] | ||||||
|
|
Space from Depression | Internet | PHQ-9 | CBT | 2 | N/A |
| Richards, 2015 [83] | ||||||
|
|
Space from Depression | Internet | BDI-II | CBT | 2 | 36.0 |
| Roepke, 2015 [31] | ||||||
|
|
SuperBetter | Internet | CES-D | CBT | 7 | 45.6 |
| Rollman, 2018 [84] | ||||||
|
|
Beating the Blues | Internet | PROMISr | CBT | 0 | 85.8 |
| Schure, 2019 [76] | ||||||
|
|
Thrive | Mobile | PHQ-9 | CBT | 3 | 58.6 |
| Sethi, 2013 [65] | ||||||
|
|
MoodGYM | Mobile | DASS-21 | CBT | 2 | N/A |
| Tighe, 2017 [74] | ||||||
|
|
ibobbly | Mobile | PHQ-9 | Mindfulness and ACT | 0 | 85.0 |
| Twomey, 2014 [50] | ||||||
|
|
MoodGYM | Internet | DASS-21 | CBT | 2 | 27.3 |
aPHQ-9: 9-item Patient Health Questionnaire.
bCBT: cognitive behavioral therapy.
cBDI-II: Beck Depression Inventory-II.
dBA: behavioral activation.
ePST: problem-solving therapy.
fN/A: not applicable; values were not reported.
gDASS-21: 21-item Depression, Anxiety, and Stress Scale.
hHADS: Hospital Anxiety and Depression Scale.
iCBDI: Chinese version of the Beck Depression Inventory.
jCES-D: Center for Epidemiological Studies Depression Scale.
kiCBT: internet-delivered cognitive behavioral therapy.
lMEiCBT: mindfulness-enhanced internet-delivered cognitive behavioral therapy.
miMT: internet-delivered mindfulness training.
nACT: acceptance and commitment therapy.
oCCAPS-34: Counseling Center Assessment of Psychological Symptoms-34.
pCDMI: complaint-directed mini-intervention.
qIDS-SR: Inventory of Depressive Symptomatology Self-Report.
rPROMIS: Patient-Reported Outcomes Measurement Information System.
The conceptualization of gamification was modeled after previous research in which gamification was defined as having three components: a design feature that uses motivational affordances to influence psychological and behavioral outcomes [23]. Another literature review that focused exclusively on the health and well-being app domain has described very similar conceptualizations of gamification elements [86]. Modeled after these gamification literature reviews, gamification for this meta-analysis was defined using the following nine motivational affordance categories: points, achievements or badges, levels, narrative stories or themes, clear goals, performance-based feedback, rewards, progress metrics (eg, progress bars), and challenges [23,86]. While gamification can also include leaderboards [19], this element was excluded from the meta-analysis, as leaderboards in the context of mental health may promote social comparison, which can be counterproductive [87,88]. First authors of the studies were contacted via email to confirm conceptualization of the number of gamification elements. The number of gamification elements included in each intervention was included as a moderator in analyses.
Raw depression scores (mean and SD) at posttreatment for each study were extracted. If a study compared more than one mental health app intervention to a control group, or if more than one independent sample was examined in an article, both were included as separate comparisons. Studies used different, but convergently valid, measures of depression. If the articles met any of the exclusion criteria, specifically missing data, they were excluded from data analysis (n=12).
Quality Assessment
The quality of each study was assessed using the Cochrane Collaboration’s risk of bias assessment tool, which provided seven basic criteria: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases [48]. Studies were scored on a scale ranging from 0 to 2, where 0 indicates “low or no bias,” 1 indicates that the “level of bias is unclear,” and 2 indicates “high bias” (Multimedia Appendix 4). In line with previous research, if a study did not address one of the categories, it was given a 1 for the lack of explanation [89]. Total scores for individual and all studies are presented in Figure 1.
Figure 1.
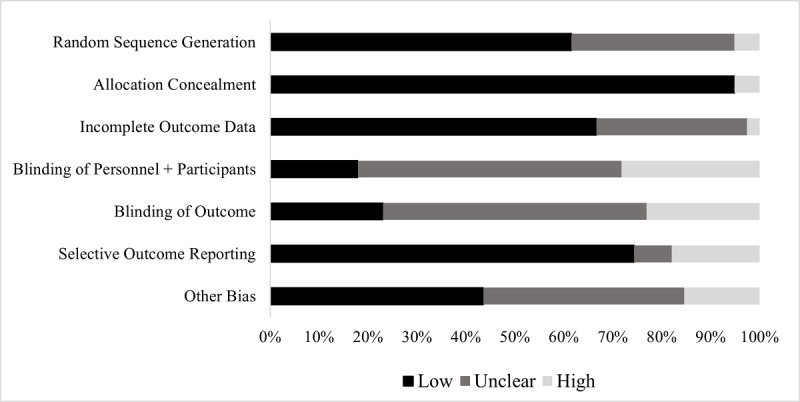
Risk of bias across all studies included in the meta-analysis based on the Cochrane Collaboration's risk of bias assessment tool.
Data Analysis
Overview
The resulting depression questionnaires included in the analyzed studies were as follows: the 9-item Patient Health Questionnaire (PHQ-9) [90]; the Beck Depression Inventory-II (BDI-II) [91]; the Center for Epidemiological Studies Depression Scale (CES-D) [92]; the depression subscale of the 21-item Depression, Anxiety, and Stress Scale (DASS-21) [93]; the Hospital Anxiety and Depression Scale (HADS) [94]; the Inventory of Depressive Symptomatology Self-Report (IDS-SR) [95]; the depression scale from the Counseling Center Assessment of Psychological Symptoms-34 (CCAPS-34) [96]; and the depression scale from the Patient-Reported Outcomes Measurement Information System (PROMIS). All questionnaires involved a 4-point scale, ranging from 0 (very low levels of depressive symptoms) to 3 (very high levels of depressive symptoms). Some studies reported sum scores, while others reported average scores. To ensure that all questionnaire data were comparable along the same scale, average depression scores were computed for analysis.
The meta-analytic data were analyzed in RStudio, primarily using the meta (version 4.18) and metafor (version 3.0) packages in R (version 3.6.3; The R Foundation) to determine effect size and between-group differences. Means and variances were aggregated for studies that included two primary measures of depression to compute a single comparison [97]. This led to a total of 50 comparisons in the meta-analysis. From this data, the pooled SD, t test value, P value, degrees of freedom, SE, and Hedges g were calculated. The Hedges g effect size provides an index of the magnitude of the difference between two means and corrects for potential biases in small samples [97,98]. The bias correction was performed using the following formula:  where n = n1 + n2 [99]. An effect size of 0.2 represents a small effect size, 0.5 reflects a moderate effect size, and ≥0.80 represents a large effect size [98,100].
where n = n1 + n2 [99]. An effect size of 0.2 represents a small effect size, 0.5 reflects a moderate effect size, and ≥0.80 represents a large effect size [98,100].
Following previous meta-analyses comparing intervention effects on depressive symptoms [26,37,41], the effectiveness of mental health apps was assessed using one outcome: difference in depressive symptoms between intervention and control groups at posttreatment. To test the hypothesis that mental health apps would be effective in reducing depressive symptoms, a random effects model was used to examine differences in the magnitude of depressive symptomology between those mental health app interventions compared to control conditions. The continuous variable of number of gamification elements was included in the random effects model as a moderator to test whether gamification elements influenced the effectiveness of mental health apps. The duration of the intervention, in months, was also included as a moderator variable. The I2 statistic was computed to determine heterogeneity across studies: an I2 value of ≤25% suggests low heterogeneity, ~50% suggests moderate heterogeneity, and ≥75% suggests high heterogeneity across studies [101]. While some articles provided follow-up time point data, only data from the postintervention period or data that were specified as the primary endpoint were analyzed in the primary meta-analysis.
Subgroup and Sensitivity Analyses
A sensitivity analysis using a random effects model with the gamification moderator was conducted to examine the effectiveness of mental health apps on depressive symptoms among the CBT-based apps that excluded ACT and mindfulness-based interventions. A secondary meta-regression analysis with the gamification moderator was performed for studies that included a measure of adherence rates (ie, percentage completion of all intervention modules or requirements) for the intervention condition. The adherence analysis included 28 studies with 37 comparisons.
Assessment of Publication Bias
A funnel plot was created to provide a visual of potential bias. The vertical line indicates the estimated effect of all studies. Pseudo-CIs were generated around this line in homogenous data sets to indicate 95% CI boundaries. Asymmetrical funnel plots suggest that the effects of an intervention in studies with small sample sizes are different—typically more impactful—than in studies with larger sample sizes and may indicate publication bias [102]. However, if model estimates suggest heterogeneity, a transformation manipulates these pseudo-CIs to take the heterogeneity into account: ±1.96 × √(SE2 + τ2) where the τ2 variable indicates the degree of heterogeneity. Its inclusion in the pseudo-CI calculation results in two curved lines asymptotic to the original estimated effect, a broader and wider funnel more inclusive of variance.
The presence of publication bias was also measured with the Egger test and the trim-and-fill approach by Duval and Tweedie. The Egger test [103] was performed to quantify whether there was significant small-study publication bias in the included studies. The trim-and-fill analysis by Duval and Tweedie was conducted to establish an unbiased estimate of the pooled effect size by correcting for funnel plot asymmetry due to publication bias [104]. Significant findings indicate whether the study sample is asymmetrical or “missing” publications that would positively or negatively bias the estimate.
Results
Results of the Review
Data collection commenced in February 2021 and ended in May 2021. As of June 2021, a total of 5597 articles were identified through the literature search. After duplicate removal, 2741 eligible articles remained for title and abstract screening. Two researchers (SGS and KAB) independently identified 101 articles as potentially eligible. Screeners had an agreement rate of 98.94% (Cohen k=0.85). Full-text screening of these 101 articles was conducted. Of the reviewed articles, 38 studies with 39 different mental health apps met the inclusion criteria and were therefore included. Figure 2 presents the study selection identification, screening, and eligibility process.
Figure 2.
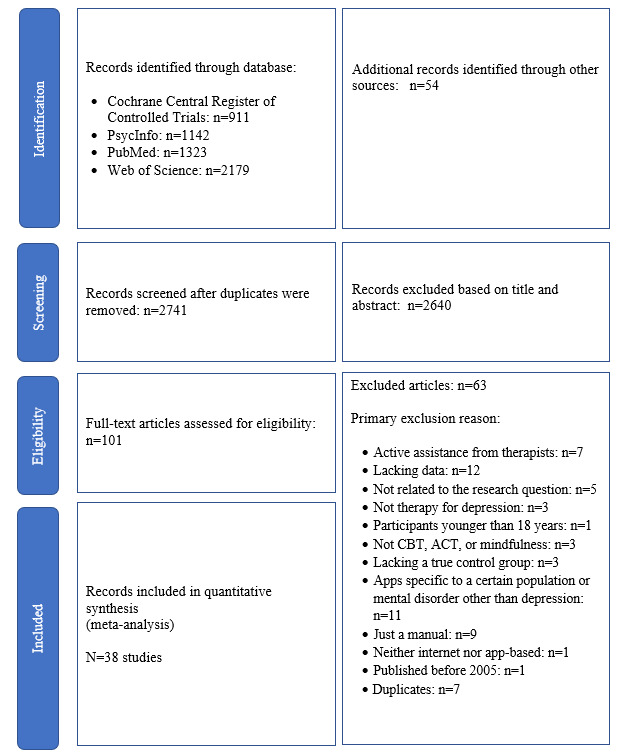
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of the studies included in the systematic review and meta-analysis. ACT: acceptance and commitment therapy; CBT: cognitive behavioral therapy.
Participant and Study Characteristics
A total of 8110 participants provided analyzable data (4362, 53.8%, in the interventions and 3748, 46.2%, in the control conditions) for this meta-analysis, with the majority of participants being female (n=4728, 58.3%; mean age 35.6, SD 7.9, years). Multimedia Appendix 3 shows descriptive information for each study. Treatment duration ranged from 10 days to 4 months. Most of the studies (26/38, 68%) used mental health apps with CBT [31,45-48,50,51,53,55-62,66-68,72-75,77-79], 32% (12/38) used mindfulness [49,52,57,63-67,69-71,74,76,82], 8% (3/38) used ACT [62,73,82], 8% (3/38) did not have a therapy associated with the app, and only 5% (2/38) used BA [54,70]. In terms of the depressive symptom outcome measures, 32% (12/38) of the studies used the PHQ-9, 26% (10/38) used the BDI-II, 16% (6/38) used the DASS-21, 11% (4/38) used the CES-D, 3% (1/38) used the HADS, 3% (1/38) used the IDS-SR, 3% (1/38) used the CCAPS-34, and 3% (1/38) used the PROMIS.
Of the 50 different comparisons used in the 38 different studies, 71% (27/38) contained gamification elements and 29% (11/38) did not. The number of gamification elements observed in each study are shown in Multimedia Appendix 5. Table 1 shows the type of intervention, app, and number of gamification elements for each article. Multimedia Appendix 6 reports supplemental meta-analytic results for long-term follow-up time points and control variables.
Primary Analysis
A forest plot for the postintervention differences between the mental health app intervention group and the control group is shown in Figure 3. The random effects model for all eligible studies (n=50 comparisons) revealed a small to medium effect of mental health apps in reducing depressive symptoms compared to controls (g=–0.27, 95% CI –0.36 to –0.17; P<.001). However, significant heterogeneity in the results were observed (I2=0.76, τ2=0.076; P<.001). The gamification moderator was not a significant predictor of depressive symptoms (β=–0.03, SE=0.04; P=.38); the intervention duration moderator was also not a significant predictor (β=–0.02, SE=0.04; P=.67).
Figure 3.
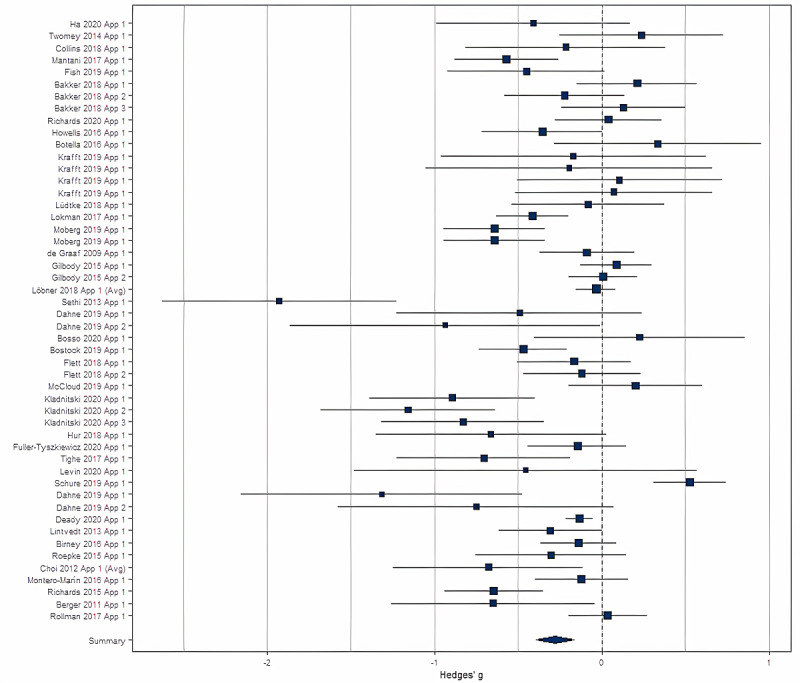
Forest plot for all studies (n=50 comparisons) showing the effect sizes for each. Author and year for each study are listed on the y-axis.
Sensitivity Analysis: CBT-Only Studies
A sensitivity analysis was performed for app comparisons that involved CBT-based therapy (37/50, 74%). The overall effect size was similar to the overall analysis (g=–0.30, 95% CI –0.42 to –0.17; P<.001), and there was no significant effect of gamification elements as a moderator (β=–0.04, SE=0.04; P=.31) or of study duration as a moderator (β=–0.02, SE=0.05; P=.69). Multimedia Appendix 7 show the funnel plot for this analysis.
Secondary Analysis: Adherence
The secondary analysis examining comparisons that included a measure of adherence (36/50, 72%) failed to show a significant effect of gamification elements (β=–1.93, SE=2.28; P=.40) on adherence rates. However, intervention duration was a significant predictor such that longer interventions were associated with higher adherence rates (β=11.33, SE=3.57; P=.003). Similarly, when examining only the CBT-based mental health apps (25/50, 50%), there was no effect of gamification elements on adherence (β=0.17, SE=2.51; P=.95), but intervention duration positively predicted adherence (β=12.23, SE=4.21; P=.008).
Funnel Plot Results
Examination of the funnel plot of the posttreatment effect SEs indicated heteroscedasticity. The Egger test of asymmetry was significant (Q50=214.46, P<.001). A trim-and-fill analysis suggested a trending finding of three missing publications to the right, though this did not reach the level of statistical significance (β=2.45, P=.13). To be conservative, the pseudo-CIs in Figure 4 were adjusted per τ2, with trim-and-fill studies as white dots. Controlling for the violations of these assumptions, the overall random effects model was significant (β=–0.26, SE=0.06; P<.001), indicating a significant improvement overall.
Figure 4.
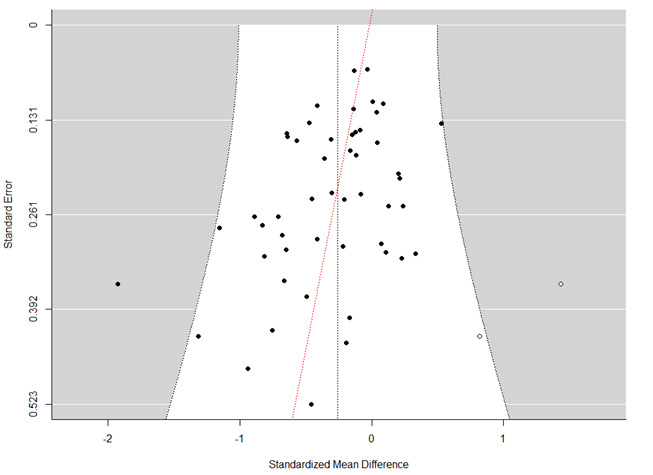
Funnel plot for all studies (n=50 comparisons) showing the heterogeneity for each.
Discussion
Principal Findings
This meta-analysis provides a comprehensive update about the effectiveness of mental health apps in reducing depressive symptoms, and it tests whether mental health apps with gamification elements are effective for reducing depressive symptoms. Results indicated that mental health apps are effective for reducing depressive symptoms, but gamification elements within mental health apps do not seem to reduce depressive symptoms or increase the adherence of using mental health apps.
Examination of mental health apps that exclusively employed computerized CBT (excluding mindfulness and ACT) similarly failed to show an effect of gamification on depressive symptom reduction. It should be noted that some of the included studies had a high risk of bias and, as such, the results should be interpreted with caution. Nevertheless, the evidence from this meta-analysis suggests that CBT effectively aids with the control, maintenance, and reduction of depressive symptoms, but gamification and reward elements embedded in mental health apps do not significantly alleviate such symptoms.
Consistent with prior systematic reviews and meta-analyses on digital interventions for depression, we found that mental health app interventions are moderately effective in reducing depressive symptoms compared to controls [26,37,38,41,89]. Effect sizes from these prior meta-analyses ranged from 0.33 to 0.58, which is slightly higher than the small to moderate effect size observed in this meta-analysis. While this research provides strong consensus of a general positive effect of mental health apps on alleviating depressive symptoms, the specific elements that contribute to this effect remain largely elusive. Previous systematic reviews have demonstrated that guidance and support from a professional can augment the effectiveness of mental health app interventions [37,105]. Other work suggests that incorporating reminders into digital mental health interventions can promote engagement and adherence with the intervention, which may, in turn, enhance the intervention’s therapeutic benefits [38]. However, the results of this meta-analysis did not show a significant relationship between gamification and adherence rates. Understanding how such features work together to mitigate depressive symptoms is critical for improving mental health app development.
One potential explanation of why gamification elements do not moderate depressive symptoms may be reward sensitivity. Depression generally has been associated with hyposensitivity to rewards, particularly among those with anhedonic symptoms [11-13,16,17]. This diminished reward-related neural activity may decrease motivation to obtain rewards or diminish the positive reward experience. While the UGM model proposes reward as a critical part of motivation to ensure engagement, it also suggests moderating effects, such as self-efficacy and locus of control. These variables have known negative relationships with depression [106,107] and may make gamification less effective. An alternative explanation for the results may be that gamification does not engender additive benefits. The included mental health apps all used strong, evidence-based therapeutic interventions, including CBT, ACT, and mindfulness. Based on the results of this meta-analysis, these interventions appear to be sufficient in mitigating depressive symptoms.
Overall, 30 studies in this meta-analysis showed a significant effect, while nine studies failed to produce significant reductions in depressive symptoms. In terms of gamification elements, four of the apps that were associated with nonsignificant findings included at least two elements of gamification: Kokoro, Headspace, MoodGYM, and Be Good to Yourself [50,52,59,67]. In contrast, two of these apps—Headspace and MoodGYM—were used in other studies, where they produced significant positive changes in depressive symptoms [31,53,64,65,68,69]. These mixed findings support the notion that while mental health apps may have a future in telemedicine and psychological settings [89,108], more research is needed to understand which mental health app features are integral to improving mental health symptoms. From there, these facets can be properly implemented as a methodologically reliable therapeutic technique.
The push for the creation of efficient and scientifically supported mental health apps grows each year as technology becomes more ubiquitous [109]. These apps could aid therapists who are unable to accept any new clients and people who may not have access to psychological centers or counselors due to financial strains, location, or disabilities. This meta-analysis adds to the current literature by suggesting against overreliance on reward and gamification elements as major reducers of depressive symptoms. These elements may be beneficial in mental health apps, but no more so than other evidence-based therapeutic features. Many of the mental health apps currently available to the general public lack valid testing of their efficacy; thus, there is a strong need for rigorous evaluation of such apps on psychological outcomes. Indeed, in this meta-analysis, nearly half of the included studies incorporated gamification elements, yet the results suggest that such elements exert minimal therapeutic benefits. Significantly more research is needed to identify which specific mental health app features maximize therapeutic effects.
Limitations
This systematic review and meta-analysis had some limitations, which were largely related to inadequacies in the studies available for analyses. Results were calculated based on aggregated samples, which may have caused a certain level of ecological bias. Due to the disparate sample of apps, heterogeneity was detected in all primary analyses. However, heterogeneity was nearly identical to past research on this topic, and we took statistical efforts to minimize this impact [38]. In addition, the meta-analysis was not exclusive to individuals with clinical levels of depression, but all experiencing depressive symptoms. No data sets were consistently available across all studies to assess clinical depression diagnoses or psychiatric comorbidities. Consequently, the findings may not generalize to individuals with severe depression or individuals with other mental health conditions.
Future Research Using Gamification Elements
The main findings of this study were that mental health apps are effective for reducing depressive symptoms, but gamification elements within these mental health apps do not seem to affect depressive symptoms. It is possible that mental health apps with gamification elements may influence patients managing anxiety, stress, or other conditions where anhedonia is not present. Thus, gamification may not be a promising app feature for depressive symptoms but may hold promise for other mental health conditions. Future research should consider examining the effectiveness of mental health apps with gamification on other mental health conditions. While previous research has investigated the effectiveness of mental health apps on anxiety and life satisfaction [50,56], the effect of gamification elements on these psychological factors remains underexplored. Moreover, there is a need for additional research to better characterize the usability benefits and user preferences of mental health apps. If gamification within mental health apps is not effective for individuals experiencing depressive symptoms, then it is important to identify other potential features. Designing specific features that may motivate users with depression toward continued mental health app adherence could lead to beneficial outcomes.
Conclusions
Mental health apps have proven to be a useful tool in reducing depressive symptoms with or without the inclusion of gamification elements. These results demonstrate that although there is a significant improvement in using mental health apps overall, there is no evidence to suggest that gamification makes outcomes significantly better or worse. Additional elements, such as personalization, motivational reminders, social support, and usability, need to be investigated. Mental health apps may provide a readily available option for global psychological care; however, supplementary research is needed on their effectiveness before reliable implementation into the health care system can occur.
Abbreviations
- ACT
acceptance and commitment therapy
- BA
behavioral activation
- BDI-II
Beck Depression Inventory-II
- CBT
cognitive behavioral therapy
- CCAPS-34
Counseling Center Assessment of Psychological Symptoms-34
- CES-D
Center for Epidemiological Studies Depression Scale
- DASS-21
21-item Depression, Anxiety, and Stress Scale
- HADS
Hospital Anxiety and Depression Scale
- IDS-SR
Inventory of Depressive Symptomatology Self-Report
- PHQ-9
9-item Patient Health Questionnaire
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PROMIS
Patient-Reported Outcomes Measurement Information System
- RCT
randomized controlled trial
- UGM
Unified Gamification and Motivation
Search terms for the meta-analysis.
Database screening tool.
Study demographics extracted from articles: sample, length, population, age, and gender.
Quality assessment screening.
Gamification screening for publications.
Sensitivity and supplemental analyses.
Sensitivity analysis for cognitive behavioral therapy (CBT)–only studies.
Footnotes
Conflicts of Interest: None declared.
References
- 1.Major depression. National Institute of Mental Health. 2019. [2021-07-12]. https://www.nimh.nih.gov/health/statistics/major-depression.html .
- 2.National Collaborating Centre for Mental Health (UK) Depression: The Treatment and Management of Depression in Adults (Updated Edition) Leicester, UK: British Psychological Society; 2010. [PubMed] [Google Scholar]
- 3.Weir K. APA offers new guidance for treating depression. Monitor on Psychology, American Psychological Association. 2019. Sep 01, [2021-07-15]. https://www.apa.org/monitor/2019/09/ce-corner-depression .
- 4.Cartwright C, Gibson K, Read J, Cowan O, Dehar T. Long-term antidepressant use: Patient perspectives of benefits and adverse effects. Patient Prefer Adherence. 2016;10:1401–1407. doi: 10.2147/PPA.S110632. doi: 10.2147/PPA.S110632.ppa-10-1401 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Stein-Shvachman I, Karpas DS, Werner P. Depression treatment non-adherence and its psychosocial predictors: Differences between young and older adults? Aging Dis. 2013 Sep 20;4(6):329–336. doi: 10.14336/AD.2013.0400329. http://europepmc.org/abstract/MED/24307966 .ad-2013-04-06-329 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wood P, Burwell J, Rawlett K. New study reveals lack of access as root cause for mental health crisis in America. National Council for Mental Wellbeing. 2018. Oct 10, [2021-07-15]. https://www.thenationalcouncil.org/press-releases/new-study-reveals-lack-of-access-as-
- 7.Van Hees S, Siewe Fodjo JN, Wijtvliet V, Van den Bergh R, Faria de Moura Villela E, da Silva CF, Weckhuysen S, Colebunders R. Access to healthcare and prevalence of anxiety and depression in persons with epilepsy during the COVID-19 pandemic: A multicountry online survey. Epilepsy Behav. 2020 Nov;112:107350. doi: 10.1016/j.yebeh.2020.107350. https://linkinghub.elsevier.com/retrieve/pii/S1525-5050(20)30529-1 .S1525-5050(20)30529-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Winerman L. By the numbers: The cost of treatment. Monitor on Psychology, American Psychological Association. 2017. Mar, [2021-07-15]. https://www.apa.org/monitor/2017/03/numbers .
- 9.Neary M, Schueller SM. State of the field of mental health apps. Cogn Behav Pract. 2018 Nov;25(4):531–537. doi: 10.1016/j.cbpra.2018.01.002. http://europepmc.org/abstract/MED/33100810 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Pew Research Center. Washington, DC: Pew Research Center; 2021. Apr 07, [2021-07-15]. Mobile fact sheet. https://www.pewresearch.org/internet/factsheet/mobile/ [Google Scholar]
- 11.Admon R, Pizzagalli DA. Dysfunctional reward processing in depression. Curr Opin Psychol. 2015 Aug 01;4:114–118. doi: 10.1016/j.copsyc.2014.12.011. http://europepmc.org/abstract/MED/26258159 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chen C, Takahashi T, Nakagawa S, Inoue T, Kusumi I. Reinforcement learning in depression: A review of computational research. Neurosci Biobehav Rev. 2015 Aug;55:247–267. doi: 10.1016/j.neubiorev.2015.05.005.S0149-7634(15)00131-1 [DOI] [PubMed] [Google Scholar]
- 13.Eshel N, Roiser JP. Reward and punishment processing in depression. Biol Psychiatry. 2010 Jul 15;68(2):118–124. doi: 10.1016/j.biopsych.2010.01.027.S0006-3223(10)00069-7 [DOI] [PubMed] [Google Scholar]
- 14.Safra L, Chevallier C, Palminteri S. Depressive symptoms are associated with blunted reward learning in social contexts. PLoS Comput Biol. 2019 Jul;15(7):e1007224. doi: 10.1371/journal.pcbi.1007224. https://dx.plos.org/10.1371/journal.pcbi.1007224 .PCOMPBIOL-D-18-01310 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Vrijen C, Ackermans MA, Bosma A, Kretschmer T. Reward responsiveness, optimism, and social and mental functioning in children aged 6-7: Protocol of a cross-sectional pilot study. JMIR Res Protoc. 2020 Sep 24;9(9):e18902. doi: 10.2196/18902. https://www.researchprotocols.org/2020/9/e18902/ v9i9e18902 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Foti D, Hajcak G. Depression and reduced sensitivity to non-rewards versus rewards: Evidence from event-related potentials. Biol Psychol. 2009 Apr;81(1):1–8. doi: 10.1016/j.biopsycho.2008.12.004.S0301-0511(08)00255-X [DOI] [PubMed] [Google Scholar]
- 17.Yang X, Huang J, Zhu C, Wang Y, Cheung EFC, Chan RCK, Xie G. Motivational deficits in effort-based decision making in individuals with subsyndromal depression, first-episode and remitted depression patients. Psychiatry Res. 2014 Dec 30;220(3):874–882. doi: 10.1016/j.psychres.2014.08.056.S0165-1781(14)00753-7 [DOI] [PubMed] [Google Scholar]
- 18.Liu W, Chan RCK, Wang L, Huang J, Cheung EFC, Gong Q, Gollan JK. Deficits in sustaining reward responses in subsyndromal and syndromal major depression. Prog Neuropsychopharmacol Biol Psychiatry. 2011 Jun 01;35(4):1045–1052. doi: 10.1016/j.pnpbp.2011.02.018.S0278-5846(11)00074-1 [DOI] [PubMed] [Google Scholar]
- 19.Blohm I, Leimeister JM. Gamification. Bus Inf Syst Eng. 2013 Jun 14;5(4):275–278. doi: 10.1007/s12599-013-0273-5. [DOI] [Google Scholar]
- 20.King D, Greaves F, Exeter C, Darzi A. 'Gamification': Influencing health behaviours with games. J R Soc Med. 2013 Mar;106(3):76–78. doi: 10.1177/0141076813480996. http://europepmc.org/abstract/MED/23481424 .106/3/76 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lister C, West JH, Cannon B, Sax T, Brodegard D. Just a fad? Gamification in health and fitness apps. JMIR Serious Games. 2014 Aug 04;2(2):e9. doi: 10.2196/games.3413. https://games.jmir.org/2014/2/e9/ v2i2e9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Schmidt-Kraepelin M, Toussaint PA, Thiebes S, Hamari J, Sunyaev A. Archetypes of gamification: Analysis of mHealth apps. JMIR Mhealth Uhealth. 2020 Oct 19;8(10):e19280. doi: 10.2196/19280. https://mhealth.jmir.org/2020/10/e19280/ v8i10e19280 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hamari J, Koivisto J, Sarsa H. Does gamification work? -- A literature review of empirical studies on gamification. Proceedings of the Annual Hawaii International Conference on System Sciences; Annual Hawaii International Conference on System Sciences; January 6-9, 2014; Waikoloa, HI. 2014. pp. 3025–3034. [DOI] [Google Scholar]
- 24.Dykens I, Wetzel A, Dorton S, Batchelor E. Towards a unified model of gamification and motivation. Proceedings of the International Conference on Human-Computer Interaction; International Conference on Human-Computer Interaction; July 24-29, 2021; Virtual. Cham, Switzerland: Springer International Publishing; 2021. pp. 53–70. [DOI] [Google Scholar]
- 25.Cole SW, Yoo DJ, Knutson B. Interactivity and reward-related neural activation during a serious videogame. PLoS One. 2012;7(3):e33909. doi: 10.1371/journal.pone.0033909. https://dx.plos.org/10.1371/journal.pone.0033909 .PONE-D-11-15712 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Li J, Theng Y, Foo S. Game-based digital interventions for depression therapy: A systematic review and meta-analysis. Cyberpsychol Behav Soc Netw. 2014 Aug;17(8):519–527. doi: 10.1089/cyber.2013.0481. http://europepmc.org/abstract/MED/24810933 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Brandt LR, Hidalgo L, Diez-Canseco F, Araya R, Mohr DC, Menezes PR, Miranda JJ. Addressing depression comorbid with diabetes or hypertension in resource-poor settings: A qualitative study about user perception of a nurse-supported smartphone app in Peru. JMIR Ment Health. 2019 Jun 18;6(6):e11701. doi: 10.2196/11701. https://mental.jmir.org/2019/6/e11701/ v6i6e11701 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Menezes P, Quayle J, Garcia Claro H, da Silva S, Brandt LR, Diez-Canseco F, Miranda JJ, Price LN, Mohr DC, Araya R. Use of a mobile phone app to treat depression comorbid with hypertension or diabetes: A pilot study in Brazil and Peru. JMIR Ment Health. 2019 Apr 26;6(4):e11698. doi: 10.2196/11698. https://mental.jmir.org/2019/4/e11698/ v6i4e11698 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Avalos LA, Aghaee S, Kurtovich E, Quesenberry C, Nkemere L, McGinnis MK, Kubo A. A mobile health mindfulness intervention for women with moderate to moderately severe postpartum depressive symptoms: Feasibility study. JMIR Ment Health. 2020 Nov 12;7(11):e17405. doi: 10.2196/17405. https://mental.jmir.org/2020/11/e17405/ v7i11e17405 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Firth J, Torous J, Nicholas J, Carney R, Rosenbaum S, Sarris J. Can smartphone mental health interventions reduce symptoms of anxiety? A meta-analysis of randomized controlled trials. J Affect Disord. 2017 Aug 15;218:15–22. doi: 10.1016/j.jad.2017.04.046. https://linkinghub.elsevier.com/retrieve/pii/S0165-0327(17)30015-0 .S0165-0327(17)30015-0 [DOI] [PubMed] [Google Scholar]
- 31.Roepke AM, Jaffee SR, Riffle OM, McGonigal J, Broome R, Maxwell B. Randomized controlled trial of SuperBetter, a smartphone-based/internet-based self-help tool to reduce depressive symptoms. Games Health J. 2015 Jun;4(3):235–246. doi: 10.1089/g4h.2014.0046. [DOI] [PubMed] [Google Scholar]
- 32.Griffiths MD, Kuss DJ, Ortiz de Gortari AB. Alternative Pain Management: Solutions for Avoiding Prescription Drug Overuse. Hershey, PA: IGI Global; 2020. Videogames as therapy: An updated selective review of the medical and psychological literature; pp. 324–363. [Google Scholar]
- 33.Lau HM, Smit JH, Fleming TM, Riper H. Serious games for mental health: Are they accessible, feasible, and effective? A systematic review and meta-analysis. Front Psychiatry. 2016;7:209. doi: 10.3389/fpsyt.2016.00209. doi: 10.3389/fpsyt.2016.00209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Wang K, Varma DS, Prosperi M. A systematic review of the effectiveness of mobile apps for monitoring and management of mental health symptoms or disorders. J Psychiatr Res. 2018 Dec;107:73–78. doi: 10.1016/j.jpsychires.2018.10.006.S0022-3956(18)30828-8 [DOI] [PubMed] [Google Scholar]
- 35.Fleming T, Dixon R, Frampton C, Merry S. A pragmatic randomized controlled trial of computerized CBT (SPARX) for symptoms of depression among adolescents excluded from mainstream education. Behav Cogn Psychother. 2012 Oct;40(5):529–541. doi: 10.1017/S1352465811000695.S1352465811000695 [DOI] [PubMed] [Google Scholar]
- 36.Fulmer R, Joerin A, Gentile B, Lakerink L, Rauws M. Using psychological artificial intelligence (Tess) to relieve symptoms of depression and anxiety: Randomized controlled trial. JMIR Ment Health. 2018 Dec 13;5(4):e64. doi: 10.2196/mental.9782. https://mental.jmir.org/2018/4/e64/ v5i4e64 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Weisel KK, Fuhrmann LM, Berking M, Baumeister H, Cuijpers P, Ebert DD. Standalone smartphone apps for mental health-a systematic review and meta-analysis. NPJ Digit Med. 2019;2:118. doi: 10.1038/s41746-019-0188-8. doi: 10.1038/s41746-019-0188-8.188 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Wahle F, Bollhalder L, Kowatsch T, Fleisch E. Toward the design of evidence-based mental health information systems for people with depression: A systematic literature review and meta-analysis. J Med Internet Res. 2017 May 31;19(5):e191. doi: 10.2196/jmir.7381. https://www.jmir.org/2017/5/e191/ v19i5e191 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Lorenz RC, Gleich T, Gallinat J, Kühn S. Video game training and the reward system. Front Hum Neurosci. 2015;9:40. doi: 10.3389/fnhum.2015.00040. doi: 10.3389/fnhum.2015.00040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Vallury KD, Jones M, Oosterbroek C. Computerized cognitive behavior therapy for anxiety and depression in rural areas: A systematic review. J Med Internet Res. 2015 Jun 05;17(6):e139. doi: 10.2196/jmir.4145. https://www.jmir.org/2015/6/e139/ v17i6e139 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Wright JH, Owen JJ, Richards D, Eells TD, Richardson T, Brown GK, Barrett M, Rasku MA, Polser G, Thase ME. Computer-assisted cognitive-behavior therapy for depression: A systematic review and meta-analysis. J Clin Psychiatry. 2019 Mar 19;80(2):e1–e14. doi: 10.4088/JCP.18r12188. http://www.psychiatrist.com/JCP/article/Pages/2019/v80/18r12188.aspx . [DOI] [PubMed] [Google Scholar]
- 42.Lukas CA, Eskofier B, Berking M. A gamified smartphone-based intervention for depression: Randomized controlled pilot trial. JMIR Ment Health. 2021 Jul 20;8(7):e16643. doi: 10.2196/16643. https://mental.jmir.org/2021/7/e16643/ v8i7e16643 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Dias LPS, Barbosa JLV, Vianna HD. Gamification and serious games in depression care: A systematic mapping study. Telematics Inform. 2018 Apr;35(1):213–224. doi: 10.1016/j.tele.2017.11.002. [DOI] [Google Scholar]
- 44.Christie GI, Shepherd M, Merry SN, Hopkins S, Knightly S, Stasiak K. Gamifying CBT to deliver emotional health treatment to young people on smartphones. Internet Interv. 2019 Dec;18:100286. doi: 10.1016/j.invent.2019.100286. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(19)30030-2 .S2214-7829(19)30030-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Russoniello C, O'Brien K, Parks J. The effectiveness of casual video games in improving mood and decreasing stress. J CyberTherapy Rehabil. 2009;2(1):53–66. https://www.researchgate.net/profile/Carmen-Russoniello-2/publication/289131468_The_effectiveness_of_casual_video_games_in_improving_mood_and_decreasing_stress/links/589b371492851c942ddac68d/The-effectiveness-of-casual-video-games-in-improving-mood-and-decreasing-stress.pdf . [Google Scholar]
- 46.Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J Clin Epidemiol. 2009 Oct;62(10):e1–e34. doi: 10.1016/j.jclinepi.2009.06.006. https://linkinghub.elsevier.com/retrieve/pii/S0895-4356(09)00180-2 .S0895-4356(09)00180-2 [DOI] [PubMed] [Google Scholar]
- 47.Six S, Byrne KA. Open Science Framework. Charlottesville, VA: Center for Open Science; 2021. May 27, [2021-11-22]. Rewards in mental health applications for aiding depression: A meta-analysis. https://osf.io/ypm4x/ [Google Scholar]
- 48.Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JAC, Cochrane Bias Methods Group. Cochrane Statistical Methods Group The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011 Oct 18;343:d5928. doi: 10.1136/bmj.d5928. http://europepmc.org/abstract/MED/22008217 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Ha SW, Kim J. Designing a scalable, accessible, and effective mobile app based solution for common mental health problems. Int J Hum Comput Interact. 2020 Apr 26;36(14):1354–1367. doi: 10.1080/10447318.2020.1750792. [DOI] [Google Scholar]
- 50.Twomey C, O'Reilly G, Byrne M, Bury M, White A, Kissane S, McMahon A, Clancy N. A randomized controlled trial of the computerized CBT programme, MoodGYM, for public mental health service users waiting for interventions. Br J Clin Psychol. 2014 Nov;53(4):433–450. doi: 10.1111/bjc.12055. [DOI] [PubMed] [Google Scholar]
- 51.Collins S, Byrne M, Hawe J, O'Reilly G. Evaluation of a computerized cognitive behavioural therapy programme, MindWise (2.0), for adults with mild-to-moderate depression and anxiety. Br J Clin Psychol. 2018 Jun;57(2):255–269. doi: 10.1111/bjc.12165. [DOI] [PubMed] [Google Scholar]
- 52.Mantani A, Kato T, Furukawa TA, Horikoshi M, Imai H, Hiroe T, Chino B, Funayama T, Yonemoto N, Zhou Q, Kawanishi N. Smartphone cognitive behavioral therapy as an adjunct to pharmacotherapy for refractory depression: Randomized controlled trial. J Med Internet Res. 2017 Nov 03;19(11):e373. doi: 10.2196/jmir.8602. https://www.jmir.org/2017/11/e373/ v19i11e373 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Fish MT, Saul AD. The gamification of meditation: A randomized-controlled study of a prescribed mobile mindfulness meditation application in reducing college students’ depression. Simul Gaming. 2019 Jun 04;50(4):419–435. doi: 10.1177/1046878119851821. [DOI] [Google Scholar]
- 54.Bakker D, Kazantzis N, Rickwood D, Rickard N. A randomized controlled trial of three smartphone apps for enhancing public mental health. Behav Res Ther. 2018 Oct;109:75–83. doi: 10.1016/j.brat.2018.08.003.S0005-7967(18)30124-4 [DOI] [PubMed] [Google Scholar]
- 55.Richards D, Enrique A, Eilert N, Franklin M, Palacios J, Duffy D, Earley C, Chapman J, Jell G, Sollesse S, Timulak L. A pragmatic randomized waitlist-controlled effectiveness and cost-effectiveness trial of digital interventions for depression and anxiety. NPJ Digit Med. 2020;3:85. doi: 10.1038/s41746-020-0293-8. doi: 10.1038/s41746-020-0293-8.293 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Howells A, Ivtzan I, Eiroa-Orosa FJ. Putting the ‘app’ in happiness: A randomised controlled trial of a smartphone-based mindfulness intervention to enhance wellbeing. J Happiness Stud. 2014 Oct 29;17(1):163–185. doi: 10.1007/s10902-014-9589-1. [DOI] [Google Scholar]
- 57.Botella C, Mira A, Moragrega I, García-Palacios A, Bretón-López J, Castilla D, Riera López Del Amo A, Soler C, Molinari G, Quero S, Guillén-Botella V, Miralles I, Nebot S, Serrano B, Majoe D, Alcañiz M, Baños RM. An internet-based program for depression using activity and physiological sensors: Efficacy, expectations, satisfaction, and ease of use. Neuropsychiatr Dis Treat. 2016;12:393–406. doi: 10.2147/NDT.S93315. doi: 10.2147/NDT.S93315.ndt-12-393 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Krafft J, Potts S, Schoendorff B, Levin ME. Arandomized controlled trial of multiple versions of an acceptance and commitment therapy matrix app for well-being. Behav Modif. 2019 Mar;43(2):246–272. doi: 10.1177/0145445517748561. [DOI] [PubMed] [Google Scholar]
- 59.Lüdtke T, Pult LK, Schröder J, Moritz S, Bücker L. A randomized controlled trial on a smartphone self-help application (Be Good to Yourself) to reduce depressive symptoms. Psychiatry Res. 2018 Nov;269:753–762. doi: 10.1016/j.psychres.2018.08.113.S0165-1781(17)32280-1 [DOI] [PubMed] [Google Scholar]
- 60.Lokman S, Leone SS, Sommers-Spijkerman M, van der Poel A, Smit F, Boon B. Complaint-directed mini-interventions for depressive complaints: A randomized controlled trial of unguided web-based self-help interventions. J Med Internet Res. 2017 Jan 04;19(1):e4. doi: 10.2196/jmir.6581. https://www.jmir.org/2017/1/e4/ v19i1e4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Moberg C, Niles A, Beermann D. Guided self-help works: Randomized waitlist controlled trial of Pacifica, a mobile app integrating cognitive behavioral therapy and mindfulness for stress, anxiety, and depression. J Med Internet Res. 2019 Jun 08;21(6):e12556. doi: 10.2196/12556. https://www.jmir.org/2019/6/e12556/ v21i6e12556 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.de Graaf LE, Gerhards SAH, Arntz A, Riper H, Metsemakers JFM, Evers SMAA, Severens JL, Widdershoven G, Huibers MJH. Clinical effectiveness of online computerised cognitive-behavioural therapy without support for depression in primary care: Randomised trial. Br J Psychiatry. 2009 Jul;195(1):73–80. doi: 10.1192/bjp.bp.108.054429.S0007125000007406 [DOI] [PubMed] [Google Scholar]
- 63.Gilbody S, Littlewood E, Hewitt C, Brierley G, Tharmanathan P, Araya R, Barkham M, Bower P, Cooper C, Gask L, Kessler D, Lester H, Lovell K, Parry G, Richards DA, Andersen P, Brabyn S, Knowles S, Shepherd C, Tallon D, White D, REEACT Team Computerised cognitive behaviour therapy (cCBT) as treatment for depression in primary care (REEACT trial): Large scale pragmatic randomised controlled trial. BMJ. 2015 Nov 11;351:h5627. doi: 10.1136/bmj.h5627. http://www.bmj.com/lookup/pmidlookup?view=long&pmid=26559241 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Löbner M, Pabst A, Stein J, Dorow M, Matschinger H, Luppa M, Maroß A, Kersting A, König HH, Riedel-Heller SG. Computerized cognitive behavior therapy for patients with mild to moderately severe depression in primary care: A pragmatic cluster randomized controlled trial (@ktiv) J Affect Disord. 2018 Oct 01;238:317–326. doi: 10.1016/j.jad.2018.06.008.S0165-0327(18)30515-9 [DOI] [PubMed] [Google Scholar]
- 65.Sethi S. Treating youth depression and anxiety: A randomised controlled trial examining the efficacy of computerised versus face‐to‐face cognitive behaviour therapy. Aust Psychol. 2020 Nov 12;48(4):249–257. doi: 10.1111/ap.12006. [DOI] [Google Scholar]
- 66.Dahne J, Collado A, Lejuez CW, Risco CM, Diaz VA, Coles L, Kustanowitz J, Zvolensky MJ, Carpenter MJ. Pilot randomized controlled trial of a Spanish-language behavioral activation mobile app (¡Aptívate!) for the treatment of depressive symptoms among United States Latinx adults with limited English proficiency. J Affect Disord. 2019 May 01;250:210–217. doi: 10.1016/j.jad.2019.03.009. http://europepmc.org/abstract/MED/30870770 .S0165-0327(18)33073-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Bosso KB. The Effects of Mindfulness Training on BDNF Levels, Depression, Anxiety, and Stress Levels of College Students [undergraduate thesis] Boca Raton, FL: Florida Atlantic University; 2020. May, [2021-11-22]. http://fau.digital.flvc.org/islandora/object/fau%3A42592 . [Google Scholar]
- 68.Bostock S, Crosswell AD, Prather AA, Steptoe A. Mindfulness on-the-go: Effects of a mindfulness meditation app on work stress and well-being. J Occup Health Psychol. 2019 Feb;24(1):127–138. doi: 10.1037/ocp0000118. http://europepmc.org/abstract/MED/29723001 .2018-19565-001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Flett JAM, Hayne H, Riordan BC, Thompson LM, Conner TS. Mobile mindfulness meditation: A randomised controlled trial of the effect of two popular apps on mental health. Mindfulness. 2018 Oct 31;10(5):863–876. doi: 10.1007/s12671-018-1050-9. [DOI] [Google Scholar]
- 70.McCloud T, Jones R, Lewis G, Bell V, Tsakanikos E. Effectiveness of a mobile app intervention for anxiety and depression symptoms in university students: Randomized controlled trial. JMIR Mhealth Uhealth. 2020 Jul 31;8(7):e15418. doi: 10.2196/15418. https://mhealth.jmir.org/2020/7/e15418/ v8i7e15418 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Kladnitski N, Smith J, Uppal S, James MA, Allen AR, Andrews G, Newby JM. Transdiagnostic internet-delivered CBT and mindfulness-based treatment for depression and anxiety: A randomised controlled trial. Internet Interv. 2020 Apr;20:100310. doi: 10.1016/j.invent.2020.100310. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(19)30128-9 .S2214-7829(19)30128-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Hur J, Kim B, Park D, Choi S. A scenario-based cognitive behavioral therapy mobile app to reduce dysfunctional beliefs in individuals with depression: A randomized controlled trial. Telemed J E Health. 2018 Sep;24(9):710–716. doi: 10.1089/tmj.2017.0214. [DOI] [PubMed] [Google Scholar]
- 73.Fuller-Tyszkiewicz M, Richardson B, Little K, Teague S, Hartley-Clark L, Capic T, Khor S, Cummins RA, Olsson CA, Hutchinson D. Efficacy of a smartphone app intervention for reducing caregiver stress: Randomized controlled trial. JMIR Ment Health. 2020 Jul 24;7(7):e17541. doi: 10.2196/17541. https://mental.jmir.org/2020/7/e17541/ v7i7e17541 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Tighe J, Shand F, Ridani R, Mackinnon A, De La Mata N, Christensen H. Ibobbly mobile health intervention for suicide prevention in Australian Indigenous youth: A pilot randomised controlled trial. BMJ Open. 2017 Jan 27;7(1):e013518. doi: 10.1136/bmjopen-2016-013518. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=28132007 .bmjopen-2016-013518 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Levin ME, Hicks ET, Krafft J. J Am Coll Health. 2020 Mar 09;:1–9. doi: 10.1080/07448481.2020.1728281. [DOI] [Google Scholar]
- 76.Schure MB, Lindow JC, Greist JH, Nakonezny PA, Bailey SJ, Bryan WL, Byerly MJ. Use of a fully automated internet-based cognitive behavior therapy intervention in a community population of adults with depression symptoms: Randomized controlled trial. J Med Internet Res. 2019 Nov 18;21(11):e14754. doi: 10.2196/14754. https://www.jmir.org/2019/11/e14754/ v21i11e14754 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Dahne J, Lejuez CW, Diaz VA, Player MS, Kustanowitz J, Felton JW, Carpenter MJ. Pilot randomized trial of a self-help behavioral activation mobile app for utilization in primary care. Behav Ther. 2019 Jul;50(4):817–827. doi: 10.1016/j.beth.2018.12.003. http://europepmc.org/abstract/MED/31208690 .S0005-7894(18)30157-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Deady M, Glozier N, Calvo R, Johnston D, Mackinnon A, Milne D, Choi I, Gayed A, Peters D, Bryant R, Christensen H, Harvey SB. Preventing depression using a smartphone app: A randomized controlled trial. Psychol Med. 2020 Jul 06;:1–10. doi: 10.1017/S0033291720002081.S0033291720002081 [DOI] [PubMed] [Google Scholar]
- 79.Lintvedt OK, Griffiths KM, Sørensen K, Østvik AR, Wang CEA, Eisemann M, Waterloo K. Evaluating the effectiveness and efficacy of unguided internet-based self-help intervention for the prevention of depression: A randomized controlled trial. Clin Psychol Psychother. 2013;20(1):10–27. doi: 10.1002/cpp.770. [DOI] [PubMed] [Google Scholar]
- 80.Birney AJ, Gunn R, Russell JK, Ary DV. MoodHacker mobile web app with email for adults to self-manage mild-to-moderate depression: Randomized controlled trial. JMIR Mhealth Uhealth. 2016 Jan 26;4(1):e8. doi: 10.2196/mhealth.4231. https://mhealth.jmir.org/2016/1/e8/ v4i1e8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Choi I, Zou J, Titov N, Dear BF, Li S, Johnston L, Andrews G, Hunt C. Culturally attuned internet treatment for depression amongst Chinese Australians: A randomised controlled trial. J Affect Disord. 2012 Feb;136(3):459–468. doi: 10.1016/j.jad.2011.11.003.S0165-0327(11)00716-6 [DOI] [PubMed] [Google Scholar]
- 82.Montero-Marín J, Araya R, Pérez-Yus MC, Mayoral F, Gili M, Botella C, Baños R, Castro A, Romero-Sanchiz P, López-Del-Hoyo Y, Nogueira-Arjona R, Vives M, Riera A, García-Campayo J. An internet-based intervention for depression in primary care in Spain: A randomized controlled trial. J Med Internet Res. 2016 Aug 26;18(8):e231. doi: 10.2196/jmir.5695. https://www.jmir.org/2016/8/e231/ v18i8e231 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Richards D, Timulak L, O'Brien E, Hayes C, Vigano N, Sharry J, Doherty G. A randomized controlled trial of an internet-delivered treatment: Its potential as a low-intensity community intervention for adults with symptoms of depression. Behav Res Ther. 2015 Dec;75:20–31. doi: 10.1016/j.brat.2015.10.005.S0005-7967(15)30045-0 [DOI] [PubMed] [Google Scholar]
- 84.Rollman BL, Herbeck Belnap B, Abebe KZ, Spring MB, Rotondi AJ, Rothenberger SD, Karp JF. Effectiveness of online collaborative care for treating mood and anxiety disorders in primary care: A randomized clinical trial. JAMA Psychiatry. 2018 Jan 01;75(1):56–64. doi: 10.1001/jamapsychiatry.2017.3379. http://europepmc.org/abstract/MED/29117275 .2661143 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Berger T, Hämmerli K, Gubser N, Andersson G, Caspar F. Internet-based treatment of depression: A randomized controlled trial comparing guided with unguided self-help. Cogn Behav Ther. 2011;40(4):251–266. doi: 10.1080/16506073.2011.616531. [DOI] [PubMed] [Google Scholar]
- 86.Johnson D, Deterding S, Kuhn K, Staneva A, Stoyanov S, Hides L. Gamification for health and wellbeing: A systematic review of the literature. Internet Interv. 2016 Nov;6:89–106. doi: 10.1016/j.invent.2016.10.002. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(16)30038-0 .S2214-7829(16)30038-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Esteves J, Valogianni K, Greenhill A. Online social games: The effect of social comparison elements on continuance behaviour. Inf Manag. 2021 Jun;58(4):103452. doi: 10.1016/j.im.2021.103452. [DOI] [Google Scholar]
- 88.Lian S, Sun X, Niu G, Zhou Z. Upward social comparison on SNS and depression: A moderated mediation model and gender difference. Acta Psychol Sinica. 2017;49(7):941–952. doi: 10.3724/sp.j.1041.2017.00941. [DOI] [Google Scholar]
- 89.Donker T, Petrie K, Proudfoot J, Clarke J, Birch M, Christensen H. Smartphones for smarter delivery of mental health programs: A systematic review. J Med Internet Res. 2013 Nov 15;15(11):e247. doi: 10.2196/jmir.2791. https://www.jmir.org/2013/11/e247/ v15i11e247 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Kroenke K, Spitzer RL, Williams JB. The PHQ-9: Validity of a brief depression severity measure. J Gen Intern Med. 2001 Sep;16(9):606–613. doi: 10.1046/j.1525-1497.2001.016009606.x. https://onlinelibrary.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=0884-8734&date=2001&volume=16&issue=9&spage=606 .jgi01114 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Beck AT, Brown GK, Steer RA. Beck Depression Inventory-II (BDI-II) Pearson. 1996. [2021-11-22]. https://www.pearsonclinical.ca/store/caassessments/en/Store/Professional-Assessments/Personality-%26-Biopsychosocial/Brief/Beck-Depression-Inventory-II/p/P100008037.html .
- 92.Eaton W, Smith C, Ybarra M, Muntaner C, Tien A. Center for Epidemiologic Studies Depression Scale: Review and revision (CESD and CESD-R) In: Maruish ME, editor. The Use of Psychological Testing for Treatment Planning and Outcomes Assessment. 3rd edition. Volume 3: Instruments for Adults. Mahwah, NJ: Lawrence Erlbaum Associates; 2004. pp. 363–377. [Google Scholar]
- 93.Lovibond PF, Lovibond SH. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995 Mar;33(3):335–343. doi: 10.1016/0005-7967(94)00075-u.0005-7967(94)00075-U [DOI] [PubMed] [Google Scholar]
- 94.Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983 Jun;67(6):361–370. doi: 10.1111/j.1600-0447.1983.tb09716.x. [DOI] [PubMed] [Google Scholar]
- 95.Rush AJ, Gullion CM, Basco MR, Jarrett RB, Trivedi MH. The Inventory of Depressive Symptomatology (IDS): Psychometric properties. Psychol Med. 1996 May;26(3):477–486. doi: 10.1017/s0033291700035558. [DOI] [PubMed] [Google Scholar]
- 96.Locke BD, McAleavey AA, Zhao Y, Lei P, Hayes JA, Castonguay LG, Li H, Tate R, Lin Y. Development and initial validation of the Counseling Center Assessment of Psychological Symptoms–34. Meas Eval Couns Dev. 2017 Mar 10;45(3):151–169. doi: 10.1177/0748175611432642. [DOI] [Google Scholar]
- 97.Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to Meta-Analysis. Chichester, UK: John Wiley & Sons, Ltd; 2009. [Google Scholar]
- 98.Lakens D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front Psychol. 2013 Nov 26;4:863. doi: 10.3389/fpsyg.2013.00863. doi: 10.3389/fpsyg.2013.00863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Hedges LV, Olkin I. Statistical Methods for Meta-Analysis. Orlando, FL: Academic Press, Inc; 1985. [Google Scholar]
- 100.Cohen J. A power primer. Psychol Bull. 1992 Jul;112(1):155–159. doi: 10.1037//0033-2909.112.1.155. [DOI] [PubMed] [Google Scholar]
- 101.Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002 Jun 15;21(11):1539–1558. doi: 10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- 102.Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editors. Cochrane Handbook for Systematic Reviews of Interventions. 2nd edition. Hoboken, NJ: John Wiley & Sons, Ltd; 2019. [Google Scholar]
- 103.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997 Sep 13;315(7109):629–634. doi: 10.1136/bmj.315.7109.629. http://europepmc.org/abstract/MED/9310563 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Duval S, Tweedie R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000 Jun;56(2):455–463. doi: 10.1111/j.0006-341x.2000.00455.x. [DOI] [PubMed] [Google Scholar]
- 105.Baumeister H, Reichler L, Munzinger M, Lin J. The impact of guidance on internet-based mental health interventions — A systematic review. Internet Interv. 2014 Oct;1(4):205–215. doi: 10.1016/j.invent.2014.08.003. [DOI] [Google Scholar]
- 106.Benassi VA, Sweeney PD, Dufour CL. Is there a relation between locus of control orientation and depression? J Abnorm Psychol. 1988 Aug;97(3):357–367. doi: 10.1037//0021-843x.97.3.357. [DOI] [PubMed] [Google Scholar]
- 107.Bandura A. Self-efficacy mechanism in human agency. Am Psychologist. 1982;37(2):122–147. doi: 10.1037/0003-066x.37.2.122. [DOI] [Google Scholar]
- 108.Hategan A, Giroux C, Bourgeois JA. Digital technology adoption in psychiatric care: An overview of the contemporary shift from technology to opportunity. J Technol Behav Sci. 2019 Mar 7;4(3):171–177. doi: 10.1007/s41347-019-00086-x. [DOI] [Google Scholar]
- 109.Czeisler MÉ, Lane RI, Petrosky E, Wiley JF, Christensen A, Njai R, Weaver MD, Robbins R, Facer-Childs ER, Barger LK, Czeisler CA, Howard ME, Rajaratnam SMW. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic - United States, June 24-30, 2020. MMWR Morb Mortal Wkly Rep. 2020 Aug 14;69(32):1049–1057. doi: 10.15585/mmwr.mm6932a1. doi: 10.15585/mmwr.mm6932a1. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Search terms for the meta-analysis.
Database screening tool.
Study demographics extracted from articles: sample, length, population, age, and gender.
Quality assessment screening.
Gamification screening for publications.
Sensitivity and supplemental analyses.
Sensitivity analysis for cognitive behavioral therapy (CBT)–only studies.