

Key Points
Question
Are changes in prices of sugar-sweetened beverages (SSBs) across cities in Mexico before and after the 2014 SSB tax associated with changes in weight-related outcomes among adolescents?
Findings
In this study, a 10% increase in SSB prices was associated with a 3% relative decrease in prevalence of overweight or obesity among adolescent girls. Improved weight-related outcomes were small and largely observed in girls with heavier weight and in cities where price increases were greater than 10% after the tax.
Meaning
Large price increases may be associated with noticeable changes in weight-related outcomes.
This study compares weight-related outcomes among adolescents living in cities in Mexico with differential price changes in sugar-sweetened beverages before and after the enactment of the 2014 sugar-sweetened beverage tax.
Abstract
Importance
Following the implementation of a tax on sugar-sweetened beverages (SSBs) in Mexico in 2014, SSB prices increased by about 10% on average, but differently across cities. It remains unclear how observed SSB price changes are associated with adolescent weight-related outcomes.
Objective
To compare weight-related outcomes among adolescents living in cities with differential SSB price changes before and after the SSB tax was implemented in Mexico.
Design, Setting, and Participants
Associations between differential SSB price changes and changes in weight-related outcomes were examined overall and by sex among 12 654 adolescents aged 10 to 18 years born between 1999 and 2002 living in 39 cities in Mexico. Multivariate regressions with individual fixed effects were applied on longitudinal individual-level yearly clinical data (height and weight) from 2012 to 2017 collected by the Instituto Mexicano del Seguro Social (IMSS) and merged with city-level SSB price data from 2011 to 2016 collected by the National Institute of Statistics and Geography (INEGI). Data were analyzed from July 2018 to July 2021.
Exposures
Yearly city-level changes in SSB prices between 2011 and 2016.
Main Outcomes and Measures
Age- and sex-specific body mass index (BMI; calculated as weight in kilograms divided by height in meters squared) percentile and indicator for overweight or obesity if BMI was at or above the 85th percentile.
Results
Before 2014, 46% of 12 654 adolescents (6850 girls and 5804 boys) included in this study had obesity or overweight. The mean (SD) age was 11.38 (1.08) years. Among girls, a 10% SSB price increase was associated with a 1.3 percentage point absolute decrease (95% CI, −2.19 to −0.36; P = .008) or a 3% relative decrease in overweight or obesity prevalence within 2 years of a price change. For girls with BMI at or above the 75th percentile pretax, this price increase was associated with a 0.59 lower BMI percentile (95% CI, −1.08 to −0.10; P = .02) or a 0.67% relative decrease. Improved outcomes for girls were observed in cities where price increases were greater than 10% after the tax. No such associations were observed for boys.
Conclusions and Relevance
In this study, increased SSB prices were associated with decreased overweight or obesity prevalence among girls but not among boys. Improvements in outcomes were small, and mostly observed for girls with heavier weight and in cities where price increases after the tax were greater than 10%.
Introduction
Given the growing evidence on adverse effects of sugar-sweetened beverages (SSBs) on adolescent obesity,1,2,3,4,5,6,7 increasing SSB prices through taxes has often been discussed as a strategy to help prevent unhealthy weight. So far, 8 US cities and 44 other countries have implemented such a public health tax.8,9 Among them was Mexico, which implemented a national excise SSB tax of Mex$ 1 (US$0.08) per liter (or about 10%) in January 2014 on beverages with added sugars, such as sodas, energy drinks, bottled teas, industrialized fruit juices, and flavored water.10 This tax was incorporated into the shelf price, making higher SSB cost more visible to the consumer than a sales tax.11
After the tax, SSB prices in Mexico increased by about 10% on average10,12,13,14 but differentially across cities. Price increases were smaller in markets facing more competition in retail and ranged from less than 5% to more than 15%.15 During this time, SSB purchases declined by about 8% on average,13,16,17,18,19,20 and by about 11% among households with adolescents,20 who consume the most SSBs of all age categories in both Mexico and the US,21,22,23 and among whom nearly one-fifth have obesity.24,25 However, 7 years after the SSB tax was enacted in Mexico, evidence on whether the observed SSB price changes have influenced adolescent weight outcomes is scarce. Prior work examining higher SSB prices or sales taxes and weight-related outcomes among adolescents is limited and so far has found either no or minimal association.26,27,28,29,30,31,32 This may be because the largely cross-sectional work has studied associations between self- or parent-reported obesity outcomes and SSB price changes or sales taxes that were possibly too small (ie, mostly below 5%26,33) to detect an effect. To our knowledge, no studies have examined how larger SSB price changes following a sizeable excise public health tax like the one implemented in Mexico may influence weight-related outcomes.
We used differential changes in SSB prices across cities before (2011 to 2013) and after (2014 to 2016) the SSB tax to provide new estimates for associations between changes in SSB prices and weight-related outcomes among urban adolescents in Mexico born between 1999 and 2002. We used multivariate individual-level fixed effects models overall and by sex and local SSB price data merged with longitudinal health records, including height and weight measured yearly between 2012 and 2017.
Methods
We analyzed data from 2011 to 2017, the years for which price and health data were available. The RAND institutional review board approved this study. Informed consent was not required as data were secondary and deidentified. Data used were free of charge and were, except for health data, publicly available. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline. Data were analyzed from July 2018 to July 2021.
Price Data
Prices, originally collected to compute the national consumer price index by the National Institute of Statistics and Geography (INEGI), were measured monthly for products sold in stores (eg, supermarkets, convenience or grocery stores, warehouse clubs, and street stalls) across 46 cities in Mexico between January 2011 and December 2016. Representative of urban areas (ie, more than 20 000 inhabitants), prices included taxes to reflect consumer prices and were tracked longitudinally for each product using a unique product code and detailed product description (ie, brand name, type, and size). Using product descriptions, we divided beverages into tax-eligible vs not (ie, with or without added sugars). We further divided tax-eligible SSBs into carbonated (eg, sodas) and noncarbonated (eg, juices, flavored water, and energy drinks). Real prices of carbonated SSBs were calculated for each year as city-level means, adjusted for inflation using the 2011 consumer price index. They were our key variable of interest because prices of noncarbonated SSBs were not collected in all cities, because sodas account for the largest share of SSB intake among adolescents,10,34 and because sodas are the main category of SSBs for which prices changed significantly after the tax.10 We also calculated yearly city-level prices of other foods that could influence outcomes irrespective of SSB price change (eAppendix 1 in the Supplement).
Health Data
We combined prices with the electronic medical records for nonpregnant adolescents aged 10 to 18 years born between 1999 and 2002 who were insured by and received outpatient health care services through the Instituto Mexicano del Seguro Social (IMSS). The IMSS is the largest public health care institution in Mexico, offering health care services for formal workers and their families (more than 50% of the population), most of whom (78%) live in urban areas and belong to the middle-income class.35,36
Height and weight were measured by a nurse or physician during each medical visit, from which we calculated yearly mean body mass index (BMI, calculated as weight in kilograms divided by height in meters squared). Data included age, sex, and diagnoses for primary cause of visit (using International Statistical Classification of Diseases and Related Health Problems, Tenth Revision [ICD-10] codes), the municipality of the clinic, and total number of medical appointments per patient per year. Our final sample was balanced and limited to patients who visited their primary care clinics at least once and up to 10 times each calendar year between 2012 and 2017. Data were averaged at a yearly level to obtain exactly 6 observations per patient.
Other Data
Publicly available nationally representative data were used to examine 2012 characteristics related to adolescent SSB intake and local environment. Databases used include the National Evaluation Council (CONEVAL), the Statistical Office for Economic Units (DENUE), and the National Health and Nutrition Survey (ENSANUT). eTable 1 in the Supplement presents details on measures obtained from these data sets.
Outcomes
Outcomes of interest were age- and sex-specific BMI percentile and indicator variables for whether adolescents had overweight or obesity (OWOB) or were at risk for OWOB, defined as having a BMI at or above the 85th and 75th percentiles, respectively. Adolescent z scores for BMI were calculated according to the World Health Organization Child Growth Reference data and converted into percentiles based on a standard normal distribution.37,38
Exposure Assignment
We combined city-level prices with adolescents’ clinical records at clinics’ municipality level. Each individual was matched to 1 of the 46 cities with the shortest distance between their clinic and the city’s municipality centroid. Adolescents were exposed to prices measured in that city. Analysis was restricted to clinics within 30 km from that city’s centroid and to adolescents who visited clinics within the same city throughout the study period (96%). The final analytic sample included 12 654 adolescents from 39 cities.
Statistical Analyses
We analyzed unadjusted trends in real SSB prices over time and across cities. Then, we divided cities into those that experienced small (<5%), medium (5% to 10%), and high (>10%) price changes after the tax vs before. For each area, we performed descriptive analyses for characteristics of adolescents and their living environments in 2012 using unadjusted means with standard deviations for continuous variables and proportions for categorical variables. We then examined unadjusted trends in prevalence of those at risk for OWOB in cities where price changes were small, medium, or high overall and by sex. Finally, we presented an ecologic association between percent changes in soda prices and BMI percentile before vs after the tax.
We estimated multivariable regression models in which key outcomes of interest were regressed on the log-transformed prices of SSB, lagged by 1 and 2 years to allow for delayed response. Coefficients describe outcome change (ie, percentage points change for binary or percent change for log-transformed continuous outcomes) for a percent change in prices, as prices are log-transformed. We reported all coefficients at the mean SSB price change of 10%. We included year fixed effects to control flexibly for general trends in outcomes and countrywide shocks (eg, national changes in soda availability and macroeconomic conditions). Regression models included a vector of individual indicators (ie, individual fixed effects) to adjust for potential confounding from individual-level (eg, genetics, preferences, and baseline differences), clinic-level, and city-level time-invariant factors, including confounders that may have influenced nonrandom price changes after the tax but that are relatively time-invariant. We included a vector of age indicators to control for age effects. Other covariates included the categories for the number of medical visits per year and an indicator variable if an individual was diagnosed with endocrine or digestive conditions that year (ICD-10 codes E00-E89 or K00-K95) (Equation 1 and eAppendix 2 in the Supplement). To examine whether BMI percentile changed differently by adolescents’ weight status pretax, we estimated our main specification for this outcome separately for adolescents who were at risk for OWOB in 2012. Models were estimated for all and by sex.
To complement descriptive analyses of unadjusted trends in outcomes across cities, we examined heterogeneous changes in outcomes before vs after the tax by areas with differential price change posttax within a regression framework. We created an after-tax indicator that equaled 1 in 2014 to 2017 and 0 otherwise. Overall and by sex, we regressed outcomes on the after-tax indicator interacted with indicators for whether a city had low, medium, or high price changes after the tax. All controls were as listed above, except that year indicators were replaced by year trends (Equation 2 in eAppendix 2 in the Supplement).
For all models, we computed 95% CIs adjusted for clustering at the city level. All analyses were conducted using Stata/MP version 16.0 (StataCorp). All P values were from 2-sided tests, and results were deemed statistically significant at P < .05.
Sensitivity Analyses
To examine medium-term effects and ignore short-term fluctuations in weight-related outcomes that may be unrelated to SSB price changes, we reestimated the main specification on a sample of outcomes measured pretax (in 2013) vs more than 2 years after the tax (2016 and 2017), excluding years 2014 and 2015. We examined whether our main results were robust to adjustments for region-specific linear time trends, for log-transformed prices of other foods lagged by 1 and 2 years, and to alternative outcomes: z BMI, Ponderal index,39 log-transformed BMI, and weight. We reproduced the analysis excluding adolescents experiencing conditions likely to influence outcomes irrespective of prices (ie, neoplasms or blood-related diseases), adjusted for the number of digestive conditions experienced per year, and associated SSB price changes with outcomes likely unaffected by them (eg, injuries and accidents).
Results
Study Sample and Exposure
The sample in this study is a balanced patient-year panel of 12 654 urban adolescents born between 1999 and 2002 (6850 girls and 5804 boys) for the period from 2012 to 2017, merged with yearly prices spanning 39 cities between 2011 and 2016. Pretax (2012 to 2013), the mean (SD) age of adolescents was 11.38 (1.08) years. The mean (SD) number of clinic visits per year was 3.59 (2.36); 0.45 (0.95) or 12.74% of total visits were because of a digestive issue and 0.109 (0.66) or 2.54% were because of an endocrine medical issue. More than half of adolescents (7111 [56.03%]) were at risk for OWOB, and 5878 (46.08%) were OWOB (Table 1).
Table 1. Descriptive Statistics for Adolescents and Their Living Environments in 2012 and 2013a.
| Characteristic | Mean (SD) | |||
|---|---|---|---|---|
| All | SSB price change posttax | |||
| Small (<5%)b | Medium (5%-10%)c | High (>10%)d | ||
| Individual characteristicse | ||||
| Unique patients, no. | 12 654 | 1499 | 6986 | 4169 |
| Age, y | 11.38 (1.08) | 11.39 (1.08) | 11.33 (1.06)f | 11.46 (1.11)f |
| Female, no. (%) | 6850 (54.13) | 839 (55.97) | 3762 (53.85)g | 2249 (53.95) |
| Male, no. (%) | 5804 (45.87) | 660 (44.03) | 3224 (46.15)g | 1920 (46.05) |
| Weight, kg | 43.26 (12.37) | 43.11 (11.81) | 42.76 (12.18) | 44.16 (12.82)f |
| Height, m | 1.45 (0.10) | 1.45 (0.10) | 1.45 (0.10) | 1.45 (0.10) |
| BMI, pct | 69.65 (30.57) | 69.29 (30.01) | 68.73 (30.66) | 71.32 (30.55)f |
| At risk for OWOB (≥75th pct) prevalence, % | 56.03 | 54.80 | 54.34 | 59.28f |
| OWOB (≥85th pct) prevalence, % | 46.08 | 44.70 | 44.42 | 49.38f |
| Digestive visits, % of total visits | 12.74 (25.61) | 16.37 (29.31) | 11.84 (24.61)f | 12.94 (25.71)f |
| Endocrine visits, % of total visits | 2.54 (13.37) | 2.86 (14.34) | 2.36 (12.88) | 2.73 (13.81) |
| No. of visits per y | 3.59 (2.36) | 3.44 (2.31) | 3.63 (2.38)f | 3.57 (2.35)g |
| Local characteristicsh | ||||
| SSB price, 2011 Mex$i | 9.81 (1.37) | 9.96 (1.46) | 10.17 (1.01) | 9.65 (1.45) |
| Daily soda intake (ages 12-18 y), mL/d | 219.76 (25.15) | 224.71 (24.29) | 212.08 (35.99) | 220.38 (22.25) |
| Middle school or more education, % | 62.32 (11.99) | 61.02 (14.32) | 69.19 (7.26) | 60.73 (11.87) |
| Extreme poverty, % | 8.60 (7.46) | 8.46 (4.45) | 6.89 (5.05) | 9.18 (8.98) |
| Informal employment, % | 58.17 (13.30) | 60.52 (12.82) | 53.88 (11.03) | 58.55 (14.30) |
| No. of supermarkets per 100 convenience stores | 5.63 (5.01) | 2.91 (1.99) | 5.14 (3.54) | 6.86 (5.83) |
Abbreviations: BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); OWOB, overweight or obesity; pct, percentile; SSB, sugar-sweetened beverages.
Table shows descriptive statistics and tests for significant differences across cities using mean comparison t tests comparing medium– and high–price change cities with small–price change cities, respectively; differences are significantly different from 0 if noted.
Includes 9 cities; 1499 individuals.
Includes 7 cities; 6986 individuals.
Includes 23 cities; 4169 individuals.
Individual characteristics are calculated from IMSS health data and are the pretax means (2012-2013).
P < .01.
P < .05.
Descriptive statistics at the city level for the cities in our sample. Data on city characteristics were obtained from La Encuesta Nacional de Salud y Nutrición (2012), the National Council for the Evaluation of Social Development Policy (2010), and El Directorio Estadístico Nacional de Unidades Económicas (2012). See eAppendix 1 and eTable 1 in the Supplement for details.
To convert 2011 Mex$ to 2011 US$, multiply by 0.08.
Figure 1A shows mean SSB prices over time. Relative to 2013, mean SSB prices increased by a mean of 10% in 2014 and remained relatively stable thereafter. Figure 1B shows that SSB price changes varied across cities, ranging from −12% to more than 25% before vs after the tax. Adolescents were therefore exposed to differential SSB price changes during our study period. Price changes were greater than 10% in 23 cities (4169 adolescents), 5% to 10% in 7 cities (6986 adolescents), and below 5% in 9 cities (1499 adolescents). We used this variation in prices to estimate associations between price changes with changes in weight-related outcomes.
Figure 1. Changes in Sugar-Sweetened Beverage (SSB) Prices Over Time and Across Cities.
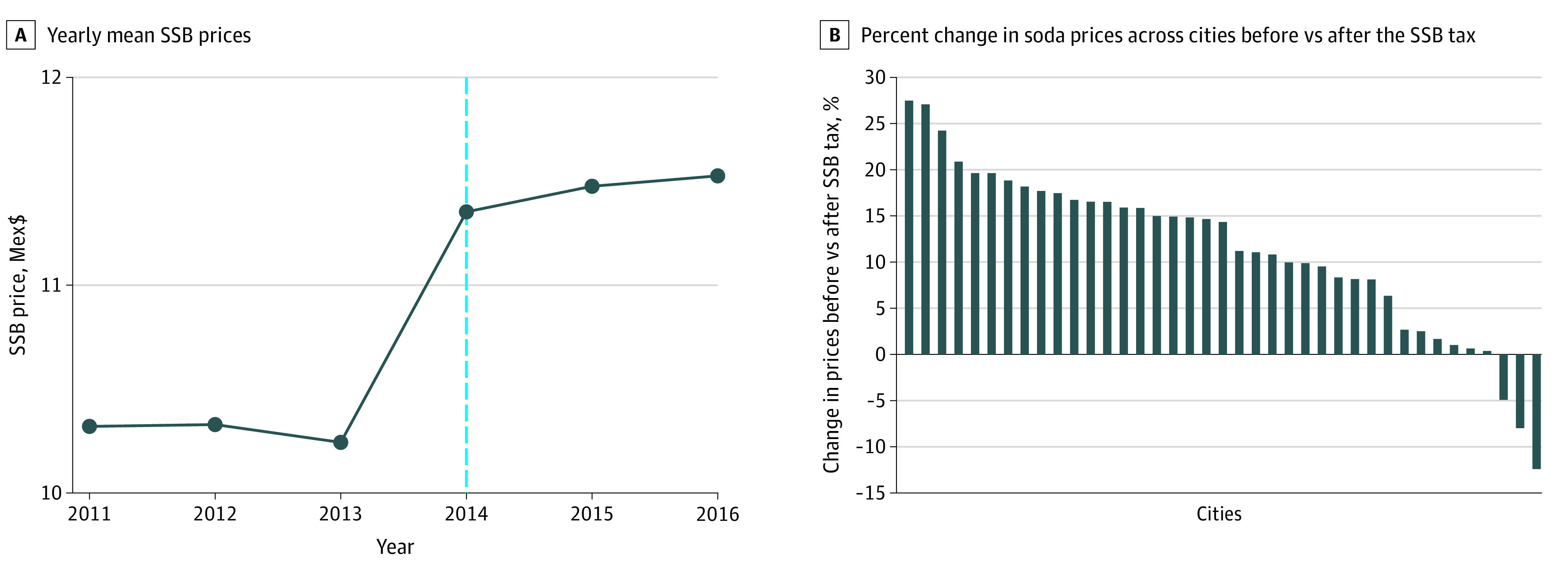
A, Unweighted mean prices of carbonated SSBs expressed per product per 1 L per year between 2011 and 2016. Nominal prices were deflated using the January 2011 consumer price index. To convert 2011 Mex$ to 2011 US$, multiply by 0.08. The dashed line indicates implementation of the SSB tax in January 2014.
B, Percent change in real prices of carbonated SSBs before and after the tax. Price changes following the tax were >10% in 23 cities (4169 adolescents), 5%-10% in 7 cities (6986 adolescents), and <5% in 9 cities (1499 adolescents).
Table 1 shows that in cities with high price change (>10%) adolescents were heavier than in cities with lower price changes (<5% and 5% to 10%) and were more likely to be considered OWOB (49% vs 44%, respectively). In terms of population and market characteristics that could be associated with price changes after the tax (eg, education, taste for SSB, or market structure8,15,40,41), we found no statistically significant differences, although the share of larger vs smaller retail (eg, supermarkets vs convenience stores) increased with price change, a finding consistent with prior work.15,41
Figure 2 shows unadjusted time trends for the at risk OWOB prevalence across cities with small, medium, or high price changes posttax. While the rates of adolescents at risk for OWOB were parallel across the 3 city types pretax, a change in slope was observed only for adolescents living in cities experiencing a greater than 10% price change after 2014, where the mean (SD) price change was 16.6% (4.25%), and not for cities with smaller SSB price changes (Figure 2A). This was observed among girls (Figure 2B) and not among boys (Figure 2C). Consistently, eFigure 1 in the Supplement presents adjusted regression estimates for changes in prevalence of at risk for OWOB before vs after the tax across cities with differential price changes. A significant decrease in this outcome posttax was observed only for girls and in cities in which SSB price changes before vs after the tax were greater than 10%.
Figure 2. Unadjusted Trends in Prevalence of Adolescents at Risk for Overweight or Obesity by Areas With Differential Price Change Following the Sugar-Sweetened Beverage (SSB) Tax.
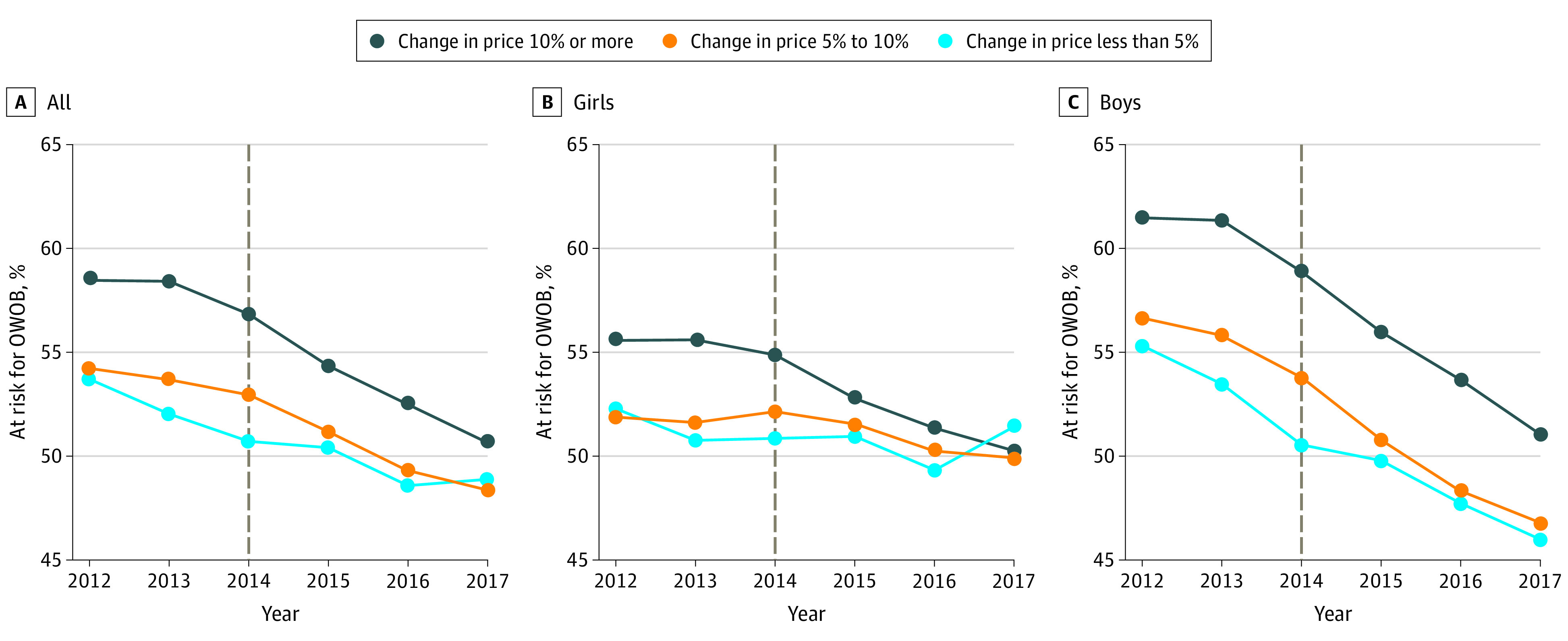
A, Mean prevalence at risk for overweight or obesity (OWOB) among all adolescents included in the study. Sample is restricted to a cohort of adolescents living in cities who were born between 1999 and 2002 and whose weight and height were measured at an Instituto Mexicano del Seguro Social clinic at least once per year between 2012 and 2017. Price changes following the tax were >10% in 23 cities (4169 adolescents), 5%-10% in 7 cities (6986 adolescents), and <5% in 9 cities (1499 adolescents). The dashed line indicates the start of the SSB tax in January 2014.
B, Mean prevalence of at risk for OWOB for girls.
C, Mean prevalence of at risk for OWOB for boys.
Associations Between Changes in SSB Prices and Weight-Related Outcomes
We observed a small negative unadjusted association between soda price changes and changes in BMI percentile at the city level (eFigure 2 in the Supplement). Table 2 presents adjusted associations between a 1- and 2-year lag of SSB prices and weight-related outcomes for all adolescents, girls, and boys, but significant associations were observed only for girls. Among girls, we observed no association between 1-year price lag and weight outcomes. However, we saw that within 2 years of a price change, a 10% SSB price increase (ie, the mean price change observed after the tax) was associated with a 1.3 percentage point (95% CI, −2.2 to −0.36; P = .008) and a 1.3 percentage point (95% CI, −2.1 to −0.38; P = .006) absolute, or a 2.4% and 3.0% relative decrease in the probability of being at risk for OWOB and OWOB, respectively. Table 3 shows that for girls at risk for OWOB in 2012, such a price increase was associated with a 0.59 (95% CI, −1.08 to −0.10; P = .02) lower BMI percentile or a 0.67% decrease relative to the pretax mean (SD) BMI percentile of 88.75 (14.20). This corresponds to a 0.35-kg weight loss given the mean (SD) weight pretax (52.62 [11.37] kg). Consistent results were found using alternative measures (ie, z-BMI, BMI, Ponderal index, weight) (eTable 5 in the Supplement). We found no significant change in this outcome for boys or girls who were not at risk for OWOB at baseline.
Table 2. Association Between Changes in Sugar-Sweetened Beverage (SSB) Prices and Weight-Related Outcomes Among Urban Adolescentsa.
| Outcome | BMI (pct) | At risk for OWOB (≥75th pct) | OWOB (≥85th pct) |
|---|---|---|---|
| All individuals (N = 12 654) | |||
| Log(price of soda)t-1 (95% CI) | −0.03 (−0.55 to 0.49) | −0.46 (−1.46 to 0.55) | −0.09 (−0.91 to 0.72) |
| Log(price of soda)t-2 (95% CI) | −0.14 (−0.46 to 0.19) | −0.66 (−1.34 to 0.01) | −0.75 (−1.44 to −0.06)b |
| Girls (n = 6850) | |||
| Log(price of soda)t-1 (95% CI) | −0.08 (−0.69 to 0.54) | −0.20 (−1.38 to 0.99) | 0.54 (−0.34 to 1.42) |
| Log(price of soda)t-2 (95% CI) | −0.45 (−0.94 to 0.04) | −1.27 (−2.19 to −0.36)c | −1.26 (−2.14 to −0.38)c |
| Boys (n = 5804) | |||
| Log(price of soda)t-1 (95% CI) | 0.13 (−0.55 to 0.80) | −0.66 (−2.10 to 0.78) | −0.74 (−1.82 to 0.34) |
| Log(price of soda)t-2 (95% CI) | 0.24 (−0.38 to 0.86) | 0.08 (−0.84 to 1.00) | −0.13 (−1.11 to 0.85) |
Abbreviations: BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); OWOB, overweight or obesity; pct, percentile.
Control variables include categories for the number of individual visits to a clinic in a year; indicator variables if the individual was diagnosed with endocrine or digestive diseases in a year; and individual, age, and year fixed effects. Confidence intervals calculated using cluster robust standard errors at the city level. All coefficients are multiplied by 10 to interpret their magnitude in terms of the mean soda price increase observed across cities following the SSB tax, which was 10%. Total observations: 63 270 (all), 34 250 (girls), and 29 020 (boys).
P<.05.
P<.01.
Table 3. Association Between Changes in Sugar-Sweetened Beverage (SSB) Prices and Body Mass Index (BMI) Percentile by Weight Status Prior to 2014 SSB Taxa.
| Outcome: BMI percentile | All | Girls | Boys |
|---|---|---|---|
| Not at risk for OWOB pretax | |||
| Log(price of soda)t-1 (95% CI) | 0.14 (−0.61 to 0.89) | −0.17 (−1.11 to 0.77) | 0.64 (−0.39 to 1.68) |
| Log(price of soda)t-2 (95% CI) | −0.04 (−0.60 to 0.52) | −0.28 (−1.11 to 0.54) | 0.24 (−0.86 to 1.34) |
| Mean BMI percentile | 0.43 | 0.43 | 0.44 |
| Unique patients | 5543 | 3180 | 2363 |
| At risk for OWOB pretax | |||
| Log(price of soda)t-1 (95% CI) | −0.02 (−0.50 to 0.46) | 0.12 (−0.53 to 0.77) | −0.11 (−0.75 to 0.54) |
| Log(price of soda)t-2 (95% CI) | −0.18 (−0.47 to 0.10) | −0.60 (−1.08 to −0.11)b | 0.28 (−0.16 to 0.71) |
| Mean BMI percentile | 0.89 | 0.88 | 0.90 |
| Unique patients | 7111 | 3670 | 3441 |
Abbreviations: BMI, body mass index (calculated as weight in kilograms divided by height in meters squared); OWOB, overweight or obesity.
Models show coefficients of regressions that include the regressors of interest; individual, year, and age fixed effects; and other controls, including categories for the number of individual visits to a clinic in a year and indicator variables if the individual was diagnosed with an endocrine or digestive disease in that year. Confidence intervals calculated using cluster robust standard errors at the city level. Sample includes a balanced panel of individuals from 2012 to 2017, observed at least once per year and up to 10 times per year for an urban adolescent cohort born between 1999 and 2002.
P < .05.
Sensitivity Analyses
eTable 3 in the Supplement shows that our findings were robust after excluding the first 2 years of data after the tax implementation (2014 and 2015) and including other prices as controls. eTable 4 in the Supplement shows our results were consistent after adjusting for regional time trends, after excluding patients diagnosed with conditions possibly affecting their weight independent of price changes (ie, neoplasms or blood-related diseases), and after controlling for the number of digestive diagnoses, and shows no significant association between prices and health outcomes unlikely affected by diet. Results were consistent across alternative weight-related outcomes for girls with heavier weight at baseline (eTable 5 in the Supplement).
Discussion
While the literature has established a consistent association between the SSB tax in Mexico, increased SSB prices, and a decline in SSB purchases after 2014,10,13,14,15,16,18,20 this study adds evidence that increased SSB prices at this time were associated with decreased OWOB prevalence among adolescent girls. A small but significant decrease in BMI percentile was observed for girls with heavier weight, and improved weight-related outcomes were observed largely in cities where price changes after the tax were greater than 10%. We observed no such results for boys, consistent with findings that soda intake posttax decreased among urban adolescent girls but not boys.17
SBB price increases observed in our data were not associated with change in BMI percentile on average, but were associated with a small reduction in BMI percentile for girls with heavier weight. This finding is consistent with prior work showing that weight at the right tail of BMI distribution is more likely to change with SSB price changes.26,42,43 Assuming that reduction in energy intake of 10 calories daily leads to a steady state weight loss of 0.45 kg over 2 years,44 the 0.35-kg weight loss calculated in this study would correspond to a reduced intake of about 7.8 calories daily. This calorie change is comparable with the SSB purchase decline expected or observed in prior work studying Mexican youth, which projects a similar weight loss using a microsimulation approach.45,46 However, our estimates are smaller compared with other modeling work, which is largely based in the US and assumes a larger reduction in calorie intake following a similar price change.47,48,49,50
Prior work has found associations of SSB prices or sales taxes with individual-level adolescent outcomes and found that in the absence of larger price changes it is unlikely that unhealthy weight will be significantly reduced for adolescents overall.26,27,29,31,33,42 These studies used beverage price changes or tax rates mostly smaller than 5% and, consistent with our findings at the level of such price changes, show minimal or no significant change in weight-related outcomes at the population level after the tax. We observed improved weight-related outcomes largely in cities where price changes after the tax were greater than 10% or 16.6% on average. If effects were linear, such a price increase would predict a 1.1% relative decrease in BMI percentile for girls with heavier weight. Prior work using US data suggests that a reduction in mean BMI of 1% to 5% is needed to achieve a meaningful improvement in health.51,52 Thus, larger increases in SBB prices could have larger population effects.
Limitations
This study has limitations. First, results are not generalizable to rural adolescents and those not covered by IMSS. Price data are representative of urban areas, and health data are limited to patients who visited IMSS clinics annually. These individuals are younger, slightly heavier, and less likely to be male than the average Mexican adolescent (eTable 2 in the Supplement). Second, owing to data limitations, we did not explore heterogeneity by socioeconomic status or baseline SSB consumption. Third, the prices we used are proxies for those to which children were actually exposed. Fourth, our results are robust to alternative specifications and weight-related outcomes, but this is not a randomized trial, so results may not be causal. Other initiatives directed at children, such as regulation of unhealthy diet in schools and in advertising, were undertaken during this time,53 but we did not have data on these variables. Our results might be upward biased if these initiatives were more aggressive in cities where price changes were the largest or attenuated if SSB manufacturers or retailers strengthened their marketing strategies in those cities. Fifth, heterogenous price changes are nonrandom and depend on local demand (ie, taste for SSB, health awareness, or income) and supply (ie, strategic behavior by retailers or soda suppliers). Several factors that proxy for these different market conditions do not differ in means across areas with differential price change (Table 1) and are likely to change slowly, but we could not identify all confounders in our data.
Conclusions
In this study, increased SSB prices were associated with decreased overweight or obesity prevalence for girls, but not for boys. Improvements in outcomes were small and mostly observed for girls with heavier weight and in cities where prices after the tax increased by more than 10%.
eAppendix 1. Data and study sample
eTable 1. Description of data sources for individual and environment characteristics
eTable 2. Descriptive statistics as observed in IMSS and ENSANUT in 2012
eAppendix 2. Statistical analyses
eTable 3. Association between soda prices and changes in weight-related outcomes for 1999-2002 birth cohort between 2013-2017 using alternative model specifications
eTable 4. Association between soda prices and changes in weight-related outcomes using alternative model specifications to address endogeneity concerns
eTable 5. Association between soda prices and changes in weight-related outcomes using alternative measures of body mass by weight status prior to tax
eFigure 1. Changes in weight-related outcomes before vs after the tax across cities with different price changes
eFigure 2. Ecological association between SSB price changes and changes in BMI percentile
References
- 1.Malik VS, Popkin BM, Bray GA, Després J-P, Hu FB. Sugar-sweetened beverages, obesity, type 2 diabetes mellitus, and cardiovascular disease risk. Circulation. 2010;121(11):1356-1364. doi: 10.1161/CIRCULATIONAHA.109.876185 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Malik VS, Schulze MB, Hu FB. Intake of sugar-sweetened beverages and weight gain: a systematic review. Am J Clin Nutr. 2006;84(2):274-288. doi: 10.1093/ajcn/84.2.274 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hu FB. Resolved: there is sufficient scientific evidence that decreasing sugar-sweetened beverage consumption will reduce the prevalence of obesity and obesity-related diseases. Obes Rev. 2013;14(8):606-619. doi: 10.1111/obr.12040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Harrington S. The role of sugar-sweetened beverage consumption in adolescent obesity: a review of the literature. J Sch Nurs. 2008;24(1):3-12. doi: 10.1177/10598405080240010201 [DOI] [PubMed] [Google Scholar]
- 5.Cantoral A, Téllez-Rojo MM, Ettinger AS, Hu H, Hernández-Ávila M, Peterson K. Early introduction and cumulative consumption of sugar-sweetened beverages during the pre-school period and risk of obesity at 8-14 years of age. Pediatr Obes. 2016;11(1):68-74. doi: 10.1111/ijpo.12023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lustig RH. Ultraprocessed food: addictive, toxic, and ready for regulation. Nutrients. 2020;12(11):3401. doi: 10.3390/nu12113401 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Keller A, Bucher Della Torre S. Sugar-sweetened beverages and obesity among children and adolescents: a review of systematic literature reviews. Child Obes. 2015;11(4):338-346. doi: 10.1089/chi.2014.0117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cawley J, Thow AM, Wen K, Frisvold D. The economics of taxes on sugar-sweetened beverages: a review of the effects on prices, sales, cross-border shopping, and consumption. Annu Rev Nutr. 2019;39:317-338. doi: 10.1146/annurev-nutr-082018-124603 [DOI] [PubMed] [Google Scholar]
- 9.University of North Carolina Global Food Research Program . Sugary drink taxes around the world. Accessed August 2, 2021. https://www.globalfoodresearchprogram.org/wp-content/uploads/2021/04/SSB_sugary_drink_taxes_maps.pdf
- 10.Colchero MA, Salgado JC, Unar-Munguía M, Molina M, Ng S, Rivera-Dommarco JA. Changes in prices after an excise tax to sweetened sugar beverages was implemented in Mexico: evidence from urban areas. PLoS One. 2015;10(12):e0144408. doi: 10.1371/journal.pone.0144408 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chriqui JF, Chaloupka FJ, Powell LM, Eidson SS. A typology of beverage taxation: multiple approaches for obesity prevention and obesity prevention-related revenue generation. J Public Health Policy. 2013;34(3):403-423. doi: 10.1057/jphp.2013.17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ng SW, Rivera JA, Popkin BM, Colchero MA. Did high sugar-sweetened beverage purchasers respond differently to the excise tax on sugar-sweetened beverages in Mexico? Public Health Nutr. 2019;22(4):750-756. doi: 10.1017/S136898001800321X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Aguilar A, Gutierrez E, Seira E. The effectiveness of sin food taxes: Evidence from Mexico. J Health Econ. 2021;77:102455. doi: 10.1016/j.jhealeco.2021.102455 [DOI] [PubMed] [Google Scholar]
- 14.Grogger J. Soda taxes and the prices of sodas and other drinks: evidence from Mexico. Am J Agric Econ, 2017;99(2):481-498. doi: 10.1093/ajae/aax024 [DOI] [Google Scholar]
- 15.Campos-Vázquez RM, Medina-Cortina EM. Pass-through and competition: the impact of soft drink taxes as seen through Mexican supermarkets. Lat Am Econ Rev. 2019;28(1):1-23. doi: 10.1186/s40503-019-0065-5 [DOI] [Google Scholar]
- 16.Colchero MA, Rivera-Dommarco J, Popkin BM, Ng SW. In Mexico, evidence of sustained consumer response two years after implementing a sugar-sweetened beverage tax. Health Aff. 2017;36(3):564-571. doi: 10.1377/hlthaff.2016.1231 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Martí Malvido E. Adolescents’ soda consumption in Mexico before and after the sugar-sweetened beverages tax: results from national health and nutrition surveys. University of Massachusetts, Amherst. Published 2018. Accessed November 15, 2021. https://scholarworks.umass.edu/cppa_capstones/48/
- 18.Colchero MA, Popkin BM, Rivera JA, Ng SW. Beverage purchases from stores in Mexico under the excise tax on sugar sweetened beverages: observational study. BMJ. 2016;352:h6704. doi: 10.1136/bmj.h6704 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Colchero MA, Guerrero-López CM, Molina M, Rivera JA. Beverages sales in Mexico before and after implementation of a sugar sweetened beverage tax. PLoS One. 2016;11(9):e0163463. doi: 10.1371/journal.pone.0163463 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Colchero MA, Molina M, Guerrero-López CM. After Mexico implemented a tax, purchases of sugar-sweetened beverages decreased and water increased: difference by place of residence, household composition, and income level. J Nutr. 2017;147(8):1552-1557. doi: 10.3945/jn.117.251892 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Wang YC, Bleich SN, Gortmaker SL. Increasing caloric contribution from sugar-sweetened beverages and 100% fruit juices among US children and adolescents, 1988-2004. Pediatrics. 2008;121(6):e1604-e1614. doi: 10.1542/peds.2007-2834 [DOI] [PubMed] [Google Scholar]
- 22.Rodríguez-Ramírez S, Mundo-Rosas V, García-Guerra A, Shamah-Levy T. Dietary patterns are associated with overweight and obesity in Mexican school-age children. Arch Latinoam Nutr. 2011;61(3):270-278. [PubMed] [Google Scholar]
- 23.García-Chávez CG, Rivera JA, Monterrubio-Flores E, Rodríguez-Ramírez S. Dietary patterns are associated with obesity in Mexican schoolchildren. Eur J Clin Nutr. 2020;74(8):1201-1209. doi: 10.1038/s41430-020-0598-3 [DOI] [PubMed] [Google Scholar]
- 24.Aceves-Martins M, Llauradó E, Tarro L, Solà R, Giralt M. Obesity-promoting factors in Mexican children and adolescents: challenges and opportunities. Glob Health Action. 2016;9(1):29625. doi: 10.3402/gha.v9.29625 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.US Centers for Disease Control and Prevention . Prevalence of childhood obesity in the United States. Accessed November 8, 2021. https://www.cdc.gov/obesity/data/childhood.html
- 26.Sturm R, Powell LM, Chriqui JF, Chaloupka FJ. Soda taxes, soft drink consumption, and children’s body mass index. Health Aff. 2010;29(5):1052-1058. doi: 10.1377/hlthaff.2009.0061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Fletcher JM, Frisvold DE, Tefft N. The effects of soft drink taxes on child and adolescent consumption and weight outcomes. J. Public Econ. 2010;94(11-12):967-974. doi: 10.1016/j.jpubeco.2010.09.005 [DOI] [Google Scholar]
- 28.Fletcher JM, Frisvold D, Tefft N. Taxing soft drinks and restricting access to vending machines to curb child obesity. Health Aff. 2010;29(5):1059-1066. doi: 10.1377/hlthaff.2009.0725 [DOI] [PubMed] [Google Scholar]
- 29.Fletcher JM, Frisvold DE, Tefft N. Non-linear effects of soda taxes on consumption and weight outcomes. Health Econ. 2015;24(5):566-582. doi: 10.1002/hec.3045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Powell LM, Chriqui J, Chaloupka FJ. Associations between state-level soda taxes and adolescent body mass index. J Adolesc Health. 2009;45(3)(suppl):S57-S63. doi: 10.1016/j.jadohealth.2009.03.003 [DOI] [PubMed] [Google Scholar]
- 31.Han E, Powell LM. Effect of food prices on the prevalence of obesity among young adults. Public Health. 2011;125(3):129-135. doi: 10.1016/j.puhe.2010.11.014 [DOI] [PubMed] [Google Scholar]
- 32.Wendt M, Todd JE. Effect of Food and Beverage Prices on Children's Weights. DIANE Publishing; 2011. [Google Scholar]
- 33.Fletcher JM, Frisvold D, Tefft N. Can soft drink taxes reduce population weight? Contemp Econ Policy. 2010;28(1):23-35. doi: 10.1111/j.1465-7287.2009.00182.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Sánchez-Pimienta TG, Batis C, Lutter CK, Rivera JA. Sugar-sweetened beverages are the main sources of added sugar intake in the Mexican population. J Nutr. 2016;146(9):1888S-1896S. doi: 10.3945/jn.115.220301 [DOI] [PubMed] [Google Scholar]
- 35.Marquez-Padilla F. When less is more: can reduced health monitoring improve medication adherence? J Health Econ. 2021;75:102387. doi: 10.1016/j.jhealeco.2020.102387 [DOI] [PubMed] [Google Scholar]
- 36.Llamas RV, Rubio MYN. Salarios e informalidad laboral en México: una perspectiva regional y empresarial. Rev Estud Reg. 2020(118):15-46. https://dialnet.unirioja.es/servlet/articulo?codigo=7695427 [Google Scholar]
- 37.Vidmar SI, Cole TJ, Pan H. Standardizing anthropometric measures in children and adolescents with functions for egen: update. Stata J. 2013;13(2):366-378. doi: 10.1177/1536867X1301300211 [DOI] [Google Scholar]
- 38.World Health Organization . Growth reference data for 5-19 years. Accessed November 8, 2021. https://www.who.int/toolkits/growth-reference-data-for-5to19-years
- 39.Zaniqueli D, Oliosa PR, Neves FS, et al. Ponderal index classifies obesity in children and adolescents more accurately than body mass index z-scores. Pediatr Res. 2019;86(1):128-133. doi: 10.1038/s41390-019-0395-7 [DOI] [PubMed] [Google Scholar]
- 40.Weyl EG, Fabinger M. Pass-through as an economic tool: principles of incidence under imperfect competition. Journal of Political Economy. 2013;121(3):528-583. doi: 10.1086/670401 [DOI] [Google Scholar]
- 41.Salgado JC, Ng SW. Understanding heterogeneity in price changes and firm responses to a national unhealthy food tax in Mexico. Food Policy. 2019;89:101783. doi: 10.1016/j.foodpol.2019.101783 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Powell LM, Chriqui JF, Khan T, Wada R, Chaloupka FJ. Assessing the potential effectiveness of food and beverage taxes and subsidies for improving public health: a systematic review of prices, demand and body weight outcomes. Obes Rev. 2013;14(2):110-128. doi: 10.1111/obr.12002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Powell LM, Chaloupka FJ. Food prices and obesity: evidence and policy implications for taxes and subsidies. Milbank Q. 2009;87(1):229-257. doi: 10.1111/j.1468-0009.2009.00554.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Hall KD, Sacks G, Chandramohan D, et al. Quantification of the effect of energy imbalance on bodyweight. Lancet. 2011;378(9793):826-837. doi: 10.1016/S0140-6736(11)60812-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Barrientos-Gutierrez T, Zepeda-Tello R, Rodrigues ER, et al. Expected population weight and diabetes impact of the 1-peso-per-litre tax to sugar sweetened beverages in Mexico. PLoS One. 2017;12(5):e0176336. doi: 10.1371/journal.pone.0176336 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Basto-Abreu A, Barrientos-Gutiérrez T, Vidaña-Pérez D, et al. Cost-effectiveness of the sugar-sweetened beverage excise tax in Mexico. Health Aff. 2019;38(11):1824-1831. doi: 10.1377/hlthaff.2018.05469 [DOI] [PubMed] [Google Scholar]
- 47.Smith TA. Taxing Caloric Sweetened Beverages: Potential Effects on Beverage Consumption, Calorie Intake, and Obesity. DIANE Publishing; 2010. [Google Scholar]
- 48.Long MW, Gortmaker SL, Ward ZJ, et al. Cost effectiveness of a sugar-sweetened beverage excise tax in the US. Am J Prev Med. 2015;49(1):112-123. doi: 10.1016/j.amepre.2015.03.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Kristensen AH, Flottemesch TJ, Maciosek MV, et al. Reducing childhood obesity through U.S. federal policy: a microsimulation analysis. Am J Prev Med. 2014;47(5):604-612. doi: 10.1016/j.amepre.2014.07.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Wright A, Smith KE, Hellowell M. Policy lessons from health taxes: a systematic review of empirical studies. BMC Public Health. 2017;17(1):583. doi: 10.1186/s12889-017-4497-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Wang YC, McPherson K, Marsh T, Gortmaker SL, Brown M. Health and economic burden of the projected obesity trends in the USA and the UK. Lancet. 2011;378(9793):815-825. doi: 10.1016/S0140-6736(11)60814-3 [DOI] [PubMed] [Google Scholar]
- 52.Levi J, Segal LM, St Laurent R, Lang A, Rayburn J. F as in Fat: How Obesity Threatens America’s Future 2012. Robert Wood Johnson Foundation; Trust for America’s Health. Published September 1, 2012. Accessed November 8, 2021. https://www.rwjf.org/en/library/research/2012/09/f-as-in-fat--how-obesity-threatens-america-s-future-2012.html
- 53.Álvarez-Sánchez C, Contento I, Jiménez-Aguilar A, et al. Does the Mexican sugar-sweetened beverage tax have a signaling effect? ENSANUT 2016. PLoS One. 2018;13(8):e0199337. doi: 10.1371/journal.pone.0199337 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eAppendix 1. Data and study sample
eTable 1. Description of data sources for individual and environment characteristics
eTable 2. Descriptive statistics as observed in IMSS and ENSANUT in 2012
eAppendix 2. Statistical analyses
eTable 3. Association between soda prices and changes in weight-related outcomes for 1999-2002 birth cohort between 2013-2017 using alternative model specifications
eTable 4. Association between soda prices and changes in weight-related outcomes using alternative model specifications to address endogeneity concerns
eTable 5. Association between soda prices and changes in weight-related outcomes using alternative measures of body mass by weight status prior to tax
eFigure 1. Changes in weight-related outcomes before vs after the tax across cities with different price changes
eFigure 2. Ecological association between SSB price changes and changes in BMI percentile