

Abstract
Background:
Sex-based differences in neuromuscular characteristics relevant to anterior cruciate ligament (ACL) injury risk may arise as compensation for divergent strength development during puberty. Strength training during this period may prevent the development of these undesirable neuromuscular characteristics.
Hypothesis:
Strength-trained middle school girls will have improved jump-landing biomechanics compared with control participants.
Study Design:
Cohort study.
Level of Evidence:
Level 3.
Methods:
Maximum voluntary isometric contraction in hip extension and abduction and knee extension and flexion as well as Landing Error Scoring System (LESS) scores were collected for healthy female middle school students of grades 6 to 8. Strength-training participants (STR: N = 30; height, 1.63 ± 0.07 m; mass, 48.1 ± 7.6 kg; age, 12.5 ± 1.0 y) were matched with control participants (CON: N = 30; height, 1.60 ± 0.09 m; mass, 47.2 ± 8.9 kg; age, 12.6 ± 0.9 y). The training consisted of a 6-month strength-training program administered through a gym class curriculum that targeted the lower extremity. A repeated-measures mixed-model analysis of variance was used for comparisons between groups and across time (α = 0.05). Stepwise linear regression was used to examine the relationship between strength change and LESS score change.
Results:
Strength values (N·m/kg) increased across time and to a greater degree in STR for hip extension (baseline 3.98 ± 1.15 vs follow-up 4.77 ± 1.80), hip abduction (4.22 ± 1.09 vs 5.13 ± 2.55), and knee flexion (3.27 ± 0.62 vs 3.64 ± 1.40) compared with CON. LESS grades significantly decreased across time in STR (5.58 ± 1.21 vs 4.86 ± 1.44) and were significantly lower than CON (5.98 ± 1.42) at follow-up (P < 0.001). The change in hip extension and knee extension strength explained 67% of the variance (P < 0.001) in the LESS change score in the STR group.
Conclusion:
A school-based strength-training program that focused on hip and knee musculature significantly improved jump-landing biomechanics (as determined by LESS) relevant to ACL injury risk. Further investigation using different strength-training approaches in this age group is warranted.
Clinical Relevance:
Strength training during adolescence holds promise as an injury prevention program. The use of a school-based approach is novel and may represent a robust opportunity for injury prevention programs, as physical education class is often mandatory in this age group.
Keywords: anterior cruciate ligament, strength training, injury risk, injury prevention
Studies have repeatedly demonstrated that female patients have a higher rate of noncontact anterior cruciate ligament (ACL) injury than male patients.7,14,27,37 Differences in lower extremity biomechanics are believed to be a significant contributor to this sex bias in injury risk.5,18,22
These differences in lower extremity biomechanics increase during maturation and are associated with a concomitant increase in injury risk.11,12,19,21,40-42 Structural changes such as with height and body mass may result in increased forces during sports activities.11,12,19,21,40-42 Increases in strength may help athletes accommodate these changes in height and mass; however, male athletes tend to gain greater strength during maturation compared with their female counterparts; peak strength gains tend to follow peak height velocity and peak mass velocity closer in male athletes. 2 This “uncoupling” of strength in both magnitude and temporal effect from changes in height and mass may help drive the development of compensatory high-risk biomechanics in female athletes and thus increase injury risk.20,28,45
Lower extremity biomechanics can be improved and the risk of ACL injury decreased via neuromuscular-based interventions.47,50 However, these studies have primarily focused on improving existing altered lower extremity biomechanics as opposed to preventing the high-risk biomechanical patterns, which may develop during maturation. An intervention that improves strength development in female athletes during maturation may serve to prevent the development of risky biomechanical patterns and hence reduce future risk of ACL injury.24,29
Strength-training interventions in prematuration female athletes may have an advantage over multicomponent injury prevention programs. It may be easier to gain acceptance by athletes and coaches because of its performance benefits. Simple strength-training regimens may also be easy to implement and could potentially even be part of the curriculum for a physical education class, which is often mandatory in middle schools in the United States. To date, strength-training interventions have had mixed results in improving lower extremity biomechanics; however, most of these studies have targeted postmaturation participants such as college-aged athletes.6,10,17,46 As such, the strength interventions in these studies were applied after the development of altered biomechanical patterns rather than as a method of preventing the development of these biomechanical patterns.
To date, there is only 1 study that has investigated the effects of strength training on lower extremity biomechanics in girls during maturation. Parsons et al 36 examined the effect of lower extremity strengthening on Landing Error Scoring System (LESS) grades in girls aged 10 to 14 years compared with upper extremity strengthening in an active control group. Although no differences were found between the 2 groups, the investigators noted that the upper extremity strengthening program in the active control group may have resulted in improvements in core strength and control. 36 This is significant, as core strengthening has been shown to improve biomechanics in postmaturation athletes.8,10,44,49 The investigators did report increases in strength measures for 10-repetition maximums of squats and lunges in the intervention group and chest presses and curls in the control group 36 ; however, they appeared to assess neither lower extremity strength gains by the control group nor strength gains by individual joint motion in either group. As such, the possibility exists that the strength-training intervention was not of sufficient intensity, frequency, or duration to create a differential effect in strength compared with the active control group. Of note, postintervention measures of grip strength, push-ups, and vertical jump height appeared to be similar across the 2 groups. 36
Given the potential for strength training during maturation to reduce ACL injury risk, it is important to gain an understanding of the effects of strength training on lower extremity biomechanics in this age group. This includes an understanding of the effects of strength training on different lower extremity muscle groups, as well as how strength develops in control participants. The purpose of this study was to examine the effect of a school physical education class–based strength training program on lower extremity strength and jump-landing biomechanics in middle school girls compared with matched control participants. We hypothesized that lower extremity strength would be greater and LESS grades would be lower in the strength-training group after implementation of a school-based strength-training curriculum compared with control participants. We further hypothesized that the magnitude of change in LESS score would be significantly associated with strength changes.
Methods
Participants were female students recruited from local area middle schools in Charlottesville, Virginia, in a clustered, nonrandomized fashion. Participants were required to be in sixth, seventh, or eighth grades at the time of baseline testing and were excluded if they had any musculoskeletal injury that would preclude participation in sports within the prior 3 months. Study participants in the strength-training group (STR; n = 30) were at a single private middle school (height, 1.63 ± 0.07 m; mass, 48.1 ± 7.6 kg; age, 12.5 ± 1.0 y) underwent a 6-month strength-training program, while control participants (CON; n = 30) (height, 1.60 ± 0.09 m; mass, 47.2 ± 8.9 kg; age, 12.6 ± 0.9 y) were selected from a separate observational study using the same data collection methods, which involved 2 public and 2 private middle schools. CON participants were matched to STR participants on a 1-to-1 basis using age (within 4 months), height (within 6 cm), and mass (within 5 kg) as the matching criteria. This study was approved by the institutional review board at the University of Virginia. Informed consent was obtained from the parents of the participants, and assent was obtained from the participants themselves.
Data Collection
In the first month of the academic school year at each location, participants were assessed for their height and mass using a standard scale and stadiometer. A handheld dynamometer (Chatillon DFX2-200; Ametek, Inc) was used to obtain the maximum voluntary contraction strength in newtons, which was then standardized to participant height and mass. Maximum voluntary contraction strength was obtained for the following motions with landmarks assessed by visual assessment and direct palpation following the protocol of the Joint Undertaking to Monitor and Prevent (JUMP)–ACL study: hip extension (prone, dynamometer positioned at posterior distal thigh, hip at neutral, 90° of knee flexion); hip abduction (side-lying dynamometer positioned at lateral distal thigh, hip at neutral, 0° of knee flexion); knee extension (sitting, dynamometer at the anterior distal leg, hip, and knee at 90°); and knee flexion (prone, dynamometer at the posterior distal leg, hip in neutral, knee at 90°). 3 Strength measures from handheld dynamometers using these and similar positions have good to excellent reliability (inter- and intrarater coefficients, ≥0.70).16,26 Each participant was allowed 1 practice trial. Each trial was for a 3-second duration during which verbal encouragement was provided to the participant. Three trials in each position were obtained, with the peak force generated during each recorded, averaged, and standardized to the height and mass of the athlete.
Landing Error Scoring System
Jump-landing biomechanics were assessed using the LESS. The LESS uses 2-dimensional video during a standard jump landing to complete a 17-item scoring rubric. 35 Briefly, the LESS assesses measures such as stance width, foot position, and joint displacement, as well as ankle plantarflexion, trunk flexion/lateral flexion, and knee flexion and medial knee positioning on landing. Individuals with a higher score (representing a higher number of errors) are considered to have worse landing mechanics compared with individuals with lower scores. This instrument has been validated against laboratory-based 3-dimensional motion analyses and has strong interrater reliability.15,35 Furthermore, the LESS has been found to be sensitive to changes in biomechanics from training interventions and have predictive capacity for ACL injuries in adolescent athletes.1,31,32,38 The LESS raters for this study completed an internal training protocol and achieved inter- and intrarater correlation coefficient values of at least 0.80, which demonstrates good reliability.
The protocol from Padua et al 35 was followed for LESS data collection. Briefly, a participant stood on a 30-cm tall box and jumped forward with both feet at the same time to a landing target positioned 50% of the participant’s height away from the box. The participant then immediately completed a second jump at maximal effort in a vertical direction. The jump landing was recorded by 2 video cameras (DCR-HC38 Camcorder; Sony Corp) positioned at a standard distance according to protocol to capture the jump-landing motion from the frontal and sagittal planes. 35 Participants were required to complete at least 1 practice jump and were allowed to complete additional practice trials until they felt comfortable with the task requirements. Participants then performed 5 jump landings during data collection, with the LESS score from the middle 3 jump landings recorded and averaged. LESS scoring was completed in a blinded fashion using a media player (VLC; VideoLAN) on standard computers.
Strength Training
This investigation took advantage of the presence of a new physical education instructor for the strength-training school. This instructor utilized a curriculum that included lower body strength training for the students. The strength training was completed twice a week over the course of the school year. Students started with initial exercises that included simple single-joint exercises performed against gravity, which were primarily intended to target the hip extensors, hip abductors, knee extensors, and knee flexors. Students were then progressed to advanced exercises that included more complex multijoint exercises such as lunges and squats (Table 1). Once these exercises could be performed, students progressed to initial exercises with resistance bands and then to advanced exercises with resistance bands. Students were switched between simple and advanced exercises depending on resistance used and other factors such as school vacation periods. Exercises were performed in 2 to 3 sets of 8 to 12 repetitions. The instructor typically required students to be able to complete all exercises at 3 sets of 12 repetitions with good biomechanical form prior to progression to other exercises; however, determinations for exercise and resistance progression were the sole purview of the class instructor, as it was a part of the instructor’s curriculum for the entire class as opposed to a student-specific investigator-led intervention. The CON participants similarly participated in a physical education class twice a week; however, the curriculum for the CON participants lacked a strength-training component and was focused on general physical activity and exposure to different sports. Both STR and CON participants repeated data collection at the end of the school year approximately 6 months after baseline data collection.
Table 1.
Outline of strength-training exercises
| Initial Exercises | |
|---|---|
| Knee extensions (supine position, hip at 45° of flexion) | |
| Knee flexions (standing position, hip at neutral) | |
| Hip extensions (quadruped position, knee at 90°) | |
| Hip Abductions (side-lying position, knee at 0 degrees) | |
| Advanced Exercises | Progression |
| Forward lunges | Increasing sets (2-3) and repetitions (8-12) |
| Side lunges | Initial to advanced exercises |
| Squats | Advanced to initial with resistance bands |
| Supine bridges | Initial with resistance to advanced with resistance as able |
| Prone planks | Increasing resistance with an exercise group |
| Side-lying planks | |
Data Analysis
SPSS Statistics (Version 27; IBM Corporation) was used for all statistical analyses. Kolmogorov-Smirnov test and Levene test were used to assess for normality and homogeneity of the data, respectively. Strength measures and LESS scores were evaluated using a mixed-model repeated-measures analysis of variance with time (baseline and follow-up) and group (intervention and control) as fixed factors. Dependent and independent t tests were used for post hoc analyses as appropriate. Stepwise linear regression analyses were performed to determine the relationship between individual cohort strength gains and change in LESS scores over time. Alpha was set a priori at 0.05.
Results
A total of 35 participants originally enrolled into the study with 5 dropping out from follow-up testing without providing a reason or being otherwise unavailable for testing at follow-up, resulting in 30 participants with complete data at both time points. These participants were then matched to CON participants based on the previously described matching rubric for age, height, and mass. There were no significant differences in participant characteristics (Table 2).
Table 2.
Participant baseline demographics
| Group | Age, y, Mean (SD) | Height, m, Mean (SD) | Mass, kg, Mean (SD) |
|---|---|---|---|
| Strength training | 12.5 (1.0) | 1.63 (0.07) | 48.1 (7.6) |
| Control | 12.6 (0.9) | 1.60 (0.09) | 47.2 (8.9) |
Strength and LESS
Participant strength and LESS scores for each cohort at each time point are listed in Table 3. The data were found to be homogeneous and distributed normally. The only difference between the 2 groups at baseline was a greater hip extension strength in the CON group than the STR group. A main effect across the combined groups was demonstrated for hip abduction strength over time. Hip extension, hip abduction, and knee flexion strength demonstrated statistically significant group × time interactions, with the STR group demonstrating strength gains over time.
Table 3.
Strength and LESS outcomes a
| Hip Extension Strength | ||||
| Group | Baseline, N·m/kg | Follow-up, N·m/kg | ||
| Strength training (STR) | 3.98 (1.15) | 4.77 (1.80) | ||
| Control | 4.63 (1.08) | 4.38 (1.13) | ||
| Analysis | F (1, 58) | P | Partial η2 | Observed Power |
| Main effect (time) | 2.810 | 0.099 | 0.046 | 0.378 |
| Interaction (group × time) | 9.990 | 0.003 b | 0.147 | 0.875 |
| Hip Abduction Strength | ||||
| Group | Baseline, N·m/kg | Follow-up, N·m/kg | ||
| Strength training | 4.22 (1.09) | 5.13 (2.55) | ||
| Control | 4.59 (1.83) | 4.97 (1.74) | ||
| Analysis | F (1, 58) | P | Partial η2 | Observed Power |
| Main effect (time) | 7.490 | 0.008 | 0.114 | 0.767 |
| Interaction (group × time) | 4.463 | 0.039 c | 0.061 | 0.512 |
| Knee Extension Strength | ||||
| Group | Baseline, N·m/kg | Follow-up, N·m/kg | ||
| Strength training | 4.66 (0.89) | 5.29 (1.66) | ||
| Control | 5.18 (1.96) | 5.29 (1.90) | ||
| Analysis | F (1, 58) | P | Partial η2 | Observed Power |
| Main effect (time) | 1.243 | 0.270 | 0.021 | 0.195 |
| Interaction (group × time) | 1.249 | 0.268 | 0.021 | 0.196 |
| Knee Flexion Strength | ||||
| Group | Follow-up, N·m/kg | Baseline, N·m/kg | ||
| Strength training | 3.27 (0.62) | 3.64 (1.40) | ||
| Control | 3.46 (0.76) | 3.29 (0.76) | ||
| Analysis | F (1, 58) | P | Partial η2 | Observed Power |
| Main effect (time) | 1.120 | 0.294 | 0.019 | 0.180 |
| Interaction (group × time) | 5.186 | 0.026 d | 0.082 | 0.610 |
| Landing Error Scoring System (LESS) | ||||
| Group | Follow-up, error grade | Baseline, error grade | ||
| Strength training | 5.58 (1.21) | 4.86 (1.44) | ||
| Control | 5.60 (1.34) | 5.98 (1.42) | ||
| Analysis | F (1, 58) | P | Partial η2 | Observed Power |
| Main effect (time) | 0.794 | 0.376 | 0.014 | 0.142 |
| Interaction (group × time) | 8.102 | 0.006 e | 0.123 | 0.799 |
Values are presented in mean ± SD.
Control (CON) greater than strength-training (STR) groups at baseline (P = 0.029); STR increased at follow-up compared with baseline (P = 0.003).
STR increased at follow-up compared with baseline (P = 0.023).
STR increased at follow-up compared with baseline (P = 0.023).
STR decreased at follow-up compared with baseline (P = 0.005); CON greater than STR at follow-up (P = 0.004).
There was also a statistically significant group × time interaction with regard to LESS scores with STR participants demonstrating significantly reduced (better) LESS scores over time, as well as significantly reduced LESS scores compared with the CON group at follow-up. Using guidelines of 0.01, 0.06, and 0.14 for small, medium, and large partial η 2 effect sizes, respectively, the effect sizes for significant effects ranged from medium to large.
Regression Analyses
Stepwise linear regression was performed to determine the effect of change in strength over time on change in LESS scores for each group. Strength and LESS scores were significantly related in the STR group, F(2, 27) = 27.879, P < 0.001, with change in hip extension strength and knee extension strength accounting for 67% of the variance in change in the LESS score (Figure 1). The variance inflation factor was less than 1.5, indicating a very low level of collinearity between the 2 predictor variables. The predicted change in the LESS score in STR participants was equal to −0.483(∆hip extension strength) –0.286(∆knee extension strength). While a significant regression equation was found for change in the LESS score for the CON group, F(1, 28) = 18.910, P < 0.001, the only predictor was change in knee extension strength, which accounted for 37% of the variance in change in the LESS score (Figure 2). The predicted change in the LESS score in CON participants was equal to −0.552(∆knee extension strength).
Figure 1.
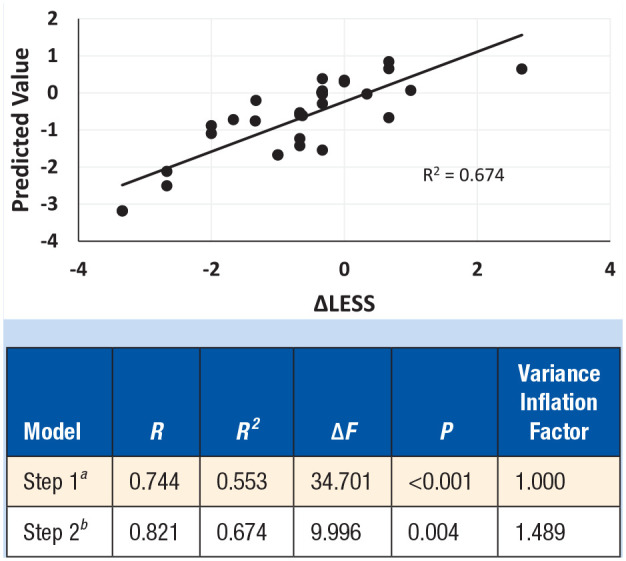
Strength training group linear regression scatterplot. LESS, Landing Error Scoring System.
aPredictors: constant, ∆hip extension strength.
bPredictors: constant, ∆hip extension strength, ∆knee extension strength.
Figure 2.
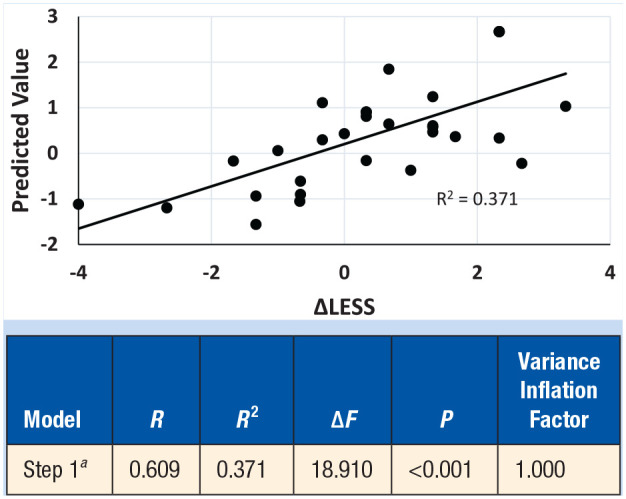
Control group linear regression scatterplot. LESS, Landing Error Scoring System.
aPredictors: constant, ∆knee extension strength.
Discussion
We hypothesized that lower extremity strength would be greater and LESS grades would be lower in the STR group after strength training compared with CON participants. STR participants experienced increases in hip extension, hip abduction, and knee flexion strength over time; similarly, the STR participants had a significant decrease in LESS scores over time, while LESS scores slightly increased in CON. These results largely confirmed our hypothesis.
These results are in contrast to a prior study investigating the effect of strength training in girls during adolescence. Parsons et al 36 randomized female athletes aged 10 to 14 years to a leg-strengthening group and an active control group (upper extremity strengthening) for a period of 12 weeks. No difference in LESS scores between the 2 groups after the intervention. The lack of findings may be attributable to several factors. Sample size was smaller (total N = 36) compared with the current investigation (N = 60). While the strength-training curriculum employed in this study had a similar training frequency (ie, twice per week), the strength training in our study was completed over a 6-month period during the school year. This may have allowed greater effects to occur over time.
Furthermore, it is unclear whether significant lower extremity strength gains were achieved by the intervention group in the study by Parsons et al. 36 They used grip strength, push-ups, and vertical jump height as the strength and performance outcome measures; however, these measures did not directly assess strength of the lower extremities. The most relevant measure (vertical jump height) did not demonstrate significant differences over time. 36 They did report strength gains in 10-repetition maximums in squats and lunges in a subset of the intervention group but did not report on strength changes in these tasks by the control group. The STR group in our investigation demonstrated significant strength gains in 3 of our 4 lower extremity measures relative to the CON group.
Finally, the authors in the prior study acknowledged potential limitations in their study concerning their control group. In using an active control that completed upper extremity strength training, the participants may have received unintended improvements in core strength and neuromuscular control. Poor core strength is considered a risk factor for injury, and core strengthening has been shown to improve neuromuscular control in previous studies.8,10,23,25,51 Thus, an active upper extremity strengthening control group may have confounded their results. The control group in our investigation did not have any formal strength training of any type.
The results from the CON group are largely consistent with previous studies, which have demonstrated a lack of significant neuromuscular performance improvement in girls during adolescence. These studies demonstrated that female athletes tend to have worse performance in lower extremity stiffness and knee abduction angles and moments with landing patterns considered to increase ACL injury risk.9,12,21 Prior studies have also demonstrated that girls tend to have no change or worsening performance in measures of strength, vertical jump height, and power over the course of adolescence.2,30,40,42 The CON group did not demonstrate statistically significant changes in strength.
We also hypothesized that the magnitude of change in the LESS score would be associated with strength changes. The LESS score change over time in the STR group was significantly associated with specific strength gains with hip extension and knee extension accounting for 67% of the variance in the LESS score change. However, the LESS score change over time in the CON group was only associated with strength gains in knee extension, which accounted for 37% of the variance in the LESS score change. It is possible that a formal strength-training program during adolescence may have effects on neuromuscular control beyond what may be gained by naturally occurring strength gains, even when of similar magnitude. This may particularly be the case when considering the types of strength-training tasks implemented toward the end of the curriculum, which included tasks requiring multijoint dynamic control such as lunges and squats. These activities may have resulted in additional mechanisms of effect on neuromuscular control through improved balance and coordination.
We were particularly curious that change in hip abduction strength did not have any predictive capacity for change in the LESS score for either group. We expected that hip abduction would significantly affect LESS scores through improvements in frontal plane control, particularly with respect to medial knee positioning and displacement. However, recent studies suggest that hip extension strength may have a significant role with respect to hip adduction and knee abduction angles.4,43,46 Thus, hip extension strength may be a particularly important target for injury prevention programs, as it may mediate its effect in both important sagittal and frontal plane neuromuscular components.
The baseline biomechanical characteristics of the study participants were generally in line with previous studies including Parsons et al 36 with average LESS scores of 6.8 and 6.4 for the intervention and control groups, respectively. LESS scores were similar to those of Padua et al 34 with demonstrated baseline LESS scores of 5.70 and 5.17 in extended- and short-duration neuromuscular control training participants, respectively, and were slightly higher than the 4.46 average LESS from a prospective cohort study by Padua et al. 32 However, the participants in both of these studies were recruited from a larger age range and included both male and female participants.32,34
It is worth noting that the average LESS improvement of 0.72 in this study is small relative to the neuromuscular training programs employed by Padua et al. 34 In their study, the short-duration group performed the neuromuscular intervention for 3 months, whereas the extended duration group performed the intervention for 9 months. The average improvement in LESS scores were 1.78 and 1.63, respectively, or twice the average gains compared with the current study. While there are differences between the present study and that of Padua et al 34 in terms of the participant populations, additional training modalities such as balance and plyometrics likely provides additional benefit to neuromuscular control.33,47,48
Limitations
This investigation has many limitations. The most significant of these was the lack of data regarding the maturational stage of the participants. This was the result of a restriction imposed by the school leadership at the strength-training school. This limitation may act as a confounding factor, particularly with regard to the matching of CON to STR participants. Furthermore, it is possible that there were differences in progression of maturation over the course of the school year between the STR and CON groups, which also may be a confounding factor.
Strength assessments were conducted using handheld dynamometers. While strength assessments using these techniques have been demonstrated to have good reliability in previous studies,16,26 reliability was not assessed in the current study.
The study was also limited in its assessment of lower extremity biomechanics. The LESS has been demonstrated to be valid and reliable in comparison with laboratory-based 3-dimensional measures of lower extremity jump landing biomechanics15,35; despite this, the relationship between the LESS and ACL injury risk is somewhat unclear. The LESS has not been demonstrated to be predictive of ACL injury in adults, 13 but has been demonstrated to be predictive of ACL injury in elite youth soccer players (mean age, 13.9 ± 1.8 years) with a LESS grade of 5 generating a sensitivity of 86% and a specificity of 64% for ACL injury during the season.
Another limitation was the lack of control in the strength-training program. The physical education instructor instituted the training as a formal component of the curriculum, as opposed to the investigators. Additionally, we did not control for activities that may have occurred outside of the physical education classroom. The advantage of this being a component of a school physical education curriculum is that it provides evidence that a school-based training program may be a feasible means of intervening to prevent the development of neuromuscular control patterns associated with an elevated risk of injury. While several other studies have demonstrated the efficacy of injury prevention programs in older age groups, widespread implementation of these training programs has been lacking. Using a school-based approach may help address these current implementation challenges. 39
Conclusion
A school-based strength training program focused on the hip and knee musculature was significantly associated with improved jump-landing biomechanics that may be relevant to ACL injury risk.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
Funding for this study was provided by the Foundation for Physical Medicine and Rehabilitation Materson Research Grant.
References
- 1. Akbari H, Sahebozamani M, Daneshjoo A, Amiri-Khorasani M, Shimokochi Y. Effect of the FIFA 11+ on landing patterns and baseline movement errors in elite male youth soccer players. J Sport Rehabil. 2019;29:730-737. [DOI] [PubMed] [Google Scholar]
- 2. Beunen G, Malina RM. Growth and physical performance relative to the timing of the adolescent spurt. Exerc Sport Sci Rev. 1988;16:503-540. [PubMed] [Google Scholar]
- 3. Beutler A, de la Motte S, Marshall S, Padua D, Boden B. Muscle strength and qualitative jump-landing differences in male and female military cadets: the JUMP-ACL Study. J Sports Sci Med. 2009;8:663-671. [PMC free article] [PubMed] [Google Scholar]
- 4. Cronin B, Johnson ST, Chang E, Pollard CD, Norcross MF. Greater hip extension but not hip abduction explosive strength is associated with lesser hip adduction and knee valgus motion during a single-leg jump-cut. Orthop J Sports Med. 2016;4:2325967116639578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Cronström A, Creaby MW, Nae J, Ageberg E. Gender differences in knee abduction during weight-bearing activities: a systematic review and meta-analysis. Gait Posture. 2016;49:315-328. [DOI] [PubMed] [Google Scholar]
- 6. Czasche MB, Goodwin JE, Bull AMJ, Cleather DJ. Effects of an 8-week strength training intervention on tibiofemoral joint loading during landing: a cohort study. BMJ Open Sport Exerc Med. 2018;4:e000273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Dai B, Herman D, Liu H, Garrett WE, Yu B. Prevention of ACL injury, part I: injury characteristics, risk factors, and loading mechanism. Res Sports Med. 2012;20:180-197. [DOI] [PubMed] [Google Scholar]
- 8. De Blaiser C, Roosen P, Willems T, Danneels L, Bossche LV, De Ridder R. Is core stability a risk factor for lower extremity injuries in an athletic population? A systematic review. Phys Ther Sport. 2018;30:48-56. [DOI] [PubMed] [Google Scholar]
- 9. DiCesare CA, Montalvo A, Barber Foss KD, et al. Lower extremity biomechanics are altered across maturation in sport-specialized female adolescent athletes. Front Pediatr. 2019;7:268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Ferri-Caruana A, Prades-Insa B, Serra-Añó P. Effects of pelvic and core strength training on biomechanical risk factors for anterior cruciate ligament injuries. J Sports Med Phys Fitness. 2020;60:1128-1136. [DOI] [PubMed] [Google Scholar]
- 11. Ford KR, Myer GD, Hewett TE. Longitudinal effects of maturation on lower extremity joint stiffness in adolescent athletes. Am J Sports Med. 2010;38:1829-1837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Ford KR, Shapiro R, Myer GD, Van Den Bogert AJ, Hewett TE. Longitudinal sex differences during landing in knee abduction in young athletes. Med Sci Sports Exerc. 2010;42:1923-1931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Fox AS, Bonacci J, McLean SG, Spittle M, Saunders N. A systematic evaluation of field-based screening methods for the assessment of anterior cruciate ligament (ACL) injury risk. Sports Med. 2016;46:715-735. [DOI] [PubMed] [Google Scholar]
- 14. Gornitzky AL, Lott A, Yellin JL, Fabricant PD, Lawrence JT, Ganley TJ. Sport-specific yearly risk and incidence of anterior cruciate ligament tears in high school athletes: a systematic review and meta-analysis. Am J Sports Med. 2016;44:2716-2723. [DOI] [PubMed] [Google Scholar]
- 15. Hanzlíková I, Hébert-Losier K. Is the Landing Error Scoring System reliable and valid? A systematic review. Sports Health. 2020;12:181-188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Hébert LJ, Maltais DB, Lepage C, Saulnier J, Crête M, Perron M. Isometric muscle strength in youth assessed by hand-held dynamometry: a feasibility, reliability, and validity study. Pediatr Phys Ther. 2011;23:289-299. [DOI] [PubMed] [Google Scholar]
- 17. Herman DC, Weinhold PS, Guskiewicz KM, Garrett WE, Yu B, Padua DA. The effects of strength training on the lower extremity biomechanics of female recreational athletes during a stop-jump task. Am J Sports Med. 2008;36:733-740. [DOI] [PubMed] [Google Scholar]
- 18. Hewett TE, Myer GD. The mechanistic connection between the trunk, hip, knee, and anterior cruciate ligament injury. Exerc Sport Sci Rev. 2011;39:161-166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Hewett TE, Myer GD, Ford KR. Decrease in neuromuscular control about the knee with maturation in female athletes. J Bone Joint Surg Am. 2004;86:1601-1608. [DOI] [PubMed] [Google Scholar]
- 20. Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33:492-501. [DOI] [PubMed] [Google Scholar]
- 21. Hewett TE, Myer GD, Kiefer AW, Ford KR. Longitudinal increases in knee abduction moments in females during adolescent growth. Med Sci Sports Exerc. 2015;47:2579-2585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Holden S, Boreham C, Delahunt E. Sex differences in landing biomechanics and postural stability during adolescence: a systematic review with meta-analyses. Sports Med. 2016;46:241-253. [DOI] [PubMed] [Google Scholar]
- 23. Kumahara R, Sasaki S, Sasaki E, et al. Effect of a simple core muscle training program on trunk muscle strength and neuromuscular control among pediatric soccer players. J Exp Orthop. 2021;8:36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Lang PJ, Sugimoto D, Micheli LJ. Prevention, treatment, and rehabilitation of anterior cruciate ligament injuries in children. Open Access J Sports Med. 2017;8:133-141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Larwa J, Stoy C, Chafetz RS, Boniello M, Franklin C. Stiff landings, core stability, and dynamic knee valgus: a systematic review on documented anterior cruciate ligament ruptures in male and female athletes. Int J Environ Res Public Health. 2021;18:3826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Mentiplay BF, Perraton LG, Bower KJ, et al. Assessment of lower limb muscle strength and power using hand-held and fixed dynamometry: a reliability and validity study. PLoS One. 2015;10:e0140822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Montalvo AM, Schneider DK, Silva PL, et al. “What’s my risk of sustaining an ACL injury while playing football (soccer)?” A systematic review with meta-analysis. Br J Sports Med. 2019;53:1333-1340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Myer GD, Ford KR, Barber Foss KD, et al. The incidence and potential pathomechanics of patellofemoral pain in female athletes. Clin Biomech (Bristol, Avon). 2010;25:700-707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Myer GD, Sugimoto D, Thomas S, Hewett TE. The influence of age on the effectiveness of neuromuscular training to reduce anterior cruciate ligament injury in female athletes: a meta-analysis. Am J Sports Med. 2013;41:203-215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Nguyen AD, Zuk EF, Baellow AL, Pfile KR, DiStefano LJ, Boling MC. Longitudinal changes in hip strength and range of motion in female youth soccer players: implications for ACL injury, a pilot study. J Sport Rehabil. 2017;26:358-364. [DOI] [PubMed] [Google Scholar]
- 31. Owens BD, Cameron KL, Duffey ML, et al. Military movement training program improves jump-landing mechanics associated with anterior cruciate ligament injury risk. J Surg Orthop Adv. 2013;22:66-70. [DOI] [PubMed] [Google Scholar]
- 32. Padua DA, DiStefano LJ, Beutler AI, de la Motte SJ, DiStefano MJ, Marshall SW. The Landing Error Scoring System as a screening tool for an anterior cruciate ligament injury-prevention program in elite-youth soccer athletes. J Athl Train. 2015;50:589-595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Padua DA, DiStefano LJ, Hewett TE, et al. National Athletic Trainers’ Association position statement: prevention of anterior cruciate ligament injury. J Athl Train. 2018;53:5-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Padua DA, DiStefano LJ, Marshall SW, Beutler AI, de la Motte SJ, DiStefano MJ. Retention of movement pattern changes after a lower extremity injury prevention program is affected by program duration. Am J Sports Med. 2012;40:300-306. [DOI] [PubMed] [Google Scholar]
- 35. Padua DA, Marshall SW, Boling MC, Thigpen CA, Garrett WE, Jr, Beutler AI. The Landing Error Scoring System (LESS) is a valid and reliable clinical assessment tool of jump-landing biomechanics: the JUMP-ACL study. Am J Sports Med. 2009;37:1996-2002. [DOI] [PubMed] [Google Scholar]
- 36. Parsons JL, Sylvester R, Porter MM. The effect of strength training on the jump-landing biomechanics of young female athletes: results of a randomized controlled trial. Clin J Sport Med. 2017;27:127-132. [DOI] [PubMed] [Google Scholar]
- 37. Prodromos CC, Han Y, Rogowski J, Joyce B, Shi K. A meta-analysis of the incidence of anterior cruciate ligament tears as a function of gender, sport, and a knee injury-reduction regimen. Arthroscopy. 2007;23:1320-1325.e6. [DOI] [PubMed] [Google Scholar]
- 38. Pryor JL, Root HJ, Vandermark LW, et al. Coach-led preventive training program in youth soccer players improves movement technique. J Sci Med Sport. 2017;20:861-866. [DOI] [PubMed] [Google Scholar]
- 39. Pullen BJ, Oliver JL, Lloyd RS, Knight CJ. The effects of strength and conditioning in physical education on athletic motor skill competencies and psychological attributes of secondary school children: a pilot study. Sports (Basel). 2020;8:138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Quatman-Yates CC, Myer GD, Ford KR, Hewett TE. A longitudinal evaluation of maturational effects on lower extremity strength in female adolescent athletes. Pediatr Phys Ther. 2013;25:271-276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Quatman-Yates CC, Quatman CE, Meszaros AJ, Paterno MV, Hewett TE. A systematic review of sensorimotor function during adolescence: a developmental stage of increased motor awkwardness? Br J Sports Med. 2012;46:649-655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Quatman CE, Ford KR, Myer GD, Hewett TE. Maturation leads to gender differences in landing force and vertical jump performance: a longitudinal study. Am J Sports Med. 2006;34:806-813. [DOI] [PubMed] [Google Scholar]
- 43. Romanchuk NJ, Del Bel MJ, Benoit DL. Sex-specific landing biomechanics and energy absorption during unanticipated single-leg drop-jumps in adolescents: implications for knee injury mechanics. J Biomech. 2020;113:110064. [DOI] [PubMed] [Google Scholar]
- 44. Sasaki S, Tsuda E, Yamamoto Y, et al. Core-muscle training and neuromuscular control of the lower limb and trunk. J Athl Train. 2019;54:959-969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Shea KG, Pfeiffer R, Wang JH, Curtin M, Apel PJ. Anterior cruciate ligament injury in pediatric and adolescent soccer players: an analysis of insurance data. J Pediatr Orthop. 2004;24:623-628. [DOI] [PubMed] [Google Scholar]
- 46. Stearns KM, Powers CM. Improvements in hip muscle performance result in increased use of the hip extensors and abductors during a landing task. Am J Sports Med. 2014;42:602-609. [DOI] [PubMed] [Google Scholar]
- 47. Sugimoto D, Myer GD, Barber Foss KD, Pepin MJ, Micheli LJ, Hewett TE. Critical components of neuromuscular training to reduce ACL injury risk in female athletes: meta-regression analysis. Br J Sports Med. 2016;50:1259-1266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Sugimoto D, Myer GD, Foss KD, Hewett TE. Specific exercise effects of preventive neuromuscular training intervention on anterior cruciate ligament injury risk reduction in young females: meta-analysis and subgroup analysis. Br J Sports Med. 2015;49:282-289. [DOI] [PubMed] [Google Scholar]
- 49. Tsai YJ, Chia CC, Lee PY, Lin LC, Kuo YL. Landing kinematics, sports performance, and isokinetic strength in adolescent male volleyball athletes: influence of core training. J Sport Rehabil. 2020;29:65-72. [DOI] [PubMed] [Google Scholar]
- 50. Webster KE, Hewett TE. Meta-analysis of meta-analyses of anterior cruciate ligament injury reduction training programs. J Orthop Res. 2018;36:2696-2708. [DOI] [PubMed] [Google Scholar]
- 51. Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J. Deficits in neuromuscular control of the trunk predict knee injury risk: a prospective biomechanical-epidemiologic study. Am J Sports Med. 2007;35:1123-1130. [DOI] [PubMed] [Google Scholar]