

In the United States, 4.6 million children live in a home with an unsecured firearm, increasing their risk for firearm-related injuries, which are the second leading cause of death in US children.1,2 In 2020, the United States witnessed an unprecedented rise in firearm sales as the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic strained communities with additional psychosocial and economic stressors.3 Current literature evaluating firearm injuries and the SARS-CoV-2 pandemic includes only single-center data, adult populations, or young children, excluding pediatric suicide.4,5 We aimed to quantify pediatric firearm-related and total encounters during the initial 2020 SARS-CoV-2 pandemic period, as compared to these periods in the previous 3 years.
METHODS
We used International Classification of Diseases, 10th Revision (ICD-10) discharge diagnosis codes to conduct a cross-sectional comparison of pediatric (age 0–18 years) firearm-related and total emergency department (ED) and hospital encounters between calendar weeks 9 and 36 (corresponding to approximately March to August) 2020 and 2017–2019 at 44 US children’s hospitals participating in the Pediatric Health Information System (PHIS) database. The primary outcome was firearm-related encounters, defined as an initial encounter for a penetrating injury from a powder-charged weapon identified by ICD-10 discharge code (see Supplemental Information).6 The median weekly volumes in 4-week blocks for 2017–2019 were compared to the median in 2020 by using the Wilcoxon rank test. Differences in medians were estimated by using quantile regression. Similarly, weekly volumes in 2020 were compared to the 25th and 75th percentile for 2017–2019.
RESULTS
There were 2510 firearm-related encounters during the 4-year study period, of which 798 (32%) occurred in 2020. Of these, 45.6% included adolescents aged 15 to 18 years, 78.8% were boys, 61.7% were non-Hispanic Black children, 62.7% lived in the South census region, and 48.9% resided in a very low Child Opportunity Index neighborhood (Table 1). There were no differences in cohort characteristics in 2020 vs 2017–2019 (Table 1).
TABLE 1.
Characteristics of Study Population, March to August 2017–2020
| Firearm-Related Encounters |
|||
|---|---|---|---|
| Characteristics | 2017–2019 (n = 1712), n (%) | 2020 (n = 798), n (%) | P |
| Age, y | |||
| 0–4 | 168 (9.8) | 94 (11.8) | .381 |
| 5–9 | 209 (12.2) | 105 (13.2) | |
| 10–14 | 516 (30.1) | 235 (29.4) | |
| 15–18 | 819 (47.8) | 364 (45.6) | |
| Sex | |||
| Male | 1339 (79) | 622 (78.8) | .905 |
| Female | 355 (21) | 167 (21.2) | |
| Race and/or ethnicity | |||
| Non-Hispanic white | 313 (18.3) | 138 (17.3) | .185 |
| Non-Hispanic Black | 1064 (62.1) | 492 (61.7) | |
| Hispanic | 222 (13) | 103 (12.9) | |
| Asian | 5 (0.3) | 8 (1) | |
| Other | 108 (6.3) | 57 (7.1) | |
| Payer | |||
| Government | 1286 (75.1) | 621 (77.8) | .135 |
| Private | 285 (16.6) | 108 (13.5) | |
| Other | 141 (8.2) | 69 (8.6) | |
| Intention | |||
| Unintentional | 988 (57.7) | 502 (62.9) | .053 |
| Intentional or self-harm | 46 (2.7) | 17 (2.1) | |
| Assault | 593 (34.6) | 243 (30.5) | |
| Undetermined | 58 (3.4) | 25 (3.1) | |
| Legal intervention | 5 (0.3) | 6 (0.8) | |
| Multiplea | 22 (1.3) | 5 (0.6) | |
| Census region | |||
| Midwest | 454 (26.5) | 192 (24.1) | .330 |
| Northeast | 99 (5.8) | 40 (5) | |
| South | 1007 (58.8) | 500 (62.7) | |
| West | 152 (8.9) | 66 (8.3) | |
| Rurality | |||
| Rural | 171 (10) | 77 (9.6) | .616 |
| Urban | 1516 (88.6) | 713 (89.3) | |
| Child Opportunity Indexb | |||
| Very low | 879 (51.3) | 390 (48.9) | .339 |
| Low | 354 (20.7) | 178 (22.3) | |
| Moderate | 232 (13.6) | 121 (15.2) | |
| High | 155 (9.1) | 64 (8) | |
| Very high | 87 (5.1) | 39 (4.9) | |
| Disposition | |||
| Died | 95.5 (5.5) | 50 (6.3) | .659 |
| ED treat and/or release | 689 (40.2) | 328 (41.1) | |
| Hospitalized | 928 (54.2) | 420 (52.6) | |
Multiple intent category used for cases with >1 assigned ICD-10 discharge diagnosis code
The Child Opportunity Index is a composite metric based on 29 neighborhood indicators collected from public and proprietary sources at the census-tract level, assigned to 5 ordered levels of opportunity (very low, low, moderate, high, and very high) to describe the level of neighborhood opportunity.12
Compared to 2017–2019, total encounters in 2020 decreased in each 4-week block and by 42.3% overall (Fig 1A). In contrast, firearm-related encounters increased by 38.8% from a median of 575 encounters in 2017–2019 to 798 encounters in 2020, increasing in each 4-week block with a range of 116.9% to 167.9% (Fig 1B). An observed increase in overall firearm-related encounters in 2020 remained when using 25th percentile (+57.7%) or 75th percentile (+26.5%) volumes for 2017–2019. The overall difference in medians was statistically significant (+9.0 encounters per week; P < .001).
FIGURE 1.
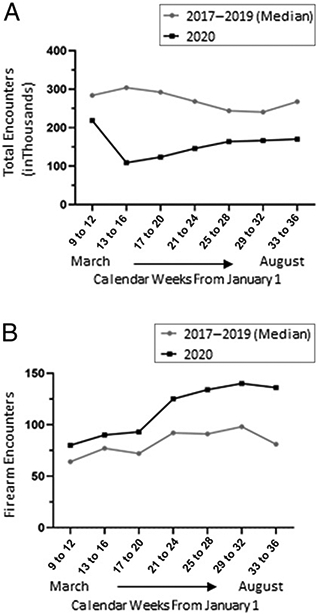
Comparing total and firearm-related encounters in 2020 to 2017–2019. A, Total ED and hospital encounter volumes in 2020 compared to 2017–2019. B, Firearm-related encounter volumes in 2020 compared to 2017–2019.
DISCUSSION
Firearm-related encounters at US children’s hospitals increased significantly in March to August 2020 compared to 2017–2019, whereas total encounters decreased substantially.
The combination of unparalleled firearm sales, heightened social and economic distress, and children atypically home from school created a uniquely risky environment for firearm injury. Consistent with previous literature, we found higher rates of firearm injuries in older non-Hispanic Black adolescent boys from Southern regions.7 In addition, we found no significant changes in demographics, rurality, or region comparing firearm-related encounters in 2020 to 2017–2019, suggesting the SARS-CoV-2 pandemic was associated with an increase in pediatric firearm injuries without a shift in the population most at risk. Additionally, nearly half of our firearm cohort resided in a very low Child Opportunity Index neighborhood. This highlights socioeconomic inequities, many of which overlap with risk factors associated with violence, including poverty, inadequate housing, and lower economic opportunity.8,9 Although in recent studies, researchers also found that firearm injuries among adults and very young children increased during the SARS-CoV-2 pandemic, this is the first report highlighting the significant increase in pediatric firearm encounters for all ages during the pandemic despite unprecedented declines in total encounters.
Limitations include retrospective design, restricted time frame of available data, and reduced generalizability to community hospitals and rural settings. Despite likely underrepresenting older adolescents managed in adult trauma centers, we demonstrated a significant increase in firearm encounters, highlighting the impact firearm injuries have on children of all ages. Although we recognize database limitations, we chose PHIS given its nationally representative sample, inclusion of inpatient and ED encounters, relatively even representation of injury intents, and up-to-date data. Lastly, we did not make inferences on the basis of coded injury intent because of known discordance between codes and injury description.10 Different trends may emerge as extended time lines and additional data sets are used.
These findings underscore the critical importance of preventing firearm injuries, intensified in the context of a global pandemic, by applying effective tools such as counseling on safe firearm storage, promoting crisis support and violence intervention resources, supporting responsible firearm legislation, and advocating for firearm safety research.11
Supplementary Material
FUNDING:
Dr Carroll was supported by grant T32HS026122 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.
ABBREVIATIONS
- ED
emergency department
- ICD-10
International Classification of Diseases, 10th Revision
- PHIS
Pediatric Health Information System
- SARS-CoV-2
severe acute respiratory syndrome coronavirus 2
Footnotes
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
REFERENCES
- 1.Azrael D, Cohen J, Salhi C, Miller M. Firearm storage in gun-owning households with children: results of a 2015 national survey. J Urban Health. 2018;95(3):295–304 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Centers for Disease Control and Prevention. WISQARS data visualization. Available at: https://wisqars-viz.cdc.gov:8006/explore-data/home. Accessed December 24, 2020
- 3.Levine PB, McKnight R. Three million more guns: the Spring 2020 spike in firearm sales. 2020. Available at: https://www.brookings.edu/blog/up-front/2020/07/13/three-million-more-guns-the-spring-2020-spike-in-firearm-sales/. Accessed December 21, 2020
- 4.Abdallah HO, Zhao C, Kaufman E, et al. Increased firearm injury during the COVID-19 pandemic: a hidden urban burden. J Am Coll Surg. 2021;232(2):159–168.e3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bleyer A, Siegel SE, Thomas CR. Increasing rate of unintentional firearm deaths in youngest Americans: firearm prevalence and Covid-19 pandemic implication [published online ahead of print January 11, 2021]. J Natl Med Assoc. doi: 10.1016/j.jnma.2020.12.005 [DOI] [PubMed] [Google Scholar]
- 6.Centers for Disease Control and Prevention. Firearm violence. 2020. Available at: https://www.cdc.gov/violenceprevention/firearms/fastfact.html. Accessed January 8, 2021
- 7.Fowler KA, Dahlberg LL, Haileyesus T, Gutierrez C, Bacon S. Childhood firearm injuries in the United States. Pediatrics. 2017;140(1):e20163486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Carter PM, Cook LJ, Macy ML, et al. ; Pediatric Emergency Care Applied Research Network (PECARN). Individual and neighborhood characteristics of children seeking emergency department care for firearm injuries within the PECARN network. Acad Emerg Med. 2017;24(7):803–813 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Centers for Disease Control and Prevention. Risk and protective factors. 2020. Available at: https://www.cdc.gov/violenceprevention/youthviolence/riskprotectivefactors.html. Accessed December 26, 2020
- 10.Donnelly KA, Badolato GM, Goyal MK. Determining intentionality of pediatric firearm injuries by international classification of disease code [published online ahead of print October 22, 2020]. Pediatr Emerg Care. doi: 10.1097/PEC.0000000000002272 [DOI] [PubMed] [Google Scholar]
- 11.Barkin SL, Finch SA, Ip EH, et al. Is office-based counseling about media use, time-outs, and firearm storage effective? Results from a cluster-randomized, controlled trial. Pediatrics. 2008;122(1). Available at: www.pediatrics.org/cgi/content/full/122/1/e15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Acevedo-Garcia D, Noelke C, McArdle N, et al. Racial and ethnic inequities in children’s neighborhoods: evidence from the new Child Opportunity Index 2.0. Health Aff (Millwood). 2020;39(10):1693–1701 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.