

Abstract
The objective of this study was to evaluate the efficacy of combination drug pulse therapy in maintaining lipid levels in patients intolerant of a daily dose of statins. Twenty‐three patients, previously receiving aggressive statin therapy, were treated twice weekly with rosuvastatin or atorvastatin in different dosages along with ezetimibe as well as daily doses of bile acid sequestrant for a mean period of 4.5 months. The recommended National Cholesterol Education Program Adult Treatment Panel III goals had already been achieved in 78% of patients (n=18) before starting combination pulse therapy. This combination therapy significantly increased high‐density lipoprotein cholesterol values by 5.82% (t=2.138, P=.044), while the increases in total cholesterol, low‐density lipoprotein cholesterol, triglyceride, and apolipoprotein B levels compared with baseline were not statistically significant. Overall, 3 of 23 patients (13%) discontinued the combination therapy because of muscle‐related symptoms over a mean course of 4.5 months of treatment.
Statins are the most effective and practical class of drugs for reducing low‐density lipoprotein (LDL) cholesterol levels to established and lower target levels in patients at high risk for atherosclerotic cardiovascular disease. Statins are easy to administer and generally have good patient acceptance. However, some patients cannot tolerate these medications when taken daily because of the effects on liver and skeletal muscles. Therefore, tolerability concerns become a particularly important issue when aggressive therapy is administered routinely. In the past, a few studies have demonstrated the effects of using every‐other‐day low‐dose statin therapy, 1 but to the best of our knowledge, no study has evaluated the efficacy of combination drug pulse therapy in maintaining lipid levels in patients intolerant of daily doses of statins.
Methods
Twenty‐three patients selected in this retrospective review chart study were initially started on daily intensive therapy with rosuvastatin or atorvastatin but were unable to tolerate this therapeutic regimen primarily because of fatigue, myalgia, and weakness. In an effort to improve tolerance, they received the same statins in different dosages along with ezetimibe twice weekly for a mean period of 4.5 months in a clinic setting. In addition, patients were given 3 tablets of colesevelam 625 mg twice a day on a daily basis. Prefasting and postfasting lipid levels were recorded before the next dose of the statin was administered. The statin doses used in pulse therapy were based on previously prescribed amounts in intensive statin therapy. Overall, 26% of patients (n=6) were treated with low‐dose rosuvastatin (5 and 10 mg), and 35% of patients (n=8) received a medium to high dose of rosuvastatin (20 and 40 mg). Nine patients (39%) received only a low to medium dose of atorvastatin (20 and 40 mg). Also, ezetimibe 10 mg twice weekly was administered in all patients (Figure 1). Pretreatment and posttreatment fasting lipid levels were measured in clinical laboratories routinely used by patients.
Figure 1.
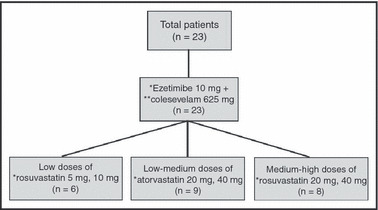
Schematic presentation of different dosages used in combination pulse therapy. *One tablet twice weekly; **3 tablets twice daily.
Results
The mean age of the participants was 59.7±10.5 years; 14 were female and 9 were male. A paired‐samples t test, which compared the pretreatment and posttreatment measures of total cholesterol, LDL cholesterol, high‐density lipoprotein (HDL) cholesterol, triglycerides, and apolipoprotein B, was conducted on the 23 patients. Although the average for all 5 measures increased from baseline, only the increase in HDL cholesterol (3.04±6.83 mg/dL) was statistically significant (t=2.138, P=.044) (Table).
Table.
Lipid Levels at Baseline and Change Post–Combination Therapy
| Lipid Value, mg/dL | Baseline | Change | Percentage Change |
|---|---|---|---|
| Total cholesterol | 151.5±33.6 | 4.3±26.0 | 5.6 |
| LDL cholesterol | 75.2±31.8 | 1.0±24.6 | 10.1 |
| HDL cholesterol | 59.0±14.9 | 3.0±6.8a | 5.8 |
| Triglycerides | 86.9±47.5 | 3.0±23.2 | 13.3 |
| Apolipoprotein B | 63.4±23.1 | 3.3±16.8 | 13.0 |
Abbreviations: HDL, high‐density lipoprotein; LDL, low‐density lipoprotein. aStatistically significant.
An analysis of variance, comparing the changes in all 5 measures by drug, was also conducted. Only the change in HDL cholesterol was significantly different by drug type, and rosuvastatin produced a significantly greater increase (F=5.604, P=.028).
A paired‐sample t test on the group receiving atorvastatin showed no significant change on any of the 5 measures. The same test on the patients receiving rosuvastatin revealed a significant increase only in HDL cholesterol (t=2.972, P=.011), thus indicating that the increase in HDL cholesterol for the group overall came primarily from the patients who received rosuvastatin (Figure 2).
Figure 2.
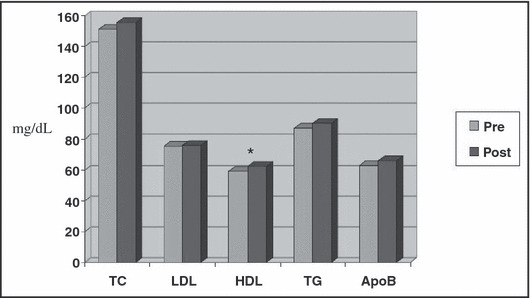
Lipid levels pre– and post–combination therapy for all measures. TC indicates total cholesterol; LDL, low‐density lipoproteon cholesterol; HDL, high‐density lipoprotein cholesterol; TG, triglycerides; ApoB, apolipoprotein B. *Statistically significant change.
It is noteworthy that before starting the combined pulse therapy, National Cholesterol Education Program Adult Treatment Panel III–recommended LDL cholesterol goals had already been achieved in 78% of patients (n=18). However, because of statin intolerance in these patients, primarily due to myalgia, this combination therapy was prescribed for them. Three patients (13%) discontinued this therapeutic regimen because of fatigue and myalgia but were included in the analysis. The remaining 87% of patients (n=20) tolerated the therapy well and were able to maintain their low levels of LDL cholesterol, total cholesterol, triglycerides, and apolipoprotein B (Figure 3 and Figure 4).
Figure 3.
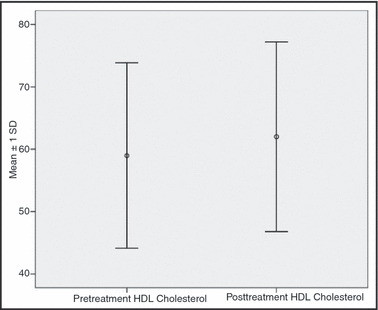
Error bar: high‐density lipoprotein (HDL) cholesterol level pretreatment and posttreatment.
Figure 4.
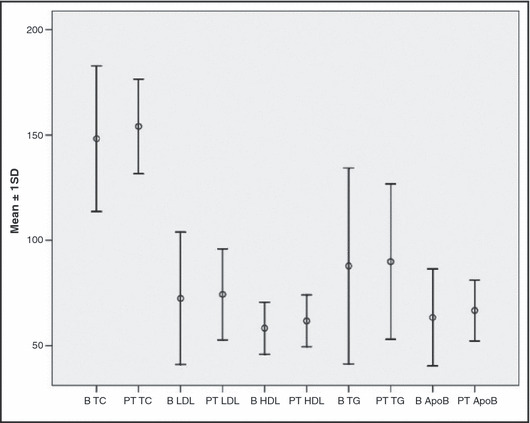
Error bar: lipid level pretherapy and posttherapy. B indicates baseline; TC, total cholesterol; PT, posttreatment; LDL, low‐density lipoprotein cholesterol; HDL, high‐density lipoprotein cholesterol; TG, triglycerides; ApoB, apolipoprotein B.
Discussion
The present retrospective chart review study presents an alternative approach to treating and maintaining lipid levels in patients unable to tolerate statins on a daily basis. A low LDL cholesterol level was maintained in 91% of patients (n=20), in accordance with guidelines from the National Cholesterol Education Program Adult Treatment Panel III. In addition, HDL cholesterol increased significantly (t=2.972, P=.011). Most authorities believe that increasing statin doses is associated with skeletal muscle symptoms. However, outcomes achieved in the present study showed that in treating patients who were intolerant to daily doses of a statin, an individualized dosage approach based on a patient’s statin history should be adopted. Furthermore, administering statins in pulse mode allows a chance for the body to recover from a statin’s myopathic effects and increases tolerance. The long half‐life of both rosuvastatin (19 hours) and atorvastatin (14 hours) further supports the use of twice‐weekly statin therapy in patients intolerant of daily doses of statins. The HDL cholesterol increases reported in our study are not in consensus with results achieved in the previous study done with twice‐weekly rosuvastatin. 2 However, HDL cholesterol did rise in another study done with every‐other‐day rosuvastatin therapy, 1 which suggests that rosuvastatin dosage should be adjusted on an individual basis.
Ezetimibe is a nonstatin lipid‐lowering agent that inhibits cholesterol absorption from the small intestine. Studies have shown that when used in combination with statins, ezetimibe results in incremental lowering of total and LDL cholesterol. 3 , 4 , 5 , 6 Moreover, it does not increase the incidence of myopathy or rhabdomyolysis when administered with statins. Similarly, the addition of colesevelam to statin therapy effectively lowers total and LDL cholesterol and does not cause any adverse effects on liver and skeletal muscles. This implies that administering nonstatin lipid‐lowering agents further enhances the overall efficacy achieved by statins.
Conclusions
In the present retrospective chart review study, we found that the combination pulse therapy was well tolerated, increased HDL cholesterol values, and maintained low LDL cholesterol levels in patients intolerant of daily doses of statins. However, the study is limited by its retrospective design and a small sample size. There was no control group. Also, we did not systemically study the statin symptoms but used patients’ ability to tolerate statin treatment for a longer period as a surrogate for improved tolerance for pulse treatment. Although we cannot reach any rigid conclusions from the present study, statin pulse therapy is a valid alternative and the results achieved in the present study could be a step forward in treating patients intolerant of daily doses of statins.
References
- 1. Wongwiwatthananukit S, Sansanayudh N, Dhummauppakorn R, et al. Efficacy and safety of rosuvastatin every other day compared with once in patients with hypercholesterolemia. Ann Pharmacother. 2006;40:1917–1923. [DOI] [PubMed] [Google Scholar]
- 2. Gadarla M, Kearns AK, Thompson PD. Efficacy of rosuvastatin twice a week in patients intolerant to daily statins. Am J Cardiol. 2008;101:1747–1748. [DOI] [PubMed] [Google Scholar]
- 3. Bruckert E, Giral P, Tellier P. Perspectives in cholesterol lowering therapy: the role of ezetimibe, a new selective inhibitor of intestinal cholesterol absorption. Circulation. 2003;107(25):3124–3128. [DOI] [PubMed] [Google Scholar]
- 4. Mauro VF, Tuckerman CE. Ezetimibe for management of hypercholesterolemia. Ann Pharmacother. 2003;37(6):839–848. [DOI] [PubMed] [Google Scholar]
- 5. Kastelein JJ. The future of lipid‐lowering therapy: the big picture. Neth J Med. 2003;61(suppl 5):35–39. [PubMed] [Google Scholar]
- 6. Weston C. Place of ezetimibe in clinical practice. Hosp Med. 2003;64(8):473–478. [DOI] [PubMed] [Google Scholar]