

Abstract
Background and Objectives
Aging is characterized by a functional shift of the immune system toward a proinflammatory phenotype. This derangement has been associated with cognitive decline and has been implicated in the pathogenesis of dementia. Diet can modulate systemic inflammation; thus, it may be a valuable tool to counteract the associated risk for cognitive impairment and dementia. The present study aimed to explore the associations between the inflammatory potential of diet, assessed with an easily applicable, population-based, biomarker-validated diet inflammatory index (DII), and the risk for dementia in community-dwelling older adults.
Methods
Individuals from the Hellenic Longitudinal Investigation of Aging and Diet (HELIAD) were included in the present cohort study. Participants were recruited through random population sampling and were followed up for a mean of 3.05 (standard deviation 0.85) years. Dementia diagnosis was based on standard clinical criteria. Those with baseline dementia or missing cognitive follow-up data were excluded from the analyses. The inflammatory potential of diet was assessed through a DII score that considers literature-derived associations of 45 food parameters with levels of proinflammatory and anti-inflammatory cytokines in the blood; higher values indicated a more proinflammatory diet. Consumption frequencies were derived from a detailed food frequency questionnaire and were standardized to representative dietary intake normative data from 11 different countries. Analysis of dementia incidence as a function of baseline DII scores was performed by Cox proportional hazards models.
Results
Analyses included 1,059 individuals (mean age 73.1 years, 40.3% male, mean education 8.2 years), 62 of whom developed incident dementia. Each additional unit of DII score was associated with a 21% increase in the risk for dementia incidence (hazard ratio 1.21 [95% confidence interval 1.03–1.42]; p = 0.023). Compared to participants in the lowest DII score tertile, participants in the highest one (maximal proinflammatory diet potential) were 3 (95% confidence interval 1.2–7.3; p = 0.014) times more likely to develop incident dementia. The test for trend was also significant, indicating a potential dose-response relationship (p = 0.014).
Discussion
In the present study, higher DII scores (indicating greater proinflammatory diet potential) were associated with an increased risk for incident dementia. These findings might avail the development of primary dementia preventive strategies through tailored and precise dietary interventions.
Population aging is poised to become one of the most significant social transformations of the 21st century, as indicated by the substantial increases in the proportion of older adults across most populations globally. The worldwide population ≥65 years of age numbered 382 million in 1980 and 962 million in 2017 and is estimated to reach nearly 2.1 billion by 2050.1 The disability burden of age-related cognitive decline and dementia is also expected to increase as a consequence of this drastic demographic transition. This is an alarming projection, considering that in the last Global Burden of Disease Study in 2010, Alzheimer disease (AD) and other dementias were already accounting for 0.46 of total global disability-adjusted life-years.2
Aging is accompanied by physiologic alterations in both the innate and adaptive arms of the immune system, a process called immunosenescence.3 One of the hallmarks of immunosenescence is the institution of a chronic low-grade subclinical systemic inflammatory state, characterized by high circulating levels of proinflammatory cytokines and mediators, including interleukin (IL)-1, IL-6, C-reactive protein (CRP), and tumor necrosis factor (TNF).4 This process is mediated mainly by chronically activated macrophages and monocytes and contributes to many aging-associated phenotypes (hence the term inflammaging).5,6 Brain-wise, inflammaging has been associated with cognitive impairment,7 AD,8 and cerebral small vessel disease, a component of vascular dementia (VaD),9 hence potentially contributing to the most common causes of dementia and cognitive decline.
Substantial evidence suggests that many foods, nutrients, and nonnutrient food components can modulate the inflammatory status both acutely and chronically.10 Therefore, diet, a modifiable lifestyle factor, might have a valuable role in combating inflammaging11 and counteracting its associated risk for dementia and late-life cognitive impairment. From this standpoint, a method to characterize and measure the inflammatory potential of individuals' diets could help develop tailored and precise dietary interventions and cognitive health maintenance strategies. A diet inflammatory index (DII) score consisting of 45 food parameters, including energy, nutrients, bioactive compounds, and foods/spices, has been described in the present literature.12 These parameters were selected from a systematic review of studies using standard dietary assessment methods and presented significant associations with biomarkers of inflammation,12 providing a comprehensive way to explore associations between the inflammatory potential of diet and different health-related outcomes.
However, only a limited number of studies have explored potential relationships between the DII and dementia. In 2 cross-sectional studies, DII scores were inversely associated with performance on cognitive tests assessing memory13 and global cognitive function,14 whereas in another study, DII was not associated with global cognitive function.15 High DII scores were also associated with increased odds for mild cognitive impairment (MCI).14 Another study also reported a strong inverse association between baseline DII and both global cognitive functioning and verbal memory evaluated 13 years later.16 Prospective data from 1 study revealed that higher DII scores were associated with significantly increased risk for MCI or probable dementia and greater cognitive decline over time.17
The aim of the present study was to augment the relatively small body of evidence regarding the DII and its potential association with the risk for dementia while addressing some of the limitations of the current literature. Specifically, the only prospective population-based study that has explored these relationships included only female participants, a fact that limits the generalizability of its results.17 The present study presents a prospective investigation of the inflammatory potential of diet, assessed through a biomarker-validated, non–population-specific DII,12 and dementia incidence in a non–sex-specific population of community-dwelling older adults without dementia.
Methods
Participants
Individuals from the Hellenic Longitudinal Investigation of Aging and Diet (HELIAD) were included in the present cohort study. HELIAD is a population-based, multidisciplinary study designed to estimate the epidemiology of dementia and other neuropsychiatric conditions associated with aging in the Greek population. Participants are being re-evaluated at intervals of ≈3 years, repeating the baseline examination and consensus diagnosis at each follow-up; 2 evaluations per person have been completed so far.18 Two centers, 1 located in Marousi (a suburb of Athens, Greece) and the other in the city of Larissa (part of the province of Thessaly in central Greece), took part in this study. Participants were selected through random sampling of community-dwelling individuals ≥65 years of age. More details about participant characteristics and the study design and methodology can be found in previously published work.18-21 The participants included in the present analyses were selected from the entire study population according to the following inclusion criteria: no baseline dementia, available follow-up data, and available baseline dietary information.
Standard Protocol Approvals, Registrations, and Patient Consents
The present study protocol has been approved by the ethical standards committees of the National and Kapodistrian University of Athens and University of Thessaly, and all participants gave written informed consent before their participation.
Diagnostic Criteria
Diagnoses were reached through diagnostic consensus meetings of all the main investigators involved in the project, both neurologists and neuropsychologists, as previously described.21 In particular, the diagnosis of dementia and type thereof was based on DSM-IV-TR criteria,22 and the designation of probable or possible AD was made according to the National Institute of Neurologic and Communicative Disorders and Stroke/Alzheimer Disease and Related Disorders Association criteria.23 The diagnosis of VaD was based on a history or clinical evidence of stroke, the presence of a clear temporal relation between stroke and the onset of dementia, and the Hachinski Ischemia Scale score.24 Lewy body and frontotemporal dementias were diagnosed from respective criteria.25,26 Dementia staging was performed by the semistructured interview of the Clinical Dementia Rating Scale, which assesses 6 domains of cognitive and functional performance.27 MCI was diagnosed according to the Petersen28 criteria.
Dietary Assessment
Dietary intake was evaluated through a semiquantitative food frequency questionnaire (FFQ) that has been validated for the Greek population.29 Briefly, the FFQ included information on all main food groups consumed during the last month (i.e., 69 questions on consumption of dairy products, cereals, fruits, vegetables, meat, fish, legumes, added fats, alcoholic beverages, stimulants, sweets).18 The questionnaire was administered by a trained dietician, and the caregiver assisted the participant during the survey when necessary. Responses were converted to daily intakes of specific food items and were extrapolated into macronutrient and micronutrient intakes by using US Department of Agriculture food composition tables and selecting items that most appropriately match foods eaten in Greece, as well as selected analyses of national recipes and local foods (eMethods 1, links.lww.com/WNL/B626).
Diet Inflammatory Index
The DII was created on the basis of evidence suggesting that dietary factors influence inflammation.12 It consists of 45 food parameters that include various macronutrients and micronutrients, bioactive compounds (including flavonoids), and foods/spices, each associated with an inflammatory effect score. A detailed description of the DII12 and its construct validation30-33 have been published elsewhere.17 Briefly, after a review of the literature, 45 foods and nutrients were found to be associated with 6 cardinal inflammatory biomarkers (IL-1β, IL-4, IL-6, IL-10, TNF-α, and CRP). A value was assigned to each food parameter according to its association with these inflammatory biomarkers: +1, 0, or −1 for a positive, null, or inverse association, respectively. Scores were weighted by the characteristics of the study reporting these associations. Weighted scores were tallied to obtain the food parameter–specific overall inflammatory effect score (eTable 1, links.lww.com/WNL/B626). Dietary intake data were standardized on the basis of mean and SD values derived from a world composite database, containing data from 11 different countries, representing a wide range of diets across diverse populations globally. Participant's exposure to each food parameter was then expressed as a z score relative to the standard global mean. The standardized dietary intake estimates were then converted to centered percentiles for each DII component. Subsequently, these centered percentiles were multiplied by the corresponding component-specific inflammatory effect scores and summed to obtain the overall DII score for each individual. The DII score characterizes an individual's diet on a spectrum from maximally anti-inflammatory to maximally proinflammatory, with a higher score indicating a more proinflammatory diet and a lower score indicating a more anti-inflammatory diet. For the purposes of the present study, 36 FFQ-derived food parameters were used for DII calculation.
Critical Evaluation of Reported Energy Intake
The validity of reported energy intake was assessed according to the methodology proposed by Goldberg and colleagues34 and revised by Black and colleagues.35 Briefly, for each participant, basal metabolic rate (BMR) was estimated with the Food and Agriculture Organization/World Health Organization/United Nations University age- and sex-specific prediction equations36; the ratio of the FFQ-estimated energy intake/BMR was then calculated. This ratio was compared to individual-specific cutoffs, calculated from the physical activity level of each participant, to assess for energy misreporting. If the energy intake/BMR ratio of a participant was below or above these cutoffs, then the reported energy intake was considered nonplausible, and these participants were classified as nonacceptable energy reporters, whereas the rest of the participants were considered to be acceptable energy reporters. In the present study, the physical activity level of each participant was derived from a validated physical activity questionnaire (Athens Physical Activity Questionnaire).37
Clinical Comorbidity Index Score
The clinical comorbidity index score was calculated as the sum of the following clinical conditions: hypertension, diabetes, coronary heart disease, myocardial infraction, congestive heart failure, heart arrhythmia, other heart disease, dyslipidemia, chronic obstructive pulmonary disease or other pulmonary disease, thyroid disease, liver disease, renal insufficiency, peptic ulcer disease, peripheral vascular disease, cancer, arthritis, traumatic brain injury, epilepsy, vitamin B12 deficiency, Parkinson disease, Huntington disease, multiple sclerosis, normal-pressure hydrocephalus, and Down syndrome.
Other Covariates
Age at study enrollment, energy intake, baseline MCI, education, and sex were also included in the analyses as possible confounders because these factors have been associated with the risk of developing dementia.38-42
Statistical Analyses
Baseline participant characteristics by availability of follow-up data, availability of dietary data, dementia incidence, DII score, and validity of reported energy intake were compared through analysis of variance for continuous variables and Pearson χ2 for categorical variables (followed by post hoc Bonferroni tests in the case of multiple comparisons).
DII score was initially treated as a continuous variable. To explore the exposure-disease relationship for nonlinearity and the potential presence of threshold effects, we also ranked DII score into tertiles, each containing a third of the study sample. In all analyses, the first tertile (maximal anti-inflammatory diet potential) was used as the reference and was compared to the other tertiles (i.e., second and third), with the last one indicating maximal proinflammatory diet potential. Age, years of education, energy intake, the clinical comorbidity index score, and the duration of follow-up interval were treated as continuous variables. Sex (female, male) and MCI (no MCI at baseline, MCI at baseline) were treated as categorical variables.
Analysis of dementia incidence as a function of DII scores was performed with Cox proportional hazards models. In these models, dementia was defined as the dichotomous outcome. The time-to-event variable was defined as time from baseline evaluation to visit of dementia diagnosis; participants who did not develop dementia were censored at the time of their last evaluation. DII score (from the baseline visit) was the main predictor (in a continuous form initially and in tertile form for trend test calculation subsequently). Covariate adjustment was conducted as follows: model 1 was unadjusted; model 2 was adjusted for age, sex, years of education, energy intake, and baseline MCI; and model 3 was further adjusted for the clinical comorbidity index score. The proportionality of hazards assumption was tested through the Schoenfeld residuals method. Because the variable expressing years of education violated the proportional hazards assumption, we included its interaction with the natural logarithm of the time variable in the adjusted Cox models.43
Sensitivity Analysis for Acceptable Energy Reporting
Sensitivity analyses were performed by recomputing the unadjusted and adjusted Cox regression models while excluding participants classified as nonacceptable energy reporters. Specifically, because the computation of our main predictor (DII) is influenced by energy intake12 and energy intake was estimated with a self-report tool (i.e., prone to reporting error),44,45 we excluded from the analyses participants with a nonplausible energy intake. This criterion was instituted to increase the validity of energy intake estimation and DII calculation.
Supplementary Analyses
To increase our confidence that the inflammatory potential of diet was not affected by early dementia processes, we conducted a moderator analysis by including the DII score × baseline MCI interaction term in an adjusted (for age, sex, years of education, energy intake, and baseline MCI) Cox model.
Statistical analyses were conducted with STATA version 16 (StataCorp LLC, College Station, TX) and IBM SPSS version 26 (IBM Corp; Armonk, NY). Hypothesis tests were 2 sided, and nominally significant α values were defined as p ≤ 0.05.
Data Availability
Anonymized data not published within this article may be shared on request from any qualified investigator for purposes of replicating procedures and results.
Results
Missing Data Analysis
The initial HELIAD study sample consisted of 1,850 participants without dementia (Figure 1). Cognitive follow-up information was available for 1,072 participants (Figure 1). Compared to participants with available cognitive follow-up, participants with missing follow-up (n = 778) were slightly older (mean [SD] age 74.1 [5.5] vs 73.2 [5.0] years; p < 0.001) and had higher proportions of baseline MCI (n = 125 [16.1%] vs 118 [11.0%]; p = 0.001). There were no significant differences between participants with missing and those with available follow-up in terms of years of education, sex, or clinical comorbidity index score. Most important, there was no difference in DII scores.
Figure 1. Flowchart Describing Sample.

There were 1,072 participants without dementia with available cognitive follow-up data; 13 of these participants were lacking baseline dietary information, so they were excluded from the analyses (Figure 1). Compared to participants with available dietary information (n = 1,059), participants with missing dietary information were less educated (mean [SD] years of education 4.8 [4.1] for those with missing data vs 8.2 [4.9] for those included; p = 0.015), but they did not differ with respect to any other characteristics.
Baseline Clinical and Sociodemographic Characteristics
Among the 1,059 participants who were included in the analyses, 62 participants developed incident dementia (53 developed AD, 5 developed VaD, 3 developed Lewy body dementia, and 1 developed dementia due to underlying psychiatric disorder) over a mean follow-up of 3.05 years (SD 0.85 years; range 6.08 years). Participants' baseline clinical and sociodemographic characteristics by dementia incidence and by the inflammatory potential of their diets (DII score tertiles) are given in Tables 1 and 2, respectively. Individuals who developed dementia were older, were less educated, had higher DII scores, and were more likely to have MCI at baseline compared to those who did not, but they did not differ in terms of sex, energy intake, or clinical comorbidity index score. Comparison of participant characteristics by DII score tertiles revealed that participants consuming diets with greater inflammatory potential were older, were less educated, and reported lower energy intakes. Moreover, compared to women, a lower proportion of men tended to consume diets with a high inflammatory potential. There was no association between DII score tertile and MCI relative frequencies or clinical comorbidity index score.
Table 1.
Participants' Baseline Clinical and Sociodemographic Characteristics by Incidence of Dementia

Table 2.
Participants' Baseline Clinical and Sociodemographic Characteristics by DII score Tertile

DII Score and Dementia Incidence in Total Sample
Both unadjusted and adjusted Cox proportional hazards models revealed that greater inflammatory diet potential was associated with a significantly higher risk for incident dementia (Table 3). Specifically, in the adjusted models, there was a 21% increase in the risk for dementia incidence with each additional unit of DII score (model 2, Table 3). Compared to participants in the lowest DII score tertile, participants in the highest one (maximal proinflammatory diet potential) were 3 times more likely to develop incident dementia (model 2, Table 3 and Figure 2). In addition, the significant test for trend was indicative of a potential dose-response relationship (model 2, Table 3). The model further adjusted for the clinical comorbidity index score revealed almost identical results (model 3, Table 3).
Table 3.
Unadjusted and Adjusted Cox Regression Models

Figure 2. Survival Curves Based on Cox Regression Comparing Cumulative Dementia Incidence in Participants Belonging to Each Diet Inflammatory Index Score Tertile (p for Trend = 0.014).
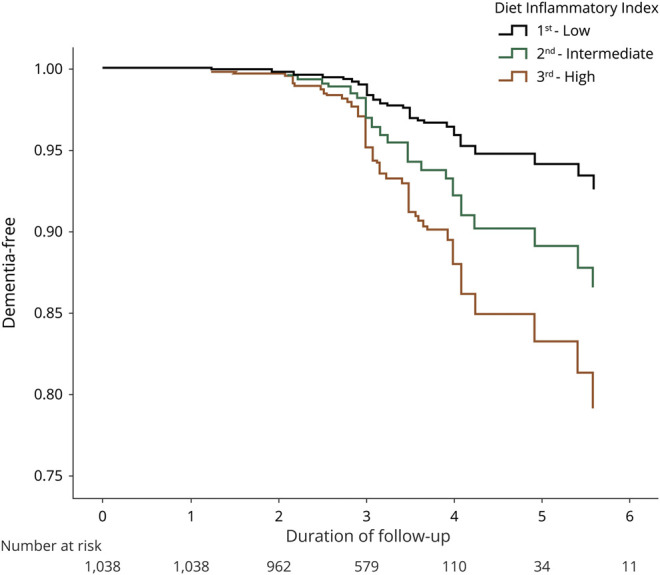
Figure is derived from a model that is adjusted for age, sex, years of education, energy intake, and baseline mild cognitive impairment.
Last, the adjusted Cox model including the DII score × baseline MCI interaction revealed a nonsignificant interaction term (hazard ratio [HR] 1.11 [95% confidence interval [CI] 0.88–1.40]; p = 0.363).
DII Score and Dementia Incidence in Acceptable Energy Reporters
Nonacceptable energy reporters (n = 244 [23%]; 105 [10%] low energy reporters and 139 [13%] high energy reporters) did not differ from acceptable energy reporters (n = 815 [77%]) in terms of age, sex, years of education, MCI relative frequencies, or DII scores. Compared to nonacceptable energy reporters, a higher proportion of men were acceptable energy reporters (n = 347 [43%] vs 80 [33%]; p = 0.006).
Both unadjusted and adjusted Cox proportional hazards models revealed that greater inflammatory diet potential was associated with a significantly higher risk for incident dementia. Specifically, in the adjusted models, there was a 26% increase in the risk for dementia incidence with each additional unit of DII score (HR 1.26 [95% CI 1.05–1.52]; p = 0.013). Compared to participants in the lowest DII score tertile, participants in the highest one (maximal proinflammatory diet potential) were 3.43 times more likely to develop incident dementia (HRhighest tertile vs lowest 3.43 [95% CI 1.25–9.46]; p = 0.017). In addition, the significant test for trend was indicative of a potential dose-response relationship (ptrend = 0.017).
Discussion
In the present study, higher DII scores were associated with an increase in the risk for dementia incidence. The gradual risk increase for higher DII score tertile, suggests a potential dose-response relationship between the inflammatory potential of diet and the risk for incident dementia. The observed associations remained unchanged and significant even after excluding from the analyses those participants who reported an energy intake that could be considered nonacceptable due to potential dietary intake misreporting.
A prospective US population-based study of 7,085 women 65 to 79 years of age revealed that higher DII scores were associated with higher risk of MCI or probable dementia and with greater cognitive decline and earlier onset of cognitive impairment.17 The present results replicate and expand these previous findings, supporting their generalizability to a non–sex-specific population of older adults without dementia; however, their validity and reproducibility need to be further explored and ascertained by future research.
Studies that have evaluated cognitive performance as a function of DII score have reported findings consistent with the present results. Specifically, higher baseline DII scores were associated with lower cognitive performance evaluated 13 years later in a French cohort of 3,080 individuals with a mean age (SD) of 52.0 (4.6) years.16 Furthermore, 2 cross-sectional studies, 1 conducted in a Korean population of 316 older adults ≥65 years of age and the other in a representative sample (n = 1723) of US older adults 60 to 85 years of age, reported inverse associations between DII scores and global cognitive function, verbal memory,14 episodic memory, working memory, and semantic memory.13
On the other hand, in a cross-sectional study conducted in 641 participants from Tasmania, Australia, with a mean age (SD) of 69.8 (7.4) years, no association was observed between DII scores and global cognitive function.15 However, the relationship between the predictor (DII score) and the outcome (global cognitive function) was evaluated at a single time point, whereas the evaluation of the rate of change of the outcome as a function of the predictor over time might have yielded different findings. Mathematically, if the former analysis is based on a function estimating the change of the outcome variable with respect to the change of the predictor variable, the latter analysis is based on the time derivative of that particular function. In other words, although 1 individual with a high DII score and 1 individual with a low DII score might have the same cognitive performance at a specific time point, the first individual might also exhibit a more rapid cognitive decline over the course of time that eventually reaches the threshold of clinical dementia.
After ≈40 years of age, similar to other systems of the body, the immune system undergoes senescence, and certain immune system features begin to reveal effectual decline.7 In addition, the immune system begins to adversely affect human aging, possibly contributing to the development and clinical course of age-related conditions such as cardiovascular, metabolic, and neurodegenerative diseases.46 Immunosenescence can be considered an example of antagonistic pleiotropy in which the beneficial effects of the immune system, attributed to the neutralization of harmful agents earlier in life, become detrimental later in life due to recent advances in life expectancy not foreseen by evolution.47
A hallmark feature of immunosenescence is the increase in cellular production of proinflammatory mediators such as CRP, TNF-α, IL-6, and IL-1β that contribute to the institution of a chronic subclinical systemic inflammatory state, a process that is collectively referred to as inflammaging. Systemic proinflammatory cytokines may reach the CNS and lead to reduced brain-derived neurotrophic factor levels, glutamatergic activation (excitotoxicity), oxidative stress, and induction of apoptosis,48 which constitute some of the mainstream neuroinflammatory and neurodegenerative pathways involved in the development of dementia.
Inflammaging has been associated with cognitive decline and has been implicated in the pathophysiology of AD, VaD, and Parkinson disease, which account for the vast majority of dementia cases worldwide. Proinflammatory mediators, especially CRP, have been associated with cognitive impairment in the elderly,46 and increased plasma levels have been observed in individuals with Parkinson disease and cognitive impairment.49 In addition, inflammaging is increasingly being recognized as a risk factor for age-related cerebral small vessel disease, which is most prevalent among the elderly and contributes to the high global disease burden of stroke and VaD in this population.9
Although immunosenescence and inflammaging are aging-related processes present in the majority of individuals, genetic, environmental, lifestyle, and nutritional factors are responsible for their interindividual heterogeneity.50 Increasing evidence has revealed that complex interactions between food components and histone modification, DNA methylation, noncoding RNA expression, and chromatin remodeling influence the inflammaging phenotype. Therefore, dietary interventions might prove to be a valuable tool in decreasing the risk for dementia and late-life cognitive impairment by counteracting inflammaging and modulating its phenotypic expression through epigenetic and other mechanisms.11 Within this framework, a widely applicable and reliable method to characterize individuals' diet according to their inflammatory potential is an important priority in the pursuit of healthy aging and cognitive health maintenance strategies.
Nevertheless, the present results should be interpreted in view of potential limitations. A significant number of study participants (n = 689) were lost to follow-up, and while they did not differ in terms of the main predictor (DII score), this might still pose a threat to the internal validity of the study by introducing informative censoring (e.g., compared to participants who developed dementia, cognitively healthy individuals may be more likely to drop out because they do not feel the need to be further examined). Dementia diagnosis was based only on clinical criteria, so the possibility of disease misclassification bias cannot be entirely excluded. In addition, the relatively short follow-up of the present study (mean 3.05 years, SD 0.85 years) raises the possibility of reverse causality. To further investigate this issue, we conducted a moderator analysis. The relationship between DII score and incident dementia was not moderated by the presence of MCI at baseline. Assuming that neuropathologic alterations related to early dementia processes would have been present in individuals with MCI, these results decrease the likelihood that reverse causality accounts for our findings. Moreover, assessment of dietary intake by an FFQ may be subject to measurement error,21 including dietary misreporting due to social desirability or cognitive deficits, which might lead to differential exposure misclassification. However, all the necessary precautions to limit food consumption misreporting were taken, including the administration of questionnaires by trained dietitians and the contribution of participant's caregiver in data collection when deemed necessary. In addition, to increase our confidence that the observed exposure-disease relationship was not affected by potential measurement errors related to energy intake estimation, we conducted sensitivity analyses restricting the sample to only acceptable energy reporters. Of note, potential errors might also arise from the fact that the US Department of Agriculture food database was applied to Greek foods for dietary intake estimation; however, selected analyses of local foods were also considered for the estimation of daily intakes. Serum levels of inflammatory biomarkers were not available to directly characterize the systemic inflammatory status of study participants. Nonetheless, on the basis of previous validation studies exploring the associations of DII with several inflammatory biomarkers among different and diverse populations, we assumed that DII scores accurately reflect the underlying inflammatory state. Furthermore, repeated measurements of DII were not available; therefore, the temporal stability of the score could not be ascertained. However, in a previous large-scale study, the average change of the DII score in a 3-year period was −0.36, representing ≈2% of the index range. In the present study, data on eugenol, ginger, onion, turmeric, garlic, oregano, pepper, rosemary, and saffron were not available; therefore, these components were not considered during DII calculation. Because all of these food parameters have anti-inflammatory effect scores, the DII scores in this study likely underestimate the anti-inflammatory potential of the participants' diets.
On a different note, the longitudinal design of the present study instills confidence in our findings and sheds some light on the temporal relationship between the inflammatory potential of diet and dementia incidence. The diagnosis of dementia was reached through expert consensus meetings and widely acceptable published criteria. The inflammatory potential of diet was evaluated with a literature-derived, biomarker-validated, population-based DII.12 Last, study participants were selected through random population sampling of community-dwelling individuals, which, together with the use of a non–population-specific DII, increases external validity and generalizability.
Aging-related immune system changes result in the institution of a chronic low-grade subclinical inflammatory state (inflammaging). This process has been implicated in the pathologic processes of AD and VaD, possibly contributing to a significant proportion of late-life cognitive impairment and dementia disease burden worldwide. Accruing evidence supports that diet plays a central role in the regulation of chronic inflammation, and dietary modulation of inflammaging might be a valuable preventive strategy for dementia and cognitive decline. In the present study, we were able to demonstrate that the inflammatory potential of diet, assessed with an easily applicable tool,12 was positively associated with the risk for dementia in community-dwelling older adults without dementia. Although the validity and reproducibility of these associations need to be ascertained by further studies, they contribute substantial information to the present literature and might assist the efforts for the development of population-level dietary guidelines and effective healthy aging strategies.
Glossary
- AD
Alzheimer disease
- BMR
basal metabolic rate
- CI
confidence interval
- CRP
C-reactive protein
- DII
diet inflammatory index
- DSM-IV-TR
Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision
- FFQ
food frequency questionnaire
- HELIAD
Hellenic Longitudinal Investigation of Aging and Diet
- HR
hazard ratio
- IL
interleukin
- MCI
mild cognitive impairment
- TNF
tumor necrosis factor
- VaD
vascular dementia
Appendix. Authors
Study Funding
The HELIAD study was supported by the following grants: IIRG-09-133014 (Alzheimer's Association), 189 10,276/8/9/2011 (ESPA-EU program Excellence Grant—ARISTEIA), and ΔΥ2β/οικ.0.51657/14.4.2009 (Ministry of Health and Social Solidarity, Greece). D. Kapogiannis was supported by the Intramural Research Program of the National Institute on Aging, NIH.
Disclosure
S. Charisis, E. Ntanasi, M. Yannakoulia, C.A. Anastasiou, M.H. Kosmidis, E. Dardiotis, A. Gargalionis, K. Patas, S. Chatzipanagiotou, I. Mourtzinos, K. Tzima, G. Hadjigeorgiou, P. Sakka, and D. Kapogiannis report no disclosures relevant to the manuscript. N. Scarmeas reports personal fees from Merck Consumer Health and Eisai and personal fees from NIH unrelated to this manuscript. Go to Neurology.org/N for full disclosures.
References
- 1.United Nations. World Population Ageing—Highlights. 2017. 10.18356/10e32e81-en [DOI] [Google Scholar]
- 2.Chin JH, Vora N. The global burden of neurologic diseases. Neurology. 2014;83(4):349-351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Aiello A, Farzaneh F, Candore G, et al. Immunosenescence and its hallmarks: how to oppose aging strategically? A review of potential options for therapeutic intervention. Front Immunol. 2019;10:2247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ferrucci L, Fabbri E. Inflammageing: chronic inflammation in ageing, cardiovascular disease, and frailty. Nat Rev Cardiol. 2018;15(9):505-522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Franceschi C, Bonafè M, Valensin S, et al. Inflamm-aging: an evolutionary perspective on immunosenescence. Ann NY Acad Sci. 2000;908:244-254. [DOI] [PubMed] [Google Scholar]
- 6.Shaw AC, Joshi S, Greenwood H, Panda A, Lord JM. Aging of the innate immune system. Curr Opin Immunol. 2010;22(4):507-513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Fard MT, Stough C. A review and hypothesized model of the mechanisms that underpin the relationship between inflammation and cognition in the elderly. Front Aging Neurosci. 2019;11:56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Giunta B, Fernandez F, Nikolic WV, et al. Inflammaging as a prodrome to Alzheimer's disease. J Neuroinflammation. 2008;5:51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Li T, Huang Y, Cai W, et al. Age-related cerebral small vessel disease and inflammaging. Cell Death Dis. 2020;11(10):932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Minihane AM, Vinoy S, Russell WR, et al. Low-grade inflammation, diet composition and health: current research evidence and its translation. Br J Nutr. 2015;114(7):999-1012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Szarc Vel Szic K, Declerck K, Vidaković M, Vanden Berghe W. From inflammaging to healthy aging by dietary lifestyle choices: is epigenetics the key to personalized nutrition? Clin Epigenetics. 2015;7(1):33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Shivappa N, Steck SE, Hurley TG, Hussey JR, Hébert JR. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014;17(8):1689-1696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Frith E, Shivappa N, Mann JR, Hébert JR, Wirth MD, Loprinzi PD. Dietary inflammatory index and memory function: population-based national sample of elderly Americans. Br J Nutr. 2018;119(5):552-558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Shin D, Kwon SC, Kim MH, et al. Inflammatory potential of diet is associated with cognitive function in an older adult Korean population. Nutrition. 2018;55-56:56-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zabetian-Targhi F, Srikanth VK, Smith KJ, et al. Associations between the dietary inflammatory index, brain volume, small vessel disease, and global cognitive function. J Acad Nutr Diet. 2021;121(5):915-924.e3. [DOI] [PubMed] [Google Scholar]
- 16.Kesse-Guyot E, Assmann KE, Andreeva VA, et al. Long-term association between the dietary inflammatory index and cognitive functioning: findings from the SU.VI.MAX study. Eur J Nutr. 2017;56(4):1647-1655. [DOI] [PubMed] [Google Scholar]
- 17.Hayden KM, Beavers DP, Steck SE, et al. The association between an inflammatory diet and global cognitive function and incident dementia in older women: the Women's Health Initiative Memory Study. Alzheimers Dement. 2017;13(11):1187-1196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Charisis S, Ntanasi E, Yannakoulia M, et al. Plasma GSH levels and Alzheimer's disease: a prospective approach: results from the HELIAD study. Free Radic Biol Med. 2021;162:274-282. [DOI] [PubMed] [Google Scholar]
- 19.Dardiotis E, Kosmidis MH, Yannakoulia M, Hadjigeorgiou GM, Scarmeas N. The Hellenic Longitudinal Investigation of Aging and Diet (HELIAD): rationale, study design, and cohort description. Neuroepidemiology. 2014;43(1):9-14. [DOI] [PubMed] [Google Scholar]
- 20.Ntanasi E, Yannakoulia M, Mourtzi N, et al. Prevalence and risk factors of frailty in a community-dwelling population: the HELIAD study. J Aging Health. 2020;32(1):14-24. [DOI] [PubMed] [Google Scholar]
- 21.Charisis S, Ntanasi E, Yannakoulia M, et al. Mediterranean diet and risk for dementia and cognitive decline in a Mediterranean population. J Am Geriatr Soc. 2021;69(6):1548-1559. [DOI] [PubMed] [Google Scholar]
- 22.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. American Psychiatric Association; 2000. [Google Scholar]
- 23.McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer's disease: report of the NINCDS-ADRDA work group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology. 1984;34(7):939-944. [DOI] [PubMed] [Google Scholar]
- 24.Hachinski VC, Iliff LD, Zilhka E, et al. Cerebral blood flow in dementia. Arch Neurol. 1975;32(9):632-637. [DOI] [PubMed] [Google Scholar]
- 25.McKeith IG, Galasko D, Kosaka K, et al. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the Consortium on DLB International Workshop. Neurology. 1996;47(5):1113-1124. [DOI] [PubMed] [Google Scholar]
- 26.Neary D, Snowden JS, Gustafson L, et al. Frontotemporal lobar degeneration: a consensus on clinical diagnostic criteria. Neurology. 1998;51(6):1546-1554. [DOI] [PubMed] [Google Scholar]
- 27.Morris JC. The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology. 1993;43(11):2412-2414. [DOI] [PubMed] [Google Scholar]
- 28.Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med. 2004;256(3):183-194. [DOI] [PubMed] [Google Scholar]
- 29.Bountziouka V, Bathrellou E, Giotopoulou A, et al. Development, repeatability and validity regarding energy and macronutrient intake of a semi-quantitative food frequency questionnaire: methodological considerations. Nutr Metab Cardiovasc Dis. 2012;22(8):659-667. [DOI] [PubMed] [Google Scholar]
- 30.Shivappa N, Steck SE, Hurley TG, et al. A population-based dietary inflammatory index predicts levels of C-reactive protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. 2014;17(8):1825-1833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Tabung FK, Steck SE, Zhang J, et al. Construct validation of the dietary inflammatory index among postmenopausal women. Ann Epidemiol. 2015;25(6):398-405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Shivappa N, Hebert JR, Marcos A, et al. Association between dietary inflammatory index and inflammatory markers in the HELENA study. Mol Nutr Food Res. 2017;61(6). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Shivappa N, Hébert JR, Rietzschel ER, et al. Associations between dietary inflammatory index and inflammatory markers in the Asklepios Study. Br J Nutr. 2015;113(4):665-671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Goldberg GR, Black AE, Jebb SA, et al. Critical evaluation of energy intake data using fundamental principles of energy physiology, 1: derivation of cut-off limits to identify under-recording. Eur J Clin Nutr. 1991;45(12):569-581. [PubMed] [Google Scholar]
- 35.Black AE. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate. a practical guide to its calculation, use and limitations. Int J Obes Relat Metab Disord. 2000;24(9):1119-1130. [DOI] [PubMed] [Google Scholar]
- 36.FAO/WHO/UNU. Human energy requirements: report of a joint FAO/WHO/UNU expert consultation: Rome, 17-24 October 2001. AO Food Nutr Tech Rep Ser. 2004:103. [Google Scholar]
- 37.Kavouras SA, Maraki MI, Kollia M, Gioxari A, Jansen LT, Sidossis LS. Development, reliability and validity of a physical activity questionnaire for estimating energy expenditure in Greek adults. Sci Sport. 2016;31(3):e47-e53. [Google Scholar]
- 38.Sharp ES, Gatz M. Relationship between education and dementia: an updated systematic review. Alzheimer Dis Assoc Disord. 2011;25(4):289-304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Riedel BC, Thompson PM, Brinton RD. Age, APOE and sex: triad of risk of Alzheimer's disease. J Steroid Biochem Mol Biol. 2016;160:134-147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Petersen RC, Stevens JC, Ganguli M, Tangalos EG, Cummings JL, DeKosky ST. Practice parameter: early detection of dementia: mild cognitive impairment (an evidence-based review). Neurology. 2001;56(9):1133-1142. [DOI] [PubMed] [Google Scholar]
- 41.Morris JC, Storandt M, Miller JP, et al. Mild cognitive impairment represents early-stage Alzheimer disease. Arch Neurol. 2001;58(3):397-405. [DOI] [PubMed] [Google Scholar]
- 42.Luchsinger JA, Tang MX, Shea S, Mayeux R. Caloric intake and the risk of Alzheimer disease. Arch Neurol. 2002;59(8):1258-1263. [DOI] [PubMed] [Google Scholar]
- 43.Tabachnick BG, Fidell LS. Using Multivariate Statistics, 6th ed. Pearson; 2012. [Google Scholar]
- 44.Horner NK, Patterson RE, Neuhouser ML, Lampe JW, Beresford SA, Prentice RL. Participant characteristics associated with errors in self-reported energy intake from the Women's Health Initiative food-frequency questionnaire. Am J Clin Nutr. 2002;76(4):766-773. [DOI] [PubMed] [Google Scholar]
- 45.Bedard D, Shatenstein B, Nadon S. Underreporting of energy intake from a self-administered food-frequency questionnaire completed by adults in Montreal. Public Health Nutr. 2004;7(5):675-681. [DOI] [PubMed] [Google Scholar]
- 46.Barbé-Tuana F, Funchal G, Schmitz CRR, Maurmann RM, Bauer ME. The interplay between immunosenescence and age-related diseases. Semin Immunopathol. 2020;42(5):545-557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.De Martinis M, Franceschi C, Monti D, Ginaldi L. Inflamm-ageing and lifelong antigenic load as major determinants of ageing rate and longevity. FEBS Lett. 2005;579(10):2035-2039. [DOI] [PubMed] [Google Scholar]
- 48.Miller AH, Maletic V, Raison CL. Inflammation and its discontents: the role of cytokines in the pathophysiology of major depression. Biol Psychiatry. 2009;65(9):732-741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Lindqvist D, Hall S, Surova Y, et al. Cerebrospinal fluid inflammatory markers in Parkinson's disease: associations with depression, fatigue, and cognitive impairment. Brain Behav Immun. 2013;33:183-189. [DOI] [PubMed] [Google Scholar]
- 50.Costantini E, D'Angelo C, Reale M. The role of immunosenescence in neurodegenerative diseases. Mediators Inflamm. 2018;2018:6039171. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Anonymized data not published within this article may be shared on request from any qualified investigator for purposes of replicating procedures and results.